
Abstract
Adolescents who need both child welfare services and mental health interventions have usually experienced various traumatic events in their early lifespan. The purpose of this study is to identify the elements of communication that can either empower traumatized adolescents in their rehabilitation process or become an obstacle in their recovery. The data consist of interviews of 19 young adults with a substitute care background. Their experiences of communication with welfare professionals in child welfare and mental health services during adolescence are analysed using the method of content analysis in a framework of communication competence that is outlined with four elements: cognitive, affective, behavioural and ethical. The role of communication is crucial while helping the adolescents. The trauma-informed capabilities of welfare professionals should be strengthened. Future research is needed on the processes, enabling the voice of this vulnerable clientele to be heard, here and in previous stages of services.
Keywords
Introduction
Young people who need both child welfare services and adolescent psychiatry interventions have usually experienced different forms of neglect and abuse in their past. Especially, adolescents who live in substitute care often experience traumatic events in their early lifespan (Salazar et al., 2013). Many clients of child welfare services and adolescent psychiatry have a history of manifold victimization and adverse childhood experiences (ACEs), such as physical, sexual or emotional abuse, mental illness of a household member, or substance abuse issues within the childhood family that usually accompany them in various ways into adulthood (Anda et al., 2006; Vederhus et al., 2022). Childhood cumulative trauma can cause long-term consequences and act as a predictor of increasing psychosocial symptom complexity in later years (Cloitre et al., 2009). Due to these factors, working with highly vulnerable adolescents requires particular sensitivity, and a special emphasis should be put on the ways of communication with them and the interpersonal skills of welfare professionals.
In this article, we examine the experiences of young Finnish people with a history of substitute care and mental health services, in regard to their communication with welfare professionals. By substitute care, we refer to arrangements for the care of young people outside their home, either in kinship care—a foster family—or an institution. We do not use the commonly used concept of out-of-home care, since some of the participants who were placed in kinship care had defined the provider of their care as a family member and the venue of the placement, before the official placement, as their second home. Our focus is on the experiences of young people about their communication with welfare professionals in child welfare and mental health services during their adolescent years. The aim of the article is to identify the elements of communication that can either empower adolescents in the process of their rehabilitation or become an obstacle in their recovery. By analysing the experiences of adolescents, we strive to promote an awareness of the professionals of both attitudes and actual activities of the client interaction who are present in young client–professional encountering.
Similar to what Mental Health Foundation (2008) suggests, we perceive mental health as how individuals think and feel about themselves and their life, and how it affects how an individual copes and manages times of adversity. We acknowledge that even normative psychological development in adolescents, including the extensive development of the brain co-occurring with internal and external stress, may affect their mental health. While the trajectories of childhood trauma vary, many of the traumatized adolescents continue to experience various mental health problems as they age out of care (Baidawi et al., 2014). We comprehend communication as an essential building block in the rehabilitative encountering of adolescents. By rehabilitative encountering, in line with the work of Saakvitne et al. (2000), we refer to communication and relations between adolescents and welfare professionals that offer adolescents both information and the feelings of connection, respect and hope—factors that support mental health. We analyse the experiences of adolescents in the framework of communication competence, which according to Cooley and Roach (1984) refers to the knowledge of effective and appropriate communication patterns, and the ability to use and adapt that knowledge in various contexts.
While studying the experiences of adolescents, we acknowledge the phenomena of trauma and traumatization, wherein it is essential that the professionals recognize the prevalence of early adversity in the lives of their clients, are aware that the problems of the clients can also be symptoms of possible maladaptive coping and have an understanding of how early trauma can shape a client’s fundamental beliefs about the world. These standpoints indicate that the trauma might affect clients’ psychosocial functioning across the whole life span (Knight, 2015; Levenson, 2017). Our study is especially relevant from the point of view of very vulnerable young clients of social and welfare services, who often have challenges in taking part in scientific research due to their poor mental condition. From a professional practice development point of view, it is essential to comprehend the different levels and forms of communication that guide client work with the young.
Communication Competence While Working with Traumatized Adolescents in Substitute Care
Adolescents with a history of ACEs and placements in substitute care are known to be at increased risk of mental health problems (Kerns et al., 2014). They often have emotional issues arising out of pre-care experiences and different forms of maltreatment and abuse (Kerker et al., 2015). It is also known that living in substitute care can itself strain the mental well-being of adolescents, for example, due to their separation from biological family (Greeson et al., 2011), placement instability (Rice et al., 2017) and the various effects on social networks (Negriff et al., 2015).
