
Abstract
Hospitals assume broad social roles in their communities as major health service institutions, large employers, and in some cases as philanthropic organizations. These roles create perceptions about the community commitment of hospitals to a local community. How these perceptions toward hospitals influence patients’ decisions in choosing a hospital for care and trust in the health care system more generally has not been explored. As part of a study examining distrust in health care, we conducted a survey of African American and white non-Latino adults in metropolitan areas. We found that patients with very favorable views about the community commitment of their local hospital were more likely to choose that hospital for major surgery and less likely to report high health care system distrust.
Hospitals can play important social roles in their communities. Most directly, they provide health care as well as local employment and economic development (American Hospital Association 2008). Many hospitals also provide further community benefit by caring for uninsured patients, delivering services to vulnerable populations, and running health education and wellness programs (Foreman 1994; The Catholic Health Association of the United States and the Coalition for Nonprofit Health Care 2002). Together, these roles among others can create perceptions about the commitment of a particular hospital to a local community. In this manuscript, we explore whether public perceptions of hospitals’ community commitment influence the choice of hospital by patients and their level of trust in the health care system.
Understanding drivers of hospital choice is increasingly important as health care delivery reorganizes around accountability for the quality and cost of care delivered to a population. Prior research has demonstrated that hospital choice is largely driven by location, service provision, and reputation (Phibbs et al. 1993; Porell and Adams 1995; Taylor and Capella 1996). Importantly, despite attempts to make quality reports a more salient consideration in the selection of a hospital, the contribution of quality scores to hospital choice is relatively small. In one recent analysis, the effect of perceived overall reputation and availability of particular clinical services on hospital choice was much larger than the effects of quality scores, perceived cost, or nonprofit status (Jung, Feldman, and Scanlon 2011).
Despite the importance of hospital reputation and the limited effect of public reporting of quality on that reputation, the factors that contribute to overall hospital reputation and thereby influence hospital choice are not well understood. Building on evidence from the consumer marketing and business literature, we hypothesized that perceived commitment of a hospital to the local community contributes to hospital reputation and in turn influences hospital choice. Prior studies have shown that activities by businesses that signal greater corporate social responsibility lead to more favorable stakeholder relationships (among both consumers and employees) and improvements in overall reputation among consumers (Barnett 2007). These benefits accrue over years of social investments and are associated with stronger financial performance (Carroll and Shabana 2010). This is driven in part by the finding that consumers are more likely to choose a product from a company they believe is “responsible” and demonstrate greater customer loyalty to these companies (Besser and Miller 2001; Keim 1978). The higher stakes of health care decisions and the salience of caring relationships in the delivery of health services suggest that these concepts are likely to be important in health care.
Perceptions of hospital commitment to the community may also have other effects on patient beliefs about health care, including levels of distrust in the health care system. Considerable evidence across many disciplines has demonstrated that trust is associated with higher functioning of organizational units and societal entities, largely by reducing “transaction costs” and strengthening social support (Fukuyama 1995). In health care, lower levels of trust have also been associated with lower patient satisfaction, lower adherence to treatment and screening recommendations, and worse health status (Armstrong et al. 2006; Bickell et al. 2009; Carpenter et al. 2009; Nummela et al. 2009; Safran et al. 1998). Although most prior research on trust in health care has focused on interpersonal trust (i.e., trust in a physician), health care system distrust, a form of social/institutional trust, has recently been shown to be far more prevalent in the United States and to be associated with multiple important outcomes, including overall health status (Armstrong et al. 2006). As with many other forms of distrust, health care system distrust is comprised of two domains—beliefs about technical competence and beliefs about values, which include motives, honesty, and equity (Rose, Shea, and Armstrong 2004). Currently, relatively little is known about the specific determinants of health care system distrust although it is likely that levels of distrust emerge from individuals’ broad perceptions and experiences from the health care system. In this study, we test the hypothesis that an individual’s perceptions about the community commitment of their local hospital are associated with health care system distrust. The formation of attitudes is well established to be driven by exposure to the subject of interest among other factors (Banaji and Heiphetz 2012). Although individuals are likely to have many exposures to information about the health care system other than those related to their local hospital, it is possible that the perceptions of the local hospital are particularly salient and frequent and, thus, may influence broader attitudes toward the health care system in general.
