
Abstract
This study aimed to investigate the perceptions of patient-centered care (PCC) among inpatients in Guangdong Province (GD), China. Based on these perspectives, we sought to understand existing PCC practices in medical institutions and identify the impacts of inpatients’ sociodemographic status on their perceived PCC. A self-developed PCC questionnaire was used to investigate inpatients’ perceptions of PCC. A cross-sectional survey was conducted in nine tertiary-level hospitals across five cities in GD. Descriptive statistics was used to describe the levels of PCC in GD. The differences in PCC levels across different sociodemographic groups were assessed using analysis of variance and multivariate linear regression. Valid responses were provided by 1863 inpatients. The mean overall PCC score was 8.58 (standard deviation [SD] = 1.36); inpatients from the Pearl River Delta and eastern GD area reported significantly higher scores than those from western and northern GD area (P<.01). Inpatients from rural areas tended to report lower PCC scores than their urban counterparts. Among the PCC questionnaire sub-domains, inpatients scored highest and lowest in “patient experience” (mean = 8.96, SD = 1.34) and “medical insurance” (mean = 7.93, SD = 2.05), respectively. This study provided a comprehensive overview of inpatients’ perceptions of PCC in the public healthcare system in GD, China. Our findings highlighted that a majority of inpatients were satisfied with the PCC in public healthcare system; however, a significant discrepancy between inpatients with different sociodemographic status remained.
Introduction
The primary goal of patient-centered care (PCC) is to empower patients to become active participants in their healthcare and improve individual health outcomes. This makes PCC an approach worth promoting in almost any healthcare delivery system. 1 The number of studies featuring the term “patient-centered care” has been continuously increasing over the past 3 decades, 2 and PCC is now recognized as an essential characteristic of high-quality healthcare services.3,4 In particular, themes such as biopsychosocial perspective, coordinated care, integrated and continuous care, proactive and prepared care teams, shared decision-making, and individual needs are commonly associated with PCC.5-7 Additionally, under the traditional healthcare system, clinicians mainly focus on treating the disease, rather than providing holistic care for the patient, and focus on using advanced technology, rather than respecting patients’ preference. However, modern medicine is complicated; an increasing number of studies have shown that PCC can effectively address this limitation, 8 reshape the humanistic nature of medical services, 9 and improve the quality and efficiency of healthcare services.10,11
The practice of PCC enjoys global consensus, as all top-performing medical systems worldwide promote PCC. 12 This trend is especially notable in China, whose healthcare system has undergone rapid and profound changes. 13 In recent years, the Chinese government has paid greater attention to promoting healthcare system reforms, such as strengthening investment in primary healthcare to improve the accessibility of medical services, 14 reforming the public medical insurance payment system to control increasing burden of medical expenses, improving the medical legal system, and providing medical professionals with remuneration that reflects the value of their services. 15 These efforts have considerably enhanced patients’ medical treatment experience and their perception of PCC. However, the current understanding of PCC’s connotation is not uniform across countries,16,17 and inpatients’ perception of PCC remains unknown in GD.
With decades of rapid economic development as its foundation, China currently has the largest number of middle-income earners in the world. This implies that Chinese people’s consumption of healthcare has become more refined; that is, people’s perceptions of health care have changed from being subsistence-based to quality-based. 17 In this context, patients develop a desire to be more involved in their medical treatment, concomitantly expecting to have better healthcare experiences, more satisfactory medical treatment environments, friendlier medical professionals, and safer and more efficient medical services. 18 These emergent patient preferences are the core characteristics of PCC19,20; therefore, it is necessary to investigate to what extent the patients’ needs have been met.
Although the benefits of PCC have been recognized by China’s medical community, 21 there has been no specific research into inpatients’ perception of PCC in China, especially in GD. Consequently, the PCC best practices for hospitals remain unclear. 22 Therefore, this study aimed to investigate the inpatients’ perspectives on PCC and identify the influential role of sociodemographic variables on their perceived PCC levels in GD, China.