In general, adolescence is a phase of life when individuals are especially sensitive to picking up hints of whether they are fully accepted or not and whether it is appropriate to speak about sensitive topics and even taboos. Adolescents tend to build their identities on the basis of the way they believe others see them (Rycek et al., 1998). Acknowledging these facts and bringing up difficult themes in client interactions with traumatized adolescents require special delicacy in terms of communication. As Brown et al. (2019) state, good care is a complex, relational process involving dedication, perseverance, compassion and trust. Both the verbal and non-verbal aspects of the interaction in addition to the general attitude towards the client can be either strengthening or discouraging from the perspective of adolescents.
Communication competence can be understood as an abstract, multidimensional set of knowledge and skills that are essential to all face-to-face welfare work. It contains knowledge about (a) appropriate and effective communication behaviours, (b) a wide repertoire of skills that encompass both appropriate and effective means of communication and (c) motivation to behave in ways that are viewed as appropriate and effective by the interactants (Rubin, 1990). Many aspects of communication competence are factors about which professionals are not even aware of, and instead, their use is often subconscious without paying any intentional attention to them. Different dimensions of communication competence are also intertwined in many ways, and sometimes, it is even impossible to define and verbalize, for example, when the motivation ends and the personal traits and endogenous knowledge of the welfare professional actually take over in communication with the client. However, it is generally stated that welfare professionals such as social workers use their personality and interpersonal skills as a central tool in the client work (Koprowska, 2020).
Working with adolescents who have faced different forms of ACEs requires a special awareness of the phenomenon and the process of trauma and traumatization. Since many clients of substitute care have also experienced physical maltreatment in their past, acknowledging the multidimensional biopsychosocial perspective along with the mind–body coping process can promote the overall health of adolescents (Larkin et al., 2014) and strengthen their resilience. Theoretically, coping and resilience are closely linked, and both concepts are essential in the formation of rehabilitation. Coping refers to the ability to manage and attempt to overcome difficulties by adapting to stressful experiences and conditions in both conscious and unconscious manners (Stanislawski, 2019). Resilience can be defined as an ability to find peace of mind, to become happy and self-sufficient, to feel satisfied and to grow after tough periods in life (Southwick et al., 2014). However, resilience is also a socially constructive phenomenon, and the support one gets, for example from family, social networks and social and welfare services, is crucial in forming and reinforcing resilience (Meng et al., 2018). In the framework of this article, we comprehend coping as a desired outcome for a rehabilitative process, in which resilience is one of the key contributors and facilitators. However, our focus is not on the process of coping or the concept of resilience itself but rather on the experiences of communication that can either promote or hinder coping and resilience, and subsequently the wider rehabilitation process of adolescents.
The aim of rehabilitative work in substitute care is to guide adolescents to a safe adulthood. Salazar et al. (2013) point out that the ongoing impact of trauma may be particularly problematic for adolescents with a substitute care background, given their often abrupt transition to independence. The transition to life outside the care system can be particularly challenging and stressful due to the responsibilities of adulthood concerning issues such as education, work, housing and budgeting (Courtney et al., 2011; Häggman-Laitila et al., 2019) and their limited sources of emotional and social support (Cashmore & Paxman, 2006). Adolescents may also lack knowledge of how to access mental health services and feel disregarded when they actually seek help (York & Jones, 2017). The lack of reliable and sustainable encountering with welfare professionals can increase the stress of adolescents in the phase of transition, which may consequently reawaken experiences of childhood neglect and therefore reinforce mental health problems. On the other hand, adolescents tend to use care workers as a secure attachment figure (Harder et al., 2013).
It is essential to guide young adults with a substitute care history to actively monitor their mental health and build a strong connection with the mental health services as they leave care and start to steer their lives independently (Narendorf et al., 2021). In this process, the foundation for therapeutic relationships, which Saakvitne et al. (2000) define as relations that offer information, connection, respect and hope, is already laid during the substitute care. Empowering the client experience in good welfare services is always linked to whether an individual feels genuinely heard and whether the aspects one has brought to the discussion are taken seriously. From a client perspective, it is crucial that the unique stories and interpretations of the situation and the contributing factors involved are taken into consideration and truly recognized in the organizing services. It is often difficult for clients who have complex vulnerabilities and mental health challenges to find their voice and to be heard in the service structure (World Health Organization, 2010). In this process, effective and empowering ways of communicating play a central role by forming the foundation for both rehabilitative encountering at the individual level and active societal agency at the structural level. As Davies and Wright (2008) have pointed out, the views of adolescents in substitute care regarding their mental health services should be a standard practice both from the individual treatment and services development points of view. Our article outlines the experiences of adolescents of their communication with welfare professionals and aims to generate new perspectives to developing professional practices while working with the young.
