
Abstract
Racial/ethnic minorities are less likely to use higher-quality hospitals than whites. We propose that a higher level of information-related complexity in their local hospital environments compounds the effects of discrimination and more limited access to services, contributing to racial/ethnic disparities in hospital use. While minorities live closer than whites to high-volume hospitals, minorities also face greater choice complexity and live in neighborhoods with lower levels of medical experience. Our empirical results reveal that it is generally the overall context associated with proximity, choice complexity, and local experience, rather than differential sensitivity to these factors, that provides a partial explanation of the disparity gap in high-volume hospital use.
Introduction
Racial/ethnic disparities in health status and medical utilization have become a focus of research (Institute of Medicine [IOM], 2003) and a concern for policy makers (Ladenheim and Groman 2006). While a portion of these disparities can be attributed to insurance coverage and broader socio-economic differences, even after accounting for these factors, there remain health care disparities (IOM 2003; Medical Care Research and Review [MCRR], 2000). Only about 20 to 25 percent of the nation’s physicians and hospitals provide most medical care for minority patients (Bach et al. 2004; Jha et al. 2007; Jha et al. 2008), and a range of quality disparities are associated with these providers and facilities: broad quality measures are lower for the hospitals and nursing homes used by minorities (Gaskin et al. 2008; Hasnain-Wynia et al. 2007; Hasnain-Wynia et al. 2010; Jha et al. 2007; Jha et al. 2008; Smith et al. 2007); process measures for specific conditions indicate lower quality (Barnato et al. 2005; Bradley et al. 2004); and minority patients are less likely to receive new treatment technologies (Groeneveld, Laufer, and Garber 2005). Blacks receive care from hospitals and surgeons with higher mortality rates (Clarke, Davis, and Nailon 2007; Konety, Vaughan Sarrazin, and Rosenthal 2005; Lucas et al. 2006; Mukamel et al. 2007; Mukamel, Weimer, and Mushlin 2006; Rothenberg et al. 2004; Skinner et al. 2005), and minorities are less likely to use higher-volume hospitals and surgeons (Bach et al. 2001; Birkmeyer et al. 2002; Birkmeyer et al. 2003; Dardik et al. 2000;Epstein et al. 2010; Harmon et al. 1999; Scarborough et al. 2010). These differences persist even after controlling for a variety of other factors (Epstein et al.2010;Gray et al. 2009; Liu et al. 2006; Losina et al. 2007; Neighbors et al. 2007; Trivedi, Sequist, and Ayanian 2006). Moreover, research results have revealed that a large portion of the disparities in quality of care for minorities appear to be associated with between-hospital differences rather than within-hospital differences, that is, racial/ethnic disparities in quality and outcomes are associated with the fact that minorities and whites are obtaining care at different hospitals rather than because they receive different levels of care within the same hospital (Barnato et al. 2005; Bradley et al. 2004; Breslin et al. 2009; Gaskin et al. 2008; Goldstein et al. 2009; Groeneveld et al. 2005; Hausmann et al. 2009; Joynt, Orav, and Jha 2011).
These findings highlight the need to better understand the factors that influence where patients receive care, but there has been relatively little study of the particular pathways that lead to these disparities. In this article, we examine several potentially influential factors, which shed new light on how patients use their local medical delivery systems. Our starting point is the decision-making complexity associated with hospital use and how patient and physician decisions are affected by several features of the local hospital environment, including what we will term proximity, choice complexity, and local medical experience. As we document below, minority patients in the United States generally live relatively close to hospitals, but they face a previously unrecognized set of disadvantages associated with the greater complexity of their hospital markets and their more limited experience with specialized medical services.
Our empirical analysis focuses on racial/ethnic disparities associated with one particular marker of hospital quality: the use of hospitals that are “high volume” providers of surgical services for which there is evidence that higher-volume hospitals have better outcomes (Dudley et al. 2000; Gandjour, Bannenberg, and Lauterbach 2003; Halm, Lee, and Chassin 2002; Luft, Bunker, and Enthoven 1979; Shahian and Normand 2003). 1 Based on a large literature, experts have advised patients to obtain their care from these high-volume hospitals (Agency for Healthcare Research and Quality [AHRQ] 2006; Birkmeyer 2000a, 2000b; Leapfrog Group 2007). A number of issues have been raised on how to act on these findings (Epstein 2002), and some researchers have questioned the use of volume as a guide for patient decision making (Browne, Pietrobon, and Olson 2009; Goshima et al. 2008) and public policy (Glance et al. 2007; Ricciardi et al. 2008). Nonetheless, for our analysis, procedure volume is a useful marker for examining where racial/ethnic minorities are treated and how their responses to hospital quality information may differ from white patients. For a number of years, especially in the period we examine, the volume–outcome relationship in hospitals was publicized in press accounts of research, and information on hospital volume became more widely available to consumers. And by the end of the 1990s, this relationship was recognized by the public: roughly two-thirds of Americans viewed the extent to which a hospital is “experienced with a given test or procedure” as revealing “a lot” about quality of care (Kaiser Family Foundation [KFF], 2000), and minorities appeared as aware of this relationship as whites (Gray et al. 2009).
As we show below, although minorities live closer than whites to these high-volume facilities, they are systematically less likely to receive care at these hospitals. Minority group members in the United States face a number of general and well-known disadvantages, including discrimination, more limited levels of economic and social resources, and difficulties in obtaining access to services. Our analysis suggests that greater complexity in the hospital markets where minorities live creates an additional set of challenges. For most minority patients, while high-volume hospitals are geographically accessible, there are often a large number of low-volume hospitals nearby as well. Drawing from the literature on decision making and bounded rationality, we hypothesize that information demands, lower levels of local experience, more limited physician assistance, and lower levels of trust make it more difficult for minority patients to navigate the health care system and identify higher-quality providers. These difficulties are magnified by the complexity of the urban hospital markets where most minority group members live in the United States, and this offsets the advantages of proximity that minorities should have when obtaining hospital care.
As we develop below, complex decision-making environments may affect the observed pattern of hospital use in two distinct ways: First, white patients may have greater advantages and minority patients greater disadvantages in adapting to decision-making complexity. And so, white and minority patients may be observed to be responding differentially, with lower and higher levels of sensitivity to the decision-making environment. Second, minorities and whites might simply be situated in different circumstances, with minorities living in decision-making environments that are more complex. Decision-making complexity might then have a greater impact on minority patients, even if for any given level of complexity, white and minority patients respond similarly to the level of complexity.
