
Abstract
Dysphagia can stem from various etiologies and cause several serious complications. Instrumental evaluation methods for swallowing require special equipment not available everywhere. Thus, an instrumental means to evaluate swallowing that could be used outside a hospital setting would be critical. Dual-axis accelerometers have been utilized in earlier research to recognize swallowing movements. However, no textile-based approaches have been reported. In this study, we developed a textile-based prototype device for identifying swallowing movements. The device used accelerometers and gyroscopes, with eight sensors attached to the fabric. Two female participants were asked to perform two tasks while wearing the device around their neck: sitting still and taking 10 sips of water. The sensor attached to the middle of the thyroid notch level and the two sensors horizontally aligned to both sides of the hyoid bone level were the most accurate in recognizing swallowing movements. No sensor alone could recognize all swallows. However, all the swallows were identified using the combined data from the sensors. Thus, based on these preliminary results, it seems like a textile-based device using accelerometers and gyroscopes could identify swallowing movements.
Dysphagia, or difficulty swallowing, is the abnormal movement of the bolus in the oropharyngeal or esophageal stages of swallowing. 1 This condition can stem from various congenital or acquired etiologies such as neurological diseases and structural abnormalities.2,3 If not evaluated and treated sufficiently, dysphagia may lead to several complications, such as malnutrition, decreased quality of life, or even aspiration pneumonia, which can detrimentally affect the patient.4,5 A swallowing evaluation usually consists of a clinical assessment. Examples are bedside observations by a speech-language pathologist; instrumental evaluation, usually a videofluoroscopic swallowing study (VFSS); or a fiberoptic endoscopic evaluation of swallowing (FEES). 6 During VFSS, the patient is instructed to swallow boluses of differing consistencies mixed with a contrast agent under an X-ray examination. VFSS allows the real-time visualization of the four phases of swallowing: oral preparatory, oral, pharyngeal, and esophageal phases. 7 VFSS also exposes the patient to radiation. Thus, the patient’s safety and radiation dosage should be considered when planning the evaluation and its length: the amount of time the patient can be exposed to radiation is limited. 8 VFSS can only be conducted in the X-ray department, which can be a problem if the state of the patient’s health is not stable enough to move the patient to the X-ray department. FEES is another widely used instrumental evaluation technique. A thin, flexible fiberoptic laryngoscope is passed through the nose to allow a view of the pharynx. The patient is offered colorful liquids and food during the evaluation. 9 FEES enables visualization of the pharynx before and after swallowing but not during all four phases. FEES is an invasive procedure, and patients often report discomfort during the evaluation. 9
The abovementioned instrumental evaluation methods require special equipment and are available mainly in hospital settings. Reliable and user-friendly swallowing assessment devices that could be used outside hospital settings would be significant. An easy-to-use technical solution could benefit many with dysphagia and their caregivers in their everyday lives. A washable, textile-based approach would be ideal to ensure the device’s comfort and wearability. In our study, we created a prototype of a textile-based approach using an elastic knitted fabric to which we attached eight sensors with Velcro tape. Each sensor contained a micro-electromechanical system inertial measurement unit (MPU-6050 MEMS-IMU) with three orthogonal accelerometers and three orthogonal angular velocity gyroscopes. The collar-like fabric was secured around the neck with Velcro tape to allow easy adjustment and opening. This study examined whether the prototype adequately recognized normal swallowing movements from the neck in two different swallowing tasks.
Noninvasive swallowing evaluation devices
As VFSS and FEES have limitations in evaluating swallowing, other instrumental swallowing evaluations have been topics of interest in research. Many noninvasive swallowing evaluation methods have been tested, including dual-axis accelerometers, piezoelectric strain sensors, throat microphones, and nasal airflow cannulas (Table 1).10–23 These solutions have been tested with varying numbers of participants and different boluses, as presented in Table 1. Some of these devices have identified only normal swallows, whereas others have identified abnormal swallows. Most of the research has been targeted to create a device that can reliably differentiate between healthy and abnormal swallows. However, this stage of development has not yet been fully reached, even though some research has produced promising results on differentiating between healthy and abnormal swallows.
Different technical solutions used in the swallowing evaluation
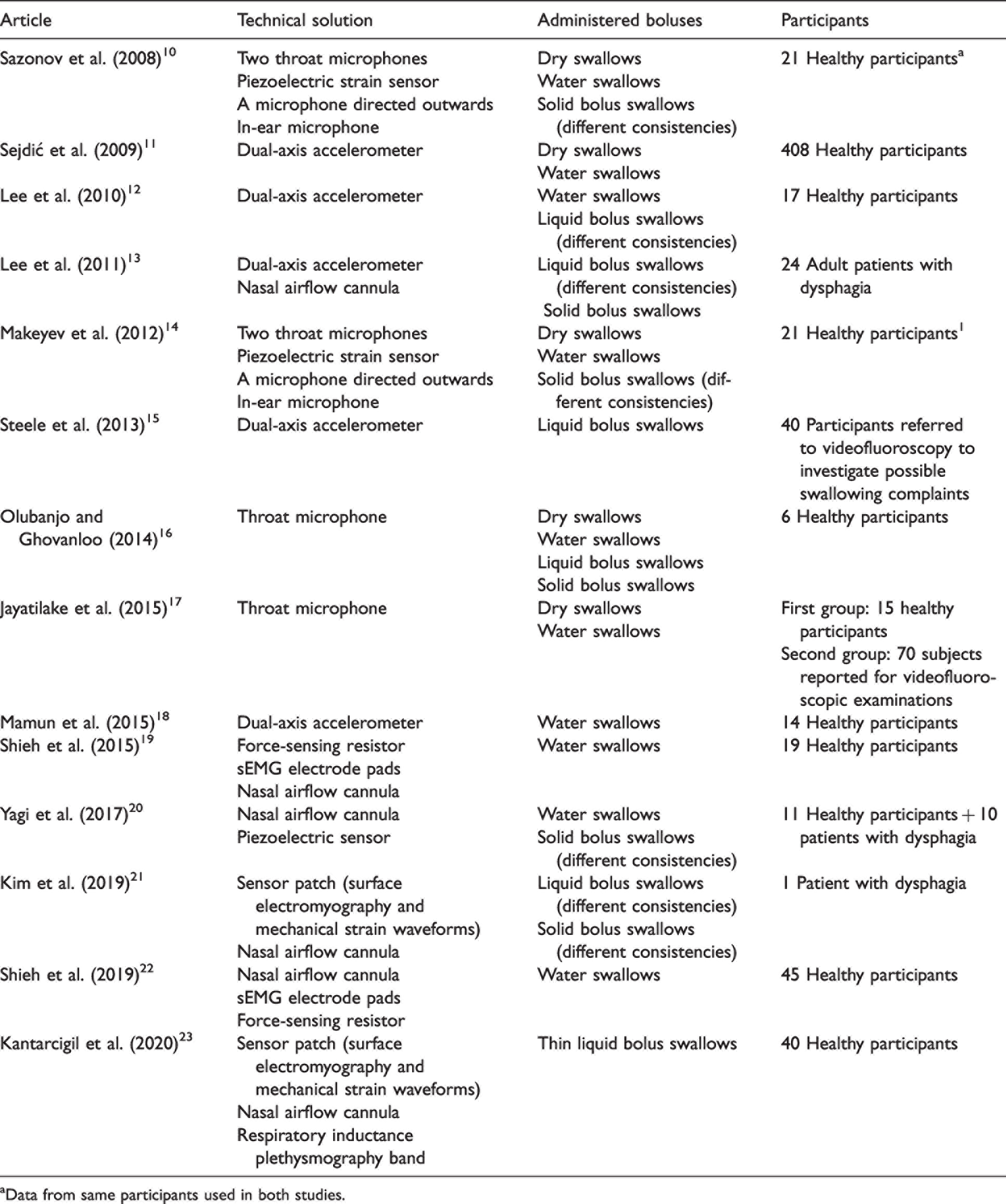
aData from same participants used in both studies.