Our study is exploratory in nature and seeks to describe associations between perceived community commitment of local hospitals and hospital choice and health care system distrust. We seek to add to the knowledge of factors that shape the choice of hospitals and distrust in the health care system. Future studies will be needed to further examine causal relationships and factors that shape perceptions about the community commitment of hospitals as well as other institutions in the health care system.
Method
We conducted a random digit dial telephone survey of African American and white non-Latino adults in the forty largest metropolitan areas (i.e., Metropolitan Statistical Areas [MSAs]) with at least 5 percent African Americans in the population. Due to Hurricane Katrina, the New Orleans, Louisiana, MSA was replaced with the Pittsburgh, Pennsylvania, MSA during the data collection period (Pittsburgh was the next largest MSA with at least 5 percent African American population). The sampling strategy was based on a larger study designed to examine differences in distrust between African Americans and whites within and across large metropolitan areas in the United States. Sampling was limited to these two racial groups due to the historical importance of race and trust in the U.S. health care system.
A random sample of telephone numbers from each MSA was selected for the survey. Business numbers were removed by matching against a YellowPages database, and nonworking numbers were removed through an automated dialing procedure that detects nonworking numbers. We oversampled African Americans within each MSA. The study was approved by the University of Pennsylvania Institutional Review Board.
Study Variables
Hospital community commitment and hospital choice
We asked respondents to name the hospital that is closest to their home to ensure that the respondent answered subsequent questions with that specific hospital in mind. We then asked the respondent, “In your opinion, how much does that hospital care about the health of people in your community?” Respondents chose from “not at all,” “a little,” “some,” or “a lot.” We then asked each respondent, “If you needed to have major surgery, would you go to that hospital or a different hospital?” We asked specifically about a “major surgery” to present the respondent with a substantial health care decision where they might have the opportunity to exercise choice (as opposed to emergency surgery or emergencies in general).
Health care system distrust and social trust
Health care system distrust was assessed using a nine-item established scale—the Revised Health Care System Distrust Scale (Cronbach’s alpha 0.83) (Shea et al. 2008). The scale includes two subscales: competence distrust that assesses perceptions of technical competence of the health care system and values distrust that assess perceptions of the health care system’s motives, honesty, and equity. We also measured social trust using a three-item instrument from the General Social Survey (Davis, Tom, and Marsden 2009).ocial trust measures respondents’ perceptions of the motives of others and whether, in general, people can be trusted. For our analysis of health care distrust, we adjust for social trust to ensure our findings do not reflect general positive or negative social views but rather views that are directly attributable to the health care system.
Health and sociodemographic characteristics
We asked respondents about their sociodemographic characteristics including race, ethnicity, income, and educational attainment using items from the National Health Interview Survey. Because of an administrative error, exact age was not collected in the survey. For 59 percent of the sample, age was able to be determined from publicly available data using the name and address of the respondent. For the rest of the sample, age was derived from the census tract adult age distribution for the race and gender of the respondent. We also collected information about health status (series of questions assessing presence of a chronic health condition) and health access (insurance coverage, health care–associated debt, usual source of care).
Survey Administration
We administered the survey using a computer-assisted telephone interview from June 3, 2006, to December 21, 2006. Individuals were offered $25 for their participation. We screened each household for eligibility with an initial question that asked if the household was “mostly . . .” Hispanic or Latino followed by the same question about race. Non-Latino households that selected “black or African American” or “white” were included in this study. The interviewer randomly selected a survey participant from a household roster provided by the answering party using an established algorithm. The race and ethnicity of the respondent was collected with two additional questions.
A total of 2,179 people completed the survey from the forty MSAs included in our sampling frame (2,029 African American or white respondents). Among eligible respondents, 64.5 percent completed the interview. The screener completion rate (i.e., number of household in which race and age eligibility was determined) was 35.1 percent. The overall response rate (i.e., the proportion of completed plus partial interviews divided by the number of interviews plus the number of refusals plus the estimated eligible proportion of noncontacted households—was 31.1 percent (calculated using the American Association for Public Opinion Research response rate #4).
