
Abstract
BACKGROUND:
The practice environment influences the quality of care and the nursing outcomes achieved in their workplaces.
AIMS:
To examine the perception of the clinical practice environment among nurses working in mental health units in the context of their participation in an action research study aimed at improving the nurse–patient relationship.
METHOD:
An explanatory sequential mixed methods study was designed. The data were collected in three phases in 18 mental health units (n = 95 nurses). Quantitative data were collected through the Practice Environment Scale of the Nursing Work Index, and qualitative data were collected through reflective diaries and focus groups in the context of participatory action research.
RESULTS:
The nurses’ assessment of their practice environment shifted from positive to negative. Nurse manager leadership was the aspect that worsened the most. In addition, the perception of their participation in the affairs of the center and nursing foundations for quality of care decreased. The nurses considered it essential to be able to influence decision-making bodies and that the institution should promote a model of care that upholds the therapeutic relationship in actual clinical practice.
CONCLUSIONS:
Nurses perceived that they should be involved in organizational decisions and required more presence and understanding from managers. Furthermore, nurses stated that institutions should promote nursing foundations for quality of care. This study contributes to understanding how nurses in mental health units perceive their work environment and how it affects the improvement of the nurse–patient relationship in clinical practice.
Introduction
The practice environment is a key element that influences the quality of nursing care, job satisfaction and the retention of nurses in health services (Oshodi et al., 2017; Roche et al., 2016). From a theoretical perspective, it was Kanter (1993) who, in his theory of structural empowerment, argued that conditions in the work environment such as access to information and resources, support from managers and opportunities to learn and develop were necessary for the proper development of employees’ work (Kanter, 1993). In addition, other authors have also conceptualized the “working environment” as “the organizational characteristics of a work setting that facilitate or constrain professional nursing practice” (Lake, 2002, p. 178). Thus, the practice environment involves factors such as leadership, teamwork, control and autonomy in clinical practice, conflict management, professional relationships, patient communication, work motivation, and cultural awareness (Erickson et al., 2009). All of these can facilitate or constrain nursing practice (Lake, 2002). Consequently, bearing in mind that these factors are modifiable in work environments (Lake & Friese, 2006), it is important to identify them in specific contexts, such as acute mental health units, in order to improve the clinical practice of nurses.
The working environment is a major determining factor for improving the quality of patient care, while improving outcomes for nurses (Aiken et al., 2011). In this regard, positive work environments are associated with a number of patient outcomes, including greater satisfaction (Aiken et al., 2012), improved quality of care (Aiken et al., 2011) and a lower rate of adverse events (Copanitsanou et al., 2017). Indeed, even at the primary care level, the nursing practice environment has been observed to affect the quality of chronic disease care (Poghosyan et al., 2018). Conversely, unfavorable working environments have been associated with higher readmissions, higher health care costs and associated complications (Copanitsanou et al., 2017).
In relation to the impact of the clinical environment on nurses, it is known that positive work environments contribute to greater job satisfaction (Lin et al., 2020) and lower burnout among professionals (Nantsupawat et al., 2017). In general, studies indicate that nurses perceive most aspects of their practice environment positively (Al-Maaitah et al., 2018; Dorigan & de Brito Guirardello, 2017; Numminen et al., 2016). Specifically, nurses tend to report positive perceptions of team relationships with physicians (Al-Maaitah et al., 2018; Numminen et al., 2016) and, conversely, less positive perceptions tend to be related to staffing and adequacy of resources (Al-Maaitah et al., 2018; Nantsupawat et al., 2017; Numminen et al., 2016). In fact, nurses’ positive perceptions of their practice environment are also known to be associated with increased professional competence (Numminen et al., 2016), an increased perception of the quality of care (Al-Maaitah et al., 2018; Numminen et al., 2016), greater job satisfaction (Lin et al., 2020; Nantsupawat et al., 2017) and a reduced intention to leave the job or profession (Nantsupawat et al., 2016; Numminen et al., 2016). In fact, nurses describe a more positive perception of the quality of nursing care perceived by their patients when the practice environment is healthy (Numminen et al., 2016; Roche et al., 2016). Thus, nurses believe that the role of nurse leaders is fundamental to the establishment and improvement of a healthy work environment (Ducharme et al., 2017; Numminen et al., 2016).
