
Abstract
Internalized homophobia (IH) negatively impacts the mental health of adolescent sexual minority men (ASMM), while self-esteem is posited to bolster their mental health. In a repeated-measures study with 599 ASMM (Mean age = 16.2 [SD = 1.3]; 75.6% racial and ethnic minorities), longitudinal structural equation models investigated the relationships among IH, self-esteem, and mental health (depression and anxiety), as well as the mediating role of self-esteem. Higher self-esteem at earlier time points was significantly associated with lower anxiety and depressive symptoms. The hypothesized mediation pathways were not statistically significant. Subgroup analyses revealed that the protective effect of self-esteem against anxiety was significant for racial and ethnic minority ASMM but not for their non-Hispanic White counterparts. These findings highlight the need for tailored interventions that address the unique experiences of ASMM from diverse racial and ethnic backgrounds.
Adolescence is a pivotal developmental period characterized by a multitude of challenges and experiences that shape individuals’ identities and self-perceptions (Pfeifer & Berkman, 2018). For adolescent sexual minority men (ASMM), this developmental period is accompanied by unique sexuality-related stressors that can significantly affect their well-being. In fact, ASMM experience increased negative mental health outcomes compared to their heterosexual counterparts (Marshal et al., 2011; National Academies of Sciences Engineering & Medicine, 2020). The observed disparities across mental health outcomes has been attributed to ASMM’s internalization of negative societal attitudes and stereotypes about their sexuality (e.g., internalized homophobia (IH) or homonegativity) (Meyer, 1995). Therefore, researchers and practitioners have sought to understand and address the role of IH in ASMM’s mental health (Berg et al., 2016; Newcomb & Mustanski, 2010).
IH may contribute to the development and exacerbation of depression and anxiety symptoms among ASMM (Meyer, 2003). Minority Stress Theory posits that IH may directly and indirectly affect mental health outcomes (Meyer, 2003). The direct effect of IH implies that IH itself can lead to heightened symptoms of depression and anxiety. ASMM who internalize negative societal attitudes and beliefs toward their sexual orientation may experience feelings of shame, self-doubt, and worthlessness, which can contribute to the onset or exacerbation of depressive and anxiety symptoms. The indirect effect posits that IH can influence mental health outcomes through intermediary factors (Szymanski et al., 2008; Williamson, 2000), including various psychological risk factors such as low self-esteem (Hatzenbuehler, 2009).
Self-esteem, defined as an individual’s positive or negative evaluation of themselves (Rosenberg, 1965; Smith et al., 2014), in the context of IH and mental health outcomes among ASMM is crucial for several reasons. Within the psychological mediation framework, self-esteem is posited to be a cognitive mediator between sexuality-related stressors and psychopathology, including emotional distress, suicidality, and substance use behaviors (Hatzenbuehler, 2009). However, the findings regarding the role of negative self-esteem as a mediator have been inconsistent; some studies found self-esteem to be a mediator (Mereish et al., 2022; Savin-Williams & Ream, 2003), while others did not (Austin et al., 2004; Rosario et al., 1996). Self-esteem is also known to have a direct association with depression and anxiety symptoms among youth (Keane & Loades, 2017; Sowislo & Orth, 2013), with large effect sizes between these variables being observed in a meta-analysis (Yeo et al., 2023). Even though IH has garnered particular attention as it encompasses the internalization of societal prejudices, leading to a self-critical and stigmatized view of one’s self-concept (Meyer, 2003), limited research has explored IH’s significance in self-esteem among ASMM. Additionally, few studies have examined whether the association between IH and mental health outcomes is mediated by ASMM’s self-esteem.
A mediating role suggests that IH first undermines self-esteem by fostering negative self-perceptions, which subsequently increases vulnerability to depression and anxiety. This conceptualization aligns with the psychological mediation framework (Hatzenbuehler, 2009), which posits that minority stressors affect mental health through internal cognitive and emotional mechanisms rather than exerting a direct or conditional influence. In contrast, treating self-esteem as a moderator would imply that it merely alters the strength of the relationship between IH and mental health outcomes, without explaining how IH contributes to psychological distress. However, empirical evidence suggests that low self-esteem is not just a contextual factor influencing this relationship but rather a key explanatory mechanism through which IH translates into adverse mental health outcomes (Mereish et al., 2022; Savin-Williams & Ream, 2003).
The experiences and consequences of IH and self-esteem may not be uniform across all ASMM. Racial and ethnic minority ASMM often encounter unique challenges and experiences due to their intersecting identities (Bostwick et al., 2014; McConnell et al., 2018). They are often subjected to distinct forms of discrimination and marginalization that arise from both their sexual orientation and racial/ethnic backgrounds (McConnell et al., 2018). Given these intersecting forms of discrimination, the role of self-esteem in mediating the effects of IH on mental health outcomes may differ between non-Hispanic White ASMM and racial and ethnic minority ASMM. Higher self-esteem may mitigate the negative effects of IH more effectively for non-Hispanic White ASMM, while for racial and ethnic minority ASMM, self-esteem might be less effective due to additional layers of discrimination or different coping mechanisms.
However, it is also important to acknowledge that racial and ethnic minority ASMM have demonstrated resilience in the face of stigma and discrimination, which may shape the role of self-esteem in unexpected ways. Studies suggest that experiences of racial stigma and discrimination, while undoubtedly harmful, can also foster a sense of collective identity, cultural pride, and resilience, which in turn may bolster self-esteem (Meyer, 2010; Singh, 2018). This suggests that rather than uniformly diminishing self-esteem, the lived experiences of racial and ethnic minority ASMM could, in some cases, contribute to a more complex and adaptive self-concept, potentially buffering against the negative effects of IH on mental health. Understanding these variations is crucial for developing targeted interventions.
