
Abstract
Reporting healthcare quality has become an important factor in healthcare delivery. Prior research has shown that patient-consumers do not frequently use information on websites reporting physician quality to guide their choice of physicians. Our aim is to understand the contextual and personal characteristics that influence patient-consumers’ decisions to trust or ignore information sources about healthcare quality. We use data from Finding Quality Doctors: How Americans Evaluate Provider Quality in the US, 2014, to examine factors that explain trust in sources reporting healthcare quality provided by physicians. Using factor analysis, 3 overarching information sources were identified: (1) employers and healthcare providers; (2) user advocacy sources; and (3) insurance companies and government. We use multiple regression analysis to understand the factors that impact trust in these 3 information sources. Our study found that contrary to previous findings, health status was not a significant factor that affects trust in sources reporting care quality data. Also, age was the only factor that significantly correlated with trusting information from all 3 sources. Specifically, younger adults trusted information from all sources compared to older adults. Furthermore, political affiliation, employment status, income, and area of residence correlated with trusting care quality information from either companies and government agencies or family and social network sources. Results suggest that individual and contextual characteristics are significant factors in trusting information sources regardless of health status and these should be taken into consideration by those promoting public reporting of healthcare quality information.
Prior research has shown that patient-consumers do not frequently use information on websites reporting physician quality to guide their choice of physicians. However, these findings are inconclusive.
Our aim is to understand the contextual and personal characteristics that influence patient-consumers’ decisions to trust or ignore information sources about physician quality. Results suggest that individual and contextual characteristics are significant factors in trusting information sources.
This study shows that sociodemographic characteristics, rather than health status of patient-consumers, account for differences in trust in sources providing data on care quality. This is advantageous to policymakers and other stakeholders interested in promoting understanding and use of healthcare information because sociodemographic characteristics are relatively easier to target for such promotions.
Introduction
According to the public, access to quality doctors is a primary concern when choosing a health plan.1,2 However, patients do not fully use resources available to them about provider quality. For instance, only 1 in 5 people have knowledge about websites that report information on healthcare provider quality and fewer still actually use these sites to search for a physician. 3 Patient-consumers are simply not using information on websites reporting physician quality to choose their physicians.4,5 A few American adults (about 11%) also use websites to review physician and provider rankings online in 2010. 6 This is counterintuitive because patient-consumers frequently use the Internet to access health information but rarely to find care quality information. 7
However, some researchers believe that empowering consumers with data on care quality will force lower quality physicians and hospitals to improve their practices and help reduce healthcare costs. 8 Thus, making data on care quality readily available and accessible to consumers and understanding influences on trust in sources that provide these data are important issues to explore. In this study, we examine the factors that explain trust in sources reporting physician care quality. Our aim is to understand the contextual and personal characteristics that influence patient-consumers’ decisions to trust or ignore information sources about healthcare quality.
Literature Review
Numerous sources are available for information on care quality, notably formal sources such as employers, healthcare providers, and government sources or informal sources such as families and friends. These sources emphasize different quality indicators, focusing on either concrete data such as experience or education or on subjective data such as interpersonal skills. Each patient assesses physician competency in a different way. 9 Assessment measures of physician competency generally covers 5 core domains which are: patient care; medical knowledge; professionalism; systems-based practice; practice-based learning and interpersonal and communication skills.10,11 The quality of physicians is an important factor in the consideration of a health plan among Americans, 1 however, different factors determine how consumers trust the sources of information on physician quality of care. While the data set used for this paper did not directly provide a working definition of trust, we belief that the underlying definition of trust is feeling that gives the ability to move on and do something in the immediate future with information gathered or at hand. 12 In this paper, trust also conveys the belief in the accuracy of the information at hand. Thus, participants seeing ratings of physicians from different sources will be able to use this information and make appropriate health decisions.
Previous research suggests that patients trust recommendations given by healthcare professionals and doctors when selecting a physician and/or healthcare plan but trust in employer advice is more suspect.1,13 Sinaiko et al 5 found that recommendations from physicians ranked second to friends and family. Several studies have noted that employer report cards are among the least trusted information sources on care quality.13,14 This is likely due to the perception that employers’ goal is to lower health care costs compared to ensuring high quality care for their employees. However, these findings are inconclusive. For instance, Feldman et al 15 reported that most employees in their study found information provided by their employers trustworthy and valuable. Isaacs 1 found that respondents would turn to a benefits manager at their workplace to recommend a physician more often than any other source aside from family and friends. It is important to note that employer recommendations are only relevant for people whose employers provide a health plan.