Many earlier methods have limitations, mainly regarding their wearability. Most of the earlier technical solutions consist of several different components or seem uncomfortable to use due to being attached to the user with tape, which is most often double sided. A textile-based approach would be better than a system requiring tape or other adhesives to be attached to the skin. Wearability is also key in creating a device suitable for long-term use, such as one a patient would wear daily when eating. A textile-based solution would also be easier and more comfortable to put on and take off than one using adhesives directly applied to the skin, as adhesives such as tape may irritate the skin.
Materials and methods
In this study, our goal was to develop a textile-based device that could recognize swallowing based on measuring swallowing movements from the neck. The developed prototype uses accelerometers and gyroscopes and consists of eight small sensors (21 mm ×15 mm × 4 mm). Each sensor contained an MPU-6050 MEMS-IMU with three orthogonal accelerometers and three orthogonal angular velocity gyroscopes. Each sensor measured acceleration and angular velocity on the X, Y and Z axes. All sensors were connected to an LPC1768 microcontroller by a single, shared inter-integrated circuit (I2C) bus (Figure 1). The multiplexing of the bus among the eight sensors was necessary because the sensor address can only be set to two differing values. The microcontroller solved the sensor address issue by changing the addresses in real time so that only a single sensor had the ‘active’ address used for communication, while the other seven had a passive address. The microcontroller fetched a complete set of accelerometer and gyro data from each sensor five times a second and sent these data to a PC through a USB port. The eight sensors were attached to the textile base using Velcro tape. The textile base of the device was an elastic knitted fabric (Figure 2). The fabric was secured around the neck with Velcro tape.
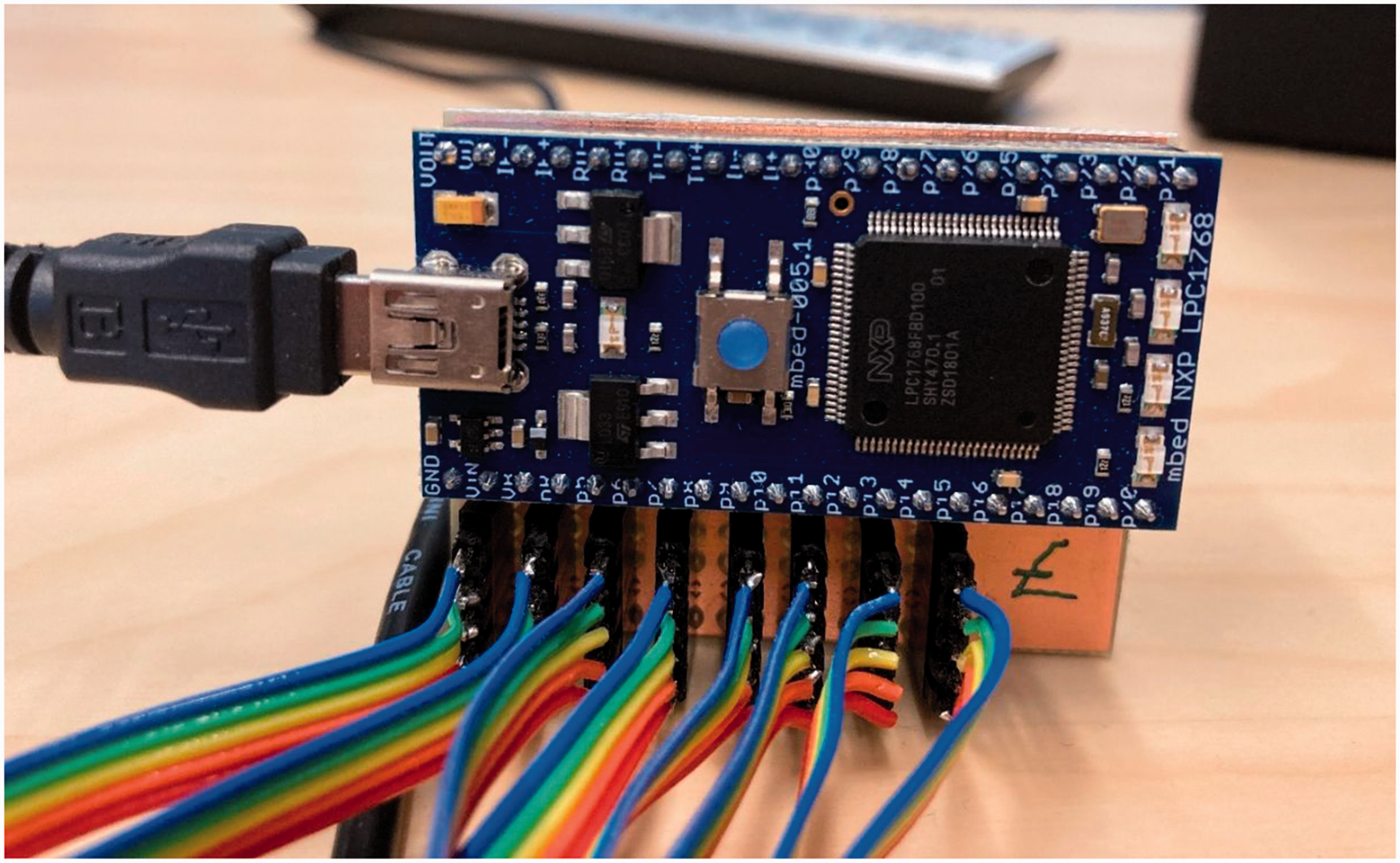
The LPC1768 microcontroller.