Methods
Study Design
A cross-sectional survey was conducted from November 2019 to January 2020 in nine tertiary-level hospitals across five central cities in GD. The target cities represent the province’s four economic regions. This ensured that the respondent sample was balanced and representative of the demographic characteristics of the sample area. The survey was conducted with a large sample of inpatients in GD to investigate their perceived issues with PCC (eg, problems in communication with medical professionals and medical expenditure) and identify the impact of inpatients’ sociodemographic status on their perception of PCC.
Setting
GD has the largest economy in China, with a population of approximately 113 million. In 2018, its gross domestic product (GDP) was 9727.8 billion RMB (US$ 1393.3 billion) and its gross health expenditure was 519.9 billion RMB (US$ 74.4 billion). 23 However, similar to the unbalanced development in different regions of China, the development levels in GD vary across regions. 24 For example, GDP per capita of the Pearl River Delta (PRD) region was US$ 18,928 in 2018, which was equivalent to that of upper-middle-income countries, and was over three times higher than that of the western and northern GD that remain extremely underdeveloped. 25 The PRD region is ranked the highest in development, followed by the western, eastern, and northern regions. 23 The per capita GDP of the PRD region was more than three times that of western GD in 2018. This variation in development among the regions indicates that considering samples from each region and the differences in their respective perspectives would be helpful for a better understanding of the status quo of PCC in China.
Sampling
We selected a total of nine tertiary-level hospitals (the highest level of hospital grading in China) from five central cities located across the four economic regions of GD. For each city, one to three of the largest and most comprehensive tertiary general hospitals were selected as investigation sites; this was done to ensure that the respondents were strongly representative of the area. The number of hospitals surveyed in each region was determined based on the number of permanent residents of that region. The target cities were Guangzhou (PRD, 3 hospitals selected), Shenzhen (PRD, 3 hospitals selected), Meizhou (east, 1 hospital selected), Shaoguan (north, 1 hospital selected), and Zhanjiang (west, 1 hospital selected).
The minimum sample size needed for this study was approximately 1,443, which was determined using a frequently used sample size calculator. 26 The key parameters used in the calculation are as follows: confidence level, 95%; confidence interval, 2.58; and population of GD, 113 million. The anticipated minimum sample sizes for each of the four regions (PRD, east, north, and west) were 807, 212, 212, and 212, respectively; these were determined based on the proportions of their respective permanent resident populations.
All inpatients present in the general wards of the target hospitals during the survey period were invited to participate in the survey anonymously. The inclusion criteria were as follows: (1) aged ≥18 years; (2) able to read and speak Mandarin; (3) no cognitive problems; and (4) able to provide informed consent.
Measurement
A self-developed PCC questionnaire was used to investigate the perception of PCC among the inpatients in GD. The questionnaire was developed based on a literature review, semi-structured focus group interviews, and expert consultation.
First, we conducted a literature review to ensure that the questionnaire contained the universal elements of classic PCC models applied worldwide, including those of the World Health Organization, 27 the Picker institute, 28 the King’s Fund, 29 and other existing models. Subsequently, we conducted semi-structured group interviews about PCC across five cities in GD. Focus group interviews were conducted with different stakeholders, which included 55 patients, 21 doctors, and 17 nurses, from orthopedics, rehabilitation medicine, endocrinology, oncology, geriatrics, and traditional Chinese medicine departments. After the interviews, domains and items of the PCC questionnaire were confirmed, and opinions of the three key participants in medical service were included in the questionnaire. Finally, expert consultation was conducted to ensure the content and face validity of the questionnaire.
The Seven Domains of the Patient-Centered Care Questionnaire and Their Definitions.