Despite this, research specifically addressing racial and ethnic differences in IH and self-esteem among adolescents is limited (Fields et al., 2016). Studies of adults show that sexual minority men from racial and ethnic minority backgrounds are more likely to report current IH compared to their non-Hispanic White counterparts (Meanley et al., 2020). For example, Latino sexual minority men reported higher levels of IH compared to non-Hispanic White sexual minority men (Barnes & Meyer, 2012), and Black sexual minority men reported significantly higher levels of IH than individuals from other racial or ethnic groups (Shoptaw et al., 2009). According to intersectionality frameworks (Crenshaw, 1989; Mink et al., 2014), this disparity in IH levels may stem from the compounded effects of multiple stigmatized identities, as racial and ethnic minority ASMM often face both racial discrimination and sexual minority stigma, potentially intensifying internalized negative beliefs. Additionally, dominant cultural and religious norms within some racial and ethnic communities may contribute to stronger anti-LGBTQ+ sentiments, further shaping an individual’s internalized stigma (Quinn et al., 2018). However, it is also important to recognize that focusing solely on IH as a singular form of stigma may not fully capture the complex and multidimensional lived experiences of racial and ethnic minority ASMM. Their intersectional identities—where race, ethnicity, and sexual orientation intersect—can influence IH in ways that differ from those of White ASMM, potentially shaping unique patterns of resilience, identity negotiation, and psychological distress (Bowleg, 2013). Given the documented disparities among sexual minority adults, it is crucial to investigate these differences among ASMM to fully understand how IH affects their self-esteem, depression, and anxiety.
Hypotheses
The goals of this study were to examine the longitudinal associations between IH, self-esteem, and depression and anxiety symptoms in a sample of ASMM at baseline, 6 months, and 12 months. We hypothesized that higher IH at baseline would be associated with lower self-esteem at 6 months, which, in turn, would be associated with worse mental health outcomes (e.g., depression or anxiety) at 12 months (Figure 1). We also hypothesized that the mediation effects of self-esteem on the relationship between IH and mental health outcomes would differ between the two groups. Specifically, we hypothesized that the mediation effect of self-esteem would be stronger among non-Hispanic White ASMM compared to racial and ethnic minority ASMM because IH would have a more direct impact on mental health for racial and ethnic minority ASMM (Cyrus, 2017; DiGuiseppi et al., 2022; Ramirez & Paz Galupo, 2019), with its effects being stronger and less influenced by intermediary factors, such as self-esteem, due to their intersecting identities.
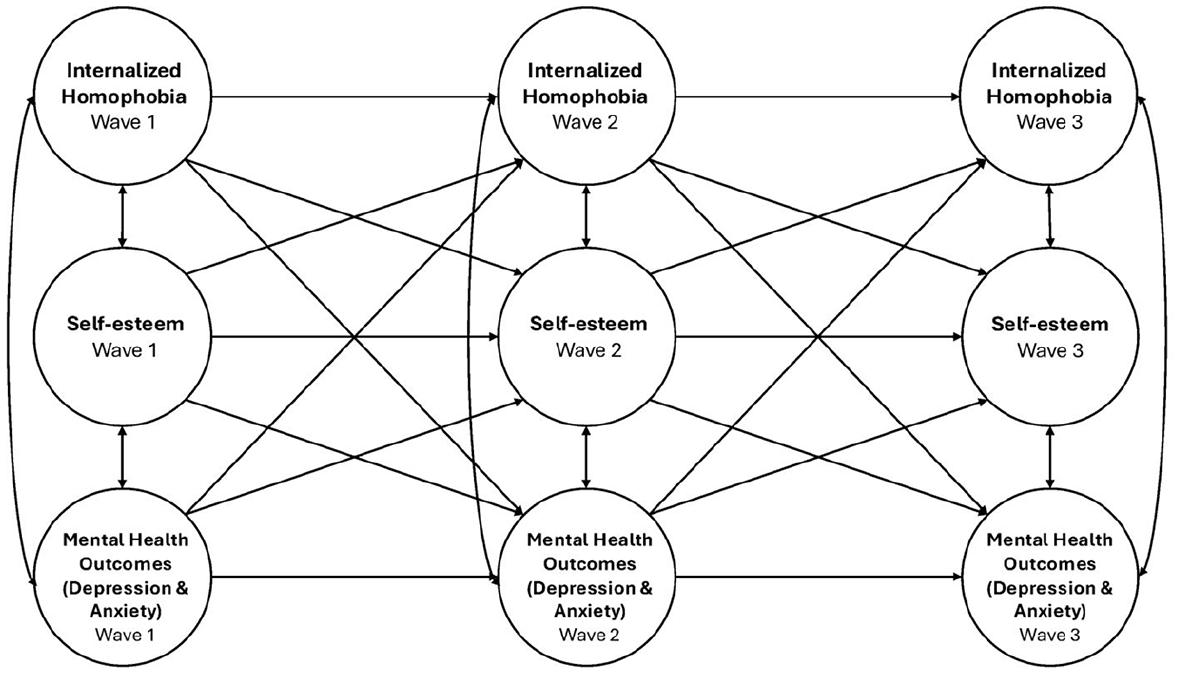
Conceptual diagram of the mediation model tested in the study.
Methods
Procedures
Data for this study comes from a randomized controlled trial (NCT03155841) designed to evaluate the effectiveness of an online intervention on cognitive and behavioral HIV-related outcomes among ASMM (Bauermeister et al., 2018). The research and ethics presented in this study were reviewed by our Institutional Review Board, and registered on ClinicalTrials.gov (NCT03155841). A waiver of parental consent was obtained to maximize ASMM’s ability to participate in the research even if they were not out to their parents or if they had limited parental support regarding their sexuality.
