
Abstract
The objective of this study was to examine variations in the determinants of joint replacement (JR) across gender and age, with emphasis on the role of social support and family dynamics. We analyzed data from the US Health and Retirement Study (1998-2010) on individuals aged 45 or older with no prior receipt of JR. We used logistic regression to analyze the probability of receiving knee or hip replacement by gender and age (<65, 65+). We estimated the effect of demographic, health needs, economic, and familial support variables on the rate of JR. We found that being married/partnered with a healthy spouse/partner is positively associated with JR utilization in both age groups (65+ group OR: 1.327 and <65 group OR: 1.476). While this finding holds for men, it is not statistically significant for women. Among women younger than 65, having children younger than 18 lowers the odds (OR: 0.201) and caring for grandchildren increases the odds (1.364) of having a JR. Finally, elderly women who report availability of household assistance from a child have higher odds of receiving a JR as compared with elderly women without a child who could assist (OR: 1.297). No effect of available support from children was observed for those below 65 years old and elderly men. Our results show that intrafamily dynamics and familial support are important determinants of JR; however, their effects vary by gender and age. Establishing appropriate support mechanisms could increase access to cost-effective JR among patients in need of surgery.
Prior literature has identified social support as a determinant of patient preferences and outcomes among patients undergoing joint replacement; however, the extent to which social support and a broader set of family dynamics influence access to joint replacement in the US population has not been fully examined.
Our research contributes to the field by providing an assessment of the role that family support and dynamics play in an individual’s decision to receive joint replacement.
Our results show that intrafamily dynamics and familial support are important determinants of joint replacement; therefore, establishing appropriate support mechanisms could increase access to joint replacement among patients in need of surgery.
Introduction
Hip and knee replacement surgeries are cost-effective procedures that yield significant improvement in pain and function.1-11 For working-age patients, joint replacement (JR) may produce societal benefits that offset the direct cost of surgery by increasing work productivity.12-14 Prior research has documented significant variation in the utilization of JR across geographic, insurance coverage, and racial groups, suggesting that certain groups of individuals may face barriers to receiving JR.15-27 The influence of social support on JR utilization, however, has received less attention.
Social support embodies the set of relationships and networks that serve as a source of emotional, financial, or informational assistance during times of stress.28,29 Social support has been associated with mortality and surgical outcomes among different patient populations.30-33 Among patients who have had major thoracic/abdominal surgery, social support has been linked to faster rate of improvement in postoperative pain and lower likelihood of having a long length of stay (7 or more days). 34 Prior literature has also identified social support as a determinant of patient preferences and outcomes among patients undergoing JR.35-37 However, the extent to which social support and a broader set of family dynamics influence access to JR in the US population has not been fully examined.
In this study, we examine the role of social support and family dynamics along with the other determinants of JR across gender and age. We investigate the extent to which familial support from a spouse or children influences men’s and women’s decisions to undergo JR. We also examine the role of family responsibilities, such as caring for young children, grandchildren, or parents, in determining JR utilization. Taken together with indicators of familial support, support provided to family members provides a holistic view of the family dynamics, the strength of family network, and their role in accessing JR. We allow these effects to vary by age, distinguishing between those below and above 65 years old.
Modeling JR utilization separately for age-gender groups is important because the elderly may have different support needs and options, such as assistance from adult children, than younger JR patients. Furthermore, intrafamily support may affect men and women differently in their decision to have a JR as a result of the distinct roles and responsibilities that men and women may hold within a family. Prior research has been inconclusive on the relationship between gender and JR. While several studies have found no difference between men and women in their propensity to receive JR, others have found gender disparities in JR utilization even after controlling for clinical factors.38-49 Furthermore, studies indicate that women undergo JR at a worse functional state compared with men.47-51 Gender-specific effects of social support on JR utilization may explain some of the observed differences in JR rates between men and women.
Materials and Methods
Study Purpose and Hypotheses
We assume that as an elective surgery, the demand for JR is influenced by a number of economic and noneconomic factors. While the typical outcome of surgery is reduced pain and improved function, there are surgical risks and a long recovery. Thus, financial considerations (eg, income, insurance coverage), expectations of outcomes, and recovery support, among other factors, influence the decision to have surgery.
