
Abstract
The federal United States government supports the Patient-Centered Medical Home (PCMH) model to improve American’s access to quality healthcare. Healthcare access in the Southern United States is especially problematic given its high rurality, hospital closure rate, number of medically underserved areas, and older adult population. This study explored older adults’ ability to obtain health services and PCMHs’ impact on reducing healthcare access disparities in rural areas. Adults 65 and older were surveyed using a modified version of the Commonwealth Fund’s Health Care Quality Survey (N = 746). Analyses included t-test, ANOVA, crosstabulation, chi-square, and multiple linear regression. A significant relationship was found between healthcare access and care source, with PCMH users more likely to report access than persons with a regular care source. PCMH use was also significantly associated with gender, age, income, urban-rural status, health status, and local healthcare quality satisfaction. PCMH accreditors should target rural areas with high rates of older adults, poverty, chronic disease, and poor healthcare quality to minimize healthcare disparities.
Keywords
Highlights
● Healthcare access in the Southern United States is especially problematic given its high rurality, hospital closure rate, number of medically underserved areas, and older adult population.
● Adults 65 and older were surveyed using a modified version of the Commonwealth Fund’s Health Care Quality Survey (N=746) to explore the Patient-Centered Medical Home (PCMH) model’s impact on reducing healthcare access disparities in rural areas.
● A significant relationship was found between healthcare access and care source, with PCMH users more likely to report access than persons with a regular care source.
● PCMH use was also significantly associated with gender, age, income, urban-rural status, health status, and local healthcare quality satisfaction.
● PCMH accreditors should target rural areas with high rates of older adults, poverty, chronic disease, and poor healthcare quality to minimize healthcare disparities.
Introduction
Despite living in one of the world’s most developed nations, Americans often struggle to access healthcare. Financial barriers, like cost and insurance coverage, impact healthcare access in the United States; however, rural Americans experience other substantial challenges in receiving care. Most notable is the lack of healthcare providers, with nearly 80% of rural America medically underserved. 1 Although 20% of the United States resides in a rural area, only 10% of physicians practice there. 2 This situation is complicated by the fact that half of the physicians practicing in rural areas are over 55, 3 with these physicians’ impending retirement occurring in the next 20 years. Fewer rural healthcare providers mean increased healthcare costs, reduced continuity of care, delayed responses to healthcare needs, and worse health outcomes. 4
Differences in health outcomes illuminate limited healthcare access among rural Americans. Rural Americans experience profound health disparities compared to urban Americans, including having higher rates of cancer, obesity, cardiovascular disease, high blood pressure, hypertension, high cholesterol, and stroke. 5 Lower preventative medicine use 6 and less health service access 7 might be why rural areas see higher rates of chronic disease. 5
Individuals in rural areas are more likely to die from preventable causes, such as respiratory disease and unintentional injury, 8 with access to high-quality healthcare becoming increasingly challenging the more isolated and impoverished a rural community. 9 Rural status is one of the strongest predictors of mortality, 10 with rural residents dying 2 and a half to 5 years earlier than urban residents. 11 Ultimately, while the rural populace has decreased, older adults in these areas have grown. 12
Southern Healthcare Access
Almost half (46.7%) of Americans residing in rural areas live in the South, 13 which is concerning as healthcare access in the Southern United States is particularly problematic. When looking at America’s South, including Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Mississippi, North Carolina, South Carolina, and Tennessee, nearly half of residents do not have their healthcare needs met, with over 20 million people (22 439 881) living in a primary care health professional shortage area. 14 Additionally, 70% of the states with the worst healthcare are located in the South. 15 Community-level factors exacerbate rural healthcare access, though individual-level factors, like more uninsured and underinsured residents and less engagement in care, 16 likely play a part.
Patient-Centered Medical Home
The Patient-Centered Medical Home (PCMH) model is supported by the United States government to address healthcare access and was developed out of a need for a cost-effective and accountable healthcare system. 17 Various medical home model iterations exist; however, the National Committee for Quality Assurance is the United States’s leading PCMH accreditor. Though minor differences exist between models, the National Committee for Quality Assurance PCMH is grounded in team-based care, knowing and managing patients, patient-centered access, care management, care coordination, performance measurement, and quality improvement. 18
PCMHs can improve population health, 19 healthcare quality, service use, health outcomes, cost, 18 primary care delivery, staff and patient satisfaction, healthcare system efficiency, 20 and chronic disease management. 21 Provider organizations, third-party payers, and the United States government, including the Health Resources Services Administration 22 and Centers for Medicare and Medicaid Services, 23 incentivize primary care providers to gain PCMH recognition with financial and technical support.