Specifically, in the field of mental health units, where the therapeutic nurse-patient relationship is key for the provision of care (Moreno-Poyato et al., 2016; Zugai et al., 2015), understanding that the creation of protected and therapeutic spaces is of particular importance (McAllister et al., 2019; Molin et al., 2019; Moreno-Poyato, El Abidi, et al., 2021). In fact, it has been shown that the nurses’ perception of a better practice environment is related to the establishment of a higher quality nurse–patient relationship (Roviralta-Vilella et al., 2019). However, some studies indicate that mental health nurses perceive their practice environment more negatively compared with other settings (Roche & Duffield, 2010). It has even been observed that mental health nurses who use more restrictive measures with patients are less satisfied with their jobs (Kurjenluoma et al., 2017). In fact, mental health nurses’ job satisfaction is related to how they perceive their work environment (Gillet et al., 2019). In addition, they experience higher levels of emotional exhaustion when they perceive their practice environment to be worse (Gabrielsson et al., 2016; Gillet et al., 2019; Wyder et al., 2017).
Consequently, the available evidence shows that positive work environments improve the quality of care, nurses’ job satisfaction, and the quality of their work (Kurjenluoma et al., 2017; Wyder et al., 2017), as well as nurses’ work commitment and outcomes in their workplaces (Huang et al., 2021). However, there is limited knowledge regarding the influence of the environment on the design and improvement of practice in the field of mental health inpatient units (Moreno-Poyato, Roviralta-Vilella, et al., 2021). Based on the knowledge that certain environmental factors are modifiable (Lake & Friese, 2006), further exploration of the involvement of the environment in the clinical practice of nurses in acute mental health units is warranted. In this sense, an approach from a global perspective is important to obtain a better understanding of the phenomenon of nurses’ perceptions and perspectives.
The aim of this study was to examine the perception of the clinical practice environment among nurses in mental health units in the context of their participation in an action research study aimed at improving the nurse–patient relationship.
Method
Design
This study was conducted following an explanatory sequential mixed methods design with the intention of obtaining complementary views on the same phenomenon and integrating quantitative and qualitative components to form inferences and conclusions (Tashakkori & Teddlie, 2008; Teddlie & Tashakkori, 2012). This study is part of a project with the main aim of improving the clinical practice of the nurse–patient relationship in mental health units in Catalonia (Spain). This study was divided into three phases, with quantitative data collected in the first and third phases. In the second phase, qualitative data were collected using the participatory action research (PAR) method, following the model by Kemmis and Mctaggart (2008) (Figure 1). To this end, a two-cycle process was designed, consisting of four stages in each cycle. The PAR method is based on the notion that participants’ actions must be filtered through experience and reflection before their practice can be improved or changed. Thus, PAR is performed by following a sequence of stages comprising a spiral of self-reflective cycles (Kemmis & Mctaggart, 2008): planning the desired change, action, and observation of the process and consequences of change, reflection on these processes and their consequences, re-planning the change, action and reobservation and further reflection. During this process, participants are asked to act and reflect, in order to simultaneously gain awareness of and transform their practice (Baum et al., 2006). This study adheres to the GRAMMS guidelines for reporting mixed methods research.