Family and friends are the most trusted and most frequently used resource for information on care quality. 16 In the past, some claimed that formal information sources were not readily available,17,18 but with the additional public reporting and patient-based rating websites, this is no longer a valid statement in most cases. Alternative explanations are that formal sources are less trustworthy,1,13 too complex 19 or that consumers do not want to devote sufficient time to choosing the “best” physician by perusing all available resources. 20
The importance attached to word-of-mouth recommendations is mirrored by the emphasis placed on patient comments when using patient-based ratings websites. 20 As it stands, most US adults know about patient-based rating websites, but, according to a study by Hanauer et al 21 only about a quarter actually use the websites and, a still smaller fraction either select or avoid physicians due to patient reviews. Those most likely to use rating websites include younger, better-educated individuals with higher incomes. 22 In part, the reluctance to use patient-based rating websites may be because patients are not primed to think about rating websites when selecting a physician. Fanjiang et al 23 found that patients were more likely to use rating websites if they were targeted during the time they were making a healthcare decision. According to Gray et al, 24 online ratings do not correspond to traditional care quality measures and the ratings may influence consumers in unexpected ways. For example, Li et al 25 found that there was a “primacy effect,” in that the willingness to use a physician’s services depended on when negative reviews were presented. Essentially, those who read negative reviews prior to positive reviews were less likely to select that physician. However, Grabner-Kräuter and Waiguny 26 found that consumers do not trust all reviews equally. While reading, the individual tries to assess the rater’s credibility and use the review appropriately. Additionally, some patients rate only physicians with whom they have had a negative experience. 27 Nonetheless, government reports are often viewed as the least trustworthy and insurance companies rank only marginally higher. 1
Previous research has indicated that trust in physician quality information cannot be assumed and is likely to vary depending on potential user’s characteristics and the context in which the information is received.28-31 For example, Blacks are more likely to trust provider and institutional sources compared with their White counterparts. 13 Older individuals tend to believe that providers have more reliable information and accurate knowledge. 32 This may suggest that there are groups that are comfortable with publicly reported information regarding physician quality, while others may require intensive efforts to bring them into the consumer mode. 13 Older and low-income workers are more likely to use information from advertisements. To the degree that such information is not accurate, these workers might be influenced by misleading advertisements. 15 Additionally, patients with chronic health conditions or recent hospital stays are more likely to consult formal information sources, and those who have had bad experiences with a physician may be more likely to seek more objective information. 33 Racial and ethnic minorities are substantially less likely than their White counterparts to seek information about doctors from family and friends, with Hispanics 14.3 percentage points less likely and Blacks 23.4 percentage points less likely. Hispanics and Blacks are more likely than Whites to use formal information sources while “others” are more likely than Whites to consult individual doctors. 34
While previous research helped advance the discourse on how sources reporting physician care data are utilized by patient-consumers, only one study by Alexander et al 13 specifically ascertained what determines trust in these data sources. However, the study focused on only people with chronic illness and findings may not be applicable to people without a chronic illness. In fact, people with chronic illness are more dependent on health care providers and feel uncertain about their health outcomes relative to their counterparts with no chronic health issues. 33 Thus, the health information preferences of people with chronic health conditions are significantly different. 13 They also have frequent interactions with the health care system. Trust may be particularly important in this context. 35 The present study examined factors that correlate with trust in physician quality data from different sources among people with chronic health conditions and those without, using a national sample of Americans aged 18 and older. In fact, people with a chronic health status may exhibit different behaviors regarding trust in care quality data from different sources relative to those who are healthy because their “needs may be unique” (p. 423). 13
Data and Methods
Data are from Finding Quality Doctors: How Americans Evaluate Provider Quality in the US, 2014, a nationally representative sample (n = 1002) of people aged at least 18 years old. The survey was funded by the Robert Wood Johnson Foundation and conducted by the Associated Press-NORC (AP-NORC) Center for Public Affairs Research at the University of Chicago in 2014. 36 Our study is a secondary analysis of this data set. Further information on the data collection can be found at https://apnorc.org/projects/finding-quality-doctors-how-americans-evaluate-provider-quality-in-the-united-states/
Outcome Measures
The outcome variables were trust in 12 different sources rating physician quality. These are:
(1) patients
(2) one’s regular healthcare provider
(3) doctors’ groups or other healthcare providers
(4) newspapers or magazines
(5) health insurance plans
(6) friends or family members
(7) employer or someone who deals with health benefits
(8) federal government agencies
(9) state government agencies
(10) free ratings websites such as Health Grades.com or Yelp
(11) paid subscription ratings websites such as Angie’s List, and
(12) community or advocacy groups.