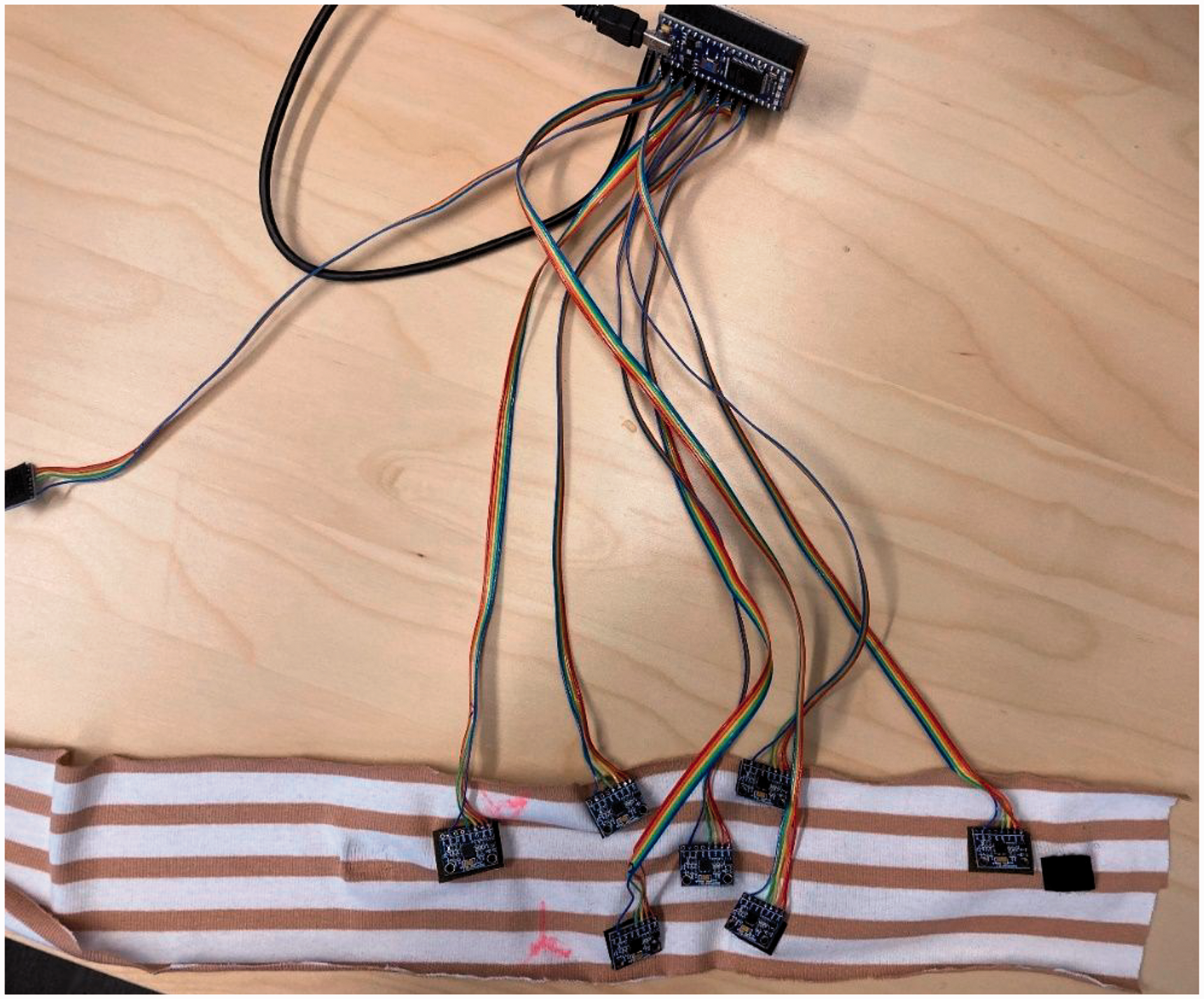
The device with the sensors attached to the fabric.
Participants and procedure
Two female participants tested the device. Participants were healthy volunteers and had no diagnosed or subjectively experienced dysphagia. The textile with seven sensors was secured around participants’ necks with Velcro tape (Figure 3). The seven sensors were placed as follows (Figure 4): One sensor was attached to the middle of the neck at the thyroid notch level (sensor 1). Two sensors were aligned horizontally to both sides of the neck at the hyoid bone level (sensors 2 and 3). Two sensors were aligned horizontally to both sides of the neck below the thyroid notch level (sensors 4 and 5). These five sensors were located this way because during a swallow, contraction of the suprahyoid muscles results in anterior and superior movement of the hyoid bone and larynx. 24 We aimed to monitor this hyolaryngeal elevation by placing the sensors at the level of the thyroid notch and bilaterally at the level hyoid bone and below the thyroid notch level. In addition, two sensors were attached at the back of the neck – one to the left and another to the right (sensors 6 and 7). The eighth sensor was not connected to the textile, as it was used as a reference. The placement of the device’s sensors was optimized to fit participant 1 by an experienced speech therapist, who palpated the location of the thyroid notch and level of the hyoid bone, and the sensors were placed based on that. For participant 2, the sensor was aligned to the middle of the neck at the thyroid notch level and placed in the same position as in participant 1. Due to the participants’ structural differences, sensors 2, 3, 4 and 5 were slightly off from ideal positioning. Small pieces of tape on both sides of the neck were used to secure the textile due to the fabric’s elasticity.