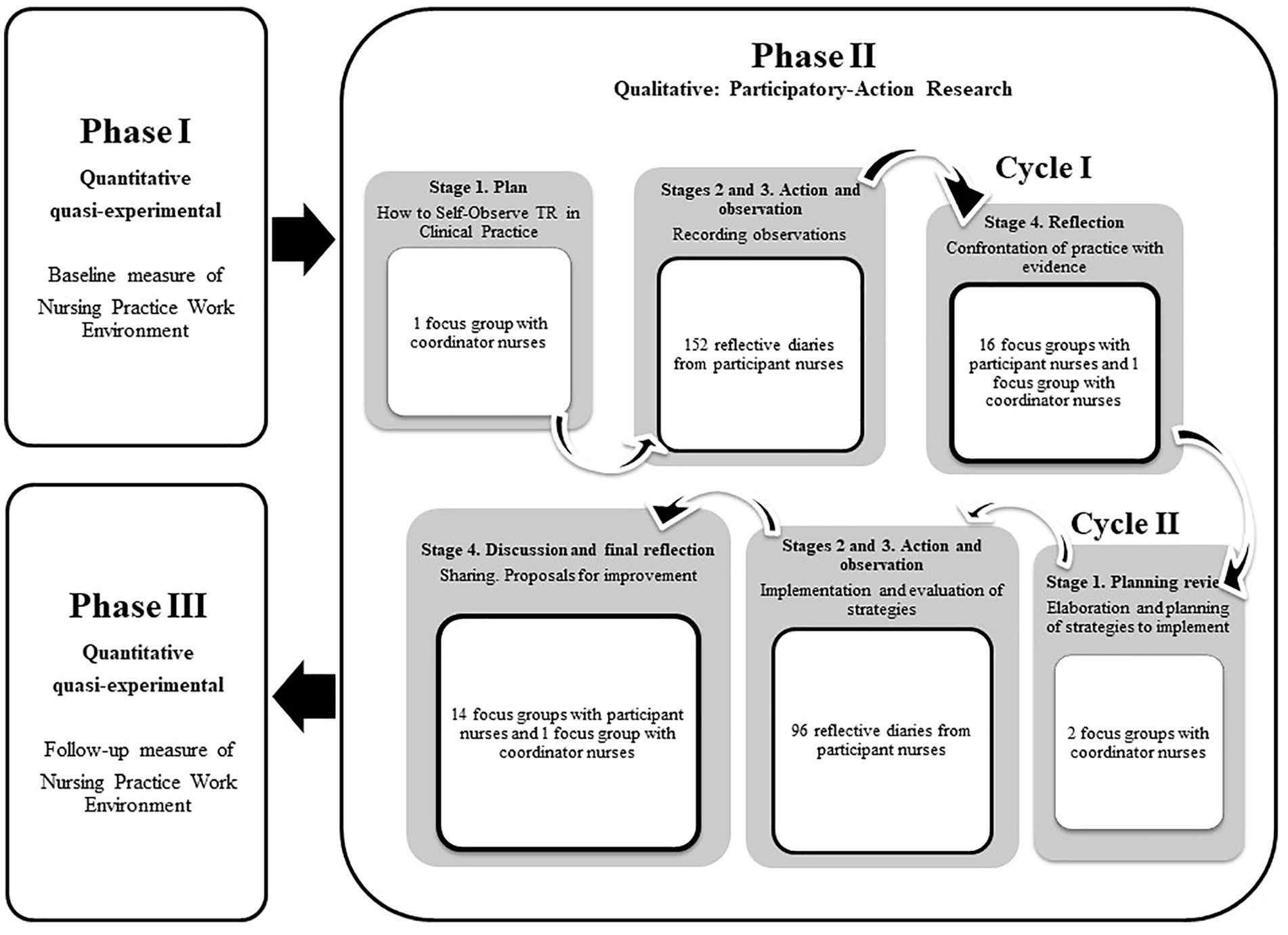
Mixed methods design.
Sample/Participants
All nurses (n = 235) in the 21 acute units of the Catalan Mental Health Network were invited to participate in the study. Only resident nurses in training were excluded. Within each unit, a nurse coordinated the study and oversaw the recruitment process. A total of 198 nurses from 18 acute care units initially participated in the study. Of these, 95 completed all three phases. For the quantitative aspect, the power of the study was calculated to detect a correlation coefficient of at least 0.3 at baseline and follow-up measurements with an alpha of .05, which was 80% in a bilateral contrast.
Data Collection
The nurse coordinators of each unit were responsible for collecting informed consent documents and nurses’ email addresses, and the principal investigator provided an individual confidential participant code to each nurse. Data collection for study Phases I and III took place between January 2018 and June 2019, whereas qualitative data were collected in Phase II, between April 2018 and November 2018.
Quantitative Data
Quantitative data collection for both Phase I and Phase III was conducted via an electronic form sent by email to the participants. This form comprised a questionnaire which gathered nurses’ sociodemographic and professional data, together with the Practice Environment Scale of the Nursing Work Index (PES-NWI; Lake 2002), which was the instrument used to measure the perceived nursing practice environment. This instrument consists of 31 items assessed on a Likert-type scale ranging from 1 to 4 points (1 = strongly disagree, 4 = strongly agree). Values above 2.5 indicate higher agreement, whereas values below 2.5 indicate disagreement. These items are grouped into five subscales: (1) Nurse participation in hospital affairs; (2) Nursing foundations for quality of care, which emphasizes the nursing principles for high quality patient care; (3) Nurse manager ability, leadership, and support for nurses; (4) Staffing and resource adequacy; and (5) Collegial nurse-physician relationships. The PES-NWI has been validated in the Spanish population by de Pedro-Gómez et al. (2009). In the case of our sample, the internal consistency obtained as Cronbach’s alpha values ranged from .77 to .92 for the five factors that constitute the scale.
Qualitative Data
Qualitative data were collected as the PAR was being carried out through reflective diaries and focus groups. Specifically, the qualitative data came from 248 reflective diaries collected at the different stages of action and observation and 30 focus groups that took place during the reflective stages of the PAR (Figure 1).
In relation to the reflective diaries, in order to further structure the reflection and its recording (Bolg et al., 2020), the research team sent a self-observation guide by email to each nurse, indicating how they were to record the self-observation data. The diary was to contain a description and reflection on the types of interactions to be self-observed in practice. As its purpose was to monitor the process of change triggered by the PAR, for each interaction, the nurses were to record the description of the situation, the type of verbal and nonverbal language they had used, their reflective intervention and a reflection on the influence of the environment on the interaction and how they had felt in the context of the interaction (Kemmis & Mctaggart, 2008).