Data and Methods
The empirical data of the study consist of the interviews of 19 young people, aged 18–27 years, who have been in substitute care and have also used or would have needed in their own opinion the services of adolescent psychiatry. One of the participants were placed in foster care and a child welfare institution, 16 solely in a child welfare institution, and 2 both in kinship care and a child welfare institution during their substitute care period. Eighteen participants identified themselves as female and one as man. Participants for the research were recruited via child welfare offices from the public sector or by experts by experience in voluntary sector organizations. Since the majority of the participants of the study are no longer clients of child welfare and are no longer in the phase of actual adolescence, we term the participants as the young and young adults and not adolescents. The interviews were carried out by three researchers between June 2021 and March 2022 using a narrative thematic interview methodology (Riessman, 2008). During the interviews, a lifeline graph was drawn in order to clarify the narration of the participants relating to their meaningful encounters with welfare professionals and the timeline of used services (Bagnoli, 2009). In this study, the focus is placed on the meaningful encounters experienced by the young and not on the timeline of the services. The interviews were held in the homes of the young people, at the University, at the research partners’ facilities or via remote access in telephone or online interviews.
Procedure
We interviewed young Finnish people who have reflected on their former encounters with welfare professionals during periods of substitute care. Instead of the original research plan for conducting in-person interviews, only 12 interviews were made face-to-face due to the COVID-19 pandemic. Seven interviews were carried out via a telephone or online connection. All of the interviews were recorded with a separate digital recorder. No online recording applications were used due to data protection issues. The participants had the right to refuse to answer any of the questions or to end the interview at any point. In order to encourage the participants to share their experiences, the interviewer looked to establish a climate for open narration. In this study, the conditions for conducting an open interview were excellent since all of the three interviewers were qualified social workers who had a long experience of professional social work with vulnerable clients in various contexts. The feelings and thoughts of each participant were reflectively discussed with the interviewer following the interview. All of the organizations distributing the invitation to participate agreed to organize psychosocial support for the participants after the interviews if needed. The researchers actively reflected on their thoughts for each interview, and the ethical questions involved shortly after interviews were concluded in their research meetings.
Data Analysis
Data were analysed by way of qualitative content analysis that aims at drawing replicable and valid inferences from the data to their context, with the purpose of providing new insights into the phenomenon under study. Both inductive and deductive reasonings were used in the process of analysis. This hybrid approach assists a researcher in identifying the most basic elements of the raw data and flexibly discovering both descriptive and interpretive meanings that appear to be interesting and relevant to the research question (Xu & Zammit, 2020). The analysis was performed by the first author. The second and third authors checked the accuracy of the analysis multiple times since they were strongly familiar with the data after performing the interviews and having read the transcripts several times. The analysis was also presented and discussed in the wider research group.
At first, all of the descriptions of the experiences of the participants of their communication with welfare professionals were separated from the overall data, in order to gain a broad description of the phenomenon (Elo & Kyngäs, 2008). At this point, the analysis was inductive. In the second phase of the analysis, the mentions of communication experiences were divided into four themes that were mostly formed on the basis of the previous literature of communication competence. In speech communication science, the concept and manifestations of communication competence have been approached from a variety of perspectives, and they have been outlined with cognitive, affective and behavioural elements (Duran, 1989; Rubin, 1990; Spitzberg, 1991; Spitzberg & Cupach, 1984).