Our empirical contribution uses hospitalization data from four states. We use these data to describe the magnitude of racial/ethnic disparities and present a set of multivariate models that estimate the impacts of proximity, choice complexity, and local medical experience on these patterns of high-volume hospital use. All three factors play a role and together are associated with about half of the observed racial/ethnic disparity in the use of high-volume facilities. Importantly, our results show that for some, but not all, of the factors we measure, minorities are differentially responsive to complexity, at least for several specific services. But for explaining the impact on the overall level of disparities, the effects of living in different market circumstances are strong and consistently found for all services that we examined, while differential sensitivity is found for only some of the factors we examine, for only some services, and it is often only modest in size. Thus, based on these data, the results indicate that the main choice-related disadvantages for minority patients are associated with simply living in a complex hospital market context and are largely not because minority patients respond differently to the various factors that influence hospital choice.
Hospital Choice: Complex Choice Sets and Bounded Rationality
Over the last three decades, researchers have explored the implications of bounded rationality and the decision-making biases that emerge under conditions of limited information for a broad range of decisions, including medical decision making (Diamond and Vartiainen 2007; Frank 2007; Rabin 1998; Simon 1987; Tversky and Kahneman 1974). We draw on this literature for our conceptual model, which focuses on how information availability and complexities in the choice environment affect patient decisions concerning hospital care. The choice circumstances of white and minority patients differ in important ways, and these differences create a previously unrecognized source of racial/ethnic disparities in the use of high-volume hospitals.
Our model of hospital choice starts with the general effects of limited information on decision making. When making decisions under conditions of limited information, individuals use a variety of strategies. These include relying on information derived from social networks (Pauly and Satterthwaite 1981), and while other sources of information have emerged, most Americans continue to use experiences of family and friends rather than expert evaluations when making medical decisions (KFF 2008). In addition, consumers employ various psychological heuristics and decision-making rules-of-thumb by, for instance, using examples that are familiar and that come readily to mind (Tversky and Kahneman 1973), following similar decisions by others (Thaler and Sunstein 2008, chap. 3), extrapolating from a small number of experiences or reports from others (Rabin 2002; Tversky and Kahneman 1971), staying with the status quo (Samuelson and Zeckhauser 1988), and following a satisficing norm (Simon 1987). These strategies allow patients to make decisions with limited information. At the same time, these strategies also reduce the incentive to gather additional information, which further reduces the likelihood of identifying higher-quality hospitals, and reinforces patients’ tendencies to choose hospitals based on convenience or familiarity.
The difficulty of analyzing medical care options increases as the number of provider options expands, creating a situation of potential “choice overload” (Iyengar and Kamenica 2007). Consumers who face choice overload often make poor decisions, and the presence of additional options may be overwhelming, leading them to disengage from the process (Gilovich and Medvec 1995), refuse to make any decision at all (Anderson 2003; Iyengar and Lepper 2000), reduce the number of alternatives under active consideration (Johnson et al. 1993; Payne, Johnson, and Bettman 1993), and defer to others who might choose for them, potentially reinforcing patient deference to their physicians (Frank 2007).
Choice overload will be especially likely in urban areas, where services are available at multiple institutions. Because the probability of choice overload increases with the complexity of the choice set, an abundance of hospital options may impede decision making. This is compounded by inadequate information and the resulting use of decision shortcuts: poorly informed patients will have greater difficulties identifying higher-quality hospitals and will rely on convenience and local referral patterns that may lead them to lower-quality hospitals. Moreover, if choice overload causes patients to disengage psychologically, they become more likely to rely on familiarity, allow others to guide their choice, or adopt a satisficing approach, assuming that any hospital will deliver care of adequate quality. These heuristics will increase the likelihood of using lower-quality hospitals and bypassing higher-quality hospitals.
Implications for Racial/Ethnic Disparities
The limitations on information availability and the difficulties of navigating complex choice situations are likely to disproportionately affect minorities. Minority patients have more limited access to informal sources of information and tend to live in urban areas where decision making is complex due to the relatively large number of hospitals. These difficulties would be less consequential if patients could simply defer to their providers, but minorities are also less connected to sources of medical guidance and less trusting of the medical care system.
First, minority patients have weaker connections to physicians than do whites: they are less likely to have a regular source of care, are more likely to use clinics or hospital outpatient departments as their usual source of care, have fewer outpatient visits than whites, and are less likely to be insured (Lillie-Blanton, Martinez, and Salganicoff 2001). Second, even when connected with a primary care clinician, minority patients face hurdles to obtaining high-quality care, and this can affect every stage of medical utilization (Einbinder and Schulman 2000). Physicians who treat minority patients report greater difficulty obtaining referrals and admissions (Bach et al. 2004), and minorities are more likely to have minority physicians, who themselves report greater difficulties in obtaining services (Hargraves, Stoddard, and Trude 2001). Minority patients use surgeons with higher mortality rates, especially when their primary care physicians have had more limited experience with the hospitals used (Mukamel, Weimer, and Mushlin 2006).
Moreover, compared with whites, minority patients have a lower level of trust toward the health care system, and they are thus likely to give additional weight to obtaining care from facilities that are seen as trustworthy. Various forms of discrimination contribute to their lower levels of satisfaction and perceptions of receiving lower-quality care (Blendon et al. 2008; LaVeist, Nickerson, and Bowie 2000; Lillie-Blanton et al. 2000). Cultural factors and language create difficulties (Brach and Fraser 2000), and minority patients who have been hospitalized report less respect for patient preferences than do whites (Hicks et al. 2005). Trust may be particularly relevant for minorities in that the use of high-volume hospitals may require that they cross social and geographic boundaries to obtain care from providers located outside their own neighborhoods, or in institutions generally perceived as “white.”
In combination, these factors increase the difficulties that minority patients face in negotiating their way through the health care system. Under these circumstances, we hypothesize that they will fall back on various decision heuristics about where to receive their inpatient care, such as simply seeking treatment at other nearby hospitals, which are familiar to patients and their social networks, and convenient because their current clinicians practice in these hospitals. The converse is found for white patients—at the individual, neighborhood, and market levels, white patients benefit from a number of socio-economic advantages that facilitate adaptations to this complexity.