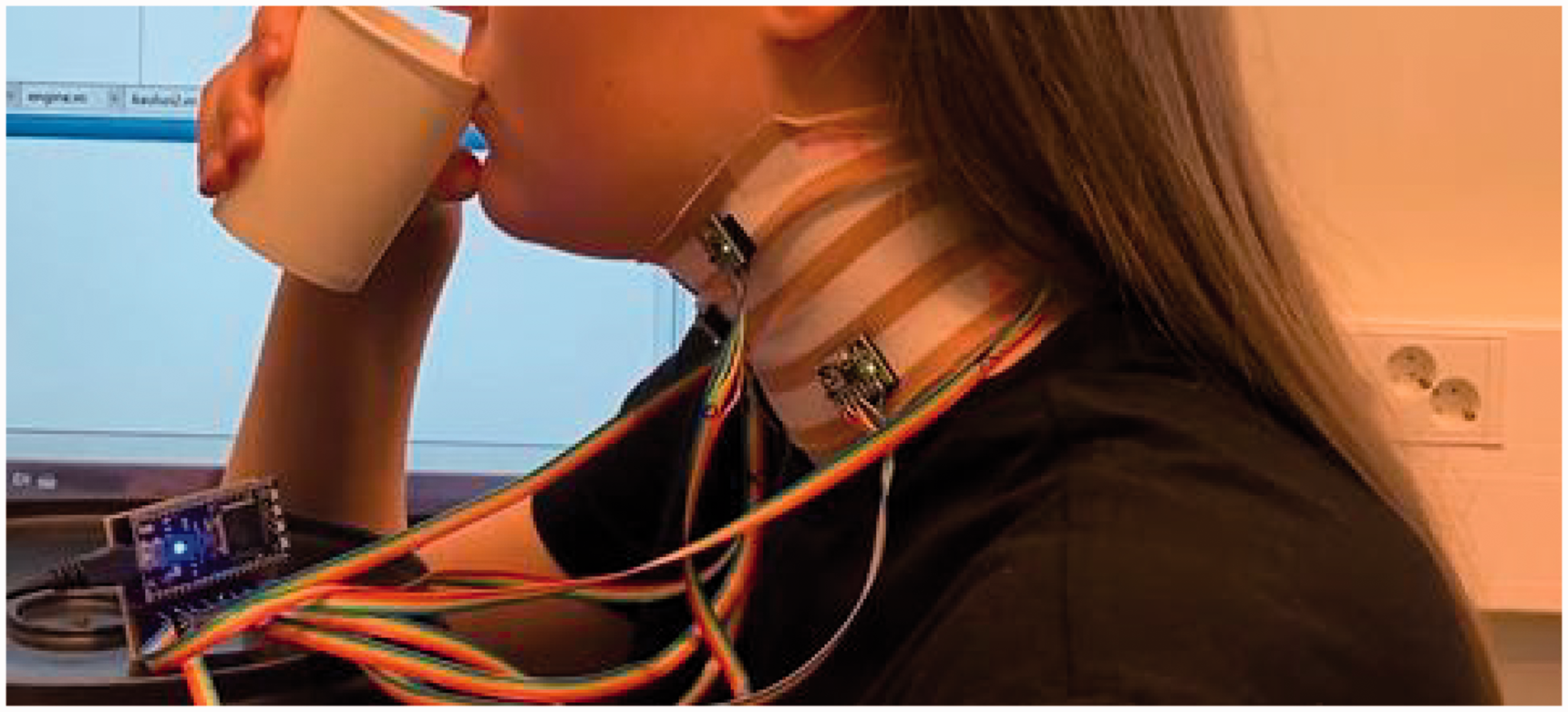
Testing setup.
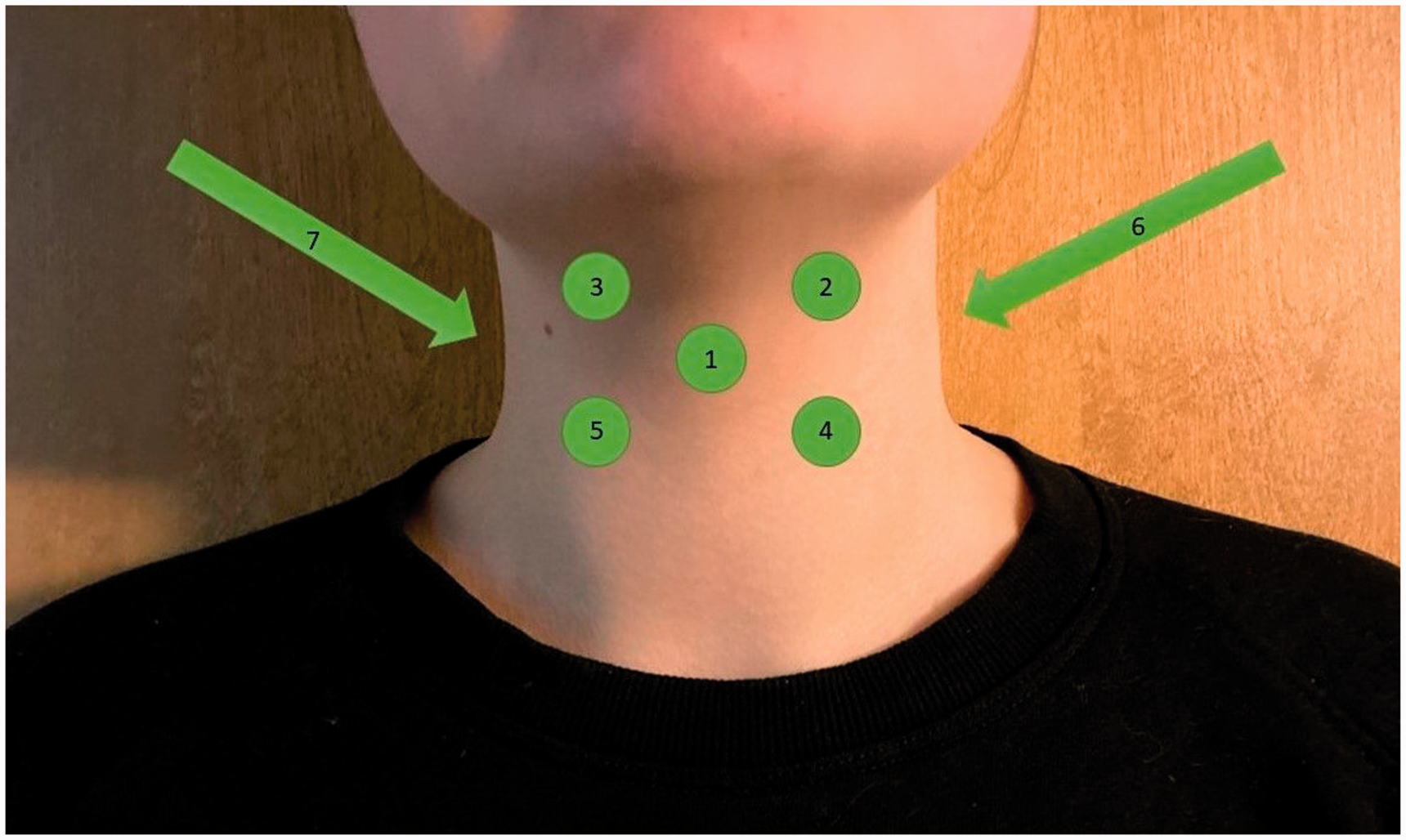
The sensor placements (1–7). One sensor (8), not pictured, was not attached to the participant.