Twenty-four percent of adults 65 or older live in rural areas, 24 with older adults being the United States’s largest primary care consumers. PCMH’s continued success depends on delivering high-value healthcare to a rapidly aging population. 25 Although the PCMH model’s widespread support is apparent, its benefits are not. PCMH research discrepancies and limited exploration into its impact on rural and older populations necessitated examining the model’s ability to minimize access disparities in the Southern United States, given their distinct needs and circumstances, namely its geography, demography, and limited health services.
Theoretical Perspective
This study was grounded in Penchansky and Thomas’ 26 Theory of Access, which posits that 5 factors influence a person’s entry into and compatibility with their local healthcare system: availability (number of and types of practice), accessibility (location in relation to services, such as distance to travel), accommodation (how resources are organized to accept patients), affordability, and acceptability (patient’s perceptions of providers and facility characteristics and actual characteristics and the decision to accept services). 27 These interrelated components affect healthcare satisfaction and use, with a deficit in any factor affecting service use. 26
Study Aims
Informed by a 2007 study by Beal et al, 28 which showed that combined with health insurance, medical homes eliminate healthcare access disparities for racial and ethnic minorities, this current study asked, “Do PCMHs minimize healthcare access disparities for older adults living in rural Georgia?” “What access differences exist between older adults using a PCMH and those using other forms of healthcare?” and “What differences in healthcare access exist for older Georgians living in rural and urban counties?” Beal and colleagues defined medical homes as “a healthcare setting that provides patients with timely, well-organized care, and enhanced access to providers” (p. 1). 28 Since their study was published, the American College of Physicians, American Academy of Family Physicians, American Osteopathic Association, and the American Academy of Pediatrics established the Joint Principles of the Patient-Centered Medical Home 29 ; hence, this study used the term PCMH.
Georgians were selected as the study population as Georgia is over 75% rural 30 and has the second fastest-growing older adult population in the South. 31 In fact, 19.0% of rural Georgia’s population is 65 or older, with a 22.0% increase expected by 2030. 32 Additionally, Georgia ranks eighth for most Health Professional Shortage Areas in a state, 33 and is tied for third for most hospital closures 34 and most rural hospital closures between 2012 and 2022. 35 These factors might contribute to Georgia’s 46 of 50 ranking on quality healthcare access. 36 As such, as of 2024, 262 Georgia practices have committed to increasing healthcare quality by becoming a National Committee of Quality Assurance-accredited PCMH. 37 Given that this study examined older adults’ access to quality healthcare in the rural South, Georgia was an appropriate state to sample.
Methods
Sample Selection
The Commonwealth Funds’ Health Care Quality Survey extends beyond a satisfaction survey and attempts to understand patients’ experiences with their healthcare providers. 28 The research team used a modified version of the Health Care Quality Survey, which was offered online and by phone to adults 65 and older living in Georgia. The 15-min Health Care Quality Survey was modified (with permission from the Commonwealth Fund) to capture older rural residents’ access to care, adding questions from the National Health Interview Survey and Behavioral Risk Factor Surveillance Questionnaire, among others.
A purposive sample of at least 384 Georgia residents 65 and older were surveyed on perceptions of healthcare access and healthcare quality and various health-related items over a 3-month period during the Summer of 2022. This proposed sample was determined by applying Georgia’s older adult population (1 638 000) to the American Research Group’s Sample Calculator with a 5% margin of error. The collection of at least 384 responses ensured the sample was adequately powered for an effect size of 0.01. Exclusion criteria were if someone was under 65 years old, did not live in Georgia, had moderate to late-stage Alzheimer’s Disease or dementia, or who resided in a residential care facility. Participants were recruited with social media advertising and outreach to aging and rural-based organizations, researchers, rural county public health departments, Area Agencies on Aging, and community partners. Older adults’ increased use of Facebook 38 and its value in health research recruitment 39 spurred using social media advertising to target older Georgia Facebook and Instagram account holders.
A consent form was embedded into the survey and explained the study’s purpose and that no known risks were associated with completing the survey. Potential respondents were also notified that the survey was configured to collect responses anonymously by excluding IP addresses.