This study recruited a diverse sample, ensuring that at least 50% of participants came from racial and ethnic minority backgrounds. To be eligible, participants had to (a) self-report as cisgender male, (b) be 13 and 18 years of age (inclusive), (c) speak and read English, (d) report same-sex attractions and/or behaviors, (e) have access to the Internet, and (f) self-report as HIV-negative at time of enrollment. Participants also had to live in one of the four geographic corridors selected for this study due to their HIV prevalence rates, and encompassed a diverse mix of urban, suburban, and rural counties: (a) Chicago, IL to Detroit, MI; (b) Washington, DC to Atlanta, GA; (c) San Francisco, CA to San Diego, CA; and (d) Memphis, TN to New Orleans, LA.
Participants were recruited online through social media advertising. Individuals who expressed an interest in participation completed a short eligibility screener. Eligible participants were asked to verify their phone number and contact information and to complete the study consent form. Consistent with best practices, automatic and manual verification processes were implemented to reduce the likelihood of bots, fraudulent accounts, and/or duplicate entries in our trial (Guest et al., 2021). Consented and verified participants were enrolled and asked to complete baseline (T1), 6-month (T2), and 12-month (T3) surveys between March 2018 and February 2022. We spaced each survey 6 months apart to balance capturing longitudinal trends with minimizing respondent burden. This spacing also allowed us to adapt and implement any necessary adjustments or refinements to the survey instrument or recruitment strategy based on feedback or emerging trends from previous surveys.
The research team sent invitations via email and text, each including a unique survey link for the participant. Among the 599 cisgender ASMM who consented and enrolled in the trial, 599 completed the baseline survey conducted immediately after enrollment, 504 (84%) completed the 6-month survey, and 490 (82%) completed the 12-month survey. Participants received an Amazon gift card as an incentive for each survey completed: $30 for baseline, $25 for the 6-month survey, and $30 for the 12-month survey.
Measures
Predictor Variable: Internalized Homophobia
The Internalized Homophobia Scale is a nine-item scale assessing IH, which aims to gauge the extent to which gay men experience discomfort regarding their sexual orientation and attempt to evade same-sex attraction (Meyer, 1995). Due to low factor loadings (e.g., less than 0.40) observed among four items, five items were retained in a shorter version of this scale (Herek et al., 2009). These items were coded negatively, and participants’ responses were recorded on a four-point Likert scale, spanning from “1 = Strongly Disagree” to “4 = Strongly Agree.” Mean scores are recommended for calculating the total score, ranging from 1 to 4 (Meyer, 1995). Higher scores on the scale indicated a higher degree of IH. The Cronbach’s alpha for the five-item scale was .80.
Mediator: Self-esteem
The Rosenberg Self-Esteem Scale is a 10-item scale designed to measure self-esteem (Rosenberg, 1965). Due to the observed low factor loadings for specific items, we included five items from a shorter version of this scale, including two positively and three negatively coded items (Monteiro et al., 2022). Participants’ responses were collected using a four-point Likert scale, with options ranging from “1 = Strongly Disagree” to “4 = Strongly Agree.” We reversed the coding for three of the negatively coded items. Mean scores are recommended for calculating the total score, ranging from 1 to 4 (Monteiro et al., 2022). Higher scores on this scale indicated a more positive level of self-esteem. The Cronbach’s alpha for this five-item scale was .84.
Outcome Variable I: Anxiety
The Brief Symptom Inventory (BSI) includes a positively coded six-item anxiety subscale, which was part of an 18-item scale designed to assess psychological distress and psychiatric symptoms (Derogatis, 2000). Participants provided responses using a five-point Likert scale, ranging from “0 = Never” to “4 = Very often.” Mean scores are recommended for calculating the total score, ranging from 0 to 4 (Derogatis, 2000). Higher scores on this subscale indicated a greater degree of anxiety. The Cronbach’s alpha for our study sample was .90.
Outcome Variable II: Depression
The Center for Epidemiologic Studies Depression Scale- Revised-10 (CESD-R-10) is a 10-item scale designed to assess depression, including two positively and eight negatively coded items (Andresen et al., 1994). Participants’ responses were collected using a four-point Likert scale, with response options spanning from “0 = Rarely or none” to “3 = All of the time.” We reversed the coding for two of the positively coded items. Sum scores are recommended for calculating the total score, which ranges from 0 to 30. Elevated scores on this scale indicate a higher level of depression, with any score equal to or above 10 considered indicative of depression (Andresen et al., 1994). The Cronbach’s alpha for our study sample was .81.