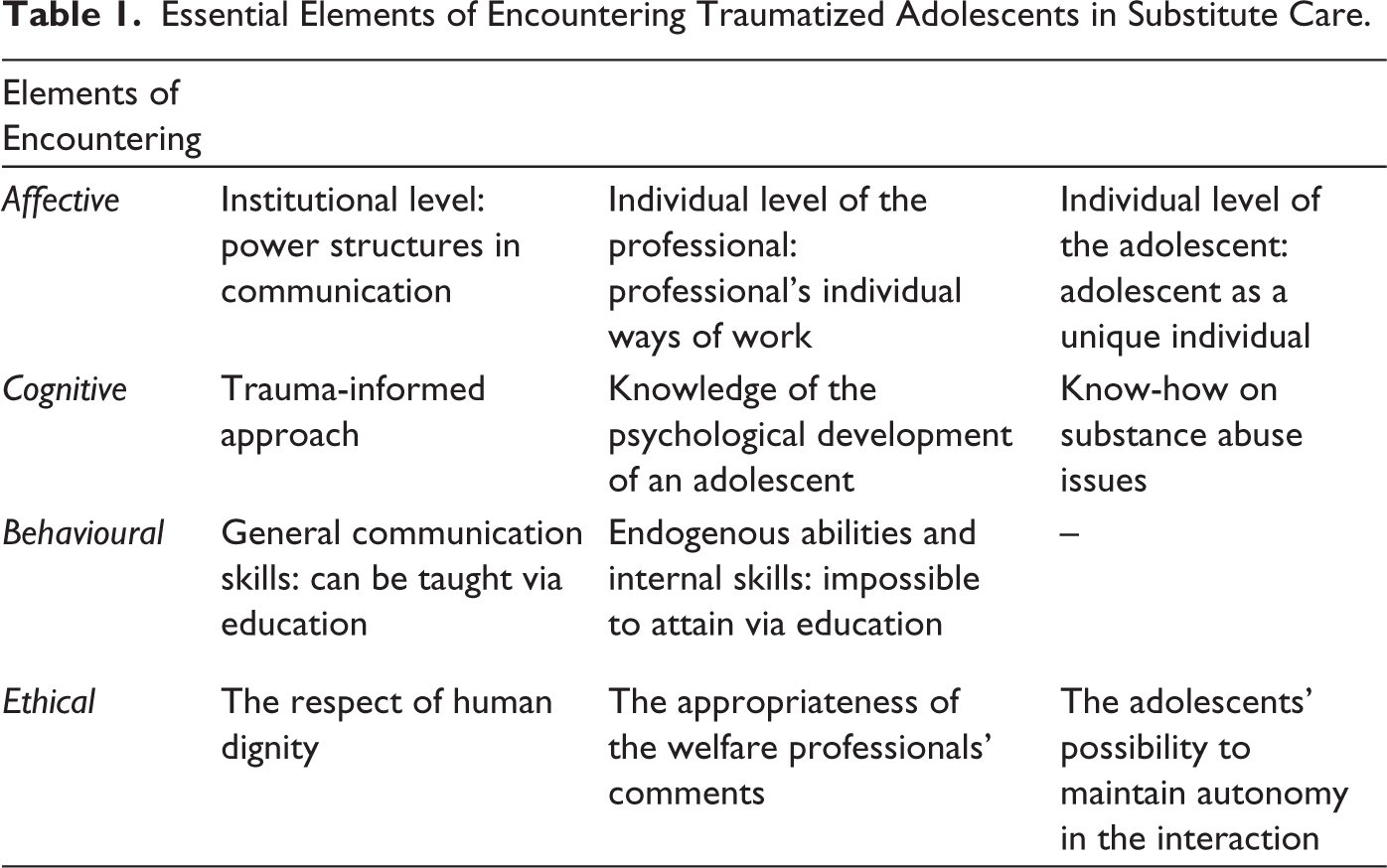
In our analysis, we outline communication competence with four elements that can be principally differentiated, even though they are intertwined in many ways. We structure the three previously described theory-based dimensions of communication competence: cognitive, affective and behavioural with the empirical-based ethical element that we found to be essential while working with vulnerable clientele. First, we interpret the knowledge of appropriate and effective communication behaviours as a cognitive dimension of communication. Second, we see the development of a repertoire of skills that encompasses both appropriate and effective means of communication as a behavioural dimension of communication. Third, we comprehend the motivation to behave in ways that are viewed as both appropriate and effective by interactants as affective and ethical dimensions that form the third and the fourth dimensions of our examination. The affective dimension covers the general communication orientation, whereas the ethical dimension includes the ways that communication orientation is realized in the actual client work. Due to this disposition, the second phase of the analysis was deductive and followed the principles of theory-guided analysis (see, e.g., Ezzy, 2002). At this point, the differences between and similarities within the different dimensions of the themes were emphasized (Graneheim & Lundman, 2004). In the third and last phase of the analysis, the theory-guided findings were reinterpreted and reorganized in more detail within the main categories of communication competence. In this process, the analysis once again became inductive and more subtle. Subcategories were then formed, and the results reached the form that they are presented in this article.
Ethical Considerations
Where research concerns vulnerable clientele, the ethical considerations involved need to be thorough. The study was accepted by the Ethics Committee for Human Sciences at the University of Turku. All of the participants received documents, providing information on the goal of the study, the participants’ rights, and the safety and confidentiality of the data collection, archiving and analysis beforehand. All of the information was also explained by the interviewer before the interviews commenced. In addition, participants were encouraged to ask any questions they had concerning the research. All of the participants provided an informed consent, either in a written form or in a recorded oral form on telephone or in online interviews.