We hypothesize that the presence of familial support positively influences the patient’s propensity to undergo JR. Prior to surgery, family members may facilitate the patient’s decision-making regarding surgery by helping him or her interpret medical and nonmedical information. After surgery, family members may help decrease the burden that comes with lower mobility and thus lower the pecuniary and nonpecuniary costs of recovery. The role of family responsibilities, however, may have an ambiguous effect on JR utilization. On one hand, the caregiving responsibility for a child, grandchild, or parent may cause the patient to delay needed surgery, particularly if alternative caregiving arrangements are too costly. On the other hand, such responsibilities may encourage patients to invest in JR in the short run to have the opportunity for providing more effective care to family members in the future.
The effect of these determinants on JR utilization may vary by age and gender. For example, women who are viewed traditionally as the primary caregivers within the family may be more able to harness familial support or more willing to accept it during recovery from surgery. Furthermore, the elderly may have more knowledge of or access to support systems outside of their family through their health care providers or peers, limiting the potential influence of familial factors in their decision to undergo JR.
Data Source and Sample Definition
Our study is based on data from the Health and Retirement Study (HRS), which is a longitudinal survey of a nationally representative sample of US adults above the age of 50 and their spouses/partners. 50 To construct our analytic sample, we used data from interviews conducted between 1998 and 2010 and data from the RAND HRS Data File and RAND HRS Family Data. 51 The variables used to construct the JR indicator came from the 1998-2010 RAND-Enhanced Fat Files, which present the original HRS data at the respondent level. Institutional review board approval was not required because the analysis did not involve data that contained identifiable patient information.
Our analytic sample consisted of respondents and their spouses/partners (hereafter collectively referred to as respondents) who had at least 2 consecutive interviews during the study period. For each 2-year interval between interviews, we refer to the first interview as baseline and the second as follow-up. We limited our sample to respondents who are aged 45 or older at baseline, reported having arthritis or rheumatism, and did not report having had JR prior to baseline. We observed them until their first reported JR within the study period.
Description of Variables
Outcome variable
Our outcome measure is the receipt of JR between baseline and follow-up. This binary variable takes on the value 1 if both of the following conditions hold: (1) the individual responded affirmatively to having surgery or any JR because of arthritis in the previous 2 years, (2) the affected joint is knee or hip. If the individual reported a hip surgery or replacement due to arthritis and a hip fracture in the same interview, the hip surgery is not counted as JR.
Explanatory variables
Our model included 4 sets of explanatory variables measured at baseline: demographics, health needs and conditions, economic factors, and family and social dynamics.
Demographic variables
Demographic factors were age, gender, and race/ethnicity. The race/ethnicity variables are used to identify the following mutually exclusive groups: Hispanic, non-Hispanic white, non-Hispanic black, and non-Hispanic other race.
Health needs and conditions
Health-related variables included those that correlate with an individual’s need for JR, as well as chronic conditions and general health status that influence an individual’s propensity for undergoing JR. Need was proxied by the presence of functional limitations related to activities involving the lower extremities. These functional limitations indicators took on the value of 1 if the respondent self-reported difficulty or inability in performing the following activities: walking 1 block, getting up from a chair, climbing 1 flight of stairs, and stooping and crouching. In addition, we included indicators for self-reported high blood pressure/hypertension, diabetes, cancer, lung disease, heart problems (heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems), and stroke. Obesity was measured as having a body mass index of 30 or above. We also included self-reported pain and health status variables in our model. The pain variable indicated whether the respondent reported experiencing pain often and rated the pain as being severe most of the time. The health status indicator took on the value 1 for self-reported health of Good, Very Good, or Excellent and 0 for Fair or Poor health.
Economic factors
Economic factors included insurance coverage, income and wealth, whether the respondent is working for pay, whether his or her health limits the kind or amount of paid work, and his or her educational attainment. We categorized respondents younger than 65 into 3 mutually exclusive health insurance coverage groups: Medicaid, any other health insurance coverage, and no insurance. Respondents who are 65 or older were categorized into another set of 3 mutually exclusive health insurance groups: Medicare, other insurance, and no insurance. Income and wealth variables were included in the analysis as measures of financial constraints affecting an individual’s decision to receive JR, and these variables were adjusted for inflation using the Consumer Price Index and expressed in 2014 dollars. Missing values were imputed by RAND using unfolding brackets, where applicable, which prompt the respondent to identify value ranges for income and asset categories. The model controlled for whether the respondent is (1) employed, (2) employed with health limitation (ie, respondent’s health limits the kind or amount of paid work he/she does), or (3) employed without health limitation. The model also included a categorical variable on respondent’s educational attainment that takes on the following values: (1) less than high school, (2) high school, and (3) some college or above.
