
Abstract
Unplanned surgery cancellation (USC) was an important quality management issue in the course of medical care for surgical patients, which caused inappropriate use of hospital resources and had negative impacts on quality and safety. This study used Lean Six Sigma to reduce the incidence of USC. Following the Lean Six Sigma DMAIC (Define, Measure, Analyze, Improve, and Control) process, the main factors influencing the USC were identified, such as the time of informing patient admission, the time of submitting operation notice, and the management of test report follow-up. A series of measures were implemented including improving the health education content of virtual bed patients, standardizing the way of communication between the Admission Management Center and the patients, improving the timing of anesthesia evaluation, optimizing the process of operation notice with an information system, and implementing the regulations of virtual bed management. The incidence of USC reduced from 10.21% in Jan. 2016 to 3.8% in Dec. 2016, and the Z-score increased from 1.25 to 1.68, which improved patient safety and demonstrated that Lean Six Sigma was an effective method to solve cross-department issues in hospital.
Lean, Six Sigma or Lean six Sigma methodology have been increasingly used in the healthcare industry in recent years, such as improving operating room efficiency, optimizing on-time surgery, reducing fixed operating room expenses, improving patient transfer process and turnover time, which were proved to be effective approaches. In hospital operation and management, the unplanned cancellation of surgery affected surgical safety and patient experience, caused inconvenience to both patients and families, wasted the resource of operating room, and reduced work efficiency. Every hospital should consider the surgery cancellation as an important issue and systematic improvement should be needed.
This study enriched the research in the field of surgery cancellation, providing evidence of hospital-related causes and effective interventions for peers, and demonstrated a case how to apply Lean Six Sigma to solve cross-department issues in hospital.
Lean six sigma could be applied to redesign and improve a wide range of healthcare processes.
Introduction
The cost of medical care is increasing globally in recent years, and medical service issues due to process designing are widespread, such as duplication of services, long waits for patients, and underutilization of existing resources. How to achieve the balanced development of quality, cost and speed is an urgent problem for hospital management. In this context, many medical institutions in the world have introduced Lean, Six Sigma and other innovation approaches to achieve high level of operational efficiency.1-4
As an advanced management concept and mode, Six Sigma originated from Motorola in the United States in 1986, which is a methodology based on data analysis and has a good framework for problem solving. Lean production originated from the Toyota Production System (TPS) created by Toyota Motor Corporation of Japan after World War II. Lean management aims to eliminate waste, optimize processes, and improve just-in-time production. 5 Value Stream Map, TAKT time, Kanban, Seven Wastes, Visual Management and 5S are some of the common lean analysis and improvement tools, which have been applied to the medical industry in recent years.6-8 Both Lean and Six Sigma are activities designed to implement continuous improvement, emphasizing customer satisfaction and system integration. The starting point of Six Sigma is to reduce variation, and the core of lean production is to eliminate all unnecessary wastes, but the process of eliminating variation itself is to reduce waste. The consistency of goals and the complementarity of tools made the combination of Lean and Six Sigma inevitable.
Lean Six Sigma is a combination of Lean thinking and Six Sigma methodology, which has been commonly used in production industries to improve process efficiency and quality, and is increasingly used in the healthcare field.9,10 For instance, it was applied to reduce the risk of healthcare-associated infections,11,12 improve operating room efficiency, 13 improve timeliness of discharge from the hospital, 14 and improve patient transfer process. 15
Taizhou Hospital of Zhejiang Province is a tertiary hospital with 1,800 open beds. Six Sigma was implemented at Taizhou Hospital in 2001 with the first wave of GB training. In 2013, the hospital integrated Lean and Six Sigma, forming three types of projects including Lean, Six Sigma and Lean Six Sigma, which covered all aspects of quality, medical procedures, and patient satisfaction. This study demonstrates a case of applying Lean Six Sigma to reduce the incidence of unplanned surgery cancellation.
