
Abstract
This study aimed to investigate the view of prediabetes and prehypertension elderly patients living around temple on long-term self-management in proficient way underneath the lifestyle intervention program based on both focus-group discussion and In-depth interview methods to fill the gap in partially successful intervention. 62 participants were selected from 220 participants of the quantitative published study by 2 researchers. The triangulation method was used to put great emphasis on the consistency and the credibility of the results. Almost all of the participants had benefited from the program regarding proper foods, suitable exercise and an inspiration of lifestyle modification. They made changes of eating behavior and exercise behavior during program attendance, however, after the program had finished, they had minimal concern to take care of themselves. Nonetheless, more than half of them demonstrated some health-related behaviors changes due to they gave the value of the suggestion in different aspects. Moreover, high-frequency program attendance was not related to blood results improvement. The knowledge obtained from program intervention together with adequate contact between the patient and the program staff, personal problems solving, personal attitude, practice and acceptable played a key role for long-term lifestyle modification and completely successful intervention.
Keywords
Lifestyle intervention is viewed as the supporter of lifestyle modification to reduce health-related diseases especially hypertension and diabetes. However, intervention programs are faced with participation diminution due to many reasons which cannot capture the patients’ attention.
This research aimed to investigate the cause of less attention and less practice toward the suggestions from the program and leftover misunderstanding of exact knowledge related to diabetes mellitus, hypertension, and daily physical activity in some group of the participants both during program attendance and after the program had finished.
Inadequate contact between the patient and the program staff, the old beliefs passed down through generations or given by word of mouth, work priorities, habitual behavior, convenience, the family members, health problems, needed friends to join activities are the reason for incompletely successful intervention program which should be utilized as the policy for lifestyle intervention program improvement.
Introduction
“Thailand Healthy Lifestyle Strategic Plan 2011-2020” was constructed from the cooperation of The Office of the National Economic and Social Development Council, The Ministry of Public Health and Mahidol University to handle lifestyle diseases such as diabetes, hypertension, cardiovascular diseases, cerebrovascular diseases and cancers with less expenditure, disability and fatality and to enhance new normal life with wellness and healthiness by focusing on lifestyle modification in every social system includes personal, family, community and country. 1 On the issue of diabetes and hypertension, the campaign “Sugary, high-fat and high sodium content diets reduction, more fruits and vegetables consumption and physical activity promotion” was released. 1 To serve a purpose of this strategic plan, lifestyle intervention among prediabetes and/or prehypertension Thai adults living in community around studied temple was delivered and the results of both short-term and long-term assessments had been published.2,3 The study findings manifested the improvements of systolic blood pressure at 12-month follow-up from baseline with mean (SD) from 126.7 (7.1) mmHg to 123.4 (9.6) mmHg, 2 while fasting blood sugar, systolic blood pressure and total cholesterol improvements were found at 24-month follow-up from baseline with mean (SD) from 97.5 (9.9) mg/dL, 126.7 (7.1) mmHg and 206.1 (35.4) mg/dL to 96.5 (11.6) mg/dL, 124.4 (13.9) mmHg, and 202.0 (33.9) mg/dL respectively. 3
Lifestyle modification is about the change of eating habit and exercise behavior in the long run to heal unsatisfied health condition. Thai people’s lifestyle in semi-urban area such as Nakhon Pathom Province involve with Buddhist Temples which are called “Wat.” Moreover, the lifestyles of Thai older adults living around temple (which can be viewed as the community) are such as they usually have the same temperament, behavior, habits, and lifestyle when living in the same area, they regularly behave themselves follow the belief given by the word of mouth or the belief passed down through their generations, they usually pay less attention to acquire knowledge via the text from internet, books, pamphlets or documents and as well as they need the support from family members and friends to make change or practice beneficial health actions. Each district in this area has a health promoting hospital which the name is frequently the same as District Buddhist Temple. Moreover, in Thailand, health promoting hospitals are classified as primary health care service which act as the first line contact between people living in the community and the essential health service to treat, promote, protect and rehabilitate the health of inhabitants and also act as the venue for patients to group together and engage with self-management behaviors. For these reasons, community-based intervention programs are vital for investigating the actual outcome of lifestyle intervention that can be utilized as the prototype to develop the precise intervention in greater scale. Despite the fact that community-based intervention programs are catered for lifestyle changes, 4 only a few temple-based qualitative research studies were conducted especially topic related to lifestyle intervention owing to lifestyle modification is delicate due to it involves with knowledge, support, motivation, attitudes, behaviors, understanding and real practice, moreover, most of the existing researches associated with diabetes and/or hypertension lifestyle intervention at community-based level in Thailand were quantitative studies2,3,5 -8 in a similar way of worldwide existing researches9 -30 and current lifestyle interventions in Thailand seem less important for people to accept to use in their own lifestyle. For these reasons, hypertension and type 2 diabetes mellitus still spread out among Thai people.31,32 National prevalence of hypertension and diabetes in Thailand increased from 11.0% in 1996 to 22% in 2004 and from 4.6% in 1996 to 6.9% in 2004, respectively. 