Family dynamics and support
We included several indicators of household composition and family dynamics in our analysis. We identified spousal support using a categorical variable that indicates the individual (1) has a healthy spouse/partner, (2) unhealthy spouse/partner, and (3) no spouse/partner. The health of the spouse is based on the self-reported health status of “Excellent,” “Very Good,” and “Good.” To capture respondent’s caregiving responsibilities, we included indicators for whether the respondent has young children (less than 18); whether he or she spent more than 100 hours during the past year helping parents or parents-in-law with errands, chores, or transportation; and whether he or she spent more than 100 hours caring for grandchildren or great-grandchildren. Finally, our analysis controlled for whether the responded has a child or child-in-law who would be willing and able to help with basic personal care activities over a long period of time if the respondent needed it.
Statistical Analysis
We modeled the probability of receiving a JR within 2 years of baseline using a multivariate logistic regression model separately by gender and age groups (<65 and 65+). In our analyses, we used person-weight, stratum, and sampling error codes provided by the HRS and Stata’s svy procedures to adjust for the complex sampling design and yield nationally representative estimates. We also conducted a sensitivity analysis by estimating a logistic regression model using person-weights and adjusting standard errors for clustering at the respondent level.
Results
The overall study sample included 10 045 people and 46 472 person-period observations. About 17% (866 of 5081) of the people in the elderly group and 9.0% (466 of 4964) of the younger group (<65) reported a JR, resulting in a total of 1312 JRs observed over the study period. The majority (78.7%) of reported JRs involved knee replacements, and 1.3% of the JRs involved both knee and hip replacement.
The annual JR rate is 14.9 JRs per 1000 among the elderly and 13.7 among those below 65 (Table 1). It is important to note that these rates correspond to our study sample of respondents with self-reported arthritis. In the broader HRS sample, without restricting to those with arthritis, the annual JR rates are 9.8 and 6.8 JRs per 1000 among the elderly and those below 65, respectively. Descriptive statistics show that unadjusted JR utilization rate is higher among those who are married, and among married people aged 65 and above, those with a healthy spouse have a higher JR rate than those who have an unhealthy spouse (P value < .001). In the younger cohort, having children younger than 18 is associated with lower JR utilization, whereas caring for grandchildren is associated with higher JR rate in both age cohorts. We find that unadjusted annual JR rate is higher among those who provide care for their parents and those with children who can provide basic personal care if needed; however, the subgroup differences in JR rates are not statistically significant.
Annual Rates of Joint Replacement.

Note. JR = joint replacement.
Population weighted annual JR rate.*P values take into account the person-weight, stratum, and sampling error codes to adjust for the complex sampling design.
In the 65+ group, 63.0% were female, 8.9% black, 5.4% Hispanic, and 1.6% other race (Table 2). About 55.3% of the elderly were married/partnered, 37.8% had a high school degree, and 34% had more than 12 years of education. In the younger group (<65), a smaller percentage was female (59.5%), and a greater percentage was non-white (20.6%). Younger people were also more likely to be married/partnered (71.2%) and have more than a high school degree (45%).
Descriptive Statistics of Select Baseline Characteristics.

Note. Analysis takes into account the person-weight, stratum, and sampling error codes to adjust for the complex sampling design.
About 34.8% of those below 65 and 20.3% of those 65 and above reported caring for grandchildren while the rates of parental care were 18.5 and 3.9% in the two groups, respectively. About 8% of the younger cohort have children younger than 18, but, as expected, the rate is much smaller among the elderly (0.5%). More than 40% of the study sample reported having a child or child-in-law who would be willing to help with personal care activities if needed in the future.
We observed several key differences between the genders in both age cohorts (see Supplementary Material, Table S1). Women were less likely to be married/partnered, had lower rates of education above high school, and had higher rates of the selected functional limitations compared with men across both age groups. In the elderly cohort, women were less likely to have a child below 18 and care for a parent or a grandchild compared with men. In the younger cohort, women were also less likely to have a young child compared with men; however, they were more likely to provide care for their grandchildren and had similar propensity to have caregiving responsibilities for their parents as the men in their age cohort. The probability of having a child or child-in-law who is able to care for the respondent is similar between older men and women while it is higher for women relative to men in the younger cohort.
