
Abstract
There is relatively little published on the socioeconomic distribution of chronic disease burden in older people. This study aims to quantify income-related inequalities in chronic disease situation among ≥45-year-old people in China. Data were collected from the 2015 China Health and Retirement Longitudinal Study. Self-reported chronic conditions included 14 diseases (ie, heart problem, diabetes). Multivariate Generalized Quasi-Poisson Regression was used to evaluate associations between prevalence and personal income. Prevalence of hypertension was highest among people above ≥ 75 (male participants 44.41%, female participants 47.53%). Heart problem prevalence increased with age. Chronic disease prevalence among population aged 45 to 59 years was greatly affected by income. Prevalence ratios (PRs) were highest for heart problems in 45 to 59 middle-income male participants and for memory-related diseases in 45 to 59 middle-income female participants. Significant inequalities in chronic conditions prevalence persist into old age, particularly among 45- to 59-year-old people. Opposite to developed countries, the prevalence of some chronic disease (ie, heart problem) is higher in richer populations in China. These findings pose the policy challenge of needing to prevent such inequalities in older years.
Previous studies on income-related inequalities in chronic conditions mainly focused on the developed countries; therefore, the results are not necessarily suitable for developing countries (ie, China).
We evaluated the differences in chronic disease prevalence among different age groups and income populations by using the 2015 China Health and Retirement Longitudinal Study data and found that China had its own situation.
This study provides implications on carrying out targeted policy intervention and health management for people of different health and income positions in China.
Introduction
China is facing serious aging problems. The size of the elder population aged ≥60 was 230 million in 2016 and reached 241 million in 2017, with an increase of 4.8% in 1 year. By the end of 2035, the size is expected to be 418 million.1,2 In China, approximately 33.8% of the elder population suffers from poor sleep quality 3 and 22.7% has depressive symptoms. 4 Moreover, the disease burden for the elder population is also increasing. 5
In recent years, the problem of chronic disease burden in China becomes increasingly serious, which has replaced the major position of infectious disease in the total disease burden and has displayed an increasing trend year by year.6-8 In 2012, the prevalence of hypertension and diabetes among the Chinese adults is 25.2% and 9.7%, respectively, which is estimated to increase by 50% by 2030 if no effective control measure is available.7,9,10
Apart from the overall prevalence, the chronic disease burden is also manifested as the imbalanced socioeconomic distribution of prevalence. Typically, there may be a difference in the prevalence of the chronic disease among populations with various socioeconomic layers; for instance, a low income and an old age will increase the risk of incidence of 2 or more multiple chronic diseases in the individuals.11,12 The income gap among different populations is shrinking, but the tiny income gap will also aggravate the difference in the prevalence of the chronic disease among the population due to the different age.
Therefore, it is of crucial importance to understand the socioeconomic distribution of chronic disease among the Chinese elderly population, so as to formulate the control measures for chronic diseases. Previous studies mainly focused on evaluating the chronic disease distribution situation from the point of view of regional economic inequality. However, from the individual level, the differences in chronic disease prevalence among different age groups and different income populations, as well as the correlation and distribution rules, remain unclear. Therefore, this study proposed to use individual income and chronic disease prevalence data among the national populations aged above 45 years collected from the China Health and Retirement Longitudinal Study (CHARLS), to learn the income-related inequalities of chronic disease situation among the Chinese populations aged above 45 years using the Multivariate Generalized Quasi-Poisson Regression method.
Through this study, we could know the topic of income-related inequalities in chronic conditions, and provide implications on carrying out targeted policy intervention and health management for people of different health and income positions in China. Faced with the increasing personal disease burden, it is of great significance and urgency to study the distribution and association of chronic disease prevalence among age groups and income status. This may bring implications for people of different age groups and income status to improve personal awareness and preparedness of chronic disease prevention. Thus, national medical finance investment can be more purposeful and more targeted health policies could be developed to address a range of income-related inequality issues in chronic conditions.
Methods
Data Sources
Data in this study were derived from the follow-up data of the CHARLS in 2015. Typically, the CHARLS had carried out a baseline survey on 450 villages from 150 counties of 28 provinces since 2011, and the samples had represented the middle-aged and elderly populations aged above 45 years in China. The contents that CHARLS investigated included personal sociodemographic characteristics, personal health and function, as well as personal and household economic income and expense. The CHARLS data can be downloaded at the official website (charls.pku.edu.cn/en).