33 From Thai National Health Examination Survey (NHES) in 2008 to 2009, it was found that, diabetes prevalence in Thai people with aged 15 years and above was 6.9%, moreover, diabetes affected 16.7% of the elderly aged between 60 and 69 years. 34 The prevalence of diabetes and hypertension in Thai adults with aged 15 years and above, rose from 6.9 in 2009 to 8.9 in 2014 and from 21.4 in 2009 to 24.7 in 2014, respectively, while the prevalence of inadequate physical activity (less than 150 minutes per week) among people in the same group rose from 18.5 in 2009 to 19.2 in 2014. 35 Crude mortality rate per 100,000 people of diabetes increased from 17.5 in 2014 to 22.3 in 2016 and hypertension rate increased from 11 in 2014 to 12.2 in 2016. 36
One community-based study in Northeast Ethiopia was found that people aged 60 years and over had higher risk for pre-diabetes than people aged less than this group. 16 In South East Asia, from 2017 to 2045, diabetic prevalence rate is predicted to be increased by 84% 37
In a global scale, the prevalence of prediabetes is found in one in 4 healthy people and the prevalence of prehypertension is appeared in one in 3 healthy people and they tend to be increased in the near future 38 and diabetes will probably find in 629 million people aged between 20 and 79 years within 2045 37 while within 2025, hypertension will possibly affect 1.56 billion people. 39
As we all know, hypertension brings about many symptoms such as dizziness, heart failure, renal failure and eye problems or it can stay with people for years without obvious symptoms and then appears when blood vessels are destroyed while diabetes mellitus brings about many complications such as retinopathy, nephropathy, neuropathy, stroke and ischemic heart disease 16 and both of them come about cardiovascular disease, disability, and mortality. 40 For these consequential damages, early identifying and controlling risk factors at pre-stage can help to prevent the development step (at least 5 years for type 2 diabetes mellitus 41 and at least 4 years for hypertension42,43) and to manage promptly. To serve the purpose of prevention, lifestyle interventions are made to modify dietary consumption and physical activity to delay the incidence of both type 2 diabetes mellitus and hypertension at the prediabetes stage (when a fasting blood sugar level is from 100 to 125 mg/dL) and prehypertension stage (when a systolic blood pressure/diastolic blood pressure is from 120-140/80-90 mg/dL) 44 by applying lifestyle interventions in group sessions with the coach to encourage the behavioral changes. 45
Focus group is often chosen by the researcher as a qualitative methodology to give an opportunity to the participants for sharing experiences and identifying the trend of consultation, to promote the individual who is lack of self-confidence in exclusive talk but is willing to share information in the group as well as to get feedback and maximize social interaction between group members, while private In-depth interview is used as the method in order to keep concealment.46 -50
The beneficial characteristics of the qualitative method for this current study include, it is apparently effective in illustrating experiences and eliciting information about health-related behaviors and experiences from the participants and this method needs sample size as much as necessary owing to saturation is a criterion for selecting the number of participants, therefore, small sample size is adequate.51 -53
This study is the first qualitative study in Thailand that focused on the feedback getting from both prehypertension and prediabetes elderly patients who attended lifestyle modification at the temple-based level by using both focus-group discussion and In-depth interview methods to investigate the proficiency of lifestyle intervention program on long-term health-related behaviors improvement of the exclusive participants via their viewpoints.
Methods
Participants Characteristics
From the quantitative published study,2,3 the research was conducted at health promoting hospitals which were named after District Buddhist Temples in Nakhon Pathom Province (which was classified as semi-urban area in Thailand). 220 participants with aged 35 to 65 years at risk for diabetes and/or hypertension, their dwellings were near 12 studied temples which surrounded by at least 100 people and they visited the temples were recruited in the intervention, moreover, they were identified as at high risk for type 2 diabetes mellitus and /or hypertension (FBS: ≥100 and <126 mg/dL; SBP: ≥120-139 mmHg). These participants were excluded if they were diagnosed with heart diseases, unstable pulmonary disease, substance abuse, severe psychiatric problems, orthopedic or rheumatologic disease, kidney disease, type 2 diabetes mellitus and/or hypertension as well as their addresses were not located near 12 studied temples. However, 188 (85%) participants achieved the 12-month evaluation and 179 (81.4%) achieved the 12-month evaluation.