Participants reported how much they trusted information from each source above. The response for each item is a Likert type scale that describes how much one trusted the source that provides physician quality ratings ranging from 1 = completely trust to 5 = not at all. We reverse coded the items such that 5 = completely trust in a source and 1 = do not trust at all. Under this scheme, higher scores correspond to higher trust levels. We simplified the data using factor analysis on the 12 different sources. This analysis generated 3 factors for analysis based on eigen values equal to or greater than 1. The values of these factors are the factor scores generated in the analysis thus making each one a continuous variable.
The first factor simply called “insurance companies and government agencies” grouped together health insurance plans, federal government agencies, and state government agencies. The second factor labeled “family, community, and media sources” has 6 items (patients, friends or family members, free rating websites, paid subscription ratings, community or advocacy groups, and newspapers or magazines). The last factor, called “health provider and employer sources,” has 3 items (doctors’ groups or other healthcare providers, one’s regular healthcare provider, and employer or someone who deals with health benefits).
Predictor Variables
Our main consideration was to assess whether there was a difference in trusting data sources on physician quality between respondents with chronic illness and those without. The presence or absence of a chronic health condition was self-reported by respondents in answer to the question: Are you currently receiving regular medical treatment or making regular visits to a doctor for any chronic health problem, or not? No follow-up questions assessed the number of chronic conditions or the type, severity, or duration of the chronic condition for respondents who answered in the affirmative.
Based on findings from prior research, we then adjusted for variables expected to correlate with trusting information sources on physician quality. Race, income, age, education level, political affiliation, employment status, region and area of residence, marital status, and sex were the independent variables in the analysis. We hypothesized that:
(1) Trust in sources reporting quality care data will depend on respondents’ health condition. Specifically, people with chronic health conditions will have more trust in different sources relative to those with no chronic health conditions.
(2) Consumers’ social and demographic characteristics will significantly affect their trust in sources that report quality data.
Analysis
We conducted OLS regression analysis to assess how the independent variables affect trust in provider quality data separately for the 3 factors generated by the factor analysis described earlier. To test the first hypothesis, respondents’ health status (whether or not they are receiving medical treatment for chronic problem) was regressed on each dependent variable, namely, trust in (1) insurance companies and government agencies; (2) family, community, and media sources; and (3) health provider and employer sources. Then, we included all the other independent variables in the regression analysis to test the second hypothesis.
Results
Table 1 presents descriptive statistics about the sample. Almost half the sample was female (49.4%). Most study participants were non-Hispanic White (72.8%) and almost a third earned less than $30 000 as household income. While over half (about 53%) were in full or part-time employment, almost 47.0% were not employed. About a third (30.3%) were college graduates or had attended graduate school with no degree. Study participants were mostly married or cohabiting (53.7%) and over 40.0% resided in suburbs. About 41% reported receiving treatment or seeing a doctor for a chronic ailment while nearly 59% did not report having a chronic condition.
Sociodemographic Characteristics of Respondents.

Table 2 presents regression results for trust in quality ratings from insurance companies and government agencies. Participants’ reported health status did not significantly affect trust in insurance companies and government agencies that report quality care (Model 1). Even with controls for the socio-demographic variables (Model 2), respondents’ health status remains non-significant. Model 2 however reveals that income level, age group, political affiliation, and area of residence significantly increased trust in quality ratings from insurance companies and government agencies. For example, compared to people who earned at least $100 000, people who earned between $75 000 to under $100 000 trusted these sources more (P = .03). Also, younger people aged 18 to 29 and 30 to 39 years trusted insurance company and government agency sources more than their older counterparts aged 65 years and over (respectively, (P = .00 and P = .04) as did Democrats over those with no political affiliation and rural residents over suburban residents.
Regression Models of Trust in Insurance Companies and Government Agencies Reporting Quality of Care of Physician Data.

P < .05. **P < .01. ***P < .001.
Table 3 shows that receiving regular medical treatment for chronic health problems significantly reduced trust in ratings from family, community, and social network sources (Model 1). However, the significant effect disappears when socioeconomic and demographic variables are controlled (Model 2). Age and political affiliation significantly affect trust in family, community, and media sources. In fact, younger people (18-29; 20-29; 40-49; 50-64) trusted ratings from family, community, and social media sources more than those aged 65 and above. Those who self-identified as independent trusted these sources more than those who did not belong to any political group.