Covariates
In our analysis, we incorporated several baseline sociodemographic characteristics (e.g., time-invariant factors) that have been previously identified as significant predictors of mental health outcomes among ASMM. These covariates included race and ethnicity, urban status, baseline age and intervention/control group assignment. Research has shown that racial and ethnic minority ASMM may face unique stressors related to identity intersectionality, which can influence their mental health (Bostwick et al., 2014; O’Donnell et al., 2011). Race and ethnicity were recorded separately. Responses for race included American Indian or Alaska Native, Asian or Asian American, Black or African American, Multiracial, Native Hawaiian or Other Pacific Islander, and White or Caucasian. Ethnicity responses included Hispanic and non-Hispanic. These variables were then categorized into non-Hispanic White and racial and ethnic minority groups (National Institute of Minority Health & Health Disparities, 2024). Studies have demonstrated that urban status can affect access to resources and support systems, which in turn impacts mental health outcomes (Fisher et al., 2014; Rosenkrantz et al., 2017). We categorized urban status based on participants’ zip codes and the National Center for Health Statistics Urban-Rural Classification Scheme (Ingram & Franco, 2014), which includes categories such as small/medium metro, rural, suburban, and urban. We further dichotomized these into urban and non-urban, with non-urban encompassing small/medium metro, rural, and suburban areas. Additionally, age is an important covariate as developmental factors may influence the experience and expression of mental health symptoms during adolescence (Shilo & Savaya, 2012). Since data collection was completed within 1 year, we included baseline age as a time-invariant covariate. As studies have reported that bisexual individuals are at greater risk of poor mental health compared to gay men (Chan et al., 2020), self-reported sexual orientation was included as a covariate. Response categories included categories such as gay/homosexual, bisexual, other, straight/heterosexual with same-sex attraction and/or behavior, same-gender loving, queer, and questioning or uncertain. Due to the exceedingly few instances of same-gender loving responses in our dataset, we combined these with the other category to ensure a sufficiently large sample size for robust statistical analysis. Intervention/control group assignment was included to account for potential differences in mental health outcomes due to intervention-related support or resources affecting IH, self-esteem, or mental health symptoms. We assessed multicollinearity by calculating generalized variance inflation factors for each independent variable, and the results showed low values for all variables.
Statistical Analysis
We utilized R version 4.4.1 to examine the longitudinal relationship between IH, self-esteem, and mental health outcomes among ASMM. We employed structural equation modeling (SEM) using the Lavaan package in R (Rosseel, 2012). SEM is a statistical method that allows for the concurrent examination of the connections between constructs within a proposed model, including latent constructs (Schreiber et al., 2006).
We initially conducted longitudinal confirmatory factor analysis (CFA) to assess the factorial validity of the latent constructs and evaluate the measurement model’s adequacy (Farrell, 1994). The longitudinal CFA was specified with metric (weak) invariance, meaning that we constrained factor loadings to be equal across time points. Establishing metric invariance indicates that the relationships between the latent constructs and their observed indicators remain stable over time, allowing for meaningful comparisons across waves (Putnick & Bornstein, 2016). To identify potential sources of misfit, we examined modification indices, offering a basis for adjusting the model as required (Schreiber et al., 2006). We introduced two residual correlations between two positively coded items within the depression and self-esteem scales. These correlations accounted for potential unique variance or measurement error and were distinct from all other negatively coded items in each scale. We then evaluated whether the proposed model demonstrated an adequate fit to the data using multiple fit indices, including the comparative fit index (CFI), non-normed fit index (NNFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) (Hu & Bentler, 1999; Schumacker & Lomax, 2004).
We constructed complete mediation structural equation models (Jose, 2016) separately for anxiety and depression as outcomes (Figure 1). These models allowed all three variables (e.g., IH, self-esteem, and anxiety or depression) to be represented at all three time points and enable testing of all six possible mediation pathways (e.g., six unique orderings of the three variables across the three time points, such as IH at T1 to self-esteem at T2 to depression at T3) (Jose, 2016). Following best practices for covariate inclusion, where covariates should be added as predictors for any dependent variable in paths where they may theoretically confound the hypothesized relationship (Newsom, 2023), we included baseline age, sexual orientation, urban status, race and ethnicity from T1 to T3, as well as intervention/control group assignment at T2 and T3, since randomization occurred after the baseline (T1) survey. Next, we conducted subgroup analyses to compare mediation models for racial and ethnic minority ASMM and non-Hispanic White ASMM. In sensitivity analyses, we examined whether factors loadings varied between the two groups and observed no differences in our model. Therefore, we constrained factor loadings to be equal across the two groups.
Our missingness rate was 379 cases out of 1,593 observations (23.8%). Given the moderate proportion of missing data, we chose not to use listwise deletion. Removing a large percentage of participants through listwise deletion could result in substantial information loss or biased estimates (Acock, 2005, 2012). Although the exact mechanism underlying the missing data was not fully understood, there were indications that the missingness was related to the observed data. Consequently, we assumed that the data were missing at random (MAR). This assumption implies that the probability of missing data on a variable is related to other observed variables in the dataset but not to the missing values themselves. To address missing data, we employed full information maximum likelihood (FIML), which leverages all available data points to estimate parameters without imputing missing values. FIML provides unbiased and efficient estimates under the MAR assumption by using the observed likelihood function for each case, ensuring that missingness does not distort model results (Enders & Bandalos, 2001).
Results
Table 1 presents the socio-demographic characteristics of the 599 baseline survey participants, as well as those who participated in either the 6-month or 12-month follow-up surveys, and those who did not participate in either. There were no significant differences between individuals who participated in either follow-up survey and those who did not participate in any follow-up. The 599 participants had an average age of 16.2 (SD = 1.3). The majority of the sample (n = 453) identified as racial and ethnic minorities, with 24.4% (n = 146) identifying as non-Hispanic White. At baseline, 56.4% (n = 338) reported living in urban areas, and more than half (60.3%) identified as gay.
Demographic Characteristics of Adolescent Sexual Minority Men Who Participated and Did Not Participate in the Follow-up Surveys.