The focus groups were conducted with the participating nurses from each unit and were led by the first author, a mental health nurse specialist (ARMP), with the collaboration of an observer, the second author (DTM) or the third author (FGP), depending on the unit where the group was held. The groups were conducted in a space set up in each participating center. The focus groups were audio recorded and lasted between 1 and 2 hours. At the beginning of each session, participants were provided with a working document containing the preliminary results obtained from the reflective diaries corresponding to the previous stage of the PAR.
Ethical Considerations
The study was approved by the referring ethical committees of the 18 participating units. Nurses signed the informed consent for participation. All data were collected in accordance with national and international privacy and confidentiality guidelines.
Data Analysis
The quantitative data were analyzed using SPSS version 27. Descriptive data are presented as the mean and standard deviation (SD) for continuous outcomes and number and percentage (%) for categorical outcomes. The paired Student’s t test was used to compare the PES-NWI between baseline and follow-up. Statistical significance was set at p < .05.
The qualitative data were analyzed using NVivo version 12. The data were analyzed using thematic content analysis (Crowe et al., 2015). During an initial stage, the text obtained was fragmented into descriptive codes assigned according to their semantic content. In the second stage, these codes were grouped into more analytical subthemes, by classifying the codes according to the meaning of the linguistic units and their combinations. Finally, during a third hierarchical stage, the semantic analysis of the previous subthemes was considered, and the codes were classified deductively according to the dimensions of the PES-NWI.
Rigor
It should be noted that reflexivity was continuous throughout the study process. The research team included both researchers with academic backgrounds and others involved in clinical practice. Therefore, this enabled a reflective and equidistant position throughout the processes of data collection and analysis. The groups were led by the first author, who had qualitative doctoral training and experience as a nurse in acute units, although without any employment relationship with the mental health services. This facilitated the creation of a peer relationship with the participants, and an atmosphere of trust. The credibility and confirmability of the data is supported by the triangulation of techniques and of the researchers in the analysis process, together with the constant auditing of the results by the participants throughout the qualitative process.
Results
Description of the Sample