Regression Models of Trust in Family, Community, and Social Network Sources Reporting Quality of Care of Physician Data.

P < .05. **P < .01. ***P < .001.
Only one variable significantly affected trust in ratings from healthcare provider and employer sources as shown in Table 4. People aged 18 to 29 trusted healthcare provider and employer sources, more than their counterparts aged 65 and above (P = .013).
Regression Models of Trust in Healthcare Provider and Employer Sources Reporting Quality of Care of Physician Data.
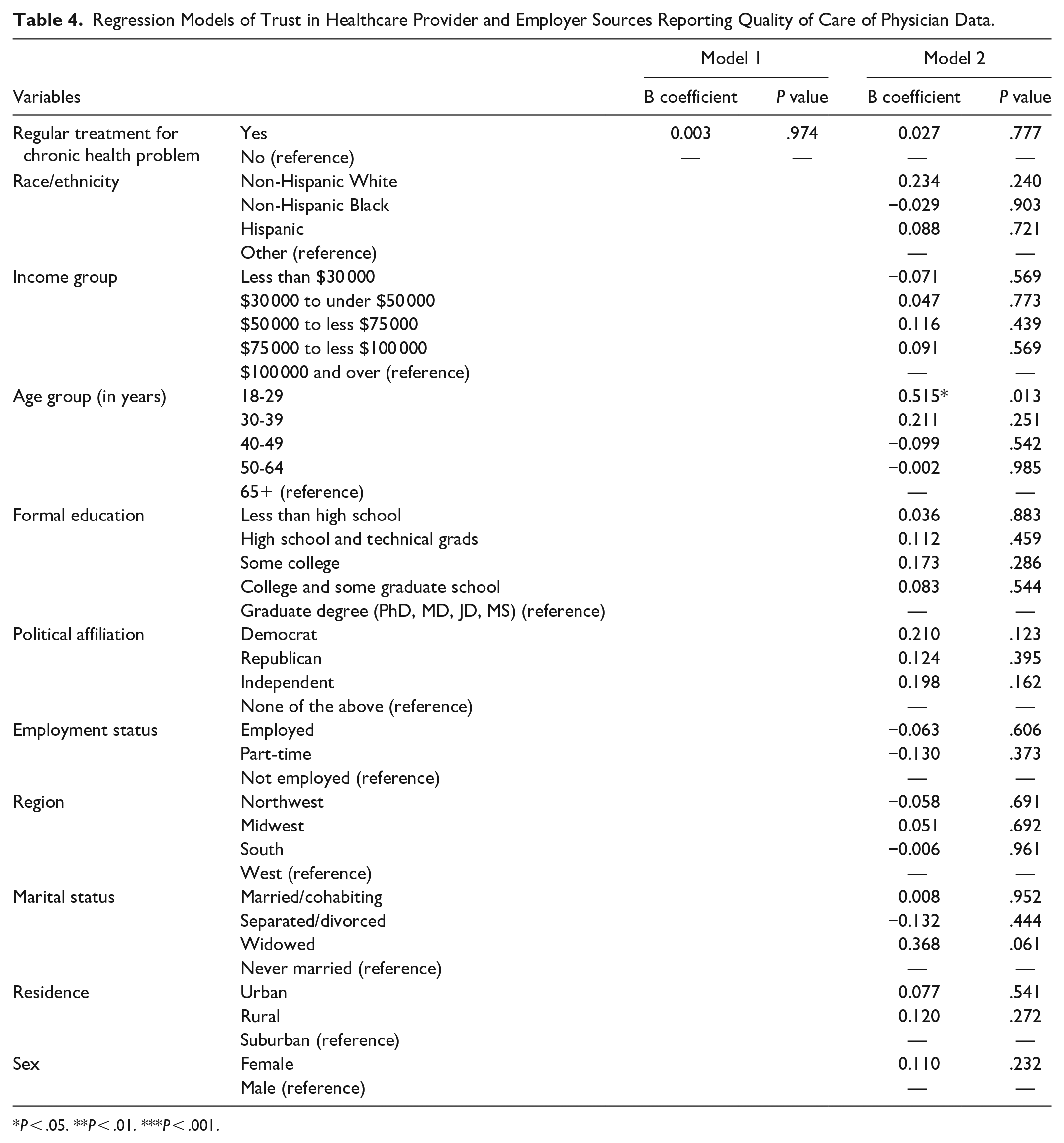
P < .05. **P < .01. ***P < .001.