Results
The experiences of the young of communication with welfare professionals can be considered as having four intertwined dimensions: (a) affective, (b) cognitive, (c) behavioural and (d) ethical. We present the results under these four categories, although we perceive that the line drawn between categories is partly artificial due to their abstract and ambiguous nature.
Affective Dimension
The affective dimension covers the general communication orientation, for example, whether the communication is perceived as a relevant and significant way in rehabilitative work, and how it is experienced (Rubin, 1990). In the context of substitute care, the awareness of the power structures between the professionals and adolescents who might live in an institution against their own will is an essential factor from the view of affective communication. The importance of these power structures was highlighted in our data, and the experiences of the participants can be divided at two levels: the institutional and the individual.
The institutional level covers the general way in which questions concerning power structures are solved. In particular, whether they can be discussed and negotiated with adolescents in a way that addresses the importance of certain principles and rules as a tool for creating a safe and stabilizing everyday life environment for adolescents or whether they are presented as non-negotiable hidden facts.
The participants underlined that from the communication point of view, professionals need a constant awareness and reflection of the inherent power imbalance that exists in the helper–client relationship. Traumatized adolescents, especially those in child welfare institutions, easily feel that they are mostly in custody, not in rehabilitation. From the perspective of an adolescent, it is essential that the professionals do their best to flatten the hierarchy and, in principle, strive for as equal communication with adolescents as possible. The proper tools for this are seen as the use of common sense and having a good eye for the game, that is, noticing and understanding the moods and situations that are meaningful from a rehabilitative perspective for the adolescent. It is also relevant to see when it is time to stretch the rules for enabling the best possible outcome, instead of sticking to them persistently.
All the counsellors and foster home caregivers were well above the adolescent, there wasn’t equality. There were very strict rules and no common sense at all or any game eye, that one could stretch the bedtime rules at least at Midsummer. (Interviewee 3)
The individual level contains the way adolescents are seen as clients; whether they are comprehended as a service user segment, or whether the importance of acknowledging the individual backgrounds, needs and wishes of adolescents are taken into account in the formulation of the rehabilitative communication. It also refers to the way that each professional builds a unique communication with an adolescent in an individual manner.
According to the participants, the recognition of adolescents’ individuality, and taking a genuine interest in their unique personalities, individual responsiveness patterns and their backgrounds are the most important aspects that contribute to rehabilitative interactions. It is important for professionals to understand that the responsive habits of adolescents are tied to what kind of life history they have. Adolescents who have suffered from ignoring, unpredictable behaviour and maltreatment from their biological caregivers need experiences of stable and predictable behaviour that create security and provide an example of ‘normal’ interpersonal interaction.
An appreciative and gentle speech and a smile. That they smile at you and are interested in what you are doing, and not getting upset about completely pointless things. Stable and predictable behavior from those adults. (Interviewee 9)
The participants also addressed the importance of youth-centred activities in the process of building effective communication with adolescents, and the professional’s individual way of work either promotes or prevents this from happening. It is fulfilling for adolescents to comprehend that the professionals are eager to do more with them than the required minimum tasks. The experienced significance of concrete activities also demonstrates the importance of the connection between both verbal and nonverbal communication while working with adolescents.
One counsellor, who I liked, she sometimes did my hair in the mornings. The adult had an interest in chatting with you and spending time with you also on her own initiative. (Interviewee 9)
Factors related to physical appearance are often important for an adolescent, and the fact that a professional takes this into account and wants to help an adolescent look good can strengthen the self-esteem and self-image of the individual who might feel worthless due to their traumatizing life history. Furthermore, paying positive attention to the appearance of adolescents can be psychologically rehabilitating in itself and creates an experience for adolescents that they are important and there are aspects of them that are worth highlighting and important to take care of.
Cognitive Dimension
The cognitive dimension concerns knowledge and information on interaction and understanding the phenomenon and processes of communication (see, e.g., Rubin, 1990). Working with adolescents who have been traumatized in their past and suffer from manifold mental health challenges requires a special awareness of the trauma-informed approach, knowledge of the normative psychological development that takes place during adolescence and young adulthood, and specific know-how in regard to substance abuse issues.
The participants brought out that their traumas had not been adequately addressed by welfare professionals. Young people described how they had not been able to deal with their traumas and hoped that the professionals would have taken the topic up more actively while working with the young.