Data Collection
To ensure a consistent level of quality regarding data collection, an investigation team comprising six recruited research assistants was formed to conduct the fieldwork for the face-to-face inpatient survey. All the field-investigation team members were provided prior specialized training in administering the questionnaires and communicating with patients. The investigators, assisted by local medical professionals, visited the wards of the target hospitals and distributed paper-based questionnaires to inpatients. Participants were asked to rate the items based on their own experience of medical service access. The investigators assured inpatients that the questionnaire would not have any impact on their use of medical services. All participants provided verbal informed consent prior to participation. This study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Ethics Committee.
Statistical Analysis
Descriptive statistics, analysis of variance (ANOVA), and linear regression models were employed to analyze the data. We described inpatients’ sociodemographic characteristics using counts and proportions. Different groups were created based on sociodemographic information, and PCC scores were calculated for each group. The scores for different groups were compared using an ANOVA test. Multivariable regression models were then used to explore the influence of sociodemographic characteristics on PCC and its seven domains.
For the grouping of sociodemographic characteristics, we adopted both common and official grouping methods. For example, groups of economic regions were determined using the official Guangdong Statistical Yearbook. “Hukou” referred to whether the respondents’ permanent address was in a rural or urban area. Medical insurance was divided into 4 groups: (1) medical insurance for urban employees (public medical insurance for people living in urban areas and employed by companies or organizations); (2) medical insurance for urban residents (public medical insurance for people living in urban areas and not employed by any company or organization); (3) people covered by the New Rural Cooperative Medical System (NCMS); and (4) other (people with no public medical insurance). We divided income level into three groups: “average” represented the middle-income range defined in the 2019 Guangdong Statistical Yearbook; “below average” represented incomes below this range; and “above average” represented incomes above this range. SPSS software was used to perform the data analyses, and P-values less than .05 were considered to indicate significance.
Results
A total of 2028 inpatients completed the questionnaire. Of these, responses from 165 were excluded because of missing information regarding sociodemographic characteristics or items from the PCC questionnaire. Consequently, 1863 valid questionnaires were included in the analysis. Of these 1863 valid responses, 1,066, 434, 151, and 212 were collected from the PRD, eastern, western, and northern areas of GD, respectively. All of these exceeded the respective minimum sample sizes for the regions and were consistent with the proportion of permanent resident populations in each region.
Sociodemographic Characteristics of the Respondents and Comparison of Mean PCC Scores.

aHukou: Location of the respondent’s permanent residence.
bRegion: The method for distinguishing the economic regions in Guangdong Province was based on the official approach applied in the Guangdong Statistical Yearbook. The ranking of the regions in terms of per capita gross domestic product is Pearl River Delta (PRD)>western>eastern>northern.
cMedical insurance: (1) Public insurance for urban employee: people living in urban areas who are employed by companies or organizations; (2) Public insurance for urban resident: people living in urban areas who are not employed by any company or organization; (3) NCMS: people covered by the New Rural Cooperative Medical System; (4) other: people with no public medical insurance.
dIncome level: “Average” represents the middle-income range of residents as defined by the “2019 Guangdong Statistical Yearbook.” “Below average” indicates incomes below this range, and “above average” indicates incomes higher than this range.
PCC: patient-centered care; SD: standard deviation.
The overall mean PCC score was 8.58 (standard deviation = 1.36). Significant differences in scores were found between the economic regions and based on the number of hospitalizations (P < .05). Comparisons using the least-significant difference revealed that the overall PCC scores for PRD and eastern GD were higher than those of western and northern GD (P < .05). Moreover, inpatients with more than 3 hospitalizations scored higher than those with 2 or 3 hospitalizations and first-time inpatients (P < .05).
Scores for the 25 Individual Items of the PCC Questionnaire.