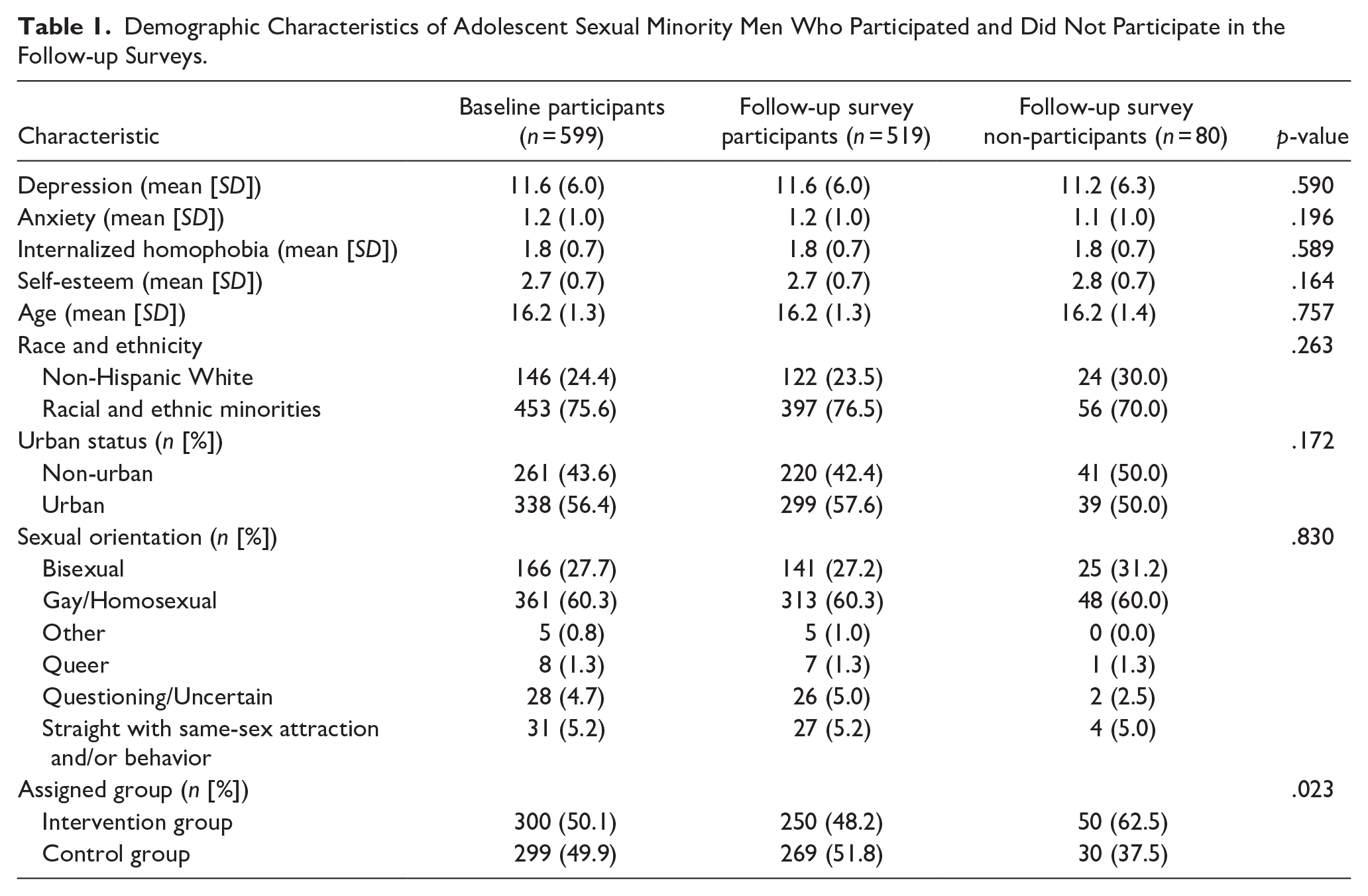
At baseline, mean depression scores between non-Hispanic White ASMM (11.0; SD = 6.2) and racial and ethnic minority ASMM (11.7; SD = 5.9) were not significantly different (p = .221). Similarly, mean anxiety scores for non-Hispanic White ASMM (1.2; SD = 1.0) and racial and ethnic minority ASMM (1.2; SD = 1.0) were not significantly different (p = .765). Mean IH scores for non-Hispanic White ASMM (1.8; SD = 0.6) and racial and ethnic minority ASMM (1.8; SD = 0.7) were not significantly different (p = .383). Similarly, mean self-esteem scores for non-Hispanic White ASMM (2.7; SD = 0.7) and racial and ethnic minority ASMM (2.7; SD = 0.7) were not significantly different (p = .247).
Measurement Model
The measurement model for anxiety demonstrated adequate fit (χ2 = 1,646.479, df = 1,016, p < .001, CFI = 0.958, NNFI = 0.953, RMSEA = 0.032 with 95% CI = 0.029–0.032, SRMR = 0.047) (Appendix A). Similarly, the measurement model for depression demonstrated adequate fit (χ2 = 2,575.893; df = 1,639, p < .001, CFI = 0.933, NNFI = 0.928, RMSEA = 0.031 with 95% CI = 0.028–0.034, SRMR = 0.057) (Appendix B).
Structural Model
Standardized coefficients for cross-lagged regression and stability paths, along with model fit statistics, are presented in Table 2 for the longitudinal structural equation model with anxiety as the outcome and in Table 3 for the model with depression as the outcome. Factor covariances for each model are presented in Appendices C and D, respectively.
The Structural Model for Anxiety as an Outcome in the Overall Sample, Racial and Ethnic Minority ASMM Group, and Non-Hispanic White ASMM Group.