Unplanned surgery cancellation (USC) is a widespread problem for many health care organizations,16-20 which causes distress and inconvenience to patients, affects health care quality, wastes operating room resource, and leads to low operational inefficiency. Many studies reported that the incidence of USC was higher than 10%, even more than 40% in Low- and middle-income countries. 21 Literature revealed many reasons for USC,22-24 such as insufficient operating room capacity, lack of hospital beds, failure of equipment, insufficient planning of surgery, absence of staff, patient no-show, and patient’s medical condition. It is essential to analyze the reasons for USC at one’s individual hospital to reduce the cancellation rate. There is little literature using Lean or Six Sigma approach to solve the problem of USC. It was hoped that through this project, hospitals would pay more attention to the medical care process of surgical patients, focus on patient needs and process efficiency, and avoid the occurrence of USC.
In 2009, Taizhou Hospital began to implement virtual bed management, which refers to performing preoperative examination and evaluation before surgery in the outpatient department. This measure effectively reduced the average length of stay and the average cost of hospitalization. However, more complaints were appeared in the daily operation from process related parties. For example, the operating room complained that the operating room resources were wasted due to USC of virtual surgery patients. The patients and families complained of repeated visits to the hospital before surgery, inadequate preoperative evaluation and surgery cancellation, which reduced the patient’s medical experience, and required urgent improvement.
Methods
The study was conducted in 2016 and adopted Six Sigma framework, which was structured according to the Define, Measure, Analyze, Improve, and Control cycle (DMAIC), and reduced the occurrence of USC through continuous rapid improvement, elimination of waste and defect. The data was analyzed by Minitab version 17. Chi-square test was used to compare the incidence of USC between different groups, and the statistical significance was set at P < .05.
Define
Based on the service satisfaction survey and the analysis of the patients’ complaints, the project team obtained the surgery patients’ demands including operation security, painless, accurate diagnosis, reasonable surgical planning and accurate preoperative preparation. A Tree diagram was used to analyze the needs of patients, which help to identify specific, measurable requirements. Combining the needs of patients with the existing hospital service capacity, the key needs of patients was confirmed, that was, no unplanned surgery cancellation event occurred.
According to statistics, 30,139 operations in surgical departments were conducted in Taizhou Hospital in 2015, including 21,955 selective operations, which means the operation is not urgent, and surgery could be chosen at the most appropriate time. In 2015, 13.2% (2,897 cases) of the selective operations were cancelled for various reasons, and the virtual bed patients accounted for 81.4%, so the key point of this improvement was to reduce the incidence of USC for virtual bed patients. This project was closely related to the strategic objectives of the hospital to improve the patient care experience, ensure the safety of the operation, and make the operation room work more efficient.
The scope of the project was established using the SIPOC (Supplier, Input, Process, Output, and Customer) diagram. In this project, the surgical procedure started with a virtual admission notice and ended with the start of the operation. Based on the scope of the project, a cross-departmental team was set up, including the Department of Quality Improvement, Department of Medical Administration, and other related departments in the process.
The Critical To Quality (CTQ) is internal quality parameters that relate to what the customers want and need. In this project, the CTQ was the rate of USC. The defect was defined as USC, which meant the operation room had received the notice of surgery and had arranged the time, but the surgery was cancelled temporarily. The incidence of USC = # cases of USC/concurrent cases of selective operation × 100%. Combined with the current data, improvement focus, and the project team capability, a goal was set reducing the rate of USC to 5% by December 2016.
Measure
Initially, a data collection form was formulated. The data was extracted from the operative anesthesia system. One of the project members was responsible for the data collection. During the first quarter of 2016, the incidence of USC was 12.3% (775 cases). The process capacity analysis showed the Z-score was 1.25, indicating a greater space for improvement. About 74.09% of the cancelled surgeries were the virtual bed patients.
Then focusing on the flowchart of surgical procedures for selected virtual patients shown in Figure 1, a brainstorming session was launched from 5 aspects: Manpower, Machines, Methods, Materials, and Environment to find out the possible influencing factors of USC. With brainstorming session, the project team listed 33 factors of USC using Fishbone Diagram (Figure 2).

Flowchart of surgical procedures for selected virtual patients.