For this qualitative study, saturation is a criterion for selecting the number of participants. Thus, 62 participants (lived near 7 Buddhist Temples) were selected from 220 participants (lived near 12 Buddhist Temples) of the quantitative published study (after they had finished the lifestyle intervention program). The extra inclusion criteria for inviting them to participate in the study included they were with aged 50 years and above, they had ability to answer the questions and they had personal satisfaction to have an interview. Demographic variables were age, sex, educational level, employment status and occupation, the data were obtained from the published study.2,3
Study Design
A qualitative descriptive approach was utilized in this study as the data collection method. Triangulation method was also used to put great emphasis on the consistency and the credibility of the results by triangulating between interview methods
Study Timeline
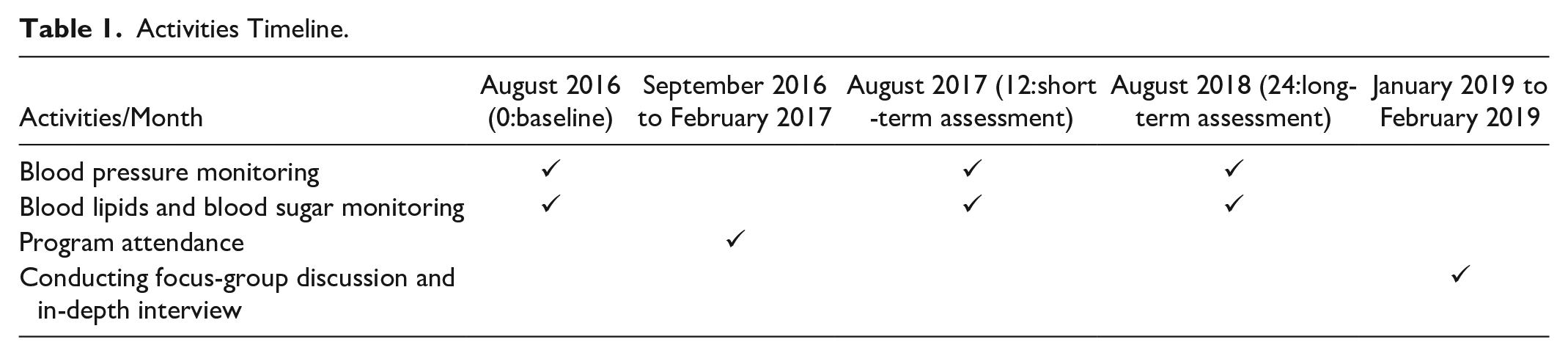
The timeline of the (previous) study can be divided into 3 parts according to the participants’ status; before attending the program, during program attendance and after the program had finished. Before attending the program, when program staff and participants first met at the health promoting hospital, which was called at baseline in August 2016, participants’ SBP and FBS were monitored to screen whether they were at high risk for type 2 diabetes mellitus and /or hypertension and they were asked about the knowledge of type 2 diabetes mellitus and hypertension. During program attendance, from September 2016 to February 2017, the participants who were included in this study were firstly asked to give their demographic information to the program staff and they were informed that they could withdraw from the study at any stage without any affected result. Then they attended 2-hour long sessions once a month for 6 months with different issue for each month at the health promoting hospital (six 2-hour group sessions of lifestyle intervention program guided by the Health Action Process Approach (HAPA) model 54 were operated by the program staff that acted as coaches and educators to help participants reduce consumption of high calories diets such as high-fat foods, sweets, and sugar-containing beverages and high sodium content diets such as salty foods and processed foods and to help them take more exercise and physical activity by giving them related knowledge, providing them blood monitoring and nutritional information about calories intake and teaching them exercise postures and assigning them food consumption record worksheet as well as getting feedback from them).
After the program had finished, participants’ blood monitoring were recorded again at 12-month (in August 2017 which was defined as short-term assessment) and 24-month (in August 2018 which was defined as long-term assessment) follow-ups intervals from baseline at health promoting hospital to see effects of intervention on diet consumption modification and physical activities/exercise modification as well as blood lipids, blood pressure, and blood sugar reductions. Focus-group discussion and In-depth interview were taken after 24-month follow-up interval (from January 2019 to February 2019) at the health promoting hospital. Activities timeline is concluded in Table 1.
Activities Timeline.
Interviews and Interview Guide
The qualitative study was conducted by using focus-group and In-depth interviews. The total number of participants attended both types of interviews depended on a sufficiency to achieve data saturation and participants’ satisfaction of having interview. Each focus-group interview contained not more than 5 people to control conversation and time. The first interviewer interviewed the participants both in In-depth interview and focus-group discussion to compare the consequences of with and without social interaction then the second interviewer did the same process to put an emphasis on the consistency of the results.
Before starting the interview, each participant gave informed consent to the researcher for the interview digital voice recording which was kept confidential. Then they received alias from the researcher for the data presentation to protect their privacy. All interviews, both In-depth and focus-group interviews, were conducted in Thai lasted between 60 and 90 minutes until all questions were answered. Transcripts were recorded and were kept secure. After that, participants were given money to compensate travel and time expenses. The discussion of both types of interviews were focused on lifestyle changes during lifestyle intervention program attendance and after the program had finished.
Semi-structured interview with open-ended questions was used as the data collection methods instead of questionnaires for participants in both types of interviews. Interview questions were structured based on the research objective and were developed from the previous researches2,3 by using proper words to guarantee that all aspects focused on experiences they had and actions they had been done to improve their health-related behaviors were captured. Therefore, the interview topics were divided into 2 main parts according to lifestyle modification; diet consumption modification (changing amount and type of food
Data Analysis
The measurement of the secondary outcomes (eating habits change and the change of physical activity level) were evaluated by noticing from the primary outcomes included TG, TC, LDL, FBS, and SBP. At baseline, participants’ SBP was monitored to appraise hypertension risk factor while FBS was monitored to appraise type 2 diabetes mellitus risk factor (FBS: ≥100 and <126 mg/dL; SBP: ≥120-139 mmHg). For short-term assessment and long-term assessment, SBP and blood lipids of those participants were monitored to appraise hypertension risk factors while FBS and blood lipids were monitored to appraise type 2 diabetes mellitus risk factors (FBS: ≥100 mg/dL ; SBP: ≥120-140 mmHg; TC: more than 200 mg/dL; TG: more than 150 mg/dL; LDL: more than 130 mg/dL).