Local Experience
As just discussed, patients tend to rely on their social networks when making medical decisions. Compared with whites, patients from minority groups are more reliant on these informal sources of information than on published performance measures (Gray et al. 2009). Moreover, minorities have lower average levels of formal education than whites, which may reduce their ability to obtain and analyze publicly available information about hospital quality. As the rate of utilization for any particular procedure varies by location, there are places where prospective patients will have a large number of potential informal advisers with personal experiences, and neighborhoods where these experiences are more limited. The reliability of this informal advice is likely to be higher in communities with a relatively high procedure utilization rate compared with communities with lower rates. But because neighborhoods with concentrated minorities tend to have below average income and education levels, and lower rates of insurance coverage and procedure utilization, the level of experience in a typical minority patient’s social network is likely to be less than for white patients.
Choice Overload
Choice overload is more likely to affect minority patients for two reasons. First, because minority populations often live in larger urban areas, they are more likely to face complex choice sets for inpatient care. Second, because many minority populations have lower levels of educational attainment, fewer minority patients will have developed the skills for dealing with complex choices.
Proximity and Distance
As we have argued, minorities have more limited access to relevant information about hospital quality and lower levels of physician assistance in making hospital decisions, at the same time that they live in more complex medical markets. One heuristic that patients might use when it is difficult to collect and assess information on numerous potential hospitals is to simply choose any nearby hospital. Although this may not be optimal as an approach for identifying higher-quality hospitals, it does minimize the need to analyze a complex array of information. In addition, a patient’s physicians are more likely to practice at nearby hospitals and will be familiar with the staff and affiliated physicians. Finally, with the lower level of assistance from physicians, minority patients are relatively more reliant on their social networks for advice, leading minority patients to be more likely to act on the basis of familiarity and the hospital experiences of friends, family, and neighbors—experiences which will be disproportionately based on care received from nearby hospitals.
Data and Methods
Based on the literature on volume and outcomes, we chose volume-sensitive services with sufficient sample sizes to provide reliable estimates, including three cardiovascular procedures, three types of cancer surgery, three orthopedic procedures, and two prostate procedures. 2 The outcome of interest is whether patients used a hospital that was a high-volume provider for the specific procedure or condition for which they were admitted, based on whether the hospital’s average annual discharges (averaged over the two-year period) met or exceeded evidence-based volume thresholds. For coronary artery bypass grafts, coronary angioplasty, and carotid endarterectomy, thresholds recommended by the Leapfrog Group were used, while for the remaining services, thresholds were based on the median volume level associated with better outcomes in the studies reviewed by Halm, Lee, and Chassin (2002). (The specific thresholds we used are presented in Table 1.)
Racial/Ethnic Disparities in Use of High-Volume Hospitals: Combined Data for Arizona, Florida, New Jersey, and Wisconsin, 2001–2002.

For each service, the cell indicates the fraction using high-volume hospitals and, in parentheses, the sample size for each racial/ethnic group. Limited to patients with valid zip codes receiving care from in-state hospitals. Excludes American Indians/Alaska Natives.
p ≤ .05. **p ≤ .01. ***p ≤ .001, for difference between each racial/ethnic minority group with whites.
We use hospitalization data for residents of Arizona, Florida, New Jersey, and Wisconsin for eleven surgical procedures in 2001–2002. These states represent the major regions of the United States and were chosen to capture the range of patient demographic characteristics. 3 These particular years are a good period to assess patient responses to information: over the previous decade, the research literature identifying the relationship between hospital volume and quality had grown substantially, significant efforts to inform the public about hospital quality had begun, and volume came to be seen as a relevant consideration for patient choice. The years 2001–2002 thus represent a period when patients were beginning to act on this information, and there might be significant racial/ethnic differences in patient responses based on access to information and the nature of decision-making complexity.
The data are based on hospital-reported information for acute care, nonfederal hospitals, collected by state agencies, and reported to the Health Care Utilization Project (HCUP). These State Inpatient Data files include all hospitalizations for nearly all nonfederal hospitals in these states. In addition to diagnostic and procedure information and patient characteristics, the data include patient zip codes, which were used to measure proximity to hospitals, and the socio-demographic characteristics of patients’ neighborhoods, based on zip code tabulation area data obtained from the Bureau of the Census.
Because of the relatively small number of observations for less common procedures, we limited the descriptive portion of this analysis to only the four largest racial/ethnic groups in the United States, coded into mutually exclusive categories: Hispanic origin (Latino), and the non-Hispanic racial categories of white, black (African-American), and Asian/Pacific Islander. Other patient characteristics obtained from the HCUP data were age, gender, insurance (Medicare, Medicaid, private insurance, uninsured), whether insurance involved managed care, whether the admission was a routine admission (as opposed to an emergency admission), and whether the patient was transferred from another hospital. The complexity of the patient’s condition was measured by an index of comorbidities (Elixhauser et al. 1998). We measured patients’ socio-economic backgrounds using Census 2000 data for each patient’s zip code, computing average household income and educational attainment based on the percentage of residents over age twenty-five who have graduated from high school but not college, and the percent college graduates.
Other aspects of neighborhoods and geographic location may be relevant too. To control for patterns of residential segregation and the geographic concentration of minorities, we also included the racial/ethnic composition of the zip code, measured as percent African-American and percent Latino. There may also be differences between urban, suburban, and rural areas in the access to medical care and communication of medical information. We proxy for these factors using the level of urbanization, measured by the percentages of the zip code population living in rural areas and in places with a population less than fifty thousand persons. 4
Proximity was measured by the distance to the closest hospital (regardless of volume) that provides each service, the distance to the nearest high-volume hospital for that service, and a dichotomous variable indicating whether the closest hospital is also the nearest high-volume hospital. Distances were calculated using the geographic centroid of the patient’s zip code and each hospital’s location as reported in the 2001 American Hospital Association annual survey. Because multi-hospital chains often report only a single headquarters address, and because of limited address information on some hospitals, we supplemented this information with street address information obtained from other sources.
To measure the complexity of patient choices, we determined the number of hospitals that provide each service within a 40-mile radius of the patient’s zip code, as well as the number of low-volume hospitals that are closer to the patient’s zip code than the nearest high-volume hospital. 5 For our measure of local medical experience, we calculated a population-based incidence rate of each procedure using the number of procedures aggregated to the three-digit zip code area divided by total population for that area.