The participants were asked to do two tasks while wearing a textile with sensors. Initially, they were instructed to sit still for 3 minutes, look forward, and spontaneously swallow whenever needed. The participants were instructed to not talk during the tasks, so the research team members in the room conversed about a subject irrelevant to the research to create natural background noise. Secondly, participants were instructed to take 10 sips from a cup of cold water. They were to decide the volumes of the sips themselves and then set the cup back down on the table between each sip to ensure a short pause between sips. Therefore, the bolus size varied between participants and swallows. An experienced speech therapist monitored the research situation at the time. Both participants were videotaped from a lateral view with a mobile device during both tasks.
A speech-language therapist student identified the swallows from the video footage under an experienced speech-language therapist’s supervision. The swallows were identified from the video based on the visible hyolaryngeal elevation, which occurs during swallowing. The exact time of when the swallow occurred was noted for every swallow. The swallows identified from the video were used as a baseline, and the swallows identified from the sensors were compared to the swallows identified from the video.
Results
Table 2 shows the number of swallows recognized from the sensors compared with the swallows that had happened, which were confirmed from the video footage. Based on the video footage, participant 1 swallowed nine times and participant 2 swallowed seven times while sitting still (Table 2). Both participants also swallowed 10 times during the water swallowing task, as they were instructed to take 10 distinct sips. The swallows were identified from the data using a set threshold (±0.04) for the water swallows and a set threshold (±0.03) for the dry. As this was a preliminary test, these thresholds were set based on the collected data, thus setting a threshold beforehand was impossible. The different thresholds were set because the water swallows were more distinct than the dry swallows. After the thresholds had been set, all swallows were identified from the data of each sensor separately. The swallows identified from the data were then compared to those identified from the video.
The number of swallows the sensors could recognize compared to those recognized from the video

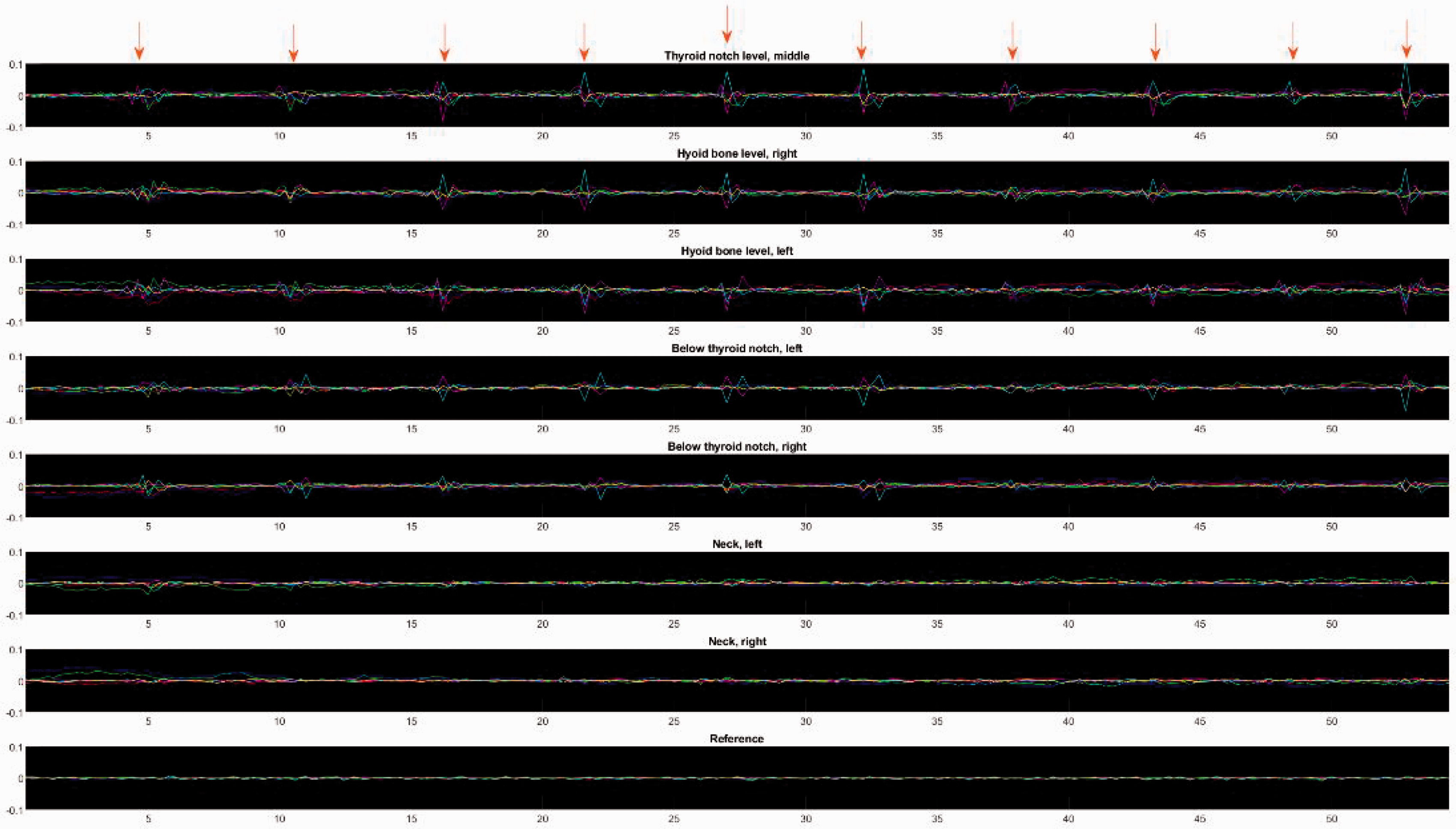
The swallowing movements from both participants can be seen as spikes in the data collected by the device (Figures 5, 6, 7 and 8). Three of the eight sensors were the most accurate in recognizing the swallowing movements: the sensor attached to the middle at the thyroid notch level (sensor 1) and the two aligned horizontally to both sides at the hyoid bone level (sensors 2 and 3) as seen in Table 2. None of these sensors could independently recognize all the swallows. However, all the swallows were differentiated using data from all three sensors. For sensors 4 and 5, their ability to identify swallows varied between participants and task types. Three of the eight sensors (6, 7 and 8) did not accurately identify swallowing movements as intended because their purpose was to serve as a reference.