Furthermore, the secondary outcomes were estimated from participants’ perspective by using focus-group and In-depth interviews. To make comprehension of the content, the conversations were listened and then transcribed verbatim by the researcher (field notes were supplemented as a complement of voice transcription) and they were translated into English by the translator. Translated interviews were brought into content analysis process. 55 The first step was to code and then arrange them to diminish information. The second step was to compare all codes and categorize them into sub categories to form the main issues. Data analysis was ceased when all points were saturated. Finally, the researcher brought final information to recheck by informant to investigate confirmation, reliability and correctness of interpretation.
Results
Demographics and Triangulating Results
Sixty-two participants were recruited from 7 out of 12 temples due to those participantswere fell into inclusion criteria of this study and it was sufficient to achieve data saturation as well as it was associated with time frame and expenditure. However, 16 of them withdrawn from the study owing to the time limit for doing their jobs, hence, the total number of the participants was 46. Focus group discussions were categorized into 2 groups by the name of Health Promoting Hospitals, Tambol Ngio Rai and Tambol Pi Hoo Chang and each group was divided into subgroup according to the interview grouping. The first group consisted of 3 subgroups: subgroup1 contained 3 participants, subgroup 2 contained 2 participants and subgroup 3 contained 2 participants. The second group consisted of 3 subgroups: subgroup1 contained 5 participants, subgroup 2 contained 3 participants and subgroup 3 contained 2 participants, hence, the total of the participants in focus group discussions was 17. A number of participants in In-depth interviews (from 6 Health Promoting Hospitals: Tambol Ngio Rai, Ban Khlong Sawang Arom, Wat Samrong, Wat Suwan, Talat Wat Makluea, and Tambol Nara Phirom) were 29.
The characteristic of the participants is shown in Table 2. The mean age of the participants was 57 years (SD = 4.57), they were between the ages of 50 and 65. Most of them were female (80%) and almost all of them (87%) were completed primary school. Almost half of them (46%) earned income from self-employed (67% worked as a farmer/agriculturist/gardener) while several participants (26%) earned income as an employee (42% worked as a freelance worker and 34% worked as a caregiver) and some of them (20%) were non-employed as they were housewife as well as the minority (4%) worked as a government officer (as public health officer and headmaster).
Participants Characteristics.

When comparing between focus-group discussion and In-depth interview, it can be found that the participants in both research methods declared their information and answered the question in the same way. This result was also expressed when comparing between 2 interviewers. When comparing the characteristics and the knowledge among all participants who lived near 7 temples, it can be found that they were low heterogeneity owing to they had little difference in age,50 -65 lifestyle (66% desired to consume unhealthy foods and irregularly took exercise before attending program), occupation (31% worked as a farmer/agriculturist/gardener), educational level (87% completed primary school) and the knowledge of diabetes mellitus and hypertension prior to program attendance (70% had little knowledge).
Lifestyle Modification Result from Lifestyle Intervention
The results of this study manifested 2 main issues. The first issue is “Having Exact Knowledge of Proper Nutrition and Exercise as well as Knowledge related to Diabetes Mellitus and Hypertension.” The second issue is “Adherence to Food Consumption Instruction and Program Exercise Postures as well as Exercise Equipment Accessibility or Exercise Activities Participation for Lifestyle Modification.” The results will be described according to the study timeline as follows,
Before attending the program
1. Lifestyle and symptoms
Before attending the program, two-thirds of the participants (66%) desired to drink high sugar beverage and they also desired to eat salty foods (foods that have been added or cured with salt, fish sauce or soy sauce such as shrimp paste peppery sauce), high–fat foods such as deep fried foods, streaky pork, crackling, egg, seafood and offal as well as coconut milk (via roasted curry and Thai dessert) and ate a lot of plates of rice or big portion of carbohydrate, moreover, they also used palm oil and soybean oil to cook food without knowing that these kinds of food were the results of high blood lipids, high blood sugar and high blood pressure levels that lead them to had high risk for diabetes mellitus and/or hypertension. A few of them (7%) took exercise. Main symptoms reported from the participants who were at high risk for hypertension were headache and dizziness or sleep problems, while some of them mentioned about family history.
2. Health problems
When asked about the health problems that prohibited them from working or pushed them to go to the hospital, more than half of them (54%) never had any problem.
The participants’ descriptions are concluded in Table 3.
Participants’ Descriptions before Attending the Program.

During program attendance
1. Exact knowledge related to diabetes mellitus and hypertension
The participants were advised by program staff to have appropriate nutrition, physical activity and exercise as well as the knowledge of diabetes mellitus and hypertension. For the exact knowledge related to diabetes mellitus and hypertension, the results were shown that the majority of participants (72%) knew from the program staff that they should use lard, canola oil, sunflower oil and rice bran oil to cook food instead of palm oil and soybean oil and they should avoid eating a large amount of high-fat foods, carbohydrate, salty foods and sugar to keep from at high risk for both diabetes mellitus and hypertension. Nevertheless, several participants (28%) denied that they received these knowledge or they received knowledge incompletely. Some of them (13%) did not know that people who have high lipids will probably be at high risk for both diabetes mellitus and hypertension and lean people do not always have low blood lipids. A few of them (7%) did not know about the normal blood pressure levels they should have or thought that they were able to go to see the pharmacist to have blood monitoring and to receive antihypertensive drugs and one of them dealt with high blood lipid levels in the wrong way by taking a steam bath instead of taking exercise. A few of them (9%) used herbs or traditional medicine to drop their blood lipids or blood pressure.