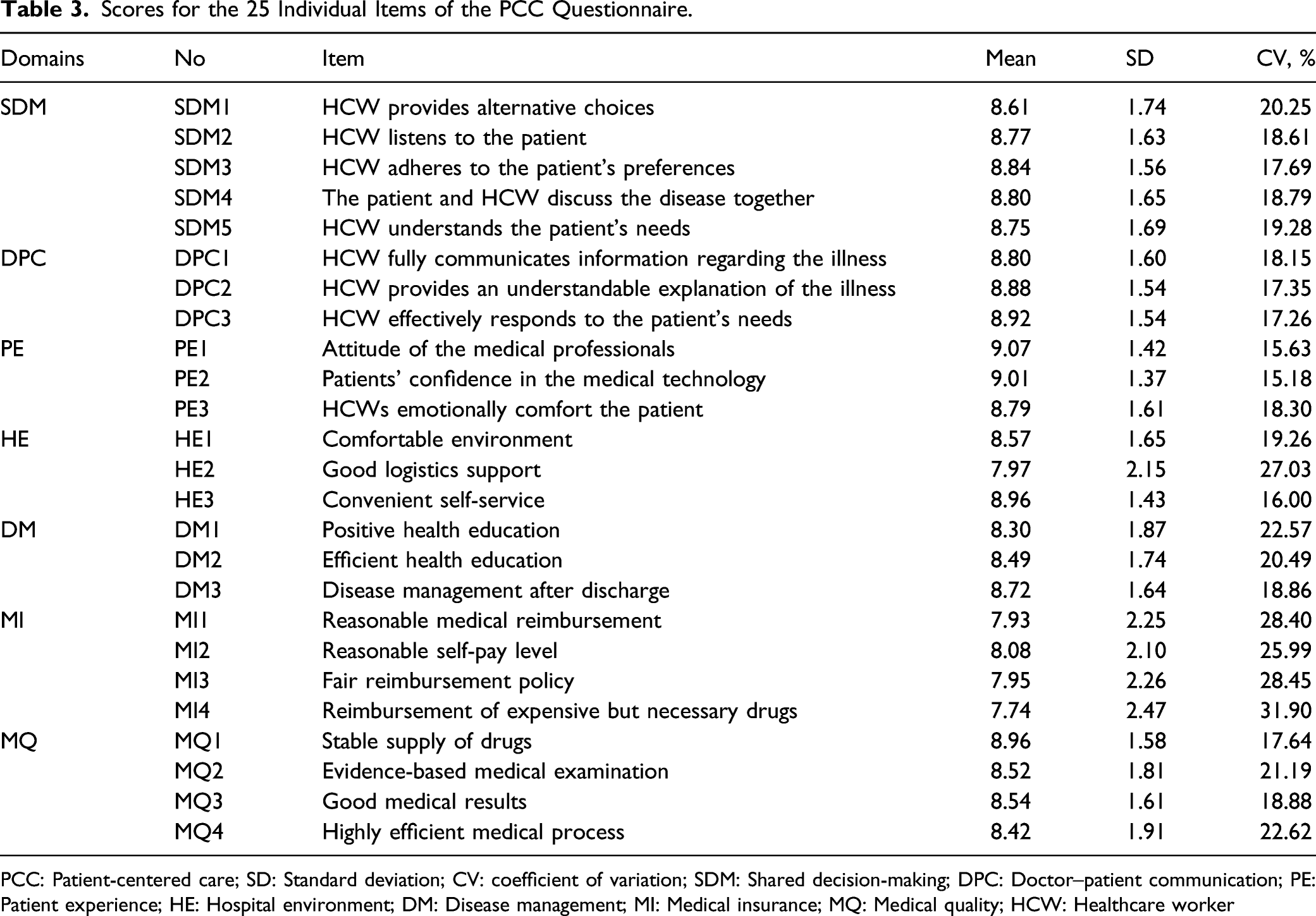
PCC: Patient-centered care; SD: Standard deviation; CV: coefficient of variation; SDM: Shared decision-making; DPC: Doctor–patient communication; PE: Patient experience; HE: Hospital environment; DM: Disease management; MI: Medical insurance; MQ: Medical quality; HCW: Healthcare worker
Overall PCC Score and Scores for its Seven Domains.