Results
The left-hand columns of Table 1 present rates of high-volume hospital use for the eleven services. Our main disparity measure is the difference between the fraction using high-volume hospitals for each minority group and the fraction for whites, which we present in the center columns. For patients from all distances, African-Americans have significantly lower rates than whites for nine of the eleven services, and Latinos have significantly lower rates for six of the eleven. For Asians, the sample sizes and the differences from the white rates are smaller, and the pattern is more mixed.
African-Americans, Latinos, and Asians living in the United States and in these four study states are more likely than whites to live in urban areas, and because proximity is important for hospital utilization, these disparity measures may be partially misleading. A simple correction for geographic accessibility is to limit the sample to patients living within 10 miles of a high-volume hospital (right-hand columns). In general, the observed rates of high-volume hospital use are higher with this sample restriction, and this is especially true for whites, as they typically live farther from high-volume hospitals. Limited to patients with ready geographic access, much larger racial/ethnic disparities are observed. For both African-Americans and Latinos, ten of the eleven services show a significant disparity compared with whites, with differences ranging between 5 and 23 percentage points. And with this sample restriction, Asians show disparities relative to whites, although these gaps are generally smaller than for the other two minority groups, and only four are significant.
To determine whether information availability and decision complexity are associated with disparities in hospital use, we focused on six of these services. These services have sufficiently large sample sizes to support multivariate modeling for the largest racial/ethnic groups, although because sample sizes for Asians are much smaller, we also limited the rest of this analysis to whites, African-Americans, and Latinos. Table 2 presents several descriptive measures of proximity, choice complexity, and local experience which show important differences for white and minority patients. The top two sets of lines show that whites’ greater usage of high-volume hospitals is not because these hospitals are closer: For all six services, whites live farther from high-volume hospitals than either African-Americans or Latinos. At the same time, whites may have one decision-making advantage: although living farther away from hospitals in general, for whites, the closest hospital is more often a high-volume hospital.
Proximity, Choice Complexity, and Local Experience: Summary Statistics.

Importantly for our analysis of choice complexity, the data indicate that many patients face large choice sets, and these choice sets are larger for minority patients: white patients typically live in markets with twenty to twenty-two hospitals offering the service, while minority patients face twenty-six to thirty hospitals. 6 Less than half of these hospitals are high-volume and for some services, only a small fraction meets the designated volume thresholds. Moreover, while there are more high-volume hospitals in market areas where minorities live, there are typically additional low-volume hospitals that also provide these services. The result is that compared with whites, minorities generally face a choice context that features both a higher number of lower-volume hospitals that are closer than the nearest high-volume hospital and a lower chance that the closest hospital is a high-volume hospital.
Finally, a third aspect of information availability is the experience embedded in local social networks. As shown in Table 2, minorities tend to live in areas with lower levels of this experience-based information availability, as measured by lower levels of utilization and lower percentages living in areas with above average utilization rates for the six services.
Multivariate Modeling
The descriptive statistics suggest that proximity, choice complexity, and local experience may affect minorities and whites differently, and might help explain a portion of the disparities identified in Table 1. To examine these factors together and to control for other confounding influences, we estimated a series of linear regressions, modeling the decision about using high-volume hospitals as a dichotomous choice. 7 In Table 3, we present the key results from these models. 8
Use of High-Volume Hospitals: Linear Probability Models.

Note. Individual-level age, gender, comorbidities, whether the admission was routine (as opposed to emergency), whether it represented a transfer, the source of payment (Medicare, Medicaid, private insurance, uninsured), whether the insurance involved managed care are based on the Health Care Utilization Project (HCUP) hospitalization files. The percentage of high school graduates, the percentage of college graduates, average household income, the percentage of African-Americans, the percentage of Latinos, and the percentages living in rural areas and places with populations of less than 50,000 persons are measured at the five-digit zip code level using the Census 2000 Zip Code Tabulation Area (ZCTA) files. For the zip code–level variables, the left-out comparison variables are the percentage with less than high school education, percentage white, and percentage living in places with 50,000 or more persons. Distances to hospitals, determination of the closest hospital, and the counts of the number of local hospitals were based on patient zip codes combined with hospital zip code information. Local utilization rates were calculated at the three-digit zip code level for each service and represent total cases per 1,000 population. The models also include fixed effects for the states (Florida, New Jersey, Wisconsin, Arizona). Because of relatively small sample sizes, patients coded as Asian/Pacific Islander, American Indians/Alaska Natives, Other race, or unknown race were excluded from the data sets used for these estimates.
For each complexity measure, the results include both a main effect coefficient (on the line with a description of the variable), and two coefficients for interactions with African-American and Latino (on lines with the name of the racial/ethnic group). Non-Hispanic whites are the left-out group.
p < .05. **p < .01. ***p < .001.
We discuss the results in two steps: First, we present the results for the main effect coefficients—results that apply to all patients, including minority patients. These main effect results indicate strong and statistically significant effects consistent with the approach we outlined above. As the decision contexts faced by minority patients differ from those of white patients (see the summary statistics presented in Table 2), adjusting for these main effects has a substantial impact on explaining racial/ethnic disparities in high-volume hospital use, a finding which we will highlight later in our presentation of Table 4.
Alternative Models: Adjusted Probabilities and Racial/Ethnic Differences Logit Probability Models.

Adjusted probabilities based on logit coefficients and estimation sample means for Whites, African-Americans, and Latinos combined. The Main Effects Models and the models with race/ethnicity interactions both control for demographic and medical characteristics, payment source, neighborhood demographic and urbanization characteristics, and state fixed effects. For details about variable specification, see note on Table 3.
We follow this with a discussion that focuses on the coefficients measuring the interactions for race and ethnicity. For some procedures and specific minority groups, the interaction results modify the main effects, but except for the level of local experience and certain aspects of proximity and complexity, the interaction results generally indicate only a modest degree of differential responsiveness by minority group members. The net impacts on use of high-volume hospitals are largely determined by the main effects results in combination with the substantial differences in the decision-making context for minorities.