The study was completed by 95 nurses aged between 22 and 62 years with a mean age of 33.4 years (SD = 9.3). Almost 70 % of the nurses were female. Their experience in mental health was 7.7 years on average (SD = 8.0). Only 23.2 % of the nurses had the official title of specialist in mental health nursing and only 22 % of the nurses had a PhD or master’s degree. Up to 80 % of the nurses had a permanent employment contract. All working shifts of the centers were equally represented in the sample.
Nurses’ Perceptions About the Clinical Practice Work Environment
As shown in Figure 2 and Table 1, the nurses’ overall assessment of the practice environment worsened significantly after the participatory process. In this regard, the scores on 4 of the 5 dimensions of the scale decreased significantly. It should be noted that, prior to the participatory process, the nurses positively scored the overall practice environment and all its dimensions, except for the adequacy of resources and staffing, which was the only item scored below neutral. However, at the end of the process, both the overall assessment of the practice environment and most of the dimensions were rated negatively.
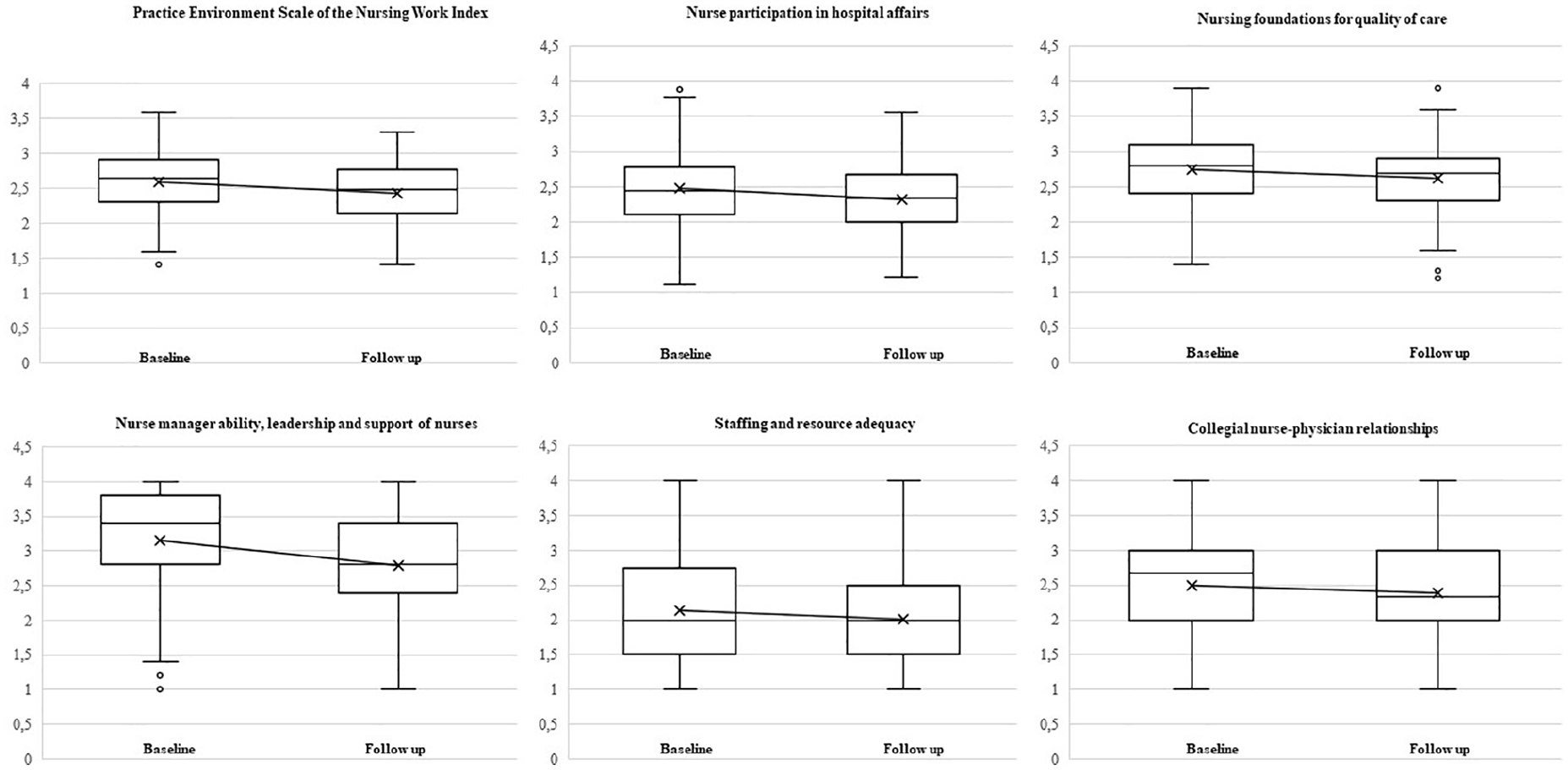
Differences in scores of the Practice Environment Scale of the Nursing Work Index.
Differences in Scores for Items on the PES-NWI.
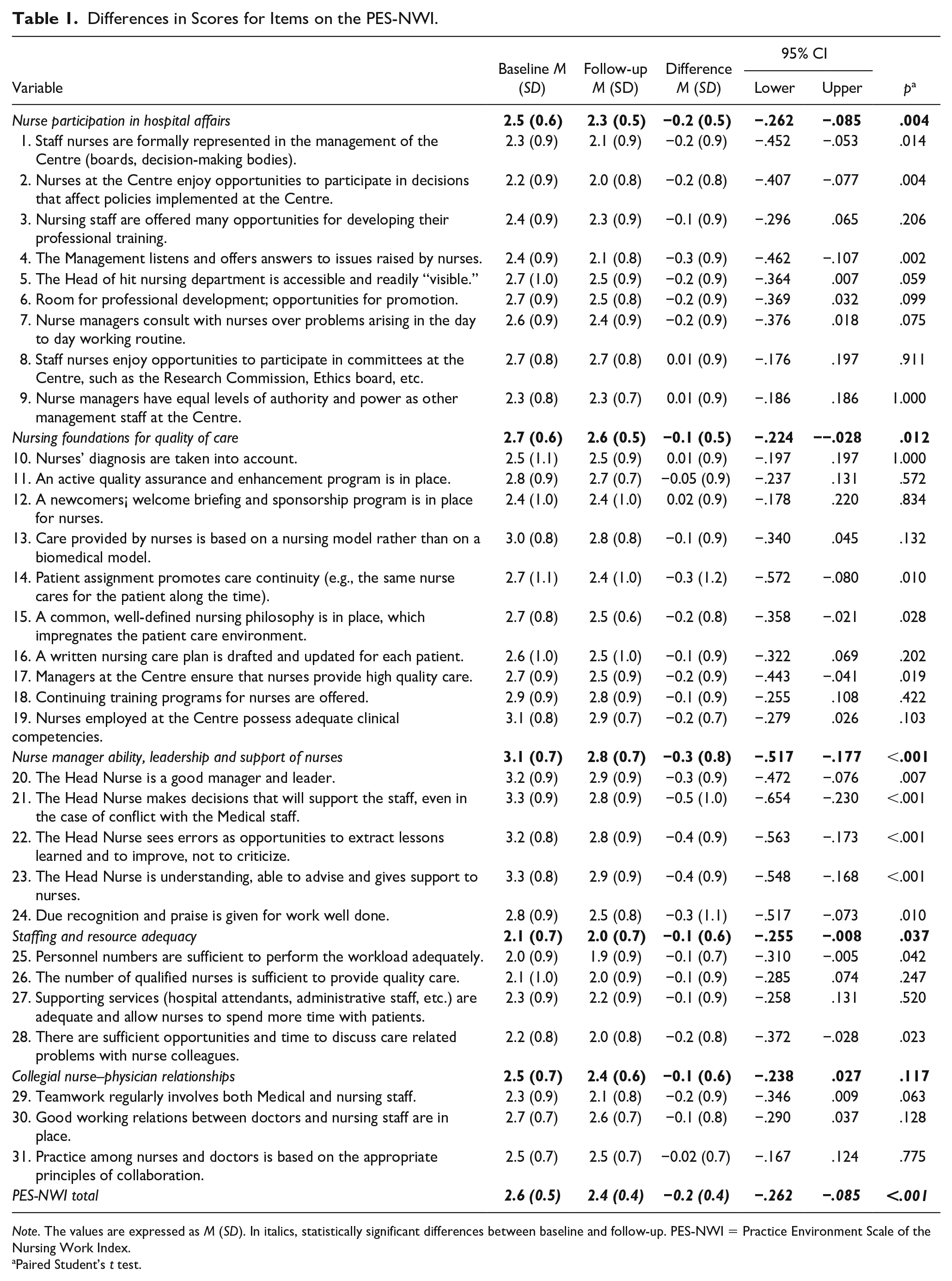
Note. The values are expressed as M (SD). In italics, statistically significant differences between baseline and follow-up. PES-NWI = Practice Environment Scale of the Nursing Work Index.
Paired Student’s t test.
Nurse Participation in Hospital Affairs
Nurses scored this dimension significantly lower following their participation in the process of change. Specifically, the items that decreased significantly were related to nurses’ perceptions of being involved in management and feeling listened to by management, where the lowest rated item was having opportunities in decision-making bodies (Table 1). Although no changes were noted, one of the items that received the lowest scores in both the baseline and follow-up measures was the perception that the nurse managers had equal levels of authority and power as other management staff at the center. In this sense, it was important for the nurses to feel the support of the organization, not only through the resources provided to them but also in terms of their ability to influence structural changes or plan certain actions aimed at improving their interventions and the therapeutic relationship.
. . . if there is a proposal that we jointly see that it would be better for it to be done differently, then you can explain it and they say go ahead, we’ll do it and we’ll try it . . . I don’t know . . . having this amount of ease to be able to change things. (12FG4P02)