When asked about whether they discussed these knowledge with their relatives, neighbors and friends or not, it was shown that several participants (24%) had done it.
2. Adherence to exercise postures taught by the program staff
On the issue of adherence to program postures, the results were shown that several participants (39%) were able to remember and practice the arms swing and legs lift up postures. Some of them (20%) were able to remember and practice other postures. A few of them (9%) chose to practice the posture from other sources because they got used to it or they had personal satisfaction while a few of them could not remember or practice any posture.
3. Exact knowledge of exercise and daily physical activity
About the exact knowledge of exercise and daily physical activity, the result was manifested that one-third of them (33%) understood that physical activities they did in their lives such as sweeping, mopping, cycling and lifting up the stuff were the same as exercise, while some of them (11%) separated these actions.
4. Lifestyle modification of health-related behaviors
On the issue of adherence to the recommendation for behavior changes, the results were expressed that more than half of the participants (52%) made a change of eating behavior with goal setting by controlling their amount and type food consumption while a few of them (7%) had family members as supporters by warning them not to eat unhealthy foods or prepared them healthier foods. Furthermore, some of them (20%) paid attention to the record of what they had eaten that was called assignment or worksheet from the program staff. About exercise behavior, several participants (37%) made a change by taking more exercise themselves or a few participants (7%) had family members as supporters by persuading them to exercise while some of them (24%) needed friends to join exercise activities, so they chose to participate in senior clubs. For sleeping behavior, participants who could not get enough sleep made a change by getting more hours of sleep. For these results, several participants (37%) experienced better health. While a small number of them (9%) made changes to please the program staff.
Nevertheless, some of them (15%) paid less attention to the training from program staff or to record of what they had eaten in the worksheet or to read the document that describes calories contained in each type of food, while, several participants (24%) did not concern about the dish intake or ingredients and about getting enough sleep due to the characteristic of their careers and time restrictions act as inhibitors or they got used to eat unhealthy food. A few of them (4%) thought that syrup is better than coconut milk while a few of them (7%) still did not cut off the amount of rice consumption. Some of their family members (11%) acted as inhibitors by cooking them high-fat foods or salty foods and buying sweets for them. For exercise, some of them (20%) paid less attention to exercise owing to they were too busy or felt lazy or they had health problems or they would do whenever they wanted or they needed friends to go with them and encourage them.
The participants’ descriptions during program attendance are concluded in Table 4.
Participants’ Descriptions during Program Attendance.

After the program had finished
1. Lifestyle modification of health-related behaviors
The results were shown that more than two-thirds of the participants (70%) found that it was not easy to adhere to the suggestion they received from lifestyle intervention courses and to understand about type of food they should eat or things they should avoid to keep from at high risk for diabetes mellitus and/or hypertension such as they still consumed high-carb foods, high-fat foods and salty foods and took less exercise as well as they were not able to not get enough sleep, at 1-year and/or at 2-year follow-ups intervals, owing to they had personal satisfaction or had health problems or they concentrated on their works or their family members acted as inhibitors or dining out made them difficult to avoid unhealthy food or they thought that the program staff abandoned them. While a few of them (4%) had weird blood pressure levels owing to their bad sleep health or they felt tired from cycling or felt excited before blood monitoring and a few of them (4%) had weird blood lipid levels owing to they dined outside.
A small number of the participants (4%) denied to cook healthy recipes due to the laziness while a few of them (7%) refused to eat fish owing to fishy smell or toxic chemicals contamination and a few of them (7%) refused to eat Parkia speciosa (bitter beans or sator) to reduce high blood pressure, the reason was it smelled bad. While some of them (13%) emptied the dish to avoid having leftover food.
However, more than half of them (59%) informed that they made some changes such as limited the portion size or had mealtime management or chose to eat healthier foods and gave the value of exercise as well as developed personal goal to be in good health. Some of them (18%) had family members as supporters for the changes, especially their children or grandchildren.
2. Accessibility to exercise equipment or exercise activity provided by local sector organization
When asked about exercise equipment and/or exercise activities provided near their village, a few of the participants (9%) reported that there were not any equipment or activities provided by Sub-district Administrative Organizations while some of them (11%) stated that there were equipment and/or activities but they still did not utilize or take part in because of the remoteness from their homes or they were too busy, and some of them (15%) informed that they had already used the equipment and/or took part in the activities.
3. Program beneficiation and recommendation from participants
When asked about the beneficiation from the program or how should the program staff do to make them keep practicing according to the recommendation or what was the source of motivation they used for lifestyle modification, the majority (83%) manifested that they got better health, received knowledge of proper foods and exercise as well as obtained an inspiration of lifestyle modification and acquired blood monitoring that they had been rejected by the primary care setting. Moreover, they assumed that after the program had finished, there was no one coming to control, so most of them did not continuously keep practicing, therefore, it depended on personal awareness and responsibility.
The participants’ descriptions after the program had finished are concluded in Table 5.