Analysis of surgery cancellation using a fishbone diagram.
The input factors could be divided into two categories: simple and clear X suitable for direct improvement (category 1 X), and X requiring further in-depth analysis (category 2 X). The simple and clear factors were classified with the Affinity Graph, and the quick win measures were implemented immediately as follows.
Quick Hit 1: Improving the health education content of virtual bed patients
After interviewing the virtual bed patients about the needs of health education, the project team revised the instruction manual of the Admission Management Center, which was described with pictures so the patients could understand easily. 19
Quick Hit 2: Standardizing the way of communication between the Admission Management Center and the patients
An information checklist for virtual admission was formulated to clarify the contents and requirements, 19 which helped to avoid important information omission before operation and controlled the fluctuation of information quality among different nurses.
Quick Hit 3: Improving the timing of anesthesia evaluation
The preoperative anesthesia evaluation of virtual patients was carried out in the outpatient department (Figure 3), which has been proved effectively in reducing the rate of surgery cancellation.25,26 The scope of assessment included age, cardiopulmonary disease, hypertension, and diabetes to reduce the number of round-trip hospitals caused by incomplete examination.
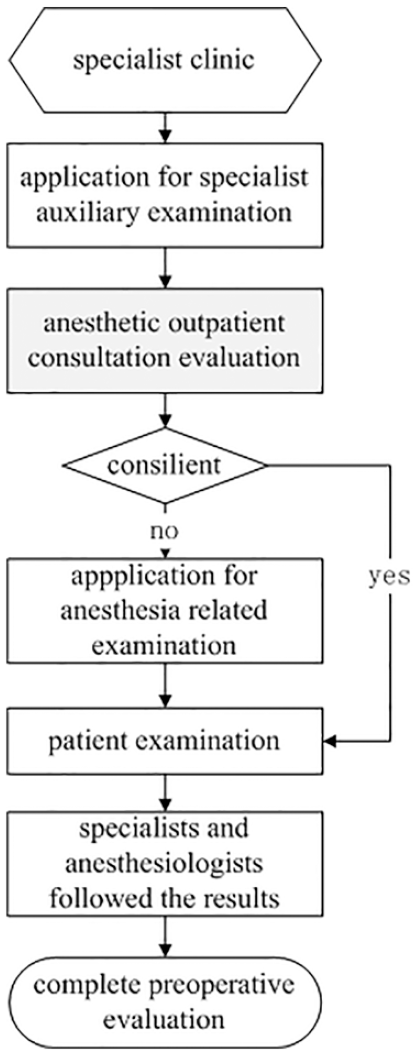
Process of preoperative anesthetic assessment after improvement.
Quick Hit 4: Improving the doctor’s problem
When prescribing the inpatient appointment card in the outpatient clinic, if patients asked to select a surgeon, the doctor could fill in the information in the “Remarks” column in the outpatient doctor workstation, which was convenient for the relevant personnel to know. After a month, USC due to patient selecting surgeon did not occur.
After the implementation of the above quick win measures, the incidence of USC reduced to 7.5% by August 2016.
Analyze
In the analysis phase, 4 important factors were further verified including X1 time of informing patient admission, X2 time of submitting operation notice, X3 mode of test report check, and X4 management of test report follow-up.
To determine which X values were the key factors impacting problem Y, data were collected with Table 1, and a chi-squared test was used, which is a statistical method commonly used for testing relationships between categorical variables (Table 2). The chi-square test revealed that X1 and X2 were significantly related to USC (P < .05), and X3 was not related to USC (P > .05).
Data collection table.

Chi-square test on the influencing factors of unplanned surgery cancellation.

For X4, the project team designed the questionnaire and conducted on-site visits with 60 doctors to follow the management status of the virtual patient beds. The results showed that nearly 60% of the departments with a high incidence of USC lacked special management and clear responsibility, so the preoperative management was the focus for improvement.
After a comprehensive analysis, the key influencing factors of Y were confirmed: (1) X1: inform patient admission 2 days in advance, (2) X2: the time of hospitalization notice needed to earlier than the operative notice, and (3) X4: special person responsible for review and test report follow-up.