The maximum score for each domain was 10. PCC: Patient-centered care; SD: Standard deviation; CV: Coefficient of variation; SDM: Shared decision-making; DPC: Doctor–patient communication; PE: Patient experience; HE: Hospital environment; DM: Disease management; MI: Medical insurance; MQ: Medical quality
Sociodemographic Characteristics Associated With Mean Scores for PCC and its Domains.
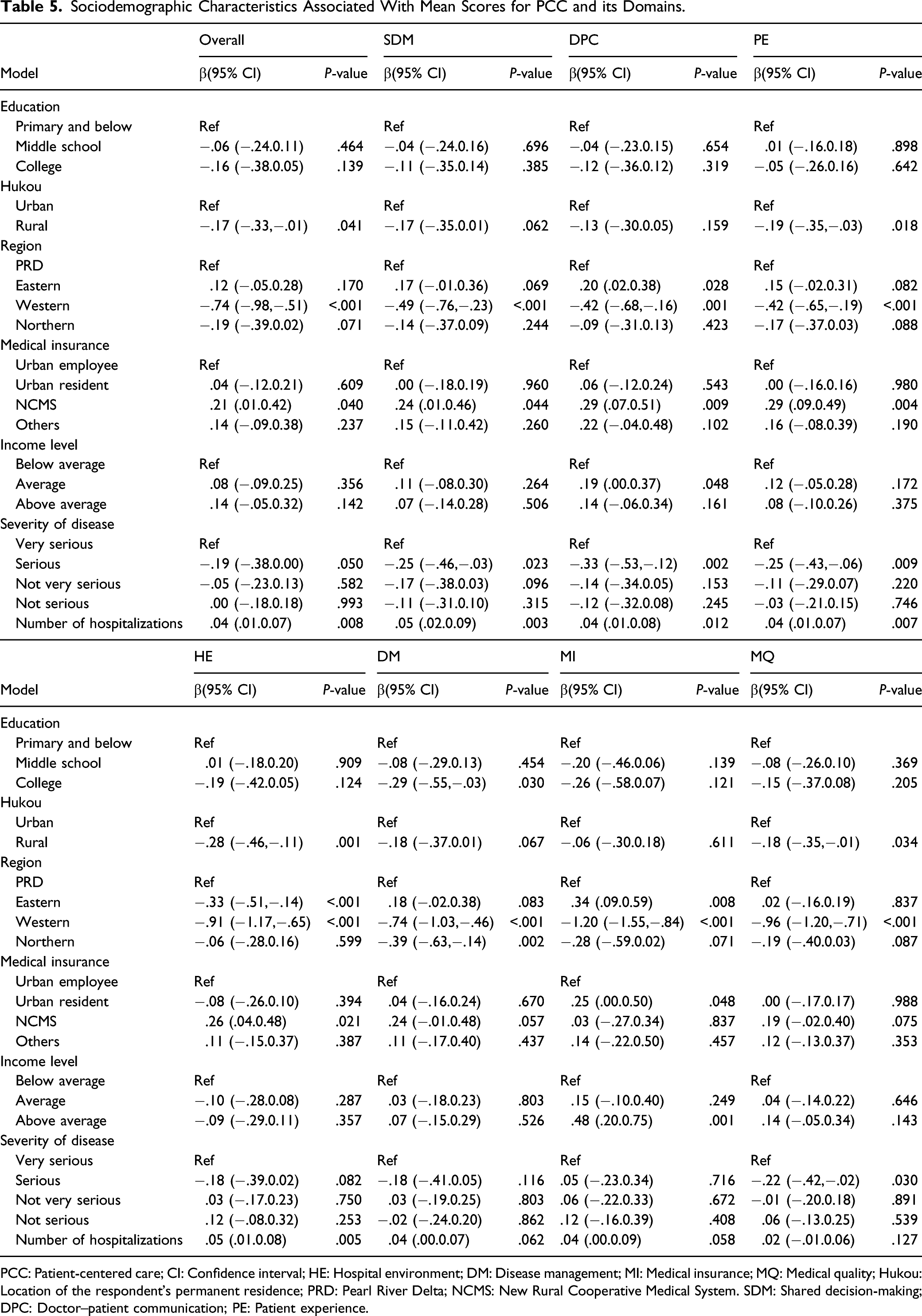
PCC: Patient-centered care; CI: Confidence interval; HE: Hospital environment; DM: Disease management; MI: Medical insurance; MQ: Medical quality; Hukou: Location of the respondent’s permanent residence; PRD: Pearl River Delta; NCMS: New Rural Cooperative Medical System. SDM: Shared decision-making; DPC: Doctor–patient communication; PE: Patient experience.