Participants’ Descriptions after the Program had Finished.

An overall summary percentages of the participants for each issue is shown in Table 6.
Percentages of the Participants Who Performed Health-Related Behaviors at Each Period of Time.

Effect of Lifestyle Intervention on Blood Pressure, Blood Lipids and Blood Sugar Profiles Improvement
From Table 7, on the issue of the trend of blood profiles and from baseline to 12-month follow-up interval and from 12-month follow-up interval to 24-month follow-up interval, the results were shown as follows,
SBP profile increased and then decreased in most of them (17%).
FBS profile increased and then decreased in most of them (43%).
TC profile increased and then decreased in most of them (38%).
TG profile increased and then decreased in most of them (24%).
LDL profile increased and then decreased in most of them (32%).
Blood Monitoring Results.

Mixed results of blood profiles in the rest of them included decreased then decreased, increased then increased, decreased then increased, strong increased then decreased, decreased then strong increased, strong increased then strong decreased, decreased then strong decreased, steady then decreased or steady then steady.
Moreover, it can be seen that blood profiles in some participants (13%) were independent, while in almost all of them (87%), the trends of TC were related to the trends of LDL and in several of them (42%) the trends of TC were related to the trends of LDL and TG. Total number of participants who had excess blood monitoring results are concluded in Table 8.
Amount of Participants with Excess Blood Values at Baseline, Short-Term and Long-Term Assessment.

*Source. 1. Blood Pressure: Blood pressure chart; www.bloodpressureuk.org.
Diabetes – Diagnosis and treatment – Mayo Clinic; https://www.mayoclinic.org.
Understanding Your Cholesterol Report; http://www.webmd.com.
In addition, when noticing from the relationship between the frequency of program attendance (from Table 2 that almost all of the participants (91%) attended the course more than 3 times from 6 times, while 33% of them completely attended) and their blood profiles (from Table 7) and between the frequency of program attendance (from Table 2) and the total number of participants who had excess blood monitoring results (from Table 8), it can be seen that high-frequency program attendance could not guarantee that they would modify their lifestyle of food consumption and exercise to achieve blood results improvement.
Discussion
This research is one of the rare qualitative studies to investigat the view of prediabetes and prehypertension elderly patients living around temple on lifestyle intervention program enhancing long-term health-related behaviors improvement to fill the gap in partially successful intervention by using a triangulation method to triangulate between interview methods (focus-group discussion and In-depth interview), places (7 Health Promoting Hospitals) and interviewers (2 interviewers) to put great emphasis on the consistency and the credibility of the results. There was little difference between the answers from the participants in focus-group interview and the participants in In-depth interview as well as between the answers interviewed by the first interviewer and the second interviewer. This might be because the participants lived in the same area and they were low heterogeneity so they had the same temperament, behavior, habits and lifestyle.
Before attending lifestyle intervention program, two-thirds of participants consumed unhealthy foods and used palm oil and soybean oil to cook food as well as irregularly took exercise that led them to have high risk for diabetes mellitus and/or hypertension owing to they had little knowledge about these health problems 56 and they got used to consume these kind of foods. Main symptoms they reported included dizziness headache and sleep problems correspond to other studies.57,58
However, more than half of them reported that they never had any health problems that prohibited them from working or pushed them to go to the hospital.
During program attendance, the participants received knowledge of suitable nutrition and exercise from program staff. It can be seen the participants’ intension to accomplish lifestyle modification from the majority of them made changes of eating behavior by themselves or they were supported by family members such as used properly oil to cook food, avoided eating high-fat foods/salty foods/a large amount of carbohydrate and sugar to keep from at high risk for both diabetes mellitus and hypertension 59 and gave the value of food consumption records that were used for developing personal goal to be in good health.49,60 They also made a change of exercise behavior by themselves 61 or by the support from friends or family members 51 and made a change of sleeping behavior by getting more hours of sleep.
However, several participants denied that they received knowledge from the program staff or they received incomplete knowledge similar to the studies done in United Kingdom which was found inadequate contact between the patient and staff 62 Some of them still misunderstood that lean people must have lower blood lipid levels than overweight people while a few of them still used herbs or traditional medicine to drop their blood lipids or blood pressure instead of changed their eating behavior and exercise behavior owing to they got this belief from the word of mouth or it passed down through generations.57,58 Some of them still paid less attention to record of what they had eaten in worksheet and to get enough sleep as well as ignored to concern about the type of food they should consume or calories contained in each type of food 57 owing to work priorities or it was their habitual behavior and convenience or their family members prepared them unhealthy food.
Needed friends was still the main reason for them both to attend and not to attend exercise activities because they wanted people to group together and join them50,53,63 -65 while some of them had health problems so they were not able to take exercise.