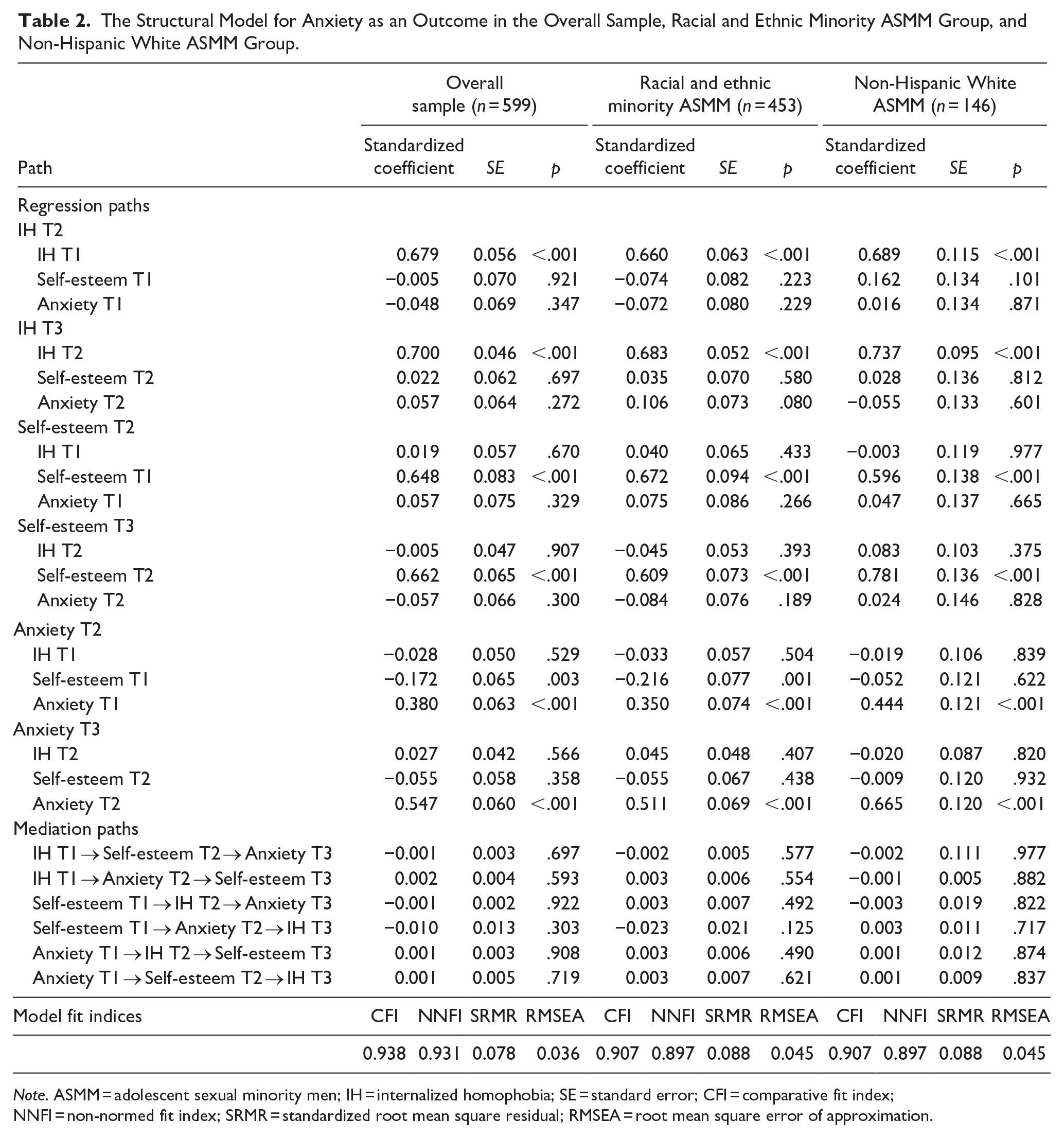
Note. ASMM = adolescent sexual minority men; IH = internalized homophobia; SE = standard error; CFI = comparative fit index; NNFI = non-normed fit index; SRMR = standardized root mean square residual; RMSEA = root mean square error of approximation.
The Structural Model for Depression as an Outcome in the Overall Sample, Racial and Ethnic Minority ASMM Group, and Non-Hispanic White ASMM Group.
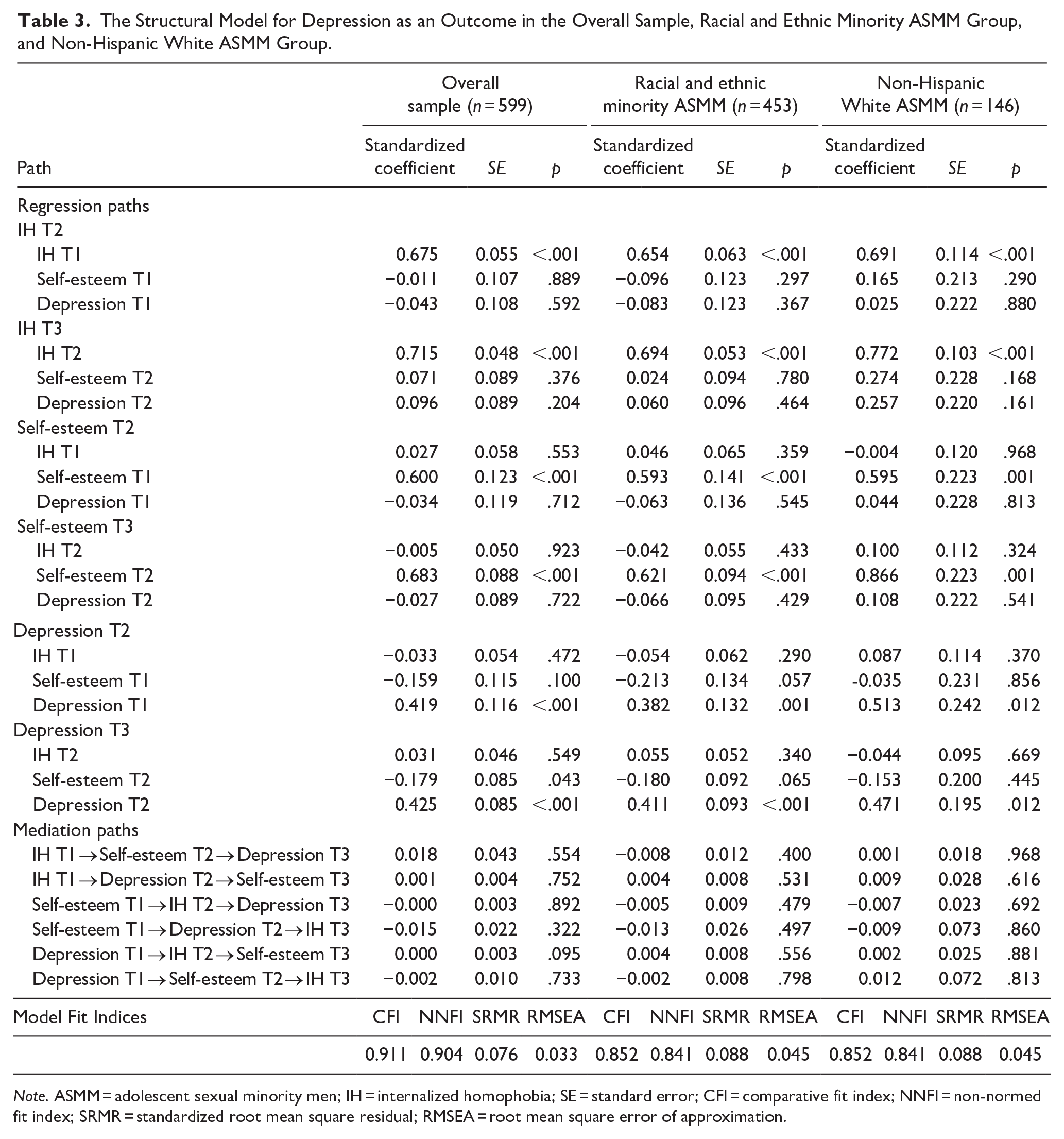
Note. ASMM = adolescent sexual minority men; IH = internalized homophobia; SE = standard error; CFI = comparative fit index; NNFI = non-normed fit index; SRMR = standardized root mean square residual; RMSEA = root mean square error of approximation.
For the overall sample, the structural model with anxiety as the outcome showed that higher self-esteem at T1 was significantly associated with lower anxiety symptoms at T2 (β = −.172, p = .003). The model demonstrated strong stability across time points for IH (β = .679; .700 [T1 to T2; T2 to T3], p < .001), self-esteem (β = .648; .662, p < .001), and anxiety (β = .380; .547, p < .001). None of the six mediation pathways were statistically significant.
For depression, higher self-esteem at T2 was significantly associated with lower depressive symptoms at T3 (β = −.179, p = .043). The model demonstrated strong stability for IH (β = .675; .715 [T1 to T2; T2 to T3], p < .001), self-esteem (β = .600; .683, p < .001), and depression (β = .419; .425, p < .001). None of the six mediation pathways were statistically significant.
Subgroup Analysis
Among racial and ethnic minority ASMM, higher self-esteem at T1 was significantly associated with lower anxiety symptoms at T2 (β = −.216, p = .001). The model with anxiety as the outcome showed strong stability across time points for IH (β = .660; .683 [T1 to T2; T2 to T3], p < .001), self-esteem (β = .672; .609, p < .001), and anxiety (β = .350; .511, p < .001). Similarly, the model with depression as the outcome demonstrated strong stability for IH (β = .654; .694, p < .001), self-esteem (β = .593; .621, p < .001), and depression (β = .382; .411, p < .001). None of the six mediation pathways were statistically significant in either model.