Measures
Beal et al used the following indicators of a medical home user: a regular source of care; healthcare office visits that are “always” or “often” well organized and running on time; the ability to communicate with a doctor by email [or patient portal]; and “not being too hard” or “not hard at all” to contact their provider by phone and get care or medical advice in the evening or on weekends. 28 Other individuals were considered “regular care source” users unless they indicated having no regular care source, and then were recoded as “no care source.” Healthcare access was determined as in the study by Beal et al 28 : “Thinking about your healthcare in general, how often do you receive the healthcare you need WHEN you need it?” Additionally, participants’ urban-rural status was based on county population, with counties having over 50 000 people considered urban and under 50 000 deemed rural. 40
Additionally, some demographic variables were recoded. Age was grouped into 3 categories: between 65 and 74 (youngest old), 75 and 84 (middle old), and 85 and older (oldest old). 41 Race was dichotomized to include Caucasian and any race other than Caucasian. Similarly, sexuality was recoded as heterosexual and any sexuality other than heterosexual. Annual household income responses were recoded as less than $30 000, $30 000 to under $60 000, and $60 000 or more. Further, educational attainment was recoded as high school or less, some college/technical college or trade school/associate degree (“some college”), bachelor’s degree, and a master’s or advanced degree (ie, PhD, MD, JD, PharmD). Variables used in the analysis but not recoded were gender, urban-rural status, care source, self-described health status, and local healthcare quality satisfaction.
Analysis
T-test and ANOVA identified bivariate differences in individual items of healthcare access and the independent variables mentioned above, and chi-square examined bivariate associations between individual items of PCMH use and the same variables. Crosstabulation also assessed whether PCMH use minimized healthcare access disparities for rural-residing Georgians, and multiple linear regression determined significant differences in healthcare access, controlling for several independent variables. Analyses were re-run numerous times by different team members to ensure completeness and accuracy of the data.
Institutional Review Board Approval
This study followed SQUIRE guidelines 42 and was approved by the University of Georgia’s Institutional Review Board (#00004713) on 10/06/2021, and the authors declare no ethical dilemmas.
Results
Data collection occurred in the Summer of 2022, and the analyses were conducted promptly after. In total, 783 older adults living in Georgia responded to the survey; however, 37 responses (4.7%) were omitted since they were less than 20% complete, with these questions necessary for the analyses since they established PCMH status.
Sample Characteristics
Table 1 shows a list of sample descriptives. Of the total analyzed sample (N = 746), 72.0% were female, 27.4% were male, and 0.6% identified as another gender. Additionally, 63.4% of the sample was between 65 and 74 years old, 31.5% were between 75 and 84, and 5.1% were 85 and older. Respondents were also overwhelmingly Caucasian (93.2%). Responses to household income included less than $30 000 (21.1%), $30 000 to under $60 000 (29.2%), and $60 000 or more (49.7%). Regarding urban-rural status, 58.6% of the sample lived in an urban county, and 41.4% lived in a rural county.
Sample Characteristics of the Entire Sample.

32.4% (n = 242) of the sample was missing either because they did not answer the question, did not live within 15 min of a doctor, or had not sought out local healthcare.
PCMH User Characteristics
A crosstabulation was also conducted to describe PCMH users’ characteristics (N = 158; Table 2). Overall, 21.2% of the sample was determined to receive care at a PCMH. Individuals with a non-PCMH regular care source or no regular care source made up 78.8% of the sample and were coded as non-PCMH users. The following results only describe PCMH users’ characteristics (N = 158). First, 100% of all PCMH users reported having insurance. This satisfies Beal et al.’s 28 condition that medical homes, when combined with having health insurance, eliminate healthcare access disparities for some populations (in their case, racial, and ethnic minorities). PCMH users predominantly resided in urban areas (69.6%), with fewer PCMH users living in rural areas (30.4%). PCMH users were also predominantly Caucasian (92.2%) and female (65.1%), which is in line with the collective sample. Further, PCMH users were younger, had higher incomes, and had more education.
Patient-Centered Medical Home User Characteristics.