For program exercise postures practicing, several participants were able to remember and practice the arms swing and legs lift up postures due to these postures were easy to remember and practice. About the exact knowledge of exercise and physical activity, one-third of them understood that activities they did in their lives such as housework and other tasks were the same as exercise although some of them did these activities less than 30 minutes. Actually, daily activity (light-intensity activity), is to use labors to complete the work by moving with a lot of postures such as do housework, gardening, running or do activities in daily life and can be considered as exercise if the participants perform them more than 30 minutes every day that is fruitful to get rid of blood lipids and to reduce blood pressure. While exercise (moderate-to-high- intensity activity) to do the only one posture repeatedly for 75 to 150 minutes per week such as aerobic dance, weight lifting, jogging, cycling, walking or swing arms for 100 times.66,67
After the program had finished, more than two-thirds of them had minimal concern to take care of themselves at 1-year and/or 2-year follow-ups intervals owing to they felt lazy29,49,50,56,64,68 or they had health problems or they concentrated on their works or they dined out with their family or their friends in holidays or social events and ceremony that was difficult to avoid unhealthy food48,50,63 or they thought that the program staff abandoned them, so there was useless to continuously practice. However, more than half of them demonstrated some changes such as limited the portion size or had mealtime management or chose to eat healthier foods and gave the value of exercise as well as developed personal goal to be in good health owing to they did not want to be a burden on family member or they were supported by family members to achieve the changes correspond to the research results from Australia 56 and from Norway 58 which were found that family members were the major supporter for behavioral changes. The confliction came from different participants gave the value of or interpreted the suggestion of behavior changes from the program in different aspects. 49
For exercise equipment accessibility or exercise activities participation, there were 3 types of the answers form the participants included there were not any equipment or activities provided by local sector organization, there were equipment and/or activities but they still did not utilize (because of the remoteness from their homes or they were too busy) 48 and they had already used the equipment and/or took part in the activities. The majority had benefited from the program regarding getting better health, receiving knowledge of proper foods and exercise as well as obtaining an inspiration of lifestyle modification and acquiring blood monitoring that they had been rejected by the primary care setting.49,64
When noticing from the trends of participant’s blood profiles that increased from baseline to 12-month follow-up and then decreased from 12-month follow-up to 24-month follow-up, it can be seen that most of the participants made changes of their lifestyle from 12-month follow-up to 24-month follow-up and when noticing from the trends of blood profiles in almost all of them, it can be seen that the trends of total cholesterol were similar to the trends of LDL. While mixed results of blood profiles were found in the rest of them. 68
When noticing from the relationships among blood profiles, the frequency of program attendance and the total number of participants who had excess blood monitoring results, it can be seen that high-frequency intervention program attendance was not able to guarantee that they would modify their lifestyle of food consumption and exercise owing to the improvement of their blood profiles and behaviors was constructed from many pillars included the knowledge and advice provided by the program staff, the good result (from the improvement) passed down by word of mouth from peer group together with personal awareness as well as their acceptability of the modification to practice in their daily lives and to be accomplished that was corresponded to those findings of worldwide existing studies which declared that program participation of the elderly associated with internal self-control and motivation to have lifestyle change49,50,58,59,62,63,64,69 -71
Strengths and Limitations
This research displayed the study findings that had been investigated to appraise lifestyle modification at the temple-based level toward pre-diabetes and pre-hypertension self-management among older adults in Thailand. The recruitment of the participants was conducted in a variety of health promoting hospitals. The triangulation between 2 interview methods can affirm the consequences of with and without social interaction. Using 2 researchers to conduct interviews and the triangulation between 7 places can certify the reliability and consistency of the results. The use of semi-structured interview with open-ended questions persuaded the participants both in In-depth interview and in focus-group discussion to reveal their experiences. Long term assessment were conducted to know better about the sustainable of food control and regularly exercise by noticing from program postures practice and exercise equipment and/or exercise activities utilization/participation as well as food consumption control. The research results were not only based on the report from the participants about lifestyle modification that might cause recall bias, interviewer bias and social desirability bias but they also based on demographics and triangulation results as well as blood results to ensure the reliability.
The limitations included participants were homogeneous owing to most of them were female and they had similar lifestyle, occupation and educational level and owing to a small sample size was sampled (although it was an adequate quantity to achieve saturation) as well as the study was conducted in health promoting hospitals in semi-urban area, the findings were inappropriate to use as a reference to private hospitals and government hospitals in urban, sub-urban and rural areas. 53 Greater scale researches are required to strengthen generalizability of research outcomes.
Conclusions
Although the participants in this study had little knowledge associated with diabetes mellitus and hypertension as well as properly food and exercise before attending the program, they received these knowledge during program attendance from program staff, therefore, most of them made a change of eating behavior and exercise behavior. However, several participants still had some incorrect behaviors owing to they got used to unhealthy lifestyle. For exercise, several participants were able to remember and practice the easy postures and they misunderstood about the proper time to exercise. Moreover, they were willing to attend exercise activities when they all grouped together owing to their peer group had a strong influence on them and motivated them to exercise. After the program had finished, most of the participants made changes of their lifestyle from 12-month follow-up to 24-month follow-up and developed personal goal this might be because it takes too much time and takes too many factors to adjust lifestyle behavior to be sustain and to be seen the satisfactory results. Their family members were both inhibitors and supporters 50 for the made changes of both eating behavior and exercise behavior and both during program attendance and after the program had finished, while their works or their attitudes were appeared to be barriers for them. Participants who had self-indulgence were less likely to accomplish the improvement than those who had self-efficacy.
Lack of accessibility to exercise equipment or exercise activities of the elderly living around temple areas due to their burdens or the remoteness from their homes or local sector organization still did not provide for them to utilize. Almost all of them had benefited from the program regarding getting better health, receiving knowledge of proper foods and exercise as well as obtaining an inspiration of lifestyle modification and acquiring blood monitoring that they had been rejected by the primary care setting.