In the database of CHARLS in 2015, there were 21 100 individuals from 12 235 households, in which 369 were missing age and 1013 were below 45 years. As a result, there were 19 718 individuals aged ≥45 years, in which 698 were missing their income. Finally, 19 020 individuals were included in our study.
Definition and Calculation of the Research Variables
The dependent variable of this study was prevalence status of chronic diseases and the independent variable was the individual’s total annual individual income. We also consider several variables as potential covariates which were commonly reported in the studies of chronic diseases, including household register, economic zone, education level, marital status, and the current status of smoking and drinking.
Total annual individual income: The total annual individual income was calculated as the sum of annual individual income only from 4 sources (wage, bonus income, pension, and government subsidy), and per capita annual household income from all other sources (eg, all crops, forestry products, all livestock, aquatic life, and property). Afterward, the total annual individual income was divided into tertiles according to the household register, and 3 levels (unit: Yuan) were defined in succession as low (urban area: 0-3410, rural area: 0-687), medium (urban area: 3411-28 800, rural area: 688-3590), and high income (urban area: >28 800, rural area: >3590).
Chronic disease prevalence: The chronic disease prevalence was obtained from the questionnaire by the question “Had some doctors once told you that you had the following chronic diseases?” and 14 chronic diseases were involved, including hypertension; dyslipidemia; diabetes or high blood sugar; cancer or malignant tumor; chronic lung disease (not included tumor or cancer); liver disease (except for fatty liver, tumor, or cancer); heart problems; stroke; kidney disease (not included tumor or cancer); stomach or other digestive disease (not included tumor or cancer); emotional, nervous, or psychiatric problems; memory-related disease; arthritis or rheumatism; and asthma. The remaining demographic characteristics (age, sex, family register, education, and marital status) could be extracted from the corresponding questions in the questionnaire.
Household register means Hukou in China. The Hukou system was implemented in China in the late 1950s. It was regarded as an institution that controls population mobility, in which an individual is required to register in 1 and only 1 place of the regular residence. The location of the household register is also related to the individual’s benefits and privileges. Depending on location, the household register (Hukou) was divided into urban and rural areas.
Economic zone: China is a vast country with seriously unbalanced regional development. According to the regional economic level and future development strategies, the National Bureau of Statistics divides China into 4 economic zones, namely the eastern (10 provinces), middle (6 provinces), western (12 provinces), and northeastern zones (3 provinces). The economic level declined from the east to the west. As the focus of future development, 3 northeastern provinces have recently been independent and established as the northeastern zone. In general, the total annual individual income was different between the 4 economic zones. Therefore, we also included the economic zone in which the individuals were located as a variable in the model.
In this study, education level included 4 levels (illiterate, elementary school, middle school or high school, and above high school). Marital status also included 4 types (married, divorced or separated, widowed, and single). The current status of smoking or drinking (yes or no) were also included as variables in the study.
Statistical Methods
The income proportion and chronic disease prevalence in this study were adjusted by the weights in CHARLS database in 2015, so as to adjust the non-randomness and non-response during the extraction of CHARLS investigation samples.
Moreover, the low-income population at each age group was treated as the reference, to calculate the prevalence ratios (PRs) in the medium income and high-income populations through Multivariate Generalized Quasi-Poisson Regression analysis.
Pearson chi-square tests were conducted to examine associations between chronic diseases and each of the potential covariates. Basically, all these variables were significantly associated with different chronic diseases (P < .05). Moreover, as a rule of thumb, multicollinearity may be a serious problem if the variance inflation factor (VIF) exceeds 10. We calculated VIF in different chronic disease regression models and none of them exceeded 10. Therefore, these variables were finally regarded as covariates and included in the model, including household register, economic zone, education level, marital status, and current status of smoking or drinking.
Descriptive statistical analysis in this study was performed using the statistic software Stata 13.0 by 2-sided test, and the α level was set at 0.05. Multivariate Generalized Quasi-Poisson Regression was conducted using R 3.5.3.
Results
Income Distribution and Chronic Disease Confirmed Prevalence Distribution Among Populations at Various Sex and Age Groups
A total of 19 020 participants aged above 45 years were recruited into the current study, including 9228 male participants and 9792 female participants. The income distribution among populations at various sex and age groups are shown in Table 1. With the increase of age, the proportion of the high-income population was gradually reduced, and the high-income population aged ≥75 had taken up the lowest proportion.