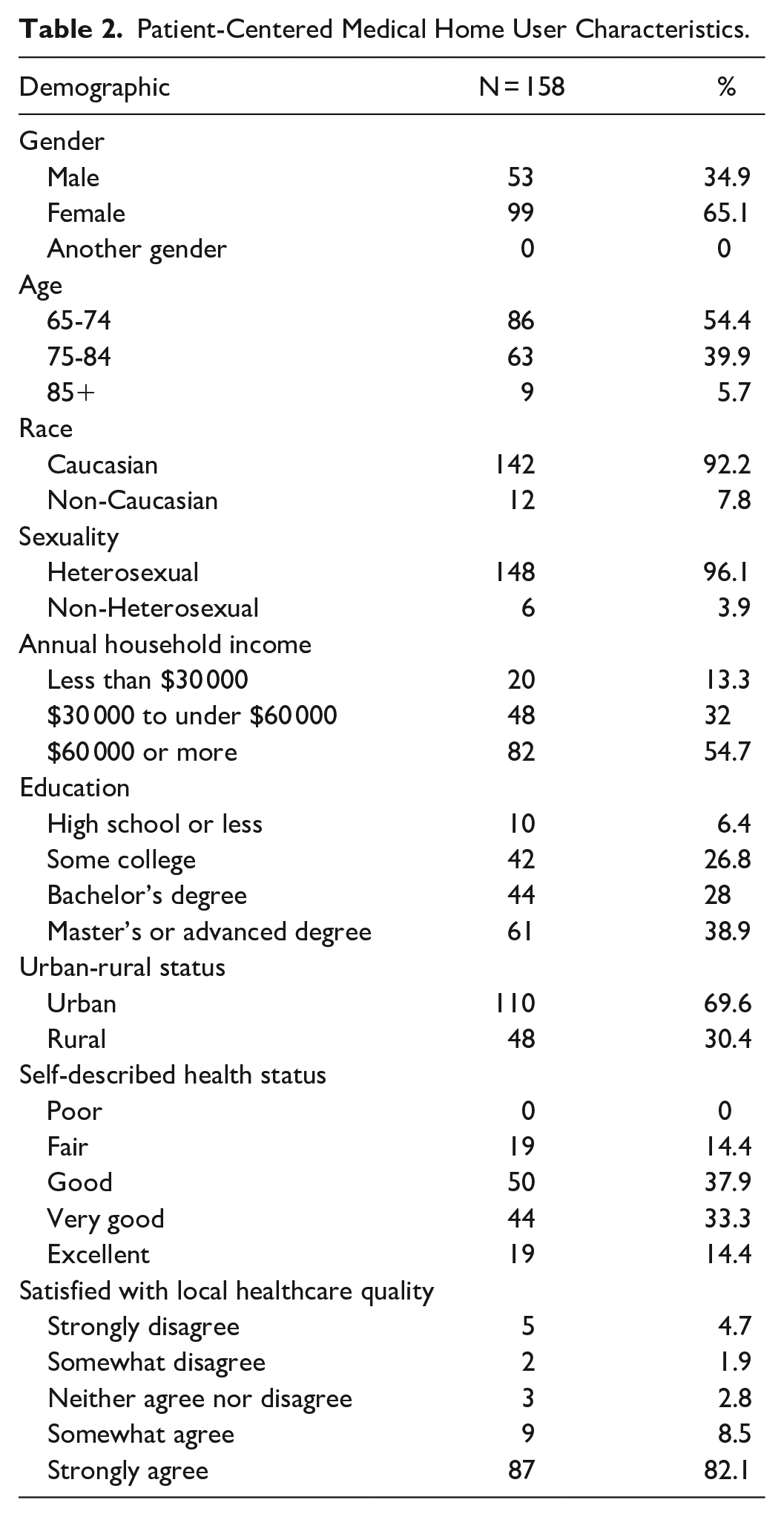
For instance, PCMH users mainly were between 65 and 74 years old (54.4%) and 75 and 84 (39.9%). Individuals 85 and older made up not only 5% of the total sample (N = 746) but 5.7% of the PCMH sample (N = 158). Likewise, only 13.3% of respondents with annual household incomes less than $30 000 were PCMH users, compared to 32.0% of respondents with incomes between $30 000 and under $60 000 and 54.7% of those with incomes of $60 000 or more. Similarly, educational attainment by PCMH users was determined as follows: high school or less (6.4%), some college/technical college or trade school/associate degree (26.8%), Bachelor’s degree (28.0%), and a Master’s or advanced degree (PhD, MD, JD, PharmD, or another advanced degree; 38.9%). Finally, within PCMH users, 0.0% reported being in poor health, 14.4% reported being in fair health, 37.9% reported being in good health, 33.3% reported being in very good health, and 14.4% reported being in excellent health.
Bivariate Associations with Healthcare Access
Healthcare access was higher for Caucasians (4.27 ± 0.85) than non-Caucasians (4.18 ± 1.07), heterosexuals (4.28 ± 0.86) than non-heterosexuals (4.12 ± 0.88), and urban (4.30 ± 0.82) than rural residents (4.20 ± 0.93), though t-test determined no significant group differences were found (Table 3). Additionally, crosstabulation showed that individuals with a regular care source reported “always” receiving medical care more than PCMH users, regardless of living in an urban or rural area (Figure 1). Among respondents “always” getting necessary care, 58.0% of urban respondents were regular care source users compared to 70.5% of rural respondents. Urban areas also had higher rates of PCMH users compared to rural areas. Nearly half of the respondents from urban areas were PCMH users (41.6%), relative to rural respondents (28.1%). Further, few urban and rural residents without a care source reported “always” receiving needed medical care (0.5% and 1.4%, respectively). Chi-square showed significant associations between care source and urban-rural status when examining responses from individuals “always” receiving care when needed, χ2 (2) = 7.48, P = .02.