For those mentioned results, it can be estimated that lifestyle intervention program had partial effects on lifestyle modification by improving the ways of eating and taking exercise of the participants, however, intervention program together with personal attitude, awareness, responsibility and acceptability59,70 were wholly productive for long-term lifestyle changes which will invigorate their healthy lives.
Recommendation for Future Researches
When noticing from participants’ narrations and behaviors, many things should be conducted for future research to improve participants’lifestyle modification and lifestyle intervention program which are able to be corresponded to their daily lives and to be accomplished by them easily. 48 Owing to the nature of older adults who live around health promoting hospitals in semi-urban and rural areas in Thailand usually pay less attention to acquire knowledge via the text from internet, books, pamphlets or documents, the program staff should completely give exact knowledge related to diabetes mellitus and hypertension face-to-face to the group of these participants on the issues of normal blood pressure level they should have, type of oil they should use for cooking foods, lean people can have high blood lipid levels and advise them to change their eating behavior and exercise behavior to deal with their blood lipids or blood pressure level instead of using herbs or traditional medicine as well as extend information about the difference between exercise and physical activity and proper time for doing daily activities at work or at home that are require more than 30 minutes every day to get rid of their blood lipids and to reduce their blood pressure levels. Furthermore, program staff should improve exercise postures teaching techniques by teaching them step by step and providing them videotape to encourage them in continually practicing at home after the program had finished. Collaborating with local sector organization to provide exercise equipment or to organize exercise activities and with primary care setting to support blood monitoring for the elderly living around temple areas are also need to be focused. Moreover, apart from the knowledge, comprehension and motivation as well as more frequent than 1 year follow-up68,70 by using telephone call or visiting them at home or organizing community activities to group together as well as making a promise not to abandon them and elevating self-awareness regarding lifestyle modification are needed to give greater effectiveness of long term behavioral changes and of blood profiles improvement50,56 because they need someone who coming to control them and they want to make certain that the program staff will not abandon them after the program had finished. In addition, clinical parameters monitoring results together with anthropometric parameters monitoring results such as body mass index (BMI) and, Waist-hip ratio (WHR) of the participants during program attendance should also be recorded to see the development of the participants and to compare with the results from before attending the program and after the program had finished.
In the future, the program should especially concern for the group of bedridden patient caregivers owing to the group of these people still had no idea how to take care of themselves because they had enormous burdens.
Supplemental Material
sj-docx-1-inq-10.1177_00469580211025209 – Supplemental material for Participants’ Views on Lifestyle Intervention Program Enhancing Long-Term Health-Related Behaviors Improvement among Prehypertension and/or Prediabetes Mellitus Older Adults: A Qualitative Study Examined in Thailand at Health Promoting Hospitals
Supplemental material, sj-docx-1-inq-10.1177_00469580211025209 for Participants’ Views on Lifestyle Intervention Program Enhancing Long-Term Health-Related Behaviors Improvement among Prehypertension and/or Prediabetes Mellitus Older Adults: A Qualitative Study Examined in Thailand at Health Promoting Hospitals by Isareethika Jayasvasti, Manisthawadee Jayasvasti, Supa Pengpid, Karl Peltzer and Pheeraya Nanthananate in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580211025209 – Supplemental material for Participants’ Views on Lifestyle Intervention Program Enhancing Long-Term Health-Related Behaviors Improvement among Prehypertension and/or Prediabetes Mellitus Older Adults: A Qualitative Study Examined in Thailand at Health Promoting Hospitals
Supplemental material, sj-docx-2-inq-10.1177_00469580211025209 for Participants’ Views on Lifestyle Intervention Program Enhancing Long-Term Health-Related Behaviors Improvement among Prehypertension and/or Prediabetes Mellitus Older Adults: A Qualitative Study Examined in Thailand at Health Promoting Hospitals by Isareethika Jayasvasti, Manisthawadee Jayasvasti, Supa Pengpid, Karl Peltzer and Pheeraya Nanthananate in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to thank National Research Council of Thailand for promoting the research project and the staff of 7 health promoting hospitals for kind supportive for providing accommodation.
Authors’ Note
IJ, KP and SP designed conceptualized and managed the project. SP proposed the project for ethics approval. IJ and PN conducted interviews. MJ arranged information. IJ and MJ analyzed data and produced the manuscript. SP reviewed/edited the manuscript and provided the research supportive budget and KP provided the publication fee. All the authors participated in approving the final draft of the manuscript and all revisions of the manuscript.
Availability of Data and Resources
The dataset generated and/or analyzed during the current study are available from the lead author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by National Research Council of Thailand.
Ethics Approval and Inform Consent
Ethics approval [MU-SSIRB: 2016/038.0202 and 2016/053 (B1)] were granted from the Committee for Research Ethics (Social Sciences), Mahidol University prior to study onset. The Committee are in full compliance with International Guidelines of Human Research Protection such as Declaration of Helsinki, The Belmont Report, and CIOMS Guidelines and are independent of all the institutions involved and had no role in the design, conduct or reporting of the research. All the participant gave informed consent to the researcher before the interviews took place.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.