Table 3 presents results of the logistic regression model estimation for select covariates (see Supplementary Material for full set of model estimates and gender-specific regression results). Since the baseline JR rates are small, we interpret the odds ratios as estimates of relative risk. Among the elderly, blacks are 45.2% less likely to receive JR relative to whites (OR = 0.548). Gender-specific regression results suggest that this difference is driven by the racial disparity in receiving JR observed in elderly black females (OR = 0.498) (Table S2). The differences in JR rates between Hispanics and whites are not statistically significant in the overall elderly population. However, we find that Hispanic males have higher utilization than white males (OR = 1.889) in the elderly population, holding other factors constant. We also find no statistically significant differences in JR rates between racial groups among those younger than 65 years old (Table S3).
Logistic Regression Results for Joint Replacement, by Age Category.
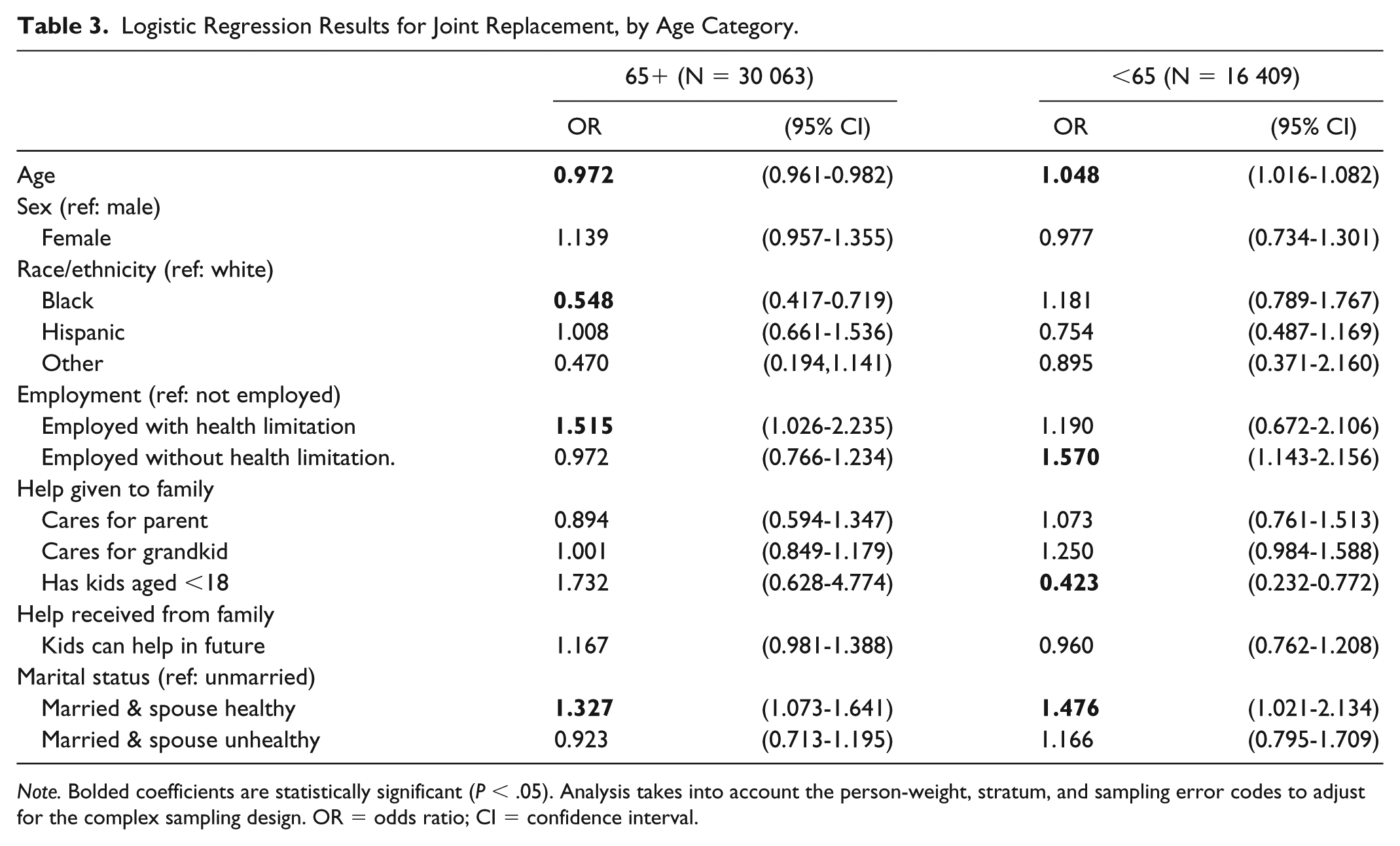
Note. Bolded coefficients are statistically significant (P < .05). Analysis takes into account the person-weight, stratum, and sampling error codes to adjust for the complex sampling design. OR = odds ratio; CI = confidence interval.