Number and Percentage of Male and Female Participants in Each Age Group, by Total Annual Individual Income Category.

Note. Numbers refer to the unweighted frequencies from analysis sample; while % refers to weighted population estimates based on analysis sample.
Table 2 had displayed the prevalence of each chronic disease. Among them, arthritis or rheumatism had the highest prevalence (35.70%), while cancer or malignant tumor had the lowest prevalence (1.47%). The prevalence of other common chronic diseases, such as hypertension and diabetes or high blood sugar, was 29.49 and 8.34%.
Prevalence of Chronic Diseases Among Chinese Aged Above 45 Years.
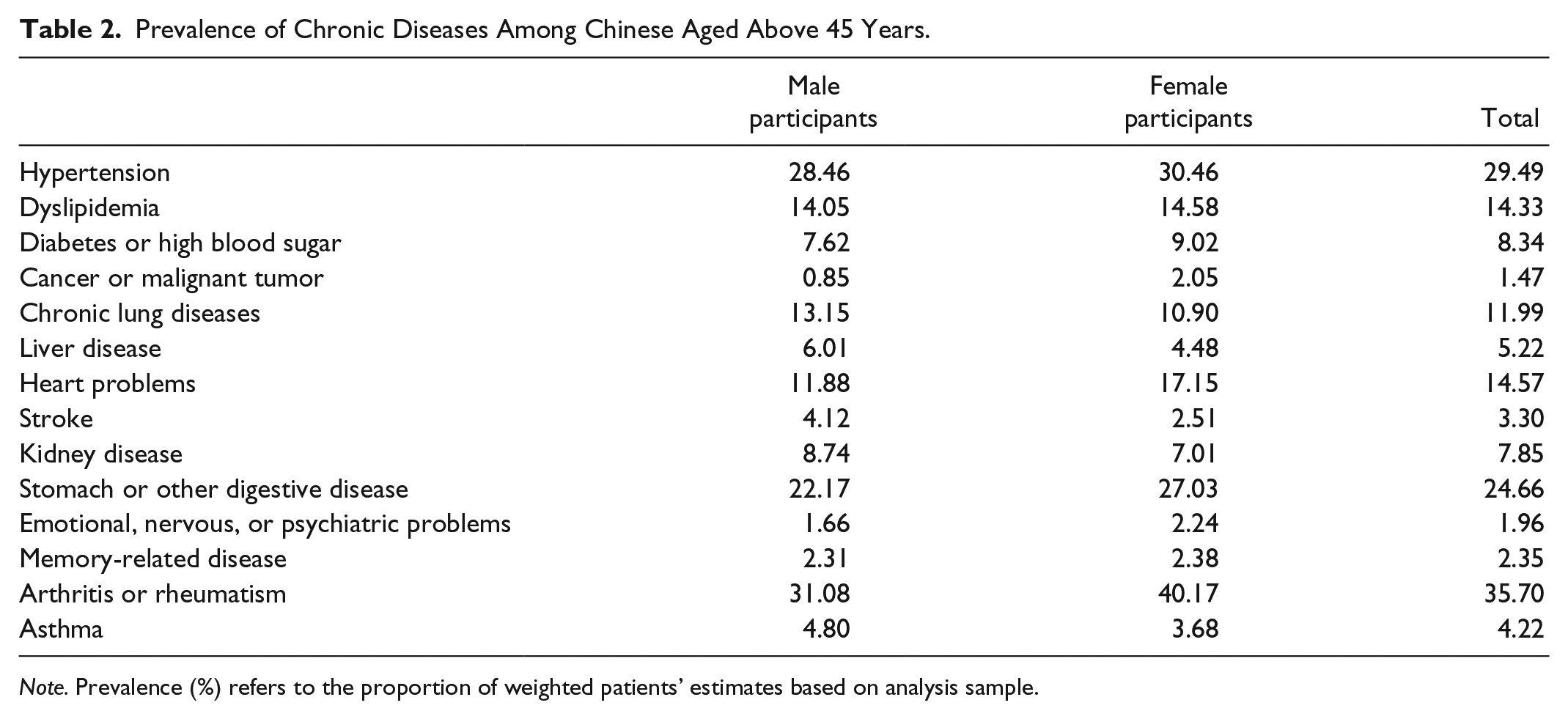
Note. Prevalence (%) refers to the proportion of weighted patients’ estimates based on analysis sample.