When we were placed there, then of course, since we had a whole world of traumas, which we have never dealt with. (Interviewee 6)
The participants also pointed out that in order to communicate effectively with adolescents, the professionals need special education regarding the psychological development of an adolescent. It is essential that the professionals comprehend that certain ways of reacting in their communication are not automatically symptoms of mental illness but, in fact, very common operation models seen in adolescence. An experienced trauma that has not been processed properly (e.g., in therapy) can bring unconscious factors to the conscious mind of an adolescent and reinforce the negative reactions of the young.
It would have helped the counsellors and adolescents alike, to have the idea that we are all minors, and we come from tricky circumstances. It’s normal to have symptoms. We are not bad, or that we should be punished for it. We just need to be guided. (Interviewee 16)
In addition to having knowledge on developmental psychology, the participants addressed the importance of substance-specific know-how of the professionals in their interactions with adolescents. Mental health and substance abuse issues often go hand in hand and reinforce one another in many ways. Many of the participants reflected on how they had used substances as a way of self-medication in order to manage anxiety or depression.
Institutions need personnel with mental health skills and knowledge of substance abuse issues. And the emotional skills, how to deal with anger. That anxiety and self-mutilation come from that they (adolescents) don’t know how to defuse those feelings any other way. (Interviewee 3)
As the citation indicates, adolescents are very sensitive to the way professionals express their emotional abilities with the young, and adolescents actively mirror their own behaviour in order to see how it is reflected in the welfare professionals.
Behavioural Dimension
The behavioural dimension addresses the perceptible speech and communication behaviours that other people can observe from the outside (see, e.g., Spitzberg & Cupach, 1984). This dimension is strongly linked to general communication skills that can be taught and adopted via education. However, skills are partly based on biological traits, such as temperament, which are also important in the formulation of the behavioural dimension.
The experiences of the participants strongly emphasized the importance of the internal communication skills of the welfare professionals. Factors such as empathy, giving an adolescent space in a shared conversation and the importance of enabling adolescents to be truly heard were seen as the backbones for genuine encounters. The participants felt that the chemistry between adolescents and the professional is the primary factor that enables the genuine—and therefore rehabilitative—encounter, and that an honest discussion about traumatic experiences is possible only if the chemistry exists.
According to the experiences of the participants, the essential, externally learnable skills were particularly attached to the therapeutic capacities that the trained psychotherapists have. Out-of-facility therapists were praised for enabling the rehabilitative encounter, while the therapeutic capabilities of staff at child welfare institutions were widely criticized and hoped to be strengthened through additional training.
He (personal psychotherapist outside child welfare institution) doesn’t judge, he tells me where my problems are. He doesn’t flatter or embellish, he just tells me what I’m capable of hearing. He has been able to keep track of my symptoms in true detail, and I feel that he knows what’s wrong with me before I know. (Interviewee 6)
Adolescents have a need to actively learn from their interactions and communication with welfare professionals. It is also reasonable to state that the role of the welfare professionals is not only limited to the way they communicate with adolescents and offering social and welfare services, but it can also be extended to a wider guidance and counselling.
Ethical Dimension
The ethical dimension covers humanity, human dignity and respecting the human will to maintain autonomy in interaction. It also contains an understanding about the importance of respecting human relationships that are not intentionally endangered in communication (see, e.g., Spitzberg & Cupach, 1984). An ethical code for interaction is crucial, but at the same time invisible; it usually becomes obvious only in situations where it is absent. Ultimately, a lack of ethics has an enormous effect on the experienced quality of the welfare services, and it is justified to state that ethics form the foundation for the whole concept of rehabilitative encountering.
The descriptions of the experiences participants had of the ethical dimension of their interactions can be presented in three dimensions: (a) the respect of human dignity, (b) the appropriateness of the welfare professionals’ comments and (c) the adolescents’ possibility to maintain autonomy in the interaction.
The Respect of Human Dignity
Social and welfare services should always be based on a respect for human dignity. Experiences of maltreatment and neglect leave deep marks on the individual, and adolescents in substitute care can often experience feelings of worthlessness and even question the purpose of their own existence on the basis of their past, negative life experiences. Handling of these issues requires that substitute care professionals take into account the trauma background of adolescents. Services are not allowed to include elements that reinforce the traumatization of adolescents and cause them to question their worth as human beings. Yet one of the most disturbing experiences in the data was a narrative in which a professional directly instructed an adolescent to cut herself in a certain way.
At that time I started to self-mutilate and they only said that I should cut vertically, not horizontally, you’ll die faster. (Interviewee 2)
Some participants were traumatized by the way they were confronted in child welfare institutions as adolescents, and these engrams have led young adults to spend long periods in psychotherapy.
