
Abstract
Debates around the benefits of flexible work arrangements for employee well-being are limited by a lack of empirical analyses on whether flexible working enables employees with work or family stressors to cope with their levels of stress. This study examines whether the availability and use of different flexible work arrangements are associated with lower allostatic load (an index of chronic stress-related biomarkers) in a large representative study of UK adults. Male and female employees who made use of reduced hours working arrangements had lower levels of allostatic load. Among women caring for two or more children aged under 15, there was a difference of almost one unit of the allostatic load index (an additional biomarker risk) between women who used reduced hours flexible work and those without such arrangements. Reduced hours flexible work arrangements could enable women who combine work and family roles to reduce their levels of chronic stress.
Introduction
Working times and workplaces have become increasingly flexible (Messenger, 2011), with greater heterogeneity in the location, timing and the amount employees work (Fagan et al., 2012). Flexible work arrangements are work options that permit flexibility in terms of where, when or how much work is completed (Rau and Hyland, 2002). Their central feature is that it is the employee, not the employer, who chooses the working arrangement (Alis et al., 2006).
The most common types of flexible work arrangements provide some degree of choice in the contracted hours of work. Employees on such ‘reduced hours’ flexible working arrangements are contracted to work less than standard, basic, full-time hours. These include working part-time, job-sharing and term-time working. Variable hours (which include flexitime and annualised hours) and restructured hours (e.g. compressed working week) involve some flexibility around working time (‘flextime’). Other types of flexibility include working from home arrangements (‘flexplace’) and informal flexible arrangements.
Flexible work may help workers manage work and family responsibilities (Edwards and Rothbard, 2000). When the demands of the working role affect the ability of a worker to perform a family role (or vice-versa), work-to-family or family-to-work interference (or conflict) is thought to occur (Frone et al., 1992). Having control over the timing and location of work can help employees cope with such potential stressors (Hammer et al., 2005). However, flexible work could also lead to role-blurring, work–family multitasking and other related stressors which could result in greater stress. For example, flexible work arrangements may result in blurred boundaries between work and home roles (Ashforth et al., 2000; Desrochers et al., 2005), leading to increased work-to-family conflict.
This study locates research on flexible work arrangements and well-being within the broader framework of the sociology of work and well-being (Tausig, 2013). This framework addresses the ways in which work and well-being are related, through social structural explanations for work-related well-being, and by extending the typical economic and social outcomes researched in the sociological study of labour markets to psychological, health and well-being outcomes. Most research on work and well-being focuses on how individual aspects of working conditions, such as psychological