Relative to other health insurance coverage, Medicaid coverage raises the odds of having JR (OR = 1.632), and lack of health insurance coverage is associated with lower JR utilization among people below 65 (OR = 0.413). Among the older cohort, having Medicare and having no health insurance do not have a statistically significant effect on JR use relative to other health insurance coverage. Age-specific model estimates yield no statistically significant relationship between health insurance coverage and JR among elderly men and women (65+) and younger women (<65).
We find some evidence of financial constraints in limiting JR use among people above the age of 65, among whom those in the highest income group are 69.0% more likely to have JR and those in the highest net wealth group are 52.5% more likely to have JR relative to lowest income and net wealth groups, respectively. Education does not have a statistically significant influence on JR utilization in the younger cohort. In the older cohort, having a high school degree is associated with higher JR utilization (OR: 1.268) compared with having less than a high school degree. We did not find a statistically significant effect associated with having at least some college education on JR use in the older cohort. Among the elderly, people who are working with health limitations are 51.5% more likely to receive JR than those who are not working while working without work limitations has no statistically significant effect on JR rate. In contrast, among the younger cohort, people who are employed without work limitations are 57.0% more likely to receive JR than those who are not working, and working with work limitations has no statistically significant effect on JR rate.
Our results suggest that familial factors may affect an individual’s propensity to undergo JR; however, the effects vary by gender. We find that people married/partnered with a healthy spouse/partner are more likely to undergo JR relative to those who are unmarried/nonpartnered. (OR = 1.476 in <65 group and OR = 1.327 in 65+ group). This variable is positively related to JR utilization only among men and does not have a statistically significant effect on JR rates for women (Tables S2 and S3). We find that individuals with an unhealthy spouse/partner are not statistically significantly different from those who are not married/partnered in terms of JR use, holding other factors constant. Having kids who may help with basic personal needs in the future has a positive effect on JR use among elderly women (OR: 1.297) and no statistically significant effect on other age-gender groups (Tables S2 and S3).
Furthermore, having children younger than 18 lowers the odds of having JR among women younger than 65 (OR: 0.201) and has no statistically significant effect on JR use in other age-gender groups (Table S2 and S3). Among people below 65, women caring for grandchildren are 36.4% more likely to have JR (Table S3). Caring for parents does not have a statistically significant effect on JR use in any of the cohorts studied.
Our findings were robust to estimation using a logistic regression model with person-weights and clustered standard errors. The results of this sensitivity analysis are provided in the Supplementary Material (Table S4).
Discussion
Our study reinforces findings from previous literature while revealing new insights related to the role of family support in determining JR utilization. Consistent with prior studies, we find lower utilization of JR in the black, elderly population although our findings suggest that this disparity may be driven by underutilization of JR among elderly black women.17,18 In terms of clinical indicators, we find obesity and functional limitations to be important determinants of JR, similar to findings in previous studies.16,18 We find that having poor self-reported health and severe pain are positively related to JR in the elderly population and are not associated with JR in the below 65 population. Our findings provide some support for previous studies that found that health insurance coverage (among those below age 65) and financial factors (eg, income and wealth among those above age 65) may influence access to JR.16,18,22
Our findings on the relationship between work status and JR rate varies between the two cohorts. We find that working with health limitations is associated with a higher JR rate among the elderly cohort, and working without health limitations is associated with a higher JR rate among the younger cohort. This finding is consistent with the hypothesis that people above 65 with arthritis postpone JR until their symptoms start limiting their work, while working age individuals (ie, younger than 65) with arthritis have JR before their symptoms start limiting their work. This suggests that the younger cohort may perceive JR as a long-term investment decision, which is plausible given that they face a longer period in labor market than the older cohort.