Associations with Access to Healthcare.

Note. Age, annual household income, care source type, educational attainment, satisfaction with local healthcare quality, and self-described health status were analyzed with ANOVA. Gender, race, sexuality, and urban-rural status were analyzed with an independent sample t-test.

Percentage of older Georgians reporting “always” getting medical care when needed based on care source type.
Further, one-way ANOVA determined significant group differences in healthcare access and care source, gender, age, annual household income, educational attainment, self-described health status, and local healthcare quality satisfaction (Table 3). Healthcare access was statistically different for groups based on their care source, F(2, 67.54) = 111.90, P < .01, with access lowest for individuals with no care source (3.07 ± 1.17) and regular care source users (4.16 ± 0.85) and highest for PCMH users (4.82 ± 0.41). Post-hoc analysis showed significant differences in the increase from no care source to PCMH users (1.75, 95% CI [1.18, 2.31] (P < .01)), regular care source to PCMH users (0.67, 95% CI [0.55, 0.78] (P < .01)), and no care source to regular care source users (1.08, 95% CI [0.52, 1.65] (P < .01)).
Healthcare access also differed based on gender, F(2, 716) = 7.63, P < .01, with access higher for males (4.46 ± 0.81) than females (4.19 ± 0.87) and another gender (4.00 ± 0.82). Post-hoc analysis revealed significance only in the increase from female to male (0.27, 95% CI [0.11, 0.44]; P < .01). Statistically significant group differences in healthcare access also existed based on age, F(2, 102.07) = 7.33, P < .01. Healthcare access was lowest for individuals 65 to 74 (4.17 ± 0.91), higher for those 75 to 84 (4.42 ± 0.76), and lower for respondents 85 and older (4.37 ± 0.82). Post-hoc analysis found significance in the increase from 65 to 74 and 75 to 84 (0.25, 95% CI [0.09, 0.40], P < .01).
Additionally, there were significant group differences in healthcare access and annual household income, with access higher for respondents with incomes of “$60 000 or more” (4.41 ± 0.79) than “$30 000 to under $60 000 (4.23 ± 0.85) and “less than $30 000” (3.99 ± 0.98), F(2, 689) = 12.65, P < .01. Post-hoc analysis showed statistically significant differences in access when income increased from “less than $30 000” to “$30 000 to under $60 000 (0.24, 95% CI [0.02, 0.45], P < .05) and “less than $30 000” to “$60 000 or more” (0.42, 95% CI [0.22, 0.61], P < .01). There was also significance in the increase from “$30 000 to under $60 000 to “$60 000 or more” (0.18, 95% CI [0.01, 0.36], P < .05), “less than $30 000” to “$30 000 to under $60 000 (0.24, 95% CI [0.02, 0.45], P < .05), and “less than $30 000” to “$60 000 or more” (0.42, 95% CI [0.22, 0.61], P < .01). Finally, post-hoc analysis showed that the increase from “$30 000 to under $60 000 to “$60 000 or more” (0.18, 95% CI [0.01, 0.36]) was significant (P < .05).
Regarding group differences in healthcare access and education, access was highest for respondents with a master’s or other advanced degrees (4.38 ± 0.79), followed by a bachelor’s degree (4.28 ± 0.87), and some college (4.11 ± 0.92). However, the mean increased slightly for individuals with a high school diploma or less (4.19 ± 0.96), F(3, 732) = 4.41, P < .05. Post-hoc analysis determined that only the increase from some college to a master’s or another advanced degree (0.27, 95% CI [0.08, 0.47]) was significant (P < .05). Healthcare access also significantly differed when examining health status, F(4, 90.31) = 7.54, P < .01, with access increasing for individuals reporting their health as poor (3.88 ± 0.96), to fair (4.03 ± 0.96), to good (4.26 ± 0.85), to very good (4.46 ± 0.81), to excellent (4.58 ± 0.60). Post-hoc analysis showed that the increase from good to excellent (0.33, 95% CI [0.06, 0.60]) was statistically significant (P < .01), as was the increase from fair to excellent (0.55, 95% CI [0.22, 0.88], P < .01) and fair to very good (0.43, 95% CI [0.13, 0.72], P < .01).