Main effects
The coefficients for the decision making variables are presented in the lower portion of Table 3.The main effect coefficients provide evidence that all three factors are associated with use of high-volume facilities. 9 As we proposed in Hypothesis 1, local experience has an impact, with higher levels of local experience associated with greater use of high-volume hospitals for all but one service. These coefficients imply that an increased local utilization rate of one case per thousand would be associated with a 3 to 5 percentage point increase in patient use of a high-volume hospital. 10
Our second hypothesis concerned choice complexity. The estimated coefficients for the choice complexity variables are in the expected negative direction for three of the services, although this is combined with positive coefficients for some services. Consider first the effect of one additional hospital within 40 miles: such a change alters the probability of obtaining care at a high-volume hospital by 0.1 to 0.3 percentage points. In urban areas with numerous hospitals, the cumulative effect for these services would be larger: patients living in an area with ten additional hospitals would have a reduction in high-volume hospital use of up to 3 percentage points. Much more important quantitatively are the estimated impacts of our separate measure of complexity and local hospital diversion: as hypothesized, an additional lower-volume hospital that is closer than the nearest high-volume hospital reduces high-volume hospital use—by 5.5 percentage points for coronary bypasses and 2 to 3 percentage points for carotid endarterectomy, lung cancer surgery, and total hip replacement. The effects are smaller but still negative for total knee replacement and open prostatectomy.
Distance to the nearest high-volume hospital has a negative relationship to high-volume hospital use, and distance to the closest hospital also affects hospital use. Patients for whom the closest hospital is a high-volume hospital are more likely to receive their care at a high-volume hospital. The coefficients on the distance to the nearest high-volume hospital range from −0.002 to −0.008. To interpret these coefficients, consider a change in distance of 10 miles: depending on the service, patients who live an additional 10 miles farther from a high-volume hospital are 2 to 8 percentage points less likely to receive their care at high-volume hospitals. The effects of distance to the closest hospital are comparable in magnitude—a difference of 10 miles alters the use of high-volume hospitals by 3 to 12 percentage points. 11 The dichotomous variable indicating that the closest hospital is high-volume has a large impact, increasing high-volume hospital use between 12 and 38 percentage points.
Interaction effects
The interactions included in the Table 3 models allow the coefficients for proximity, choice complexity, and local experience to vary across the racial/ethnic groups, which permits us to test for whether disparities arise because racial/ethnic minorities are differentially responsive to complexity compared with white patients, or whether disparities arise because minorities are disproportionately located in urban hospital markets that feature a higher level of complexity.
We start by observing that a large portion of the estimated interactions are not significant–indicating that minority patients are not clearly behaving differently compared with whites. These more ambiguous interaction results contrast quite strongly with the main effects results, for which nearly all of the estimated coefficients are statistically significant and large enough to be substantively relevant. For the interactions, of the seventy-two estimated coefficients (six variables of interest for two minority groups for six services), slightly less than half (32 of 72) are significant at the 5-percent level.
Second, the interaction results that are significant and consistent indicate that African-Americans and Latinos are comparatively more responsive to local experience than are whites for several services, as we proposed in our first hypothesis. In particular, this is the case for coronary artery bypass and carotid endarterectomy for both African-Americans and Latinos, and for total knee replacement and lung cancer surgery for Latinos. For coronary bypass, carotid endarterectomy, and total knee replacement, the estimated interaction coefficients for the two minority groups are comparable in magnitude to the estimated main effects, and thus minorities are shown to be approximately twice as responsive to local experience as are white patients. 12 This enhanced responsiveness, however, is not shown for the remaining services. As we argued above, minority patients suffer from a number of information and choice-related disadvantages when seeking specialized care. The results for our measure of local experience indicate that when they live in neighborhoods where there is a higher level of experience, they disproportionately benefit from the experience of their neighbors.
The presence of a high-volume hospital as the closest hospital increases use of high-volume hospitals by African-Americans for carotid endarterectomy, lung cancer surgery, and total knee replacement. We hypothesized that less well-informed patients will tend to use nearby hospitals, and when the very closest hospital is also a high-volume hospital, the result is a greater likelihood of receiving care at a high-volume facility. But this effect was not found for Latinos—for two services, Latinos benefited less—suggesting that other factors besides proximity are affecting Latino hospital use.
The remaining interaction results include coefficients that are small in magnitude, inconsistent in direction across minority groups, and generally statistically insignificant. This is the case for the interaction coefficients for the distance variables, supporting a conclusion that except for the proximity effect associated with a nearby high-volume hospital, the effects of distance are similar for white and minority patients. For the measures of complexity—that is, the interactions with the number of hospitals and the number of hospitals closer than the nearest high-volume hospital—there are a number of significant coefficients. However, the magnitudes of the estimated interaction effects are often small. For both measures of complexity, the main effects dominate the results, again indicating that for these factors, white and minority patients are not very different from each other in their responses to choice complexity.
Thus, except for local experience and certain aspects of proximity and complexity, the results do not indicate a high level of differential responsiveness, but instead, the general pattern is that patients of all races and ethnicities are affected by complexity in a similar way, with differences mostly due to the market contexts where patients live. We assess this in Table 4, which reports the results of simulated probability calculations for each racial/ethnic group using the models we estimated. The first set of rows in the table provides the unadjusted probabilities and differences between the racial/ethnic groups shown in Table 1. The second and third sets of rows give the results of the simulations.
These simulations used the sample means and the estimated coefficients from the models to calculate the probabilities that would be expected if members of each of the racial/ethnic groups are assumed to be living in “average” market circumstances. For the second set, we use the overall sample averages and the coefficients from a simplified model that estimates only main effects coefficients for our key variables of interest and coefficients for the control variables included in the models. For the third set of results, we use the interacted models presented in Table 3 that include racial/ethnic interactions with those key variables. Comparing the first and second sets of predicted probabilities shows the effects of our basic model, while the differences between the second and third sets of probabilities reveal the additional effects of incorporating the interaction coefficients into the model.
Compared with the unadjusted probabilities, the full model (third set of lines) reduces the disparity gaps substantially: For African-Americans, the unadjusted gap of 7 to 18 percentage points across the range of services is reduced to 5 to 9 percentage points; for Latinos, the unadjusted gap of 5 to 26 percentage points is reduced to 0 to 17 percentage points. Across the six services, the mean unadjusted disparity gap is 13 percentage points for African-Americans and about 14 percentage points for Latinos. The full model reduces this to 6.3 to 6.8 percentage points. For five of the six services—all except open prostatectomy—the gap is reduced by at least one-third, and for several services, the adjustment reduces the disparity gap by more than half of the unadjusted gap.