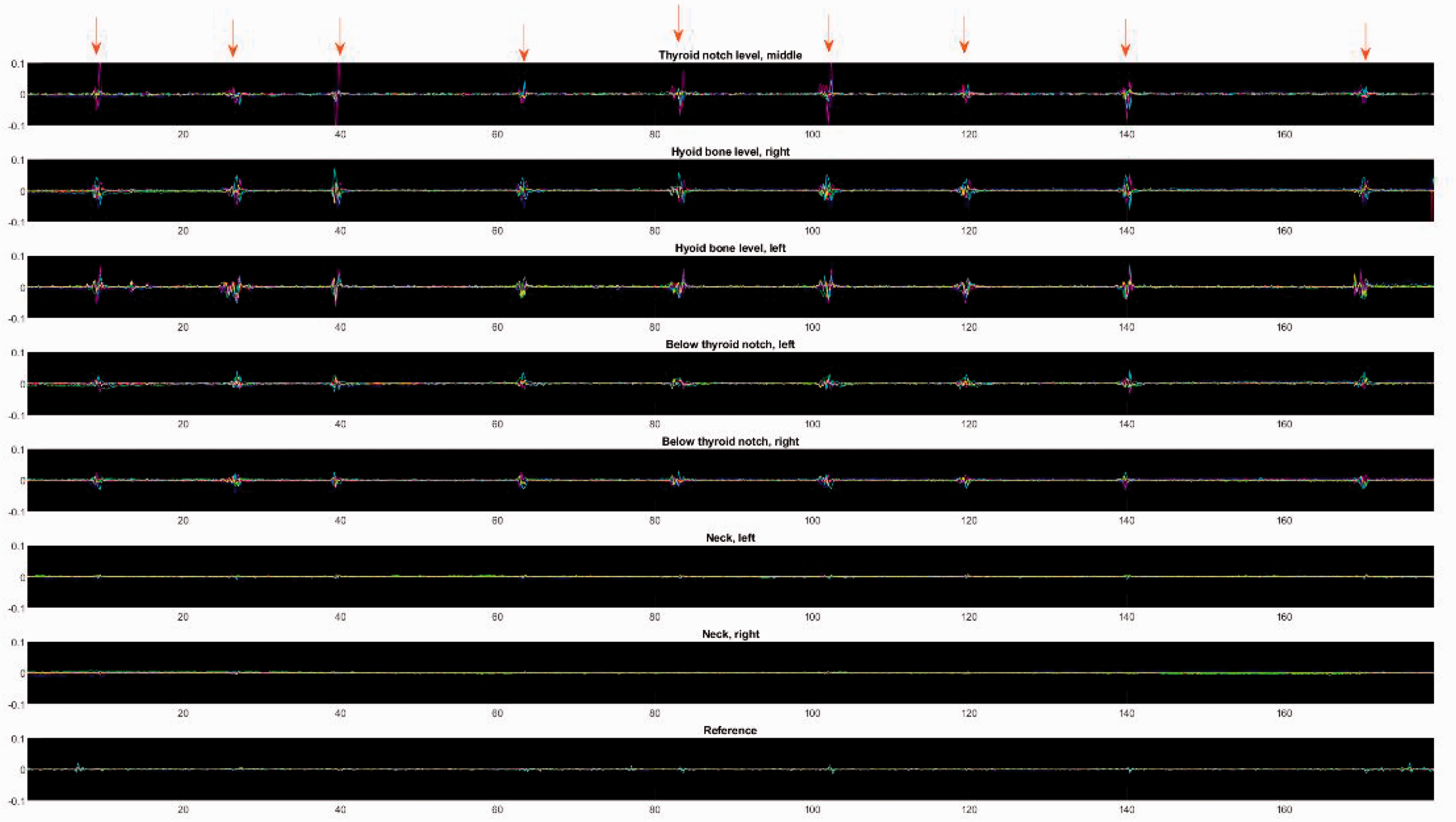
Participant 1 sitting still. The swallows are marked with red arrows. The X axis shows the time in seconds, the Y axis shows the fetched data values. The different colors represent the six different values measured by the sensors. Acceleration on the X axis is marked with red, acceleration on the Y axis is marked with green and acceleration on the Z axis is marked with blue. Angular velocity on the X axis is marked with cyan, angular velocity on the Y axis is marked with magenta and angular velocity on the Z axis is marked with yellow.