Lastly, significant group differences were found in healthcare access and local healthcare quality satisfaction, F(4, 135.72) = 25.20, P < .01. Access decreased for individuals somewhat disagreeing with the statement, “I am satisfied with the quality of doctors who are located within a 15-min drive of where I live” (3.73 ± 0.90) when compared to those strongly disagreeing (3.82 ± 1.11). Further, access increased for individuals neither agreeing nor disagreeing (4.05 ± 0.86), to somewhat agreeing (4.17 ± 0.73), to strongly agreeing (4.65 ± 0.62). Post-hoc analysis showed that the increase from somewhat agrees to strongly agree (0.48, 95% CI [0.26, 0.69]) was statistically significant (P < .01), as was the increase from neither agrees nor disagrees to strongly agrees (0.60, 95% CI [0.22, 0.99], P < .01), somewhat disagrees to strongly agrees (0.92, 95% CI [0.56, 1.27], P < .01), strongly disagrees to strongly agrees (0.83, 95% CI [0.40, 1.27], P < .01), and somewhat disagrees to somewhat agrees (0.44, 95% CI [0.06, 0.82], P < .05).
Chi-square revealed statistically significant higher percentages of PCMH users being male (χ2 (2, N = 719) = 6.28, P < .05), between 75 and 84 years old (χ2 (2, N = 746) = 7.15, P < .05), having incomes of $60 000 or more (χ2 (2, N = 692) = 6.94, P < .05), living in an urban area (χ2 (1, N = 746) = 10.07, P < .01), reporting excellent health (χ2 (4, N = 641) = 18.13, P < .01), and strongly agreeing with being satisfied with the quality of local doctors (χ2 (4, N = 504) = 74.08, P < .01). Race, education, and sexuality were not significantly associated with PCMH use.
Multivariate Associations with Healthcare Access
Multiple linear regression was conducted using healthcare access as the dependent variable and the independent variables: gender, age, race, sexuality, income, education, urban-rural status, care source, health status, and local healthcare quality satisfaction (Table 4). Overall, males reported significantly higher levels of healthcare access in reference to females (B = 0.23, P < .05), and non-heterosexuals reported significantly lower levels of access in reference to heterosexuals (B = −0.38, P = .02). Furthermore, PCMH users reported significantly higher levels of access in reference to regular care source users (B = 0.34, P < .05) with persons having no care source reporting significantly lower levels of access in reference to persons with a regular care source (B = −0.61, P < .05). People in fair health also reported significantly lower levels of access in reference to people in excellent health (B = −0.30, P < .05).
Predictors of Healthcare Access.

Finally, a significant relationship was found between healthcare access and quality. People strongly disagreeing (B = −0.66, P < .05), somewhat disagreeing (B = −0.59, P < .05), neither agreeing nor disagreeing (B = −0.48, P < .05), and somewhat agreeing (B = −0.38, P < .05) with being satisfied with the quality of local doctors reported lower levels of access than respondents strongly agreeing. Multiple linear regression showed that age, race, income, education, and urban-rural status were not significant.
Discussion
This study assessed whether PCMHs minimized healthcare access disparities for older adults living in rural areas and attempted to understand if this model has the same benefits for rural and urban populations given its federal support. Several significant findings substantiating current PCMH research were revealed. For example, significant group differences in perception of healthcare access were found based on care source, with access highest for PCMH users, then regular care source users, and then individuals with no care source.
The difference between no care source and PCMH user was statistically significant, as was the increase from regular care source to PCMH user. A significant relationship was also found between healthcare access and care source, with PCMH users more likely to report access than persons with a regular care source. Such findings contribute to the literature on medical homes’ ability to improve healthcare access. Unfortunately, findings showed that rural residents were less likely to be PCMH users than urban residents despite the potential benefits for rural practices. For instance, PCMHs reduce hospital days, emergency room use, costs, and the need for outpatient specialty care, 43 all of which burden rural health practices. Thus, PCMH adoption might address healthcare access without increasing the number of rural practices.