Discussion
This study was the first to provide insights into the perceived levels of PCC among inpatients in China. In general, we found that inpatients reported high satisfaction with PCC during their hospitalization. To make medical services more patient-friendly in recent years, the Chinese government developed ambitious programs, such as the “Action Plan for Further Improvement of Health Services 2018–2020” 31 As a result, hospitals in GD have made great efforts to provide high-quality medical services to improve patients’ experiences of using public healthcare services. Our study was the first to assess the efficiency and effectiveness of these policies and confirmed that the quality of medical services has improved inpatients’ perception of PCC considerably.
Among the domains of the PCC questionnaire, the medical insurance domain was rated the lowest by the inpatients in this study. This suggests that, even though satisfaction improved, inpatients still experienced issues related to certain basic components of the healthcare system, such as unfair reimbursement policies from public medical insurance systems and limited breadth and depth of reimbursement. 32 For example, some frequently used drugs were not covered by the medical insurance, and the reimbursement rate of some expensive drugs was also very low. 33 This dissatisfaction with medical insurance indicates that inpatients' perceived disease burden requires further improvement.
Inpatients, who came from western GD, an economically developed region, reported a lower PCC level of than those from eastern GD, which is an economically under-developed region. As such, economic development levels may not be the primary factor affecting inpatients’ perception of PCC, but rather the relative extent of government investment in the medical system and the patients’ perceived level of medical technology. 34 To address this, the relative extent of government investment in hospitals to improve the medical system plays a key role in the improvement of inpatients' perception of PCC. Furthermore, this study found that the higher the number of hospitalizations experienced by patients, the higher their PCC scores. There is no research on the relationship between number of hospitalizations and patients’ PCC scores; this may be because patients reporting more hospitalizations show greater understanding and tolerance to medical staff. However, the specific reasons need to be confirmed by further empirical studies.
This study found that inpatients from rural areas got a lower PCC mean score compared with those from urban areas. Although the China General Office of the State Council issued guidelines on promoting the development of a hierarchical medical system in 2015, 35 in this study, 51.02% (n = 476) of the rural inpatients who rated their health status as “not very serious” also reported visiting tertiary-level hospitals. The main reasons for this phenomenon may be the low quality of and patients distrust in doctors' skills at rural healthcare facilities, which led to wastage of time, and higher costs.36,37 Therefore, additional resources need to be invested to improve the doctors’ skills in rural medical institutions. Conversely, inpatients covered by the NCMS scored PCC higher than those covered by the public medical insurance for urban employees. However, rural patients can only avail the NCMS, which covers permanent rural residents, and its overall financing and reimbursement levels are lower than those covered by public urban medical insurance. This unusual finding indicates two things. First, in recent years, GD has invested considerable resources into improving its primary healthcare system, especially in rural areas. 38 Nevertheless, compared to urban patients, lower overall PCC scores indicated that rural inpatients have greater dissatisfaction with medical services. Second, compared to the medical insurance schemes for urban patients, in recent years, the Chinese government has increased the reimbursement rate for patients who are covered by the NCMS 39 ; thus, rural residents’ disease burden has been significantly reduced. 40 This key development strategy has greatly improved rural patients’ expectations, as stated by most participants in our study, who reported that they can access medical services more conveniently and at affordable rates.