Statistical Analysis
Our analysis consisted of three main questions. First, we examined the associations of respondent demographic and health characteristics with perceptions of the community commitment of their local hospital to the health of their community. Second, we examined the association of perceptions of hospital community commitment with hospital choice preference for “major surgery” of the respondent. Third, we examined the association of perceptions of hospital community commitment with distrust in the health care system. In each analysis, we tested bivariate associations with chi-square statistics. In our analyses testing for independent associations, we used logistic regression. The dependent variable in the hospital choice analysis was whether the respondent reported a preference to go to the closest hospital if they needed “major surgery” versus a different hospital. The dependent variable in the distrust analysis was high distrust representing the top quartile of reported distrust compared with the bottom three quartiles. We also tested an OLS model with distrust as a continuous variable. The independent variable in both the distrust and hospital choice analyses was a perception by the respondent that their local hospital cares “a lot” about the health of their community compared with “some,” “a little,” or “not at all.” We also tested models where perceived community commitment was coded as a categorical variable.
Sampling weights were used in the analyses to account for the complex sampling design. The sampling weights represent the inverse probability of inclusion in the sample adjusted for nonresponse bias based upon the estimated proportion of eligible household among the unresolved numbers. In addition, clustered standard errors were used in our multivariate analyses to account for the clustered (i.e., at the MSA level) sampling design. All p-values computed were two-sided. All analyses were performed using the Stata software program, version 9.2 (StataCorpLP; College Station, Texas).
Results
The demographic characteristics of survey respondents are presented in Table 1. Overall, 63 percent of respondents reported that their local hospital cares “a lot” about the health of their community compared with 25 percent responding “some,” 9 percent “a little,” and 3 percent “not at all.” Table 2 reports associations of respondent demographic and health characteristics with perceptions about the community commitment of their local hospitals. We modeled these associations using multivariate logistic regression models where the dependent variable was whether the respondent reported their local hospital cares “a lot” about their community. Middle- and older-aged respondents (age forty and above) were more likely to report that their local hospital cared “a lot” (Table 2) while those who had experienced health care cost barriers in the past year were less likely (OR = 0.47; p = .002). We did not find significant differences in perceptions by race, income, education, sex, health status (presence of a chronic disease), or by prior experience of having been referred to a collections agency for medical debt. We also modeled these associations using multivariate ordinal logit models and found similar results (Table 2).
Respondent Characteristics.

Note. Weighted percentages account for complex sampling design (i.e., probability of inclusion in the sampling frame, nonresponse bias).
Independent Associations of Respondent Demographic and Health Characteristics and Perceived Community Commitment of Local Hospital.

Note. In Model 1, the dependent variable (perceived commitment) is categorical with four categories: “not at all,” “a little,” “some,” and “a lot.” Odds ratios greater than 1 indicate higher levels of perceived commitment. In Model 2, the dependent variable perceived commitment is dichotomous (1 = “a lot” compared with the three other potential response categories). OR = odds ratio; CI = confidence interval.
Community Commitment and Hospital Choice
We examined unadjusted associations between perceived community commitment and hospital choice in a hypothetical situation where the respondent needed major surgery. Respondents that perceived higher levels of community commitment of their local hospital were more likely to choose that hospital. Among those who reported their local hospital cares “a lot,” 70 percent stated they would choose that hospital compared with 34 percent who reported “some,” 28 percent who reported “a little,” and 22 percent who reported “not at all” (p < .001).
We then adjusted for demographic and health characteristics using multivariate logistic regression. The results are presented in Table 3. Those who reported the highest level of perceived community commitment of their local hospital were more likely to state they would choose that hospital (OR = 8.24, p = .007). The intermediate levels of perceived community commitment were not associated with hospital choice when compared with the lowest level of perceived commitment. Among the demographic and health characteristics we included in our models, African American race, lower educational attainment, middle age (age thirty to forty-nine), and presence of a chronic health condition were associated with a lower likelihood of choosing their local hospital (Table 3). There was no significant interaction between perceived community commitment and race.
Perceived Community Commitment of Local Hospital and Likelihood of Choosing that Hospital for Major Surgery.