However, comparing the second and third sets of results shows that most of this gain is achieved by a model that uses the main effects for our key variables, and that adding racial/ethnic interactions only modestly improves the level of explanation. For example, for total knee replacement, the unadjusted differences are 15.4 percentage points for African-Americans compared with whites, and 15.2 percentage points for Latinos versus whites. Using our main effects model, the predicted rate of high-volume hospital use for minority patients rises, and the differences with whites decline: to 8.5 percentage points for African-Americans and 10.4 percentage points for Latinos. Adding the interactions in the final model reduces these differences to 6.1 and 9.7 percentage points, only moderately different from the differences that result from using the predicted probabilities of the main effects model. Averaging across the six services, the main effects models for both African-Americans and Latinos reduce the apparent disparity with whites by about 6.6 to 7.3 percentage points for these services. On average, the models with the additional racial/ethnic interactions reduce this further by only 0.3 to 0.5 percentage points.
Impact of Complexity
The multivariate results show that, at least for decisions to use high-volume hospitals, there are impacts associated with the presence of nearby, low-volume hospitals, which divert patients away from high-volume hospitals. To provide a more intuitive appreciation of this, we present the rates of high-volume hospital use for patients living in different choice contexts. In Table 5, patients are stratified based on the number of hospitals closer than the nearest high-volume hospital. As the number of additional nearby hospitals increases, use of a high-volume hospital declines—an effect that occurs for all racial/ethnic groups. For example, 87 percent of white patients use a high-volume hospital for coronary bypass if there are no low-volume hospitals closer than the nearest high-volume hospital, but this falls to 59 percent if there is one low-volume hospital that is closer. Similarly, the rates for African-Americans and Latinos fall from 78 to 79 percent to 49 to 54 percent. For nearly all of the combinations of services and hospital contexts shown in the table, the reduction in high-volume hospital use associated with simply adding a nearby low-volume hospital is larger than the size of the disparity gap between whites and minorities.
Choice Complexity and High-Volume Hospital Use.

Importantly, the results in Table 5 show that while this effect occurs for all racial/ethnic groups, it is larger for African-Americans and Latinos than for whites, so racial/ethnic disparities in the use of high-volume hospitals grow as this form of complexity increases. Moreover, because minorities are more likely to live in areas that feature a larger number of nearby low-volume hospitals (see Table 2), they will be disproportionately located in the hospital choice contexts defined by the lower lines of the table. The combined effects of greater sensitivity to choice complexity and location in more complex market contexts increase overall racial/ethnic disparities in high-volume hospital use.
Limited Connectedness, Trust, and Decisions to Bypass Hospitals
As we argued above, minorities have more limited connections to physicians, a lower level of trust in the health care system, and more limited access to guidance and information. Because of this, they may be especially interested in receiving care at familiar institutions. These are not necessarily the closest facilities, and this leads us to one additional observation based on these data.
In general, it would be expected that more familiar institutions will include those that are geographically closest to patients. But the institutions that patients or their social circles are familiar with in a particular area may also be slightly farther away, especially in urban areas where there are a number of hospitals within a relatively short distance. Indeed, familiarity may lead patients to use hospitals that appear to be less conveniently located than the nearest high-volume hospital, and this may account for surprising differences in the patterns of minority hospital use compared with that observed for white patients.
In Table 6, we separate patients into two groups, based on whether the closest hospital providing the service is a high- or low-volume hospital. For the most part, when the closest hospital exceeds the volume threshold, minorities and whites are similar in their use of this facility, although for coronary bypasses, modest differences do seem to exist.
Responding to Proximity Racial/Ethnic Differences in High-Volume Hospital Use.
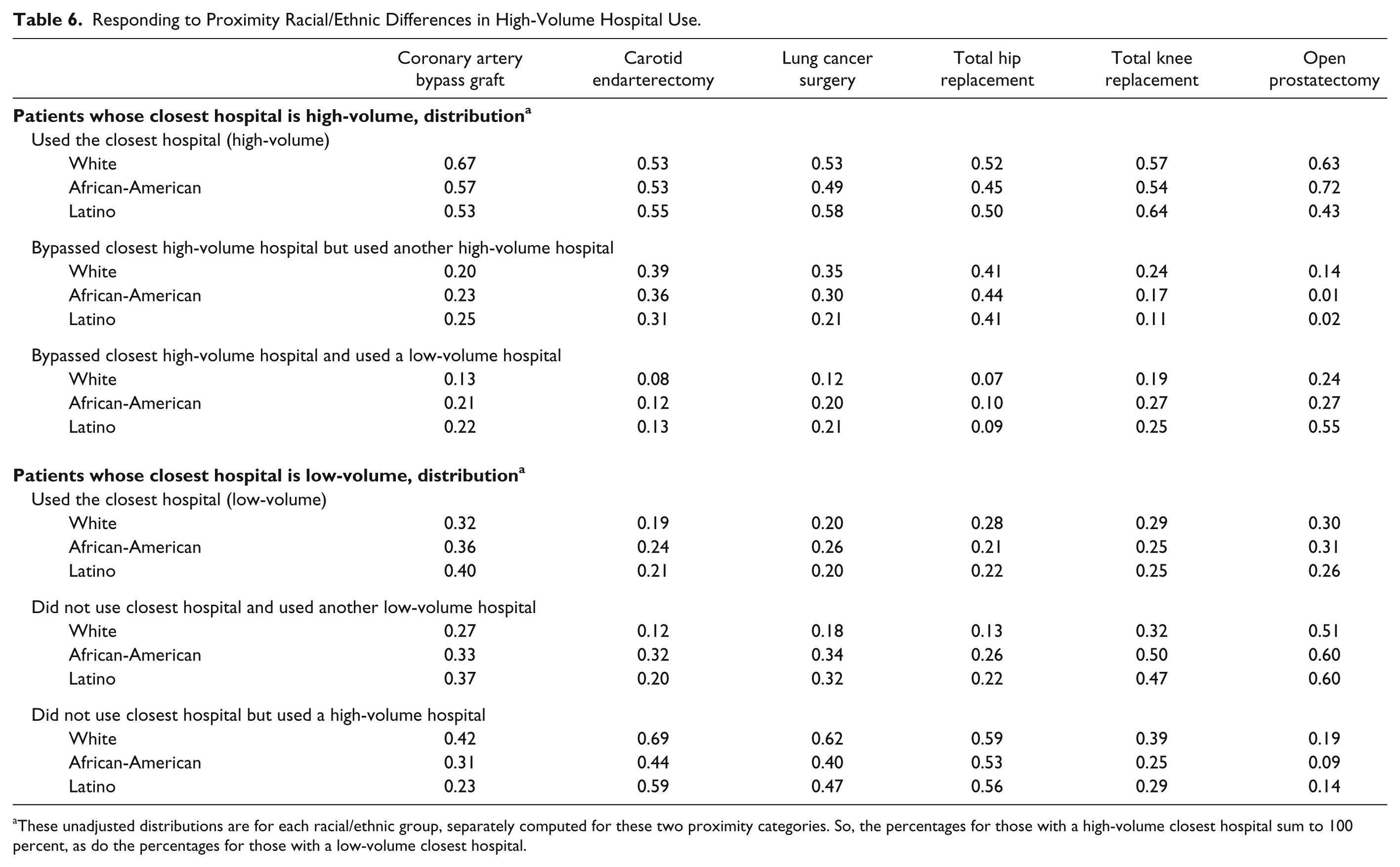
These unadjusted distributions are for each racial/ethnic group, separately computed for these two proximity categories. So, the percentages for those with a high-volume closest hospital sum to 100 percent, as do the percentages for those with a low-volume closest hospital.