However, the nurses questioned the management of the nursing directors. They felt that they did not defend the role of nurses and did not strive to give nurses their rightful place at the institutional level. Likewise, the nurses perceived that the managers did not give them the opportunity to raise the problems that the nurses faced in their daily work, even though they were the professionals who were present at all hours of the day and those who accompanied the people admitted to the acute units.
There are many things for which nurses should be consulted more, because in the end we nurses are the ones who are there the most. On Saturdays and Sundays, you spend all your time with patients and there are no doctors anywhere, so in the end they should consider nurses’ opinions more. (12FG4P04)
Nursing Foundations for Quality of Care
The score given by the nurses to this dimension was also significantly lower after the participatory process. For the participants, the type of allocation of patients to individual nurses in the centers, the existence of a common nursing philosophy and the concern on behalf of managers that nurses provide quality care were the items that significantly decreased (Table 1). However, although unchanged, the lowest rated item in this dimension was the existence of a welcome and mentoring program for new nurses. For the nurses, the position and discourse of their institutions regarding the therapeutic relationship was highly ambiguous. They indicated that their institutions did not have a clear philosophical model that defended the therapeutic relationship, stating that the nursing staff did not prioritize this in their day-to-day work either and that ultimately, what they prioritized were instrumental tasks, rather than relational ones.
The therapeutic relationship is not strengthened, when there is no technique involved, or there is no specific need, it is not strengthened by the institution. This is why some of the staff spend a lot of time on administrative tasks instead of spending time at the bedside. (12RD2P06)
Moreover, the nurses recognized specific training limitations in mental health, due to the difficulty of adapting the theoretical content on which the TR is based to the reality experienced in the acute units, generating insecurity in their approaches.
Although the therapeutic relationship is highly valued, I miss refresher training courses on the therapeutic relationship. (03RD2P09)
In addition, the nurses expressed their discomfort at the overload of having to supervise or redirect the actions of the new professionals, as they were sent to work in units they were unfamiliar with, without having prior information about the unit or sufficient knowledge to work in these environments.