Discussion and Conclusion
We used data from Finding Quality Doctors: How Americans Evaluate Provider Quality in the US, 2014, a nationally representative sample, to examine factors that explain trust in sources reporting care quality among physicians. We investigated whether trust in these sources vary by health condition and if consumers’ socio-demographic characteristics and political affiliation influenced trust in sources. Several findings need to be emphasized. First, different patient-consumers groups trusted different sources that provide data on care quality. This means that all sources are not equal from consumers’ perspectives. For instance, people aged 18 to 29 years, have more trust in all the sources that report data relative to people aged 65 and above. However, all the age groups trusted family, community, and social network sources relative to consumers aged 65 and above. This finding may reflect a generational difference. As observed by some studies that have examined declining trust and confidence in others and America’s public institutions,37,38 the decline may be mainly a period effect as all generations are losing trust and confidence in institutions. However, a generational difference is also apparent “with Boomers expressing the lowest confidence in institutions” 37 than their progeny, Generation X and Millennials. Thus, the age effect we found in this study may not mean that younger generations actually trusted these information sources but rather that their mistrust is not as deep compared to the older generation. Also, the results for political affiliation for the 3 factors clearly reveal the biases inherent in political ideology about personal responsibility and government’s role in matters related to healthcare. While respondents who identified themselves as Democrats significantly trusted information provided by insurance companies and government agencies, people who identified themselves as Independent rather trusted community, and social network sources. This generally fits the expectation that Democrats would be more likely to trust the federal government and more positively view government data compared to others such as Republicans 39 who would be least expected to have faith in government provided information. Nonetheless, it is important for healthcare policy makers to be aware of these findings and devise strategies to educate consumer-patients not only to be aware of their own biases but also on how data sources are created and the importance of trusting these sources. Otherwise, the underlying goal of public reporting of provider quality data to encourage consumers to select healthcare providers that offer comparatively better-quality care will be defeated.
Additionally, contrary to hypothesis 1, we found that trust in sources providing care data was not affected by health conditions controlling for patient-consumers’ social and demographic characteristics. This is contrary to a premise by Alexander et al 13 which is that people with a chronic health status will exhibit different behaviors regarding trust in quality care data relative to those who are healthy because their “needs may be unique” (p. 423). While the health information seeking behavior may be different between people with and without chronic health conditions, people with chronic health conditions tend to be older 40 and trusting those sources that provide physician quality data may be a different issue. Thus, this study shows that sociodemographic characteristics, rather than health status of patient-consumers, account for differences in trust in sources providing data on care quality. This is advantageous to policymakers and other stakeholders interested in promoting understanding and use of healthcare information because sociodemographic characteristics are relatively easier to target for such promotions. Messages can be tailored for various groups based on these characteristics to greater effect.
A few limitations need to be reported. First, data are cross sectional and we cannot infer causation. Second, the data set did not provide a specific definition of trust. This is assumed. Third, neither differences in severity of chronic health conditions nor the duration of conditions among study participants were assessed. Lastly, data are self-reports, and there may be issue with social desirability and recall. Despite these limitations, this study adds to the discourse on availability and use of provider quality data. By making care quality data readily available and accessible to consumers, healthcare providers with low-quality ratings will be obliged to improve the care they provide. Also, as health system strives to put consumers at the center of health decision-making, having health care quality data will assist both consumers and providers. This will ultimately improve care quality in general. However, studies indicate that patients are not utilizing these data.4,5 One reason is that some patient-consumers do not trust the sources that report these data in keeping with declining trust in public institutions. Hence, it is important that stakeholders inquire the reasons for distrust in the different ratings sources and then develop targeted programs to educate the specific groups. For instance, older people may have certain values and norms that make them distrust the rating sources. Ascertaining what these values and norms are will allow stakeholders to develop appropriate programs that will educate older Americans to understand how important the rating sources are and reasons these sources should be trusted and used. More research, both qualitative and quantitative, is needed to understand patient-consumer behavior toward trusting rating sources, especially, ways to improve trust level among consumers. Qualitative research should focus on different groups and reasons why they trust or distrust sources reporting quality care data. Isolating the characteristics that influence trust in information sources is only one part of the challenge. The other part is understanding the reasons for not trusting available information.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Secondary data set is used for the study.