More striking and persistent racial/ethnic differences emerge among those who use a hospital that is more distant than the nearest high-volume hospital. White patients who do this are far more likely (for five of the six procedures) to use another high-volume hospital. Similarly, when the closest hospital is a low-volume hospital, for all six services, whites are more likely than minorities to bypass this hospital in favor of a high-volume hospital. In contrast, when African-Americans and Latinos bypass the closest, high-volume hospital, they disproportionately receive care at a low-volume hospital. Similarly, when they bypass a low-volume hospital, they are also more likely to receive care at another low-volume hospital. Thus, for both forms of bypass, a disproportionate share of minorities who do not use the closest hospital ultimately receive care in lower-volume hospitals, while whites who engage in bypass are more likely to obtain care at a high-volume hospital.
Limitations
We note several limitations for this analysis. First, we used data from only four states for 2001–2002. These states were selected based on the availability of patient zip code information essential for our analysis and to capture the range of racial/ethnic groups in the United States. These states are broadly similar to the nation as a whole, but our data are not a nationally representative sample. At this point, we do not have information that disparities in high-volume hospital use have changed over time, but starting around 2008, critiques of the volume–outcome literature began to emerge, and this has the potential for altering patient and provider decision making. It is not clear that this would alter our analysis of the impacts of complexity on hospital decisions for minority patients, but additional analyses that examine more recent time periods and different locations will enhance our understanding of how patients use hospitals, and racial/ethnic differences in those decisions.
Second, the data available for our regression models allowed us to control for a broad range of patient-level characteristics that may affect hospital use, but these data do not include individual or family income or individual-level educational attainment. We constructed proxy measures for these characteristics using zip code–level income and education, but these are not perfect measures of individual patient characteristics. We also control for the racial/ethnic composition of patient neighborhoods, and level of urbanization, but it is possible that there are also other neighborhood and community-level character-istics that affect hospital use.
Third, because our data are based on hospital discharge records, we do not have information about patient perceptions about hospitals, the medical care that may have preceded the hospitalization, and the knowledge and perceptions of their physicians. We also are assuming that the count of number of patients receiving a particular service is an accurate measure of volume, and we lack other potential measures of the quality of care beyond measured volume. It is possible that there are unmeasured aspects of quality that we fail to observe because of our use of volume as a proxy for quality. We also are unable to observe details about the administration of health insurance. Compared with whites, racial/ethnic minorities may be more likely to obtain insurance through managed care plans, and the plans that minorities join may impose relatively greater restrictions on utilization and on access to specialists and hospitals than the plans that serve white patients. Unfortunately, we lack information on all of these issues, which limits somewhat our understanding of why patients of different racial and ethnic groups use the hospitals that they do.
Our results also indicated some differences by racial/ethnic group that we are unable to explain. The economic and social circumstances of each racial/ethnic group differ, and factors other than information and decision complexity undoubtedly contribute to what sources of medical care are used. One difficulty, however, is that there are more limited sample sizes for racial/ethnic minorities, reducing our ability to estimate precisely group differences.
Finally, it should be noted that the market complexity associated with multiple competing hospitals presents not just an information challenge for patients and the professionals who serve these patients. The existence of multiple hospitals and the referral patterns that emerge among primary care providers, specialists, and hospitals in these markets may also lead to segmentation of an area’s medical market and potentially the emergence of de facto segregation of care that may disadvantage racial/ethnic minorities. Future analyses should examine how race and ethnicity interact with historical limitations in access to care, neighborhood residential segregation, provider referral patterns, and hospital market segmentation. These analyses will be helpful for understanding the full range of factors that affect medical care for minority patients and will assist in designing interventions that will enhance patient choices even in the context of complexity and existing patterns of hospital use.
Discussion
These results show that racial/ethnic disparities in the use of high-volume hospitals are common. Our analysis highlights several ways that the decision-making complexity faced by minority patients is associated with lower use of high-volume hospitals. Our results show that patients of all racial/ethnic groups are affected by decision-making complexity, but minorities face greater levels of complexity: African-Americans and Latinos differ from whites with respect to the volume status of their closest hospitals, the degree of choice complexity in their areas, and the extent of local experience with specialized services.
As a result, minorities are less well situated than white patients. Although they live closer than whites to high-volume hospitals on average, minorities live in areas with relatively limited local experience with specialized hospital services, are more likely to reside in places that have multiple, competing hospitals, and are less likely have a high-volume hospital as their geographically closest hospital. These differences are associated with significant reductions in their use of high-volume hospitals, and these differences persist even after controlling for a wide range of individual-level demographic and economic characteristics, as well as neighborhood characteristics including income, education, urbanization, and racial/ethnic residential patterns.