. . . personally, at this moment, due to my lack of experience, I feel that I still lack the resources, training and experience to resolve these situations better (10RD2P11) . . . yes, because normally, we are very busy, because with someone who has no experience, you have to explain how to do things and at the same time you have to be with this patient who is pre-agitating . . . (15FG4P01)
Nurse Manager Ability, Leadership, and Support of Nurses
This dimension, despite continuing to be the most highly rated by the nurses after the participatory process, was the one that decreased the most. As shown in Table 1, the scores for all the items that conform to the dimension decreased significantly, with the item with the lowest score being the recognition and praise of work well done by managers. The nurses expected their managers to be motivated and present in the unit for them to understand and be involved in what was happening on a day-to-day basis. However, they questioned the role of the managers, as they considered them to be absent figures, who did not defend the interests of the service, the people admitted, or the nursing staff themselves.
Involvement is important, he should spend more time with us, he should ask how it’s going, he should be involved, obviously. But I think it should be important for a supervisor to spend x hours on a shift, to see how it’s going . . . (10FG4P02)
Staffing and Resource Adequacy
This dimension received the worst rating by the nurses at both baseline and follow-up and decreased significantly after the participatory process. Specifically, the items that worsened significantly were adequacy of staffing and time to discuss care-related problems with other nurse colleagues (Table 1). In this regard, nurses reported that lack of human resources was one of the greatest and most important constraints they had to face. This severely limited the type, quality, and quantity of interactions that nurses were able to have with the people they cared for. The lack of adequate ratios for the needs of the unit generated an overload and a risk, which affected the safety of the users, and that of the staff themselves. This often meant that many of the interactions they carried out were more extensive with those users who were more demanding or who presented more behavioral alterations, to the detriment of those who were isolated or who did not make explicit demands and who might need it just as much as the other more demanding people.
In the end, when you are saturated with work, you dedicate yourself to the most behavioural things and the person who is very sick . . . who is in his own world, but is calm, on the medical record you may state that he is calm when you haven’t even seen him . . . he is still a sick person, a sick person who is suffering. I don’t know how this can be solved! (12FG4P05)
Moreover, the nurses stated that time was one of the most important and most necessary factors for the development of the TR, yet it lacked the most during their working days. The nurses perceived that this lack of time greatly affected the TR, given that not having the time they needed to dedicate to the people they cared for put the quality of the relationship and the care provided at risk.
The lack of time to perform each of the tasks is evident as the ratio of patients per nurse is very high and the distribution of direct interventions with patients is limited. (07RD2P02)
Thus, the nurses identified that this lack of time was also related to factors of the nursing activity itself. Clinical nursing practice involves many activities that are highly varied and with different levels of complexity. Thus, the nurses pointed out that there were some tasks that were fixed and had to be carried out at certain times. Fixed schedules that often marked the tempos of the whole working day and took precedence over any relational activity.
. . . you are not always able to treat patients according to their needs, due to the number of tasks (many of them bureaucratic) that have to be carried out and that take time away from being able to have a deeper interaction with the patient. (03RD2P10).
Collegial Nurse–Physician Relationships
This dimension showed very little change after the nurses’ participatory process, remaining close to a neutral value. The item that decreased the most and was the worst rated by the nurses in this dimension was the perception of performing teamwork with the doctors (Table 1). In this sense, for the nurses it was important to carry out the first assessments together. They felt that it favored the collection of information. They valued and assigned great importance to the cohesion between them, as this was the way to be able to carry out coherent and therapeutic actions.
When new people come, I tell them: see if you can be in the first interview that the psychiatrist does . . . the attitude he has if you are there or not, sometimes you find that they say no, not with this nurse. But the first interview already gives you a lot of information and a relationship with the patient, it’s like a more direct link, he knows that you are his nurse and that you are going to monitor him. etc. (10FG4P01)
However, the nurses expressed difficulties due to a lack of communication and cohesion. For them, this lack of communication ended up affecting the nurse–patient relationship. In this sense, they stated that, at times, the medical teams made decisions without considering the nurses, generating an important loss of professional authority in the eyes of the people they cared for. For them, this loss of authority also occurred when certain members of the medical team undermined their authority in front of the patients or breached the established rules of the unit, putting their relationship with the users at risk. When these actions occurred, they felt a lack of support and professional recognition for the contributions and assessments they made as nurses.