Among non-Hispanic White ASMM, no statistically significant cross-lagged regression paths were observed in either model. The model with anxiety as the outcome showed strong stability across time points for IH (β = .689; .737 [T1 to T2; T2 to T3], p < .001), self-esteem (β = .596; .781, p < .001), and anxiety (β = .444; .665, p < .001). Similarly, the model with depression as the outcome demonstrated strong stability for IH (β = .691; .772, p < .001), self-esteem (β = .595; .866, p = .001), and depression (β = .513; .471, p = .012). None of the six mediation pathways were statistically significant in either model.
Discussion
The psychological mediation framework suggests that self-esteem may serve as a cognitive mechanism linking minority stressors to mental health (Hatzenbuehler, 2009); however, empirical evidence regarding its mediating role among sexual minorities has been inconsistent (Austin et al., 2004; Rosario et al., 1996; Savin-Williams & Ream, 2003). These inconsistent findings may indicate that other factors such as coping strategies, social support, or emotion regulation may play a more significant role in shaping the relationship between minority stress and mental health outcomes (Meyer, 2010, 2015). Moreover, it is possible that the inconsistent findings may be linked to differences based on the age range, racial and ethnic composition, and developmental stage of participants included in these studies. Therefore, in this study, we sought to examine the longitudinal associations between IH, self-esteem, and mental health outcomes among a racially and ethnically diverse sample of ASMM. While we hypothesized that self-esteem would mediate the relationship between IH and mental health outcomes, we found no support for our mediation hypotheses. Moreover, we found limited evidence to support our hypothesis that there would be racial and ethnic differences in these relationships. Despite these results, our findings contribute important insights to the existing literature on minority stress, self-esteem and mental health among ASMM.