Minorities appear to be somewhat more sensitive to the effects of local experience and proximity. But for the most part, our results indicate that minority patients are generally not very different from whites in their responses to complexity. Importantly, even when the degree of responsiveness is similar, minority patients tend to live in market circumstances where they face higher levels of complexity and lower levels of local experience than are typical for white patients. These differences in circumstances affect the likelihood of receiving care at high-volume hospitals.
Our results are consistent with the expected behavior of patients with limited connections to sources of medical advice who, as a result, are less able to act on quality differences among hospitals. As we hypothesized, overall cognitive complexity does have an effect, but these effects are much smaller in magnitude than the diversionary effects associated with the presence of alternative nearby hospitals. And so, the decision-making complexity that is most prominent is not the existence of numerous hospitals and “choice overload” per se, but the particular difficulties that arise when there are a number of low-volume hospitals nearby. For the goal of encouraging patients, especially minority patients, to use higher-volume hospitals, optimal patient decision making may require that they, in effect, adopt new decision heuristics to shift their attention away from more familiar, but low-volume hospitals, in favor of higher-volume hospitals that are typically geographically accessible as well.
We cannot provide here a full analysis of potential policy interventions that might facilitate such a change, nor can we discuss all of the potential trade-offs that might be raised about potential interventions. But given the importance of these disparities, it may be helpful to comment on a few possible policy implications of our results.
These results reveal one negative consequence of hospital market competition: the existence of multiple, nearby hospitals that provide specialized services tends to reduce the overall use of high-volume hospitals, and this effect is particularly important for minorities living in urban hospital markets. Market competition may have other beneficial effects, giving hospitals, under certain conditions, an incentive to reduce costs, improve quality, and to serve additional patients. But patients in general and minorities in particular might benefit from a reduction in the number of low-volume providers of volume-sensitive services. To the extent that volume is causally related to quality, efforts to consolidate volume-sensitive services at particular hospitals would improve the quality of medical care. And from the standpoint of decision making and cognitive overload, fewer hospitals providing a service would reduce the complexity of the choice situation and the possibility that patients and their referring physicians would choose a relatively low-volume hospital.
The results for local experience suggest that a higher level of information within a community is beneficial for patient decision making in general, and additional local experience often has an especially large benefit for minority patients, which we argue is due to their more limited access to information and sources of medical advice. This in turn implies that efforts to disseminate information about quality differences and to improve connections with providers might lead to better decisions. In recent years, there has been considerable interest in using web-based sources and computer technology to enhance the level of information available to patients and their physicians. While it has the theoretical potential for improving decision making, when there is decision-making complexity, additional information may not have this effect, and if patients differ in how well they can act on it, greater information may even aggravate racial/ethnic disparities and other disparities associated with income and education. From the standpoint of reducing racial/ethnic disparities in hospital use, it is important that the information be tailored to address the choice complexities faced by minorities and that steps be taken to improve the connectedness of minority patients to high-quality physicians and specialists to facilitate decision making about hospital care. Without taking account of these issues, simply introducing additional consumer information using new technology may not achieve the desired improvement in minority health care.
As others have suggested (Bach et al. 2004; Jha et al. 2007), it is also possible that quality-improvement interventions could be focused on the hospitals that minority patients already use, thereby reducing the need for patients to understand hospital quality variations and to incur the costs and difficulties of choosing among multiple competing hospitals. Given the decision-making challenges involved in the choice of hospitals, it may be unrealistic to expect that simply providing additional quality-related information about hospitals will alter patients’ hospital choices to any substantial degree, particularly for procedures about which they may have little or no previous experience. But quality improvement efforts can still enhance many aspects of quality at these hospitals and can lead to better patient outcomes. Implementing these approaches is particularly important in the subset of hospitals that are disproportionately used by minority patients.
Finally, anything that might shift the decision heuristics currently used by patients and referring physicians could have significant social benefits, especially for minority patients who face the disadvantages of a more complex choice context and more limited connectedness to medical advice. Our results show that a significant fraction of minority patients are actually bypassing high-volume hospitals in favor of lower-volume hospitals that are located farther away. Any intervention that would reduce the number of minority patients who bypass high-volume hospitals would have a measurable effect on the overall use of high-volume hospitals for minorities. As one example of bypassing behavior, consider coronary artery bypass surgery. If the rate at which African-American patients bypass a high-volume hospital in favor of a more distant lower-volume hospital could be altered, this by itself could increase the rate of high-volume hospital use by African-Americans by 3 to 8 percentage points. 13 As the overall disparity between blacks and whites for this service is 14.5 percentage points, even a modest change of 3 to 8 percentage points would represent an important reduction in the current disparity gap. One potential decision heuristic for patients and physicians would be to determine whether the nearest hospital is a high-volume hospital for a particular service, and if so, to simply use that hospital rather than some other nearby hospital. Widespread adoption of this heuristic would simultaneously improve patient outcomes, increase convenience, and reduce decision complexity. It is not clear, however, what kind of intervention would alter patient and physician decision making to accomplish this.
Decision-making complexity and the market environment are clearly not the only factors important for understanding racial/ethnic disparities. Minority groups in the United States continue to suffer from the effects of discrimination, de facto segregation in housing and access to services, and a wide range of economic and social disadvantages. To this, our contribution is to add the finding that the medical market context for minorities differs as well. Those areas feature multiple, competing hospitals, and complex physician and hospital referral patterns. Interventions designed to enhance patient decision making and efforts to ameliorate racial/ethnic disparities will need to give explicit attention to these local hospital environments, the potential racial/ethnic segmentation of the market, the nature of patient connectedness to the medical care system, and the information demands of this complexity. For minority patients, the complexity of these environments compounds the more general disadvantages they face, including more limited access to services and more limited levels of economic and social resources, and contributes to the persistence of racial and ethnic inequalities.
Footnotes
Acknowledgements
Helpful comments were provided by participants in the faculty research seminar at the Baruch College School of Public Affairs, and by the editor (Alan Monheit). Thanks are also due to Tracey Thomas, who spent more time than she ever expected locating hospitals and manipulating data sets for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial funding was provided by a grant from the Robert Wood Johnson Foundation (Bradford Gray and Mark Schlesinger, principal investigators) and a Professional Staff Congress/City University of New York faculty grant (Kronebusch).