Income-Related Distribution of Chronic Disease Prevalence Among Populations at Various Age Groups
The income-related distribution of chronic disease prevalence among populations at various age groups is displayed in Figure 1. As could be discovered from the figure, hypertension had the highest prevalence in the population aged ≥75 years among all chronic diseases (male participants: 44.41%, and female participants: 47.53%), especially in the high-income population at the age group (male participants: 50.74%, and female participants: 47.07%). As for disease with the lowest prevalence, cancer or malignant tumor (not included mild skin cancer) had the lowest prevalence (0.13%) in the high-income population aged 46 to 59 years in male participants, while the memory-related diseases (such as Alzheimer disease, brain atrophy, and Parkinson disease) had the lowest prevalence (0.61%) in the high-income population aged 46 to 59 years in female participants.

Income-related distribution of chronic disease prevalence among populations at various age groups.
On the whole, the prevalence of chronic disease showed an increasing trend with age, such as hypertension, diabetes or high blood sugar, chronic lung disease, stroke, memory-related disease, and asthma. Apart from age, chronic disease prevalence would also display an increasing or decreasing trend with the increase in income; for instance, the prevalence of hypertension in male participants aged ≥75 years and that of diabetes or high blood sugar at all age groups were increased with the increase in income, whereas that in malignant tumor such as cancer among female participants aged ≥75 years, and that of emotional and mental disease in male participants aged 45 to 49 years were decreased with the increase in income.
Moreover, there was also a difference in the distribution of chronic disease prevalence between different sexes; for instance, the prevalence of chronic lung disease and asthma in male participants was higher than that in female participants, while that of the stomach or other digestive disease in female participants was higher than that in male participants.
Multivariate Generalized Quasi-Poisson Regression Analysis of Income-Related Inequality of Prevalence
As could be discovered through Multivariate Generalized Quasi-Poisson Regression analysis, chronic disease prevalence was associated with income and age. The relative income inequality of prevalence at each age group is shown in Figure 2. Taking the low-income population as the reference, the medium- and high-income populations were associated with a higher risk of prevalence of some chronic diseases, such as dyslipidemia, heart problem, stroke, kidney disease, and memory-related diseases. On the contrary, the risks of the prevalence of some other chronic diseases were lower in the medium- and high-income populations, such as emotional and mental disease, arthritis, or rheumatism.

Associations between income levels and chronic disease prevalence among populations at various age groups.
To be specific, the chronic disease with the largest PRs in male participants was heart problem among the medium income population aged 46 to 59 years (PRs: 1.52, 1.07-2.16), while that with the lowest PRs among the high-income population aged 46 to 59 years was emotional and mental disease (PRs: 0.15, 0.04-0.65). In female participants, the chronic disease with the largest PRs was memory-related disease among the medium-income population aged 46 to 59 years (PRs: 2.26, 1.02-5.00), while that with the lowest PRs among the high-income population aged 46 to 59 years was cancer or malignant tumor (PRs: 0.40, 0.17-0.94). At the same time, the above results and Figure 2 also suggested that income had a great effect on the chronic disease prevalence in population aged 45 to 59 years.
Discussion
Different from most of the published studies evaluating chronic disease distribution situation through regional economic inequality, this article had evaluated the income-related inequality of chronic disease prevalence from the point of view of personal income based on the 2015 CHARLS follow-up data. Findings in this study indicated that the chronic disease prevalence in Chinese population aged above 45 years was partially correlated with the age group and income, which displayed regular distribution characteristics.