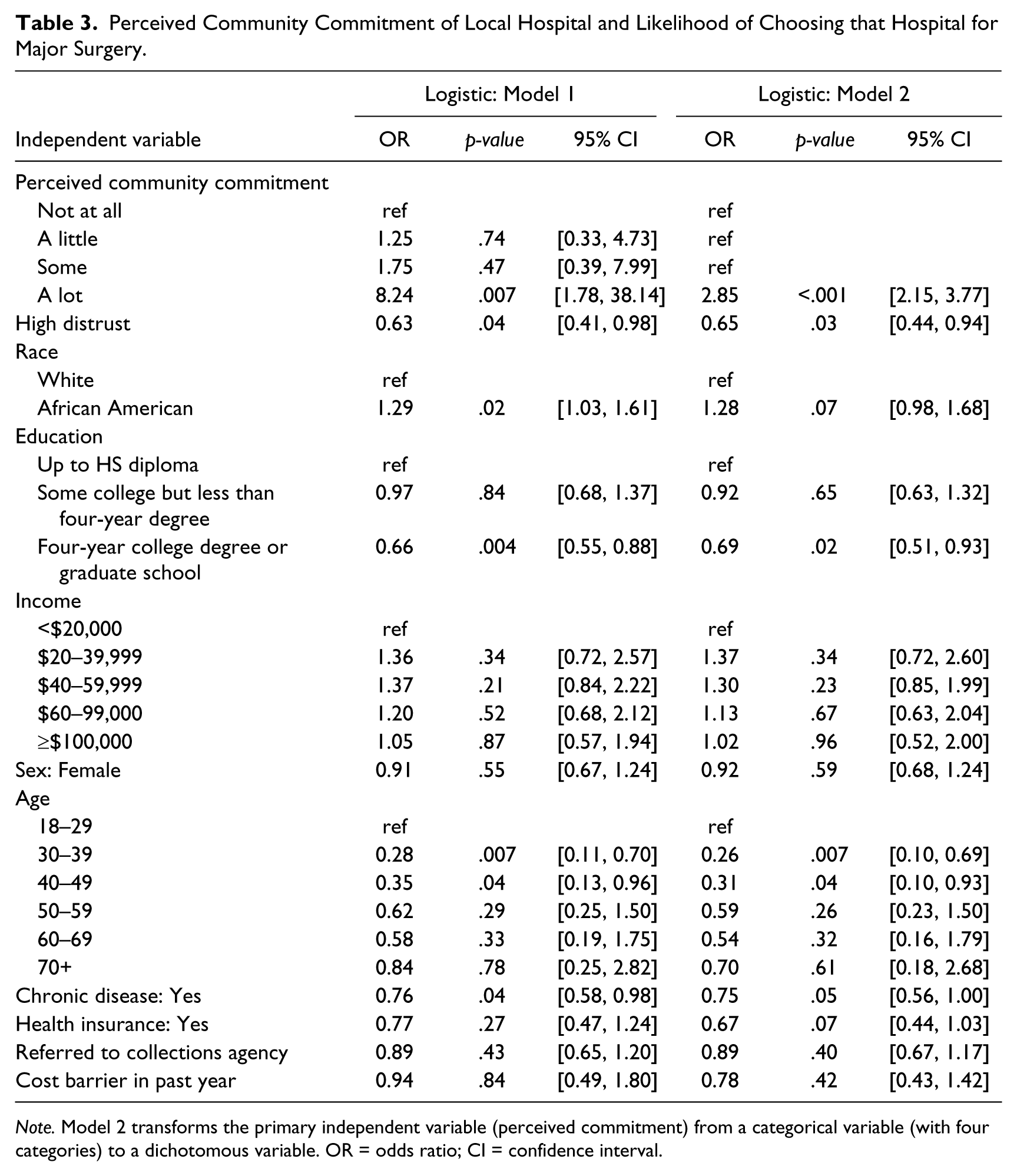
Note. Model 2 transforms the primary independent variable (perceived commitment) from a categorical variable (with four categories) to a dichotomous variable. OR = odds ratio; CI = confidence interval.
Community Commitment and Distrust
We tested unadjusted associations between perceived community commitment and distrust in the health care system. Respondents that perceived higher levels of community commitment of their local hospital were less likely to report high levels of distrust. Among those who reported their local hospital cares “a lot,” 16 percent reported high health care distrust compared with 29 percent who reported “some,” 34 percent “a little,” and 49 percent who reported “not at all” (p < .001). We adjusted for demographic and health characteristics using multivariate logistic regression (Table 4). Respondents who reported the highest level of perceived community commitment of their local hospital were less likely to report high levels of distrust in the health care system. There were no statistically significant associations between intermediate levels of perceived hospital community commitment and distrust. Higher educational attainment, female sex, and lower social trust were also independently associated with higher levels of health care system distrust. We repeated the multivariate analysis with distrust as a continuous variable and found a similar relationship.