Some of our findings deviate from previous research. We find that within the elderly population, Hispanic men are more likely to receive JR compared with white men with similar clinical, economic, and family backgrounds while previous studies have reported either lower or similar utilization of JR among the Hispanic population relative to the white population.16,41 We also find a positive effect of education on JR utilization in the elderly cohort and no effect of education on JR utilization in the younger cohort while prior research documented a positive relationship between educational attainment and JR.16,17
The primary contribution of this work is our assessment of family support and dynamics in determining the use of JR. Our results show that intrafamily dynamics are important determinants of JR; however, their effects vary by gender and age. Lack of familial support contributes to lower utilization of JR for certain age and gender groups. For men, support from a healthy spouse/partner increases likelihood of JR; for women above 65, support from children regarding basic personal needs raises JR propensity.
In addition to support received from family members, we also examine the relationship between support provided to family members and JR utilization. We find that support provided to family may influence JR probability, but the effect is evident only among women below 65. Our findings suggest that having children younger than 18 lowers the probability of JR among women below 65. On the contrary, caring for grandchildren increases the probability of JR for the same cohort. These results demonstrate the opposing effects caregiving responsibilities may have on JR use. The caregiver in need of JR may forego the surgery if the costs of substitute caregiving arrangements in the short-term are too high relative to the benefit of providing care in the long run. We did not find any statistically significant association between caring for parents and the rate of JR.
Our findings underscore the fact that the effects of JR determinants on the overall population may mask gender differences. For example, Steel et al found that being married or cohabitating predicted hip or knee replacement, with an odds ratio of 1.43 relative to being single, widowed, or divorced, but this effect was not statistically significant. 17 However, Steel did not differentiate between genders or individuals with healthy and unhealthy partners. Steel also found no statistically significant effect of caring for grandchildren on JR use in a pooled sample of men and women.
This study has a number of limitations. First, we estimated the relationship between observable characteristics and the likelihood of JR, but these effects may not be causal. Second, we included respondents who reported not receiving a JR within 2 years prior to the baseline interview. Some of these patients may have received a JR in years prior to that period. Third, our measures of patient need for JR are relatively limited and based on self-reported information.
Our study shows that lack of family support may limit access to JR among men and elderly women. Because JR is a cost-effective procedure, such barriers may impose unnecessary costs on patients and society. Over the last several years, payers and providers have increasingly engaged in alternative payment models (APMs) that are based on linking payments to quality and patient outcomes. Although the primary objective of these payment models is to incentivize providers to enhance value of care, they may also provide incentives to providers to focus on patients’ postdischarge support mechanisms and thus improve access to JR.
Accountable Care Organizations (ACOs) and the Comprehensive Care for Joint Replacement Model (CJR) serve as two examples with the potential to prompt providers to develop and/or engage in support networks for JR patients after discharge from the hospital. As a population-based payment and service delivery model, ACOs have financial incentives to improve quality and reduce health care costs for their defined populations through care coordination and postdischarge management of conditions. Similarly, CJR incentivizes care coordination among providers and reduced costs by holding acute care hospitals accountable for quality and cost of a patient’s episode of care. Ensuring that patients are informed about and utilize social support mechanisms available to them after surgery positively impacts outcomes and thus can motivate providers under both payment systems to focus on patients’ social support following JR. Research is needed to assess the extent to which APMs may have spurred utilization of social support mechanisms and led to improved access to care among JR patients. Furthermore, policy makers should develop and test models to encourage the development and provision of support mechanisms to those patients who may face barriers in accessing JR.
Supplemental Material
Supplementary_Material – Supplemental material for Determinants of Hip and Knee Replacement: The Role of Social Support and Family Dynamics
Supplemental material, Supplementary_Material for Determinants of Hip and Knee Replacement: The Role of Social Support and Family Dynamics by Berna Demiralp, Lane Koenig, Jennifer T. Nguyen and Samuel A. Soltoff in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors acknowledge the contribution of Elizabeth Hamlett, Delia I. Belausteguigoitia, and Sheila Sankaran with research support and manuscript editing.
Declaration of Conflicting Interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors’ employer, KNG Health Consulting, received previous funding from the following medical device organizations for prior work: Stryker, Smith & Nephew, Zimmer Biomet, and DePuy Synthes.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Advanced Medical Technology Association. The funders were able to review and comment on draft of the study, but the authors were solely responsible for study design, data collection, data analysis, and drafting the report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.