The Appropriateness of the Welfare Professionals’ Comments
In their communication, the professionals have an opportunity to outline the whole purpose of the intervention to the adolescent. However, the participants found it inappropriate if the support offered was presented in the form of a punishment, which at the same time incriminated adolescents for the mistakes of their past. Accordingly, it is recognized that in rehabilitative work, a future-oriented method often works better than clinging to the past.
… It could have been better underlined that this is for you, and that we want to help you and encourage you to accept the offered help. Not to make you feel guilty for what you’ve done. (Interviewee 3)
The participants also hoped to be informed properly in consideration of their mental condition and also honestly about decisions regarding their lives and the reasoning behind them. Accurate information on the planned rehabilitation process is a key factor in forming the experience of participation in young people’s own affairs. But acting behind an adolescents’ back and, for example, surprising moves from one foster care unit to another were perceived as being particularly traumatic. Some of the participants even pondered how they might have had the possibility to change their behaviour to avoid serious interventions if had they only had the proper information on the planned process beforehand.
The urgent placement was 30 days and it was in a local institution. It was such a short time that you didn’t really think that it would take you to that point, you could still have done something to avoid the final placement. (Interviewee 3)
The above citation indicates that the way adolescents perceive periods of time can differ from the manner by which professionals discern timelines. Adolescents tend to live in the moment and are not always capable of understanding and carrying out the desired timetables for change that are set by the welfare professionals. Therefore, adolescents need clear communication and information on any instructions and guidelines given that concern the evaluation of their situation.
The Adolescents’ Possibility to Maintain Autonomy in the Interaction
The possibility to maintain autonomy in the interaction is fundamental from the ethical point of view of rehabilitative work. In that process, the avoidance of generalizations and stereotyping is essential. The participants found it particularly humiliating to be defined as a faceless mass of institutionalized young who is solely seen as the target of the interventions. The need to be seen and accepted as one’s unique self is both human and fundamental. Being able to express their own views is also a prerequisite for an individual to be genuinely heard in social and welfare services; yet this opportunity is often narrowed down for adolescent substitute care clients with mental health challenges.
One of the participants vented her frustration at being diagnosed with schizophrenia based on only one short appointment with a doctor, mostly because schizophrenia has run in her family. She would have liked to tell her version of the genesis of her anxiety and substance abuse, but the mental health diagnosis was made without hearing her. In spite of the exposing medical factors, it is important to take the social determinants of health and the patients’ reflection of the situation into account while forming an overall picture of a patient.
He diagnosed me with schizophrenia on that first visit. It can’t even be diagnosed like that! He justified it so that when I have taken these drugs and reportedly been in mild psychosis and when it has lasted so long, it can be called schizophrenia. (Interviewee 4)
In this particular case, the diagnosis was changed after a short period. However, it is important to comprehend that decoding a possible misdiagnosis is not automatically easy and can lead to improper treatment and medication that at the worst worsens the patient’s condition even further and prevents the root causes of problems from being raised. Furthermore, improper diagnosis can also raise the stigma that follows adolescents to other welfare services. The key findings of the study are presented in Table 1.
Essential Elements of Encountering Traumatized Adolescents in Substitute Care.
Discussion
In this article, we have examined the experiences of young people with a history in substitute care and mental health challenges in regard to their communication with welfare professionals in four frameworks of interpretation: affective, cognitive, behavioural and as an ethical aspect of interaction. We conclude that empowering, rehabilitative communication requires a genuine encounter that arises from actively taking all of the previously described factors into account in client interactions, throughout the process. Our data indicate that raising an awareness of both the attitudes and the actual activities in the communication of welfare professionals is crucial from the point of view of a rehabilitative encountering of adolescents in substitute care.
We also conclude that the role of communication cannot be exaggerated enough while working with adolescents. From an adolescent perspective, the communication takes forms of which the professionals might not even be aware of in their everyday work. For example, adolescents perceive professionals also as potential counsellors who they can widely learn from. It is therefore important to reinforce the awareness of the dimensions of the communication, together with the communication based, non-written roles of welfare professionals in their education.