Improve
According to the root causes confirmed in the analysis phase, improvement plans were formulated and the priority order was evaluated from the aspects of implementation time, scope, difficulty and effect.
According to X1 and X2 improvement, the process of operation notice was optimized with an information system (Figure 4). The doctor could submit an operative notice, only when the information was confirmed correctly with the patient by the Admission Management Center, which controlled the factors of USC due to the patient failing to come to hospital or physiological factors.

Process of submitting operative notice (before and after improvement).
According to X4 improvement: (1) each medical team was assigned a doctor responsible for virtual bed management, (2) training of preoperative management for surgeons was conducted, (3) the regulation of virtual bed management were implemented, (4) the results were monitored with multichannel feedback (Bulletin, Mobile message, etc.), (5) communication and discussion was carried out in the key departments and key groups to reach a consensus, and (6) Health Enze APP was promoted to use, which was convenient for doctors to check the test reports of virtual bed patients anytime, anywhere.
Control
A control plan was formulated after the implementation of the improvements. The project team continuously monitored the data of the operation and anesthesia which was published weekly in the hospital network, and the departments with high rate of USC were reminded by mobile message, and improvement measures were employed when the data were not in place or abnormal. A control chart was used to assess and monitor the process.
Results
The standardization content of improvement measures in this study could be summarized into three aspects, including institutionalization of specially-assigned management in the process of preoperative assessment, redesigning the procedure of submitting the operation notice, and standardizing the health education and communication methods in the process of admission notification.
The rate of USC was plotted monthly with specially designed visual graph which was pasted on the strategic wall of the operating room. Over the study period from January to December in 2016, the highest cancellation rate was observed in March (11.4%) and the lowest in December 2016 (3.8%). During the fourth quarter of 2016 which was considered as the post-interventional phase, 5953 surgeries were scheduled, of which 278 cases were cancelled displaying a cancellation rate of 4.67%. We employed the chi-square test to compare the rate of USC before and after intervention. Table 3 showed that there were significant differences between the two groups (P < .05). The process capacity analysis showed that the Z-score increased from 1.25 to 1.68, which represented an obvious improvement.
Comparison of the rate of USC before and after intervention in 2016.

Figure 5 showed control chart of USC in pre-interventional phase (from Jan. 2015 to Sept. 2016) and post-interventional phase(from Oct. 2016 to Dec. 2017). In the pre-interventional phase, samples 5, 20 and 21 were abnormal. In the post-interventional phase, the cancellation rates appeared more controlled with only one point violating control rules, and the average cancellation rate decreased from 10% to 2.91%.

The Control Chart of USC before and after intervention.
The project team continued to track and monitor the process from 2017 to 2019. Figure 6 showed that the incidence of USC was continually stable and controllable which was kept under 5% after intervention. The results confirmed that the key interventions have significantly improved the USC.

The incidence of USC from 2015 to 2019.
Discussion
Optimizing the Management Process of Surgical Patients to Achieve Improvement of Quality, Efficiency, and Cost
The surgical procedure is the key process of medical service in the hospital. The influencing factors of USC varied in different hospitals, which could be classified into three categories: hospital-related, patient-related, and surgeon- or anesthesia-related reasons. Evidence confirmed most cancellations were preventable.20,24,27 In this study, we found the root causes were the process management related issues. For virtual bed patients of selective surgery, relevant departments and personnel involved inpatient wards, Admission Management Center, operating room, auxiliary examination departments and patients, so the causes of surgery cancellation such as “patient no show” had to be further analyzed to find the root causes.
In this study, firstly the team focused on the demands of the related parties in the process, and then turned the demands into CTQ. Through the analysis of the Fishbone Diagram and hypothesis test, the real causes were determined and countermeasures were put forward. After interventions, the incidence of USC decreased from 10.21 to 3.8% in 2016, which improved patient surgical safety, maximized the use of surgical resources, and improved the patient care experience. The project was shared within Enze Medical Center, and communicated with medical peers outside the center.