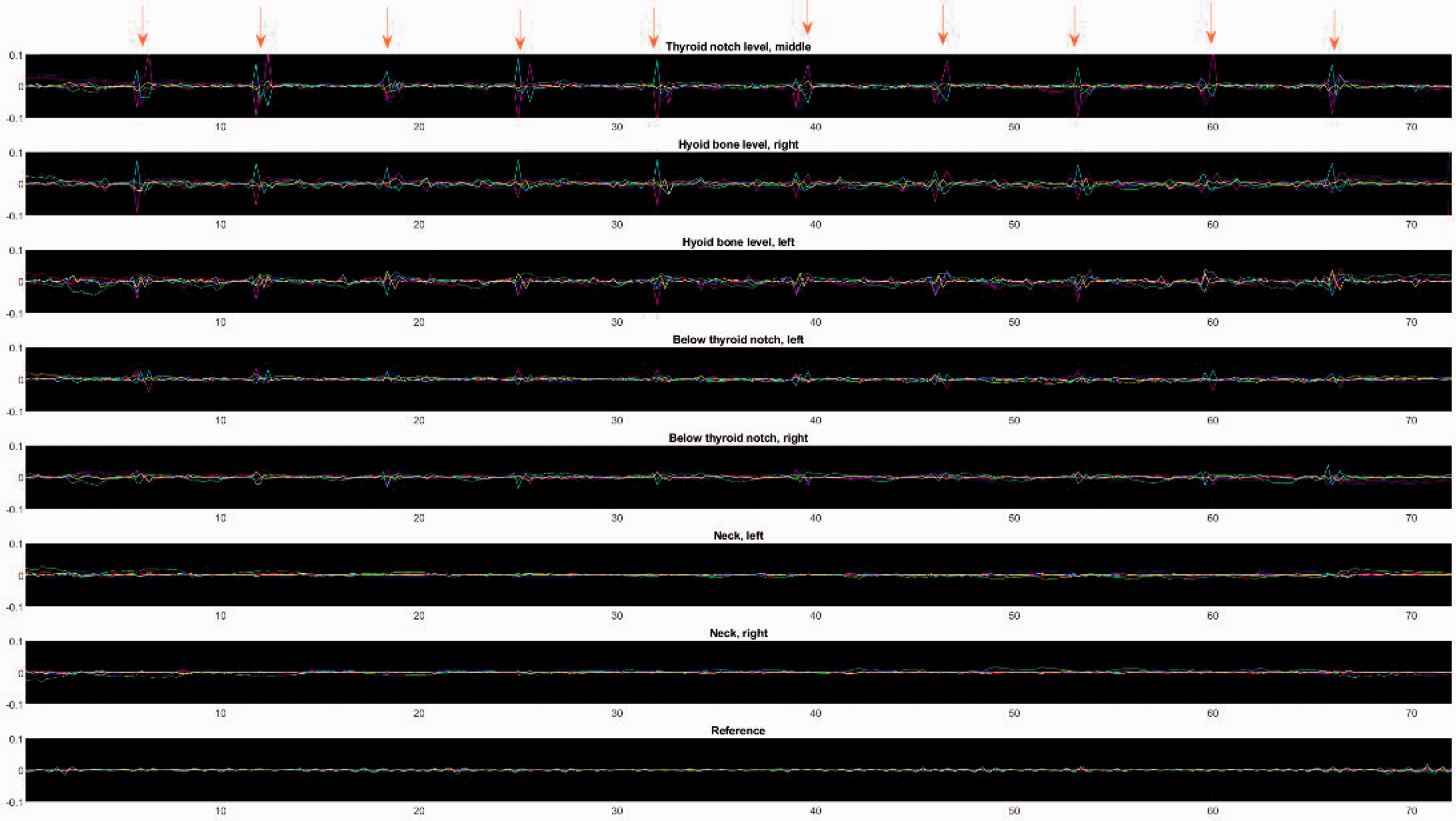
Participant 1 taking 10 sips of water. The swallows are marked with red arrows. The X axis shows the time in seconds, the Y axis shows the fetched data values. The different colors represent the six different values measured by the sensors. Acceleration on the X axis is marked with red, acceleration on the Y axis is marked with green and acceleration on the Z axis is marked with blue. Angular velocity on the X axis is marked with cyan, angular velocity on the Y axis is marked with magenta and angular velocity on the Z axis is marked with yellow.
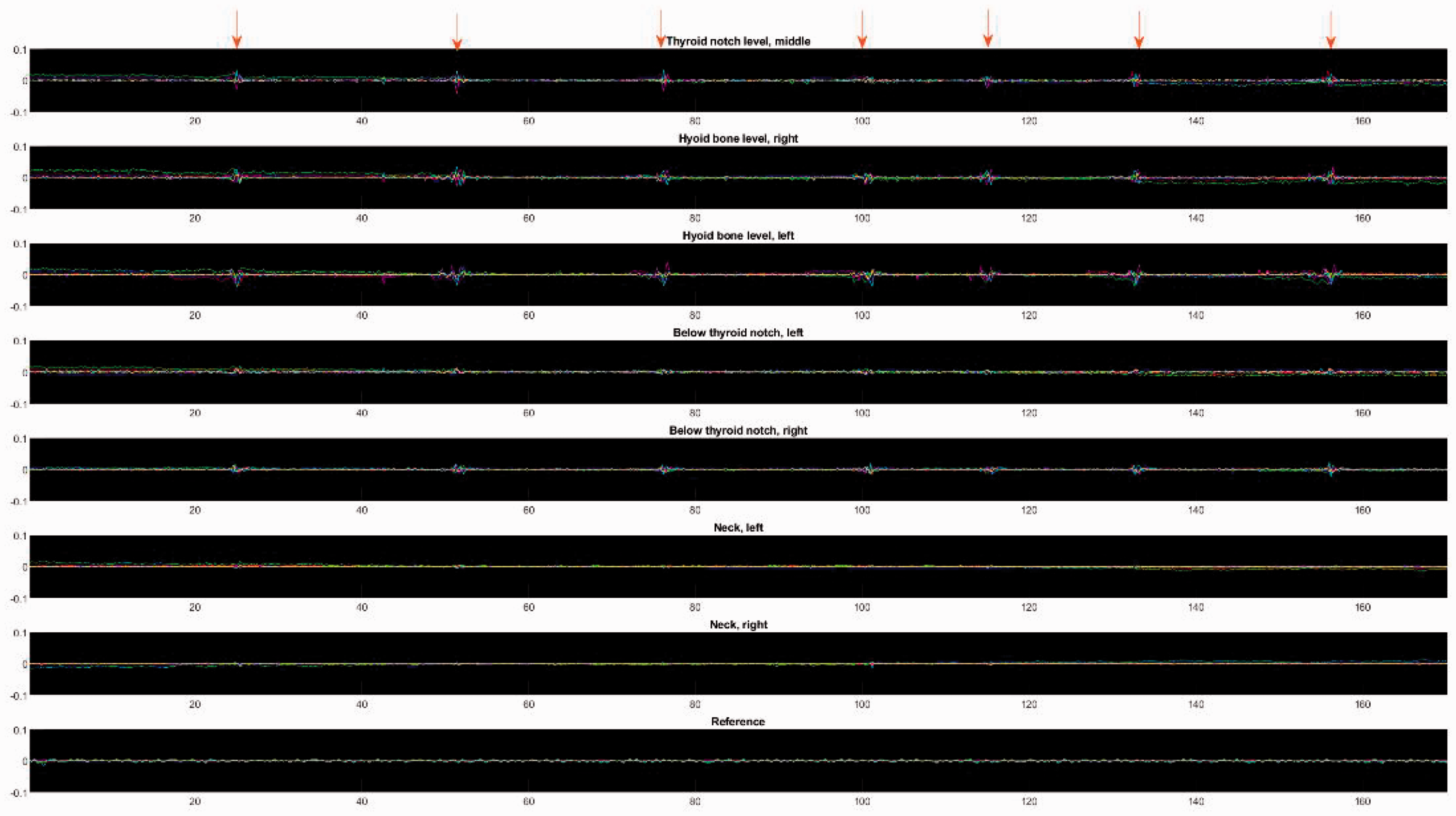
Participant 2 sitting still. The swallows are marked with red arrows. The X axis shows the time in seconds, the Y axis shows the fetched data values. The different colors represent the six different values measured by the sensors. Acceleration on the X axis is marked with red, acceleration on the Y axis is marked with green and acceleration on the Z axis is marked with blue. Angular velocity on the X axis is marked with cyan, angular velocity on the Y axis is marked with magenta and angular velocity on the Z axis is marked with yellow.
Participant 2 taking 10 sips of water. The swallows are marked with red arrows. The X axis shows the time in seconds, the Y axis shows the fetched data values. The different colors represent the six different values measured by the sensors. Acceleration on the X axis is marked with red, acceleration on the Y axis is marked with green and acceleration on the Z axis is marked with blue. Angular velocity on the X axis is marked with cyan, angular velocity on the Y axis is marked with magenta and angular velocity on the Z axis is marked with yellow.
Discussion
This prototype had eight sensors. Based on the initial data, it seems the number of sensors could be reduced. The two reference sensors (6 and 7) attached at the back of the neck could be replaced with a single sensor; the reference sensor 8 will be unnecessary because the sensor attached at the back of the neck can be a reference. Although the two sensors aligned horizontally to both sides below the thyroid notch level (4 and 5) did not accurately detect the swallowing movements in the two tasks, these sensors might help detect swallowing movements in other tasks, such as talking while eating, which is a task that will be tested with the next version of the device.
The prototype in this study was optimized for participant 1; for participant 2, only the sensor on the thyroid notch level was in its optimal place. This can be seen in the data, which show more visible swallowing movements for participant 1 than participant 2. That the device could not identify the swallows of participant 2 as efficiently due to the other sensors being slightly out of optimal placement is possible. Notably, a speech-language therapist specializing in swallowing stated that based on palpation and visual assessment, the movement of the thyroid notch during swallowing was smaller in participant 2 than in participant 1. This might partly explain the variation of the results between the participants, as previous research suggests variability exists in hyoid and laryngeal displacement during swallowing due to several factors. 25