According to our data, welfare professionals working with adolescents in substitute care need to actively pay attention to the importance of the experienced trauma that may lie in the past of an adolescent. The trauma-informed approach can be seen as an appropriate tool for professionals for recognizing the significance of early adversity in the lives of adolescents. As Levenson (2017) states, trauma-informed practice lays a special emphasis on the symptoms of adolescents that can be understood as an indication of maladaptive coping, instead of problems and behaviour disorders themselves. A shared understanding of how early trauma can shape the worldview of the clients assists professionals in supporting the healthy psychosocial functioning of adolescents. It also advances the evolvement of an open dialogue between adolescents and the professionals and thus contributes to good encountering. In interpreting communication, as Hargie (2019) states, the external world comes into contact with the internal world of memories, expectations, hopes, needs and even fears. An awareness of the trauma helps to understand adolescent response patterns and thus reconciles internal thought patterns to the demands of the external world, which creates safety and trust—the conditions for a therapeutic, rehabilitative encounter. Accordingly, the trauma-informed capabilities of staff at child welfare institutions should be strengthened through additional training.
Our findings indicate that despite the severe manifold symptoms, adolescents usually have the will and urge to become active agents in the management of their own affairs. But in order to feel genuine participation in their rehabilitation, adolescents need both information and support. The communication with welfare professionals plays an essential role in this process. At its best, empowering communication promotes the rehabilitation of an adolescent, but at its worst, communication can form an obstacle in recovery by reinforcing their traumatic experiences. An effective rehabilitative communication requires time and special reflective attention from the professionals.
Although communication forms the backbone of client work, various elements of interaction have been little studied or analysed in the framework of substitute care clients. Again, this study did not examine direct interaction, but rather adolescents’ experiences and reflections on them. From the perspective of developing professional practices, our study indicates that the welfare professionals need constant awareness of the inherent power imbalance in the professional–client relationship and do their best to flatten the hierarchy in communication. It is also essential that the professionals comprehend that these power structures are always present at both individual and institutional levels of the communication. It is possible to influence both of these by way of one’s own actions, and so active critical reflection on both individual working methods and the structural guidelines on welfare work and service structure should be an intrinsic part of all work concerning substitute care.
The advantage of our study was that we managed to give voice to 19 young adults who represent a very vulnerable clientele whose possibilities to express themselves are often restricted. The participants were able to reflect their own role, their interactions with professionals and the way professionals had faced adolescents. Some degree of selection may have occurred while forming the overall data. In particular, young people who have experiences of a certain kind and have wanted to underline specific themes have possibly been ones who wanted to take part in the research. However, the participants were recruited from different organizations of the child welfare services of the public sector and also voluntary organizations of experts by expertise. Furthermore, the participants were also from different regions of the country. Our sample comprised mainly females, which may reflect some bias. Two males cancelled their participation last-minute. Previous studies show that young men may have more externalizing symptoms than women, and disorders with disruptive behaviour, such as attention-deficit/hyperactivity disorder and conduct disorder, are more common among males (Gyllenberg et al., 2018), which may rise their threshold to participate in research. The gender was not a criterion for selecting participants. Instead, we were interested in the experiences of individuals.
The experiences of the participants were mainly negative without gender differences. In the citations, comments from particularly traumatized young people may have been emphasized. This is due to the fact that the participants in question reflected their experiences from various perspectives and often phrased their experiences in more vivid ways than others. Varying time has also passed since the participants had the encounters they described, and it is possible for later negative experiences to influence how they remembered the encounters. It is also noteworthy that most of the participants had been in a child welfare institution, in which the climate for communication can in general be different from that of a foster family or kinship care.
Our study contributes to generating new perspectives to developing professional practices. In the future, attention must be paid to the processes enabling the voice of this vulnerable clientele to be heard in earlier stages of the services—not only reflecting the experiences of the past. The prevention of cynicism among welfare professionals should also be acknowledged. As Saakvitne et al. (2000) point out, safe rehabilitative relationships are always consistent, predictable, non-violent, non-shaming, and non-blaming. An adequate staff size in substitute care facilities and mental health services and access to sufficient professional supervision are tangible ways to combat cynicism among professionals.
Professionals need to reflect their communication competence on a regular basis. The development of communication skills should also be supported by the working conditions and continuous training. The trauma-informed approach should cover the entire service systems, crossing professional and organizational boundaries. An example of good practice is, for example, the Sanctuary model, where the trauma-informed approach steers the operation of the entire organization (Galvin et al., 2022). We recommend that the child welfare field should enhance child welfare policies to address the traumatic experiences of the young and widely educate professionals about the trauma-informed practices.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The results presented in this article are part of LANUPS project (“Co-research and Co-development of Child Welfare Social Work and Adolescent Psychiatry in Western and Eastern Finland”). The project was funded by the Finnish Ministry of Social Affairs and Health for 2021–2022. The aim of the project was to identify realized services and the service needs of those adolescents, who have been clients of both, substitute care in child welfare and adolescent psychiatric outpatient or inpatient care.