Fostering a Culture of Interdepartmental Collaboration
In the current mode of the hospital’s operation, the departments were set up by function, making it easy to focus on the function of the department and ignore the benefit of the whole process. In this project, focusing on the patient, the team tracked the process of virtual bed patients, and found that patients had to traverse several departments in the hospital, such as the outpatient doctor, hospital admission management center, examination departments, ward area, and operating room. It was essential to foster a culture of interdepartmental collaboration to carry out improvements. 28
Pursuing Continuous Improvement
From the perspective of process, represented as Y = f(x), the input factors must be managed to generate favorable results. 29 In this study, by improving the process input factors, such as patient education, the timing of anesthesia evaluation, the time of operative notice, and the management mode of virtual beds, the target goal of the project was reached, and fluctuations in the output were controlled.
Using Scientific Methods to Solve Problem Effectively
On the methodology, Lean Six Sigma emphasizes system integration and innovation, which is not just about applying statistical techniques to solve problems. In this project, common quality management tools, Lean tools, statistical techniques, and information technology were used, so Lean Six Sigma is an integrated system for improvement.
Synthesis of Lean Thinking and Six Sigma
Six sigma provides a general analytic framework for problem solving, while Lean offers a number of standard solutions to common problems. The combination of the two methodologies can not only solve the problems related to variation, but also optimize the process. In this project, following DMAIC cycle, lean thinking and tools were integrated into analysis and improvement. For example, in the process of preoperative examination, radiology, ultrasound and other medical technology departments carried out lean practice, arranged ultrasound, CT and MR examinations according to the daily order amount, and implemented Kanban management to monitor the rate of examination completion. All the examinations were scheduled by the Admission Management Center following First-In-First-Out (FIFO), and completed in one visit to the hospital, avoiding many times runs for virtual bed patients. In the process of preoperative assessment, visual management was introduced to manage the patients’ report completion time with “red, yellow and green” color, which reminded doctors to timely complete the review and evaluation of report results, and reduced the report inventory. Before the patient received the operation notice, pull system was set up to control the number of inpatients in one week according to the average length of stay in each department. Process optimization was carried out by adopting ECRS principle (Eliminate, Combine, Rearrange, Simplify), which reduced the cancellation due to patients’ failure to turn up. Doctors used mobile APP to review examination results at any time, so as to change the previous large-batch audit into small-batch audit and save doctors’ working time.
Conclusions
Many quality improvement projects occurred rebound after the end of the project, so it was necessary to keep track of the project for a year or more, and continuously monitor and solidify the results through standardization, visualization, information system and other measures. In this study, the incidence of USC was kept at about 2.5% in the past three years, indicating that the improvement of this project was successful.
In conclusion, Lean Six Sigma was an effective way to reduce the rate of USC. This project was successfully promoted to provide reference for other cross-departmental operational issues in hospital.
Both Lean and Six Sigma were originated from manufacturing and had great advantages in eliminating waste and controlling volatility. At present, with the increase of patient demands and the deepening of payment reform, medical organizations should constantly pursue the balanced development of quality, cost and speed. The application of Lean Six Sigma in the service industry has great potential.
The implications of this study for hospital management are as follows: First of all, consensus among process stakeholders is the basis for solving problems. Secondly, the organization should create a culture focusing on customers, eliminating waste, optimizing processes and pursuing perfection, which guiding the behavior habit of employees. Thirdly, education and training should be carried out to improve staff’s ability to solve practical problems with lean, six sigma and other management tools.
However, this study has some limitations in providing evidence. Since some improvements were implemented simultaneously, the contribution of single improvement to the reduction of the incidence of USC cannot be calculated. The reasons for surgery cancellations were inquired from the surgeon and recorded in the system by the operating room nurse, which was possibly introduced a bias for data collection. The existing data could not accurately provide the proportion of USC for each type of reasons, nor could it do multivariate logistic regression analysis. However, these limitations could be usefully addressed in future studies applying Lean Six Sigma to improvement and innovation activities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the project of Taizhou science and technology bureau (1701KY19).