Correlation of Income-Related Inequalities With Age Group
On the whole, this study had revealed no difference in the chronic disease prevalence in population aged ≥75 years among different income groups, namely, the population aged ≥75 years was associated with the lowest income-related inequality of chronic disease prevalence. On the contrary, the chronic disease prevalence among the population aged 45 to 59 years was greatly affected by income, such as heart problem, and these results were consistent with foreign studies.13,14
In other words, the relative income inequality of chronic disease prevalence would be shrunk with the increase in age, which might be because that, the population aged 45 to 59 years was still the labor force population, and the personal income could reflect their job nature, working environment, and surrounding contact population to some extent. The differences in working environment and social environment might aggravate the difference in the risk of chronic disease prevalence by affecting the chronic disease-related factors (such as smoking, obesity, static activity, and health management) through a complicated mechanism. 15 In contrast, the population aged ≥75 years had lost the basic labor force, their mobility and range of motion were limited, and thus the influence of income on prevalence would also be limited, regardless of the difference in income. Moreover, the population aged ≥75 years might also be associated with the survival effect, which was that such population was survived after the influence of income inequality, leading to the little difference in prevalence among different income groups. 16
Correlation of Income-Related Inequalities With Disease
For an individual disease, the relationship between each chronic disease and income was different. This might be due to different risk factors for all kinds of chronic diseases, and the impact of income on these risk factors was also different. For instance, compared with the low-income population, the high-income population was associated with a lower risk of arthritis or rheumatism and a higher risk of dyslipidemia. Heavy physical labor might be the key factor affecting the relationship between arthritis and income. 17 As for dyslipidemia, high income mainly increased its incidence by affecting the risk factor of obesity.18,19
In the most chronic diseases, income-related inequalities in China was basically consistent with that in other countries, including diabetes, 14 cancer, 14 arthritis, 20 and emotional problem.21,22 However, some of the results were contrary to other counties, including heart problem, stroke, 23 and memory-related problems. 24 Taking heart problem as an example, this study indicated that, the medium-income Chinese population aged 45 to 59 years had a higher risk of prevalence than the low-income population. However, foreign research had come to opposite results, suggesting that the foreign low-income population aged 45 to 64 years had suffered from a higher risk of heart problem. 14 This might be because that, the high-income population in developed countries had paid more attention to health management, while China, a developing country, had paid attention to chronic disease health management in recent years, the overall health consciousness in the population was not high, and the distribution of heart problem risk factors (eg, obesity) in the medium- and high-income populations was higher than that in the low-income population. As a result, the income distribution of heart problem prevalence in China was different from that in foreign countries. 15
Implications for Health Policy Making in China
The challenges for health policy making in chronic disease prevalence among different age groups and different income populations are complex but the findings of this article may be a valuable tool for both personal perspective and national health policy development.
For the personal perspective, personal awareness and preparedness of chronic disease prevention could be better improved for people of different age groups and income status. The chronic disease management among the population aged 45 to 59 years should be focused, and a healthy lifestyle, happy working environment, and balanced working psychology should be advocated.
For health policy making, targeted health policies could be developed to gradually ease the seriousness of income-related inequality issues in chronic conditions for people of different age groups and income status. The supportive policy for social health management industry should be further developed, and the utilization rate of health management means in the population that can afford that industrial consumption expenditure should be enhanced. Certainly, the above-mentioned measures are the targeted interventions based on the current situation, and it remains the long-term challenge in the future to truly alleviate or eliminate such inequality.
Limitations of This Study
This study is associated with certain limitations. First, all the chronic disease prevalence data were derived from the sample self-report, which might lead to recall bias. Second, this study was a cross-sectional study, with limited adjustment variables incorporated into the regression model, and the causality between income and chronic disease prevalence had not been definitely confirmed. Third, this study was carried out on the premise that other inequality factors were homogeneously distributed among different income groups; for instance, the self-reported error rate of chronic disease was basically consistent among all income groups. Moreover, the data in this study were derived from the CHARLS national survey results, and some participants made no response to the questionnaire; to this end, the results in this study were corrected using related weights.
Conclusion
Previous studies on income-related inequalities in chronic conditions mainly focused on evaluating the chronic disease distribution situation in developed countries. This study quantified income-related inequalities in chronic disease situation among ≥45-year-old people in China (a developing country). The results showed that significant inequalities in chronic conditions prevalence persist into old age, particularly among 45- to 59-year-old people. Opposite to developed countries, the prevalence of some chronic disease (ie, heart problem) is higher in richer populations in China. These findings pose the policy challenge of needing to prevent such inequalities in older years.
Footnotes
Acknowledgements
We would like to acknowledge the China Health and Retirement Longitudinal Study (CHARLS) team for collecting nationally representative data and for making the data public. We also acknowledge its financial support from National Institute on Aging, World Bank, and National Natural Science Foundation of China. We thank Dr. Li from Capital Medical University for helping us analyze the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (grant number: 71704042).