Perceived Community Commitment of Local Hospital and High Distrust of Health Care System.

Note. Model 2 transforms the primary independent variable (perceived commitment) from a categorical variable (with four categories) to a dichotomous variable. OR = odds ratio; CI = confidence interval.
Discussion
A majority of respondents in our survey had very favorable views of their local hospital’s commitment to the health of their community. However, a sizable minority (almost 40 percent) held equivocal or negative views about their local hospital. Patients who have very favorable perceptions of their local hospital were more likely to report they would choose their local hospital if they needed major surgery rather than seek care elsewhere. Similarly, these patients were less likely to report high levels of distrust in the health care system. Race did not modify either relationship.
Our study has several limitations. First, the findings may not generalize to the U.S. population. Our results are representative of African American and white patients residing in large metropolitan areas of the United States where multiple hospitals are likely to be accessible for a planned major surgery. While more than 40 percent of the U.S. population lives in the metropolitan areas represented in our study, hospital choice in rural areas or even smaller metropolitan areas may be much more constrained. Second, we had a relatively low response rate to our survey. Nonresponders may differ from responders in important ways. Third, the survey asked patients about a hypothetical future health care decision because the ability to assess actual behavior surrounding surgery was limited by sample size and measurement issues. However, intentions have been shown to be strongly correlated with behavior in many settings, and it is unlikely that any misclassification of actual hospital choice would lead to bias in the association with perceptions of hospital community commitment (Kim and Hunter 1993). Fourth, we did not measure hospitals’ community benefit activities, so we do not have any way to know the extent to which hospital’s actual community activities correlate with patient perceptions. We also did not have data on the for-profit status of hospitals. Although one prior study suggests patients may perceive nonprofit hospitals to be of lower technical quality (Schlesinger, Mitchell, and Gray 2004), it is not clear patients are aware of the profit status of individual local hospitals or that they necessarily associate profit status of an individual hospital with community commitment. However, our primary interest was on understanding the potential impact of perceptions of community commitment. Future studies are needed to understand what hospital activities, characteristics, or behaviors drive these perceptions and whether activities that have a clear community health benefit improve perceptions. Finally, our study is not able to demonstrate causal relationships, a limitation of most cross-sectional survey research. For example, we are unable to measure whether community commitment truly shapes health care system distrust or whether health care system distrust is a lensthrough which patients judge the community commitment of health care institutions.
Our study has several implications. Given that perception of community commitment appears to influence choice of hospital for a planned major surgery, there may be an unrecognized or underappreciated business case for community benefit activities. In addition to the potential tax benefits, hospitals may find that investments in their community relationships may improve their ability to attract more patients for services such as a planned “major surgery” (as we asked in our survey) that often have relatively high profit margins. At the same time, this investment may be synergistic with future changes to payment systems that demand more population-level accountability. Furthermore, if these same investments in community relationships could lead to lower levels of distrust in the health care system, there are other potential benefits to hospitals including higher patient satisfaction and adherence, important factors in current and future efforts to assess health care quality. Given that our study does not measure the relationship between particular community benefit activities or the marketing of such activities and patient perceptions, future research is needed to determine which activities would have the greatest impact in these arenas. This would help determine whether community benefit activities with the greatest population health impact could be aligned with the business interests of a hospital.
The discussion of community benefit has been dominated by controversy over how to measure it and creating policies that establish minimum standards for nonprofit hospitals (Buchmueller 1996; Gray 1996; Pauly 1996). As a reflection of this controversy, the IRS recently started requiring nonprofit hospitals to start measuring and reporting their community benefit activities (Hellinger 2009). While this effort is important as a matter of public policy and accountability of public dollars, these activities may have benefits for hospitals beyond their tax-exempt status. Perhaps the goals of the community and hospital financial performance may be more aligned than previously thought.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:David Grande reports serving as an expert witness on behalf of the Attorney General of the State of Vermont, received honoraria from Johns Hopkins University CME Program, served as a voluntary member of the Board of Directors of the National Physicians Alliance (previously) and Healthy Philadelphia (currently).
Funding
The author(s) disclosed receipt of the financial support for the research, authorship, and/or publication of this article:This research was supported by the National Human Genome Research Institute (R01 HG 2689-01) and the American Cancer Society (Research Scholar Award PBP-104351). David Grande received support from the Healthwell Foundation.