Significant associations also occurred between PCMH use and gender, age, income, urban-rural status, health status, and local healthcare quality satisfaction. Findings showed fewer PCMH users were 85 and older, with incomes under $30 000, living in rural areas, in poor health, and less satisfied with local healthcare quality. Rural areas might benefit most from the PCMH model because their residents are lower income, in worse health, 44 and experience less access to quality healthcare 45 than their urban counterparts. Given that the number of Medicaid recipients is typically higher in rural areas and that the PCMH model can improve healthcare quality for Medicaid recipients, 46 PCMH implementation is a promising approach to improving rural residents’ healthcare quality. Such efforts are ignited by the Patient Protection and Affordable Care Act, which provides increased federal funding to states for medical homes serving Medicaid beneficiaries. 47
For example, in 2009, Montana received a technical assistance grant to advance the multi-payer PCMH Initiative, which expanded PCMH benefits to most children enrolled in Montana’s Medicaid and Children’s Health Insurance Program. 48 While 23 other states serve part of their Medicaid population through PCMHs, 49 more states could explore similar approaches. Rural practices’ shared PCMH aspirations, like improved quality, safety, outcomes, and cost reduction, 50 suggest buy-in to incorporating this model to improve access. Ultimately, assisting rural practices interested in adopting the PCMH model is essential to meeting rural resident’s health needs.
Figure 1 shows that regular care source users reported “always” getting medical care when needed more often than PCMH users, possibly because more respondents had a regular care source than received care at a PCMH. Also, although urban PCMH users reported “always” getting care more often than rural residents, rural residents with a regular care source reported “always” receiving medical care more often than urban residents. Shorter wait times for rural residents’ receipt of immediate care, like in emergency rooms, 51 might contribute to this finding. Regardless, receiving care when needed was substantially higher for PCMH users and regular care source users than for individuals with no care source.
Results also showed significant group differences in healthcare access based on age, particularly the increase from 65 to 74 and 75 to 84. More frequent use of health services by adults over 75 could explain why they have greater access than individuals under 75. Additionally, the group differences in healthcare access among household incomes and education levels are expected, given the relationship between educational attainment and job earnings. Since lower-income individuals experience worse outcomes 52 and the model can improve health outcomes, 18 this study sheds light on one way to address this issue. Ultimately, investigating how to address external factors related to social determinants of health can improve older adults’ access to care.
Significant relationships between healthcare access and gender, sexuality, health status, and satisfaction with local healthcare quality were also revealed. Significant differences in healthcare access based on gender were unsurprising since women often face substantial healthcare barriers, including affordability, accessibility, and insufficient education, research, and treatment. 53 Rapp et al 54 also attribute “state-level sexism in perpetuating gender disparities in healthcare” (p. 2). Additionally, non-heterosexuals reported less healthcare access than heterosexuals. Since heterosexuals are more likely to have a regular healthcare provider than sexual minorities, 55 these findings support the current literature.
People in fair health were less likely to report access than those in excellent health, possibly because someone in excellent or very good health might rate healthcare access higher if, by default, they access medical care less often. Such circumstances give fewer opportunities for individuals not to have access to healthcare, as substantiated by the United States Census Bureau, 56 which showed that individuals in excellent health visit healthcare providers less often than people in poor health. Finally, although physical access to health services is necessary, healthcare quality might be as important, given its potential to affect a patient’s overall health 57 and perception of local rural healthcare access. 58 Quality improvement efforts can improve health outcomes and access by increasing rural provider recruitment and retention. 59
Strengths
Given the PCMH model’s widespread adoption, assessing its potential to minimize disparities has substantial policy implications. 46 This study contributes to the empirical evidence on the PCMH model and points the National Committee for Quality Assurance and other accreditors to how they should support PCMH recognition. Because PCMH users reported healthcare access more often than non-PCMH users and significant associations existed between PCMH users and several sociodemographic variables (ie, gender, age, income, health status), health practices serving these underserved groups should be recruited for PCMH accreditation and notified about opportunities benefiting their communities. Because significant differences in access existed based on gender, sexuality, fair health status, and local healthcare quality satisfaction, support should target females, sexual minorities, people in fair health, and residents of areas with low healthcare quality ratings.