Adolescence is a critical period for identity formation and heightened vulnerability to stressors, but it is also a time when resilience and coping strategies are actively developing (Pfeifer & Berkman, 2018). It is possible that the effects of internalized homophobia on self-esteem and mental health are not yet fully established during this developmental stage, and a longer follow up period may be necessary to capture these relationships accurately. Therefore, one possible explanation for the non-significant mediation effect is the relatively short interval between waves in our longitudinal study. A six-month period may not be sufficient to capture meaningful changes in self-esteem and mental health, particularly given that identity-related processes such as the internalization of stigma and its psychological consequences often unfold gradually over time (Igartua et al., 2009). Another key consideration is the developmental stage of our sample. Longitudinal studies with extended follow-up from adolescence into young adulthood could help clarify whether self-esteem plays a mediating role at later stages of identity development. Future research in this area is warranted.
Despite the absence of hypothesized mediation pathways, our findings reinforce the important role of self-esteem in shaping mental health outcomes among ASMM, particularly in relation to anxiety. The longitudinal association between higher self-esteem and lower anxiety symptoms suggests that self-esteem serves as a psychological resource that helps mitigate distress over time. This aligns with prior research highlighting self-esteem as a critical protective factor against mental health challenges in sexual minority youth (Bauermeister et al., 2010; Hall, 2018). Given that sexual minority adolescents often face unique stressors related to external stigma and discrimination associated with mental health outcomes (Bauermeister et al., 2022; Hatzenbuehler & Pachankis, 2016; Russell & Fish, 2016), fostering self-esteem may be a key target for interventions aimed at improving mental health outcomes in this population.
Our subgroup analyses further revealed racial and ethnic differences in the relationship between self-esteem and anxiety. Specifically, the protective effect of self-esteem against anxiety symptoms was significant for racial and ethnic minority ASMM but not for their non-Hispanic White counterparts. These findings align with an intersectionality framework (Crenshaw, 1989; Mink et al., 2014). Racial and ethnic minority ASMM may navigate unique intersectional stressors, such as racial discrimination, socioeconomic adversity, and sexual orientation-related minority stress, which could intensify the psychological impact of stigma while simultaneously fostering resilience. In this context, self-esteem may function as a particularly salient protective factor, as it can counteract the compounded effects of these stressors by reinforcing a sense of self-worth and agency (Meyer, 2010, 2015). However, these subgroup findings should be interpreted with caution, as differences in statistical significance could be partially attributed to disparities in sample sizes across racial and ethnic groups. Small subgroup sizes may limit statistical power and affect the detectability of associations. Moreover, our analyses were unable to include latent factors for these additional forms of stress; therefore, we are unable to fully understand self-esteem’s role in the presence of these concurrent stressors. Future studies with larger and more diverse samples are needed to further examine racial and ethnic variations, considering both structural and cultural factors that may shape the relationship between self-esteem and mental health outcomes in ASMM.
Given the limited adolescent-specific research on racial and ethnic differences in IH and self-esteem, the strength of this study lies in its theory-based investigation of IH, self-esteem, and their impact on mental health outcomes among racially diverse ASMM. The use of a diverse sample from various U.S. regions, including a substantial proportion of racial and ethnic minority ASMM, enhances the generalizability of the findings. However, this study has several limitations. The sample predominantly consisted of English-speaking ASMM with internet access, which may limit the generalizability of the findings to ASMM facing greater socioeconomic challenges. Second, ASMM who participated in the study were willing to self-report their same-sex attractions in order to participate in the study. This may result in selection bias and affect the observed relationships under study, as we recognize that ASMM who are unable to acknowledge their sexual orientation identity may experience greater IH, have greater conflicts regarding their self-concept, and/or experience greater psychological distress. Additionally, while the research examined racial and ethnic differences broadly, it did not explore the distinct experiences of specific racial or ethnic subgroups within these categories. Lastly, there may be unmeasured confounders, such as family support, peer acceptance, or resilience, that were not explicitly modeled.
Notwithstanding these limitations, this study contributes to ongoing theoretical discussions about the mechanisms through which IH impacts mental health among ASMM. Additionally, by leveraging a robust longitudinal design, this study highlights the temporal associations between self-esteem and mental health outcomes, particularly in relation to anxiety, reinforcing the importance of self-esteem as a protective factor. To deepen our understanding of these dynamics, future research could benefit from conducting longitudinal studies with extended follow-up periods, accounting for multilevel confounders such as social support and LGBTQ-related policies in their social environments. Such multifaceted research approaches are essential for developing tailored and effective interventions that address the unique needs and experiences of ASMM across diverse racial and ethnic backgrounds.
Supplemental Material
sj-docx-1-yas-10.1177_0044118X251338311 – Supplemental material for Mediation Analysis of Internalized Homophobia, Self-esteem and Mental Health in Adolescent Sexual Minority Men: A Repeated Measures Study
Supplemental material, sj-docx-1-yas-10.1177_0044118X251338311 for Mediation Analysis of Internalized Homophobia, Self-esteem and Mental Health in Adolescent Sexual Minority Men: A Repeated Measures Study by Hyunmin Yu, Jennifer T. Tran, Stephen Bonett, James R. Wolfe, Keith J. Horvath, Amanda D. Castel, Lisa B. Hightow-Weidman, Patrick Sullivan and José A. Bauermeister in Youth & Society
Footnotes
Authors’ contributions
HY, JT, JW, and JB made contributions to the conception and design of this article. HY, JT, SB, JW, and JB contributed to the acquisition, analysis and interpretation of data. HY drafted the manuscript. JT, SB, JW, KH, AC, LH, PS, and JB revised the manuscript. All authors approved the final manuscript.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a U01 grant from the National Institute of Minority Health and Health Disparities (1U01MD011274-01), and the Centers for AIDS Research at the University of Pennsylvania (P30AI045008) and at Emory University (P30AI050409). Views expressed in this manuscript do not necessarily represent the views of the funding agency.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the University of Pennsylvania Institutional Review Board (#825686).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.