This study presented an early prototype with several practical and technical downsides. The most significant functional problem was that the prototype was not wireless: wires limit the use and testing of the device and the movement of the person wearing it. Wires also add to the sensors’ weight, possibly causing the sensors to move the fabric out of place. As the prototype consisted of a single layer of fabric, the sensors had to be attached using Velcro tape. This method of attaching the sensors is not ideal and is not a true textile-based solution, and the sensors should be integrated in the next prototype. The next version is wireless and has all the electronics seamlessly integrated inside two textile layers. Thus, the next step is producing a wireless version with individual small power sources attached to each sensor.
The textile-based approach seemed a good fit for both participants but could not be easily optimized. Thus, a different system to optimize the placement of the sensors for all users is needed. This could be achieved with several changes, such as adding different sizes to ensure a good fit for varying neck circumferences. The fabric in this prototype was not ideal, as it was too stretchy and would not stay put. Additional adhesives were required to keep the material in place: small pieces of tape were attached to both sides of the neck to prevent the cloth from moving. As this was just a prototype, the fabric choice was not ideal. Various fabric choices should be considered for the next version: the fabric should be elastic but stiff enough to stay stationary, so its movement will not affect the sensors. Furthermore, by replacing the connectors with conductive thread, which is extensively studied in the field of textile electronics,26–28 a more textile-integrated prototype will be created next. The participants still considered the current textile-based approach comfortable to use, encouraging even more research on textile-based solutions. To evaluate the comfort of a textile-based device further, usability and the user experience should be evaluated in a separate study with more participants. The usability of the textile-based solution will be evaluated more in depth in a parallel study regarding the design and fabrication of the improved device.
Conclusions
Based on this pilot study, a textile-based device with accelerometers and gyroscopes seems like it could be a viable option in identifying swallowing movements. This result aligns with earlier research on using accelerometers to identify swallows from healthy individuals.11,12,18 Based on these promising results, a textile-based device works as well as other technical solutions. Furthermore, a textile-based device is more comfortable for the user, especially for long-term use. More research on textile-based options should be conducted. The next prototype should be wireless with sensors fully integrated into the fabric to improve usability, and tested on more people to determine whether a textile-based swallowing evaluator can identify swallowing movements from those with varying anatomical structures while performing different tasks.
Footnotes
Author’s Note
Johanna Virkki is also affiliated from Tampere Institute for Advanced Study, Tampere University, Tampere, Finland.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this articleL This research is funded by Academy of Finland (decisions 332168, 337861).