PCMHs decrease healthcare costs for payers and patients, 60 with 1 study showing Medicare savings of almost $1 100 per patient. 61 Long-term financial benefits possibly prompt the federal government’s support of medical home model recognition. For instance, the Health Resources and Services Administration assists health centers in enrolling in the PCMH recognition program for free to offset initial start-up and maintenance costs. 62
However, despite federal PCMH support, little research is specific to the Southeastern United States. As such, researchers and policymakers in the Southeast should consider these findings as results convey social determinants of health disparities within PCMH use and highlight sub-populations served by the model, representing a “high-value benefit to the healthcare system [with] the potential to reduce the long-standing socioeconomic disparities in health that continue to persist” (p. 2002). 63 The United States government is well-positioned to abate some of these issues by supporting PCMH access for rural residents and older adults. Additionally, financial and targeted support to providers in these areas could increase sustainable PCMH accreditation and activities. The Health Resources and Services Administration Accreditation and Patient-Centered Medical Home Recognition Initiative, which improves primary care coordination and ongoing quality improvement through PCMHs, 62 is only 1 example of such efforts. Others include the Safety Net Medical Home Initiative, which was a partnership between the Commonwealth Fund, Qualis Health, and MacColl Institute that “assist[ed] safety net primary care clinics in becoming high-performing PCMHs through partnerships between safety net providers and community stakeholders” (para. 35). 64 Widespread promotion of this initiative’s Change Concepts for Practice Transformation framework could provide needed support to practices desiring PCMH accreditation.
Limitations
This study’s primary limitation is its inability to determine causal effects associated with PCMHs given its correlational design. 65 Another limitation was the disproportionate number of female survey respondents, particularly since females report more healthcare access barriers. 54 Additionally, despite conducting outreach in racially and economically diverse counties in Georgia, other limitations include a primarily Caucasian and highly educated sample. The high percentage of individuals with post-bachelor degrees might contribute to 49.7% of the sample reporting an annual household income of $60 000 or more. Additionally, the literature shows that African Americans are less likely to participate in health research, 66 have little trust in the healthcare system, and express less confidence in doctors and hospitals than Caucasians. 67 Such factors could contribute to this study’s underrepresentation of African Americans.
Given the Southern United States’ demographics, this study has limited generalizability. Thus, a more diverse sample must be collected if this study is replicated since racial and ethnic minorities experience some of the most significant access barriers. 68 More males should also be surveyed for a more proportionate and representative sample. Further, although the survey was offered by phone, the participants exclusively used the online version. Hence, inherent bias might exist because higher-income respondents could have more access to the Internet or cell phones. Regardless, the number of older adults using the Internet 69 necessitated the online option. Additionally, the Health Care Quality Survey is an established instrument developed by the Commonwealth Fund. 70 With permission, some questions were eliminated and added to be more applicable to rural-residing older adults. However, the modified survey was piloted several times with various groups, including quantitative, rural, and public health experts, and older adults. Finally, while a strength of the analysis is that it is exploratory in nature, a follow-up action to this work is a more rigorous statistical analysis where associations are examined for a more comprehensive model to predict PCMH use.
Conclusions
The National Committee for Quality Assurance PCMH model is deemed a “tool for success” by the Rural Health Information Hub 71 and is supported by the Health Resources Services Administration, Centers for Medicare and Medicaid Services, and payers to improve healthcare quality and access. Rising medical costs and over 200 rural hospital closures across the United States 72 suggest that America’s healthcare crisis is growing and necessitated the exploration of whether deployed healthcare models, such as PCMHs, are appropriate for multiple populations. The Southern United States rurality and rapidly growing older adult demographic spearheaded this study on whether the PCMH model meets older adults’ healthcare needs. Findings suggest that rural areas with high rates of older adults, poverty, chronic disease, and poor healthcare quality should be targeted by PCMH accreditors to combat access disparities. Through directed PCMH support, healthcare access can be increased by enhancing the quality of already established rural practices. Ultimately, policymakers, researchers, and stakeholders can use this study to inform and expand PCMH implementation and rural health policy across America.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251335809 – Supplemental material for Patient-Centered Medical Homes: How the Federally Supported Model Minimizes Healthcare Access Disparities for Older Adults in Rural Areas
Supplemental material, sj-docx-1-inq-10.1177_00469580251335809 for Patient-Centered Medical Homes: How the Federally Supported Model Minimizes Healthcare Access Disparities for Older Adults in Rural Areas by Elisa M. Childs and Orion Mowbray in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author’s Note
The abstract for this study was previously published as part of the Gerontological Society of America’s conference proceedings in 2023.
Ethical Considerations
This study was approved by the University of Georgia’s Institutional Review Board (#00004713) on 10/06/2021, and the authors declare no ethical dilemmas.
Consent to Participate
Survey respondents provided consent to participate in this study.
Author Contributions
Dr. Elisa M. Childs established the concept behind the study and executed the survey, analysis, and write-up of the manuscript while preparing charts and references. Additionally, Dr. Orion Mowbray assisted with the analysis and manuscript development and preparation. Each author has revisited, approved, and endorsed this manuscript’s submission and assumes accountability for its accuracy and integrity in relation to the criteria set forth by ICME.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Access to this research’s data can be requested.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.