. . . You saw a person smoking twice, you took away his permission to go out and the psychiatrist comes by and says “no, no, he can go out.” Now, excuse me! If there are rules and the nurse has told him that he can’t go out because those are the rules, how can you come up with this now? Are you discrediting us? (12FG4P02)
Discussion
This study aimed to explore the effects on the perception of the practice environment among nurses in mental health units in the context of their participation in a process for improving the nurse–patient relationship. The quantitative results of the study showed a significant worsening of the nurses’ perception of their practice environment. Additionally, the qualitative findings of this study enabled us to identify the most relevant aspects of the environment that affected the nurses in order to establish a better nurse–patient relationship in clinical practice. The first fact that should be highlighted is the general worsening perceived by the nurses in relation to their environment. The nurses shifted from a positive assessment of their environment before starting the action research to a negative perception of the same. This finding can be explained by the nurses’ greater awareness of the importance of the environment in order to establish a quality therapeutic relationship (Roviralta-Vilella et al., 2019). This may have led to nurses acquiring a more critical sense of the context of care through their participation in the action research process (Bush et al., 2018; Salzmann-Erikson, 2017).
More specifically, the dimension that suffered the greatest decrease was that of nurse manager leadership although it continued to be one of the dimensions most highly valued by nurses (Farmakas et al., 2014; Kurjenluoma et al., 2017; Redknap et al., 2016; Roche et al., 2011; Van Bogaert et al., 2013). The nurses pointed out that managers should motivate staff, and should have a presence on the units to understand and advocate for the needs of the team and the patients (Kanter, 1993; Wyder et al., 2017).
However, as in other studies, the lowest rated dimension by nurses was Staffing and resource adequacy (Gabrielsson et al., 2016; Hanrahan & Aiken, 2008; Hanrahan et al., 2010). Although this dimension did not suffer a significant decline in the context of the action research process, as this negative assessment already existed for the nurses, the process served to identify that the lack of resources and time put the quality of the relationship at risk (Kanter, 1993; Moreno-Poyato et al., 2016). In this sense, for nurses, fixed tasks took precedence over any relational activity (Busch et al., 2019), primarily affecting the safety of both patients and staff (Vahidi et al., 2018).
Another notable finding was the worsening of the nurses’ perception of their involvement in the affairs of the center. While it was important for them to be involved in management, to have influence to be able to make changes and to feel heard and supported by management, the nurses stated that the management did not advocate for them or consider them to be able to raise issues or discuss the need for change (Roche et al., 2011; Wyder et al., 2017).
The perception of nursing foundations for quality of care also decreased for the nurses. In this regard, they pointed out that there was no clear philosophical model advocating for the TR in their practice, such as patient allocation per referring nurse, and that this directly affected the fragmentation of care (Busch et al., 2019). In addition, they identified limitations in terms of training and orientation of new staff (Hooper et al., 2016).
Finally, the doctor-nurse relationship did not undergo significant changes. The process allowed the nurses to confirm the importance of cohesion and teamwork between them, as this was the way to be able to carry out coherent and therapeutic actions with the patients (Gabrielsson et al., 2016; Wyder et al., 2017).
Strengths and Limitations
This study has several strengths and limitations. Regarding the limitations, from a quantitative point of view, the single-group design does not allow the effect of the changes to be compared with a control group. Second, it is important to bear in mind the duration of the intervention. This could have influenced the rate of nurse dropout, since there were a significant number of service transfers during the study. Likewise, the changes in the work environment of each unit beyond those produced directly by the intervention should be considered. However, given the purpose of the study, the use of mixed methods enables the ability to complement and gain a deeper understanding of the phenomenon studied by integrating and inferring results. Third, it should be considered that the source of data collection was only from the perspective of the nurses in the units. One of the strengths of the study was the representativeness obtained by the number of units and the number and characteristics of the nurses that participated, which enables these results to be generalized to the Catalan and Spanish context. Finally, regarding future lines of research, the findings suggest the need for more in-depth studies on the factors in the practice environment that influence the quality of the therapeutic relationship. Such studies should address the perspective of the directors and managers of the institutions, as well as research the relationship between the environment and indicators of quality of care and examine the perspective of the patients themselves.
Conclusions
Nurses consider that they are hardly involved in decision-making processes. Furthermore, they require more presence and understanding from managers in order to identify real needs and to participate in decisions and thus improve the day-to-day clinical practice in the units. For them, the practice environment, more specifically, the lack of time and resources, affects their safety and that of their patients and conditions the therapeutic relationship by reducing the quality and quantity of interactions. Finally, nurses consider that the institutions should promote nursing foundations for quality of care, where, for example, priority is given to plans for welcoming the recruitment of new staff and ongoing training on the therapeutic relationship.
By using a mixed approach, this study contributes to a deeper understanding of how nurses in mental health units perceive their work environment and how it affects the improvement of the nurse–patient relationship in clinical practice. Thus, while the quantitative results provide information on the changes in the nurses’ assessment of the environment, the qualitative data shed light on the most important aspects of the environment according to the nurses for the establishment of a quality therapeutic relationship.
Footnotes
Acknowledgements
We would like to acknowledge all the nurse’s participants in the MiRTCIME.CAT project.
Author Roles
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the College of Nurses of Barcelona (PR-218/2017).