In this study, a self-developed questionnaire was used to measure the PCC, which provided empirical evidence to assess the quality of healthcare services from Chinese patients’ perspective. As we know, currently, there is no instrument that assesses PCC, developed for the Chinese context.35,41 All the existing PCC-related instruments have been developed in the context of Western healthcare systems; their validity and reliability have never been assessed in the Chinese population, and thus, their findings may not be generalizable to the Chinese context. In this study, the PCC questionnaire was developed based on a rigid process in the context of GD, one of the most populous regions in China, while also considering the socioeconomic disparities within the province. More importantly, this study directly investigated the patients’ perspective on PCC’ thus, providing novel insights for future PCC studies and enriching the existing knowledge on PCC in China. However, despite the psychometric properties of the questionnaire being satisfactory, its performance needs further assessment in the other regions of the country.
Despite these significant contributions, several limitations need to be addressed. First, this was a cross-sectional study; thus, no causal relationships between sociodemographic characteristics and PCC could be established. In future studies, longitudinal data should be collected and analyzed. Second, items and mean scores showed ceiling effects to some extent, which is a common problem in patient experience and outcome measures. Some inpatients in this study may not have been completely convinced by our repeated assurances that their responses to the survey will not affect their access to medical services; thus, it is possible that some participants may have scored some items too high. In the future, researchers should take effective steps to control the ceiling effect of patient scores. Third, inpatients living in rural areas tended to report a poor PCC; however, since all the inpatients investigated in this study were selected from hospitals in big cities, their ratings may be less comprehensive in terms of the primary healthcare system. Therefore, further research should be conducted in primary healthcare institutions.
Conclusion
This study provided a comprehensive overview of inpatients' perceptions of PCC in tertiary-level hospitals in GD, China, and found that inpatients reported high satisfaction with PCC during their hospitalization. Inpatients from rural areas perceived a lower level of PCC compared to those from urban areas, whereas inpatients covered under the NCMS reported higher PCC score than those under the public medical insurance for urban employees. Moreover, inpatients in western GD reported a lower PCC score than those in eastern GD. Heterogeneity in PCC between different sociodemographic status groups indicates that, despite a high level of PCC reported by inpatients in this study, some fundamental issues regarding PCC are need to be improved.
Footnotes
Author Contributions
Conceptualization: DW; Methodology: LZ and RX; data collection: LZ, YX, and JC; statistical analysis: LZ; Writing—Review and Editing: LZ and RX. All authors have read and agreed to the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the “Guangdong Basic and Applied Basic Research Foundation (2021A1515011973); a grant from Philosophy and Social Sciences of Guangdong College for the project of “Public Health Policy Research and Evaluation” Key Laboratory (2015WSYS0010), The Natural Science Foundation of Guangdong Province, and Public Health Service System Construction Research Foundation of Guangzhou, China.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Second Affiliated Hospital of Guangzhou Medical University (Project identification code: 2019-ks-28).
Data Availability
The data might be achieved by contacting the correspondence author.
Appendix
Reliability Test of the PCC Questionnaire and its Seven Domains

| Domains | PCC | DPC | SDM | PE | HE | DM | MI | MQ |
|---|---|---|---|---|---|---|---|---|
| Value of Cronbach’s α | .971 | .941 | .956 | .895 | .800 | .928 | .924 | .845 |
PCC: Patient-centered care; DPC: Doctor–patient communication; SDM: Shared decision-making PE: Patient experience; HE: Hospital environment; DM: Disease management; MI: Medical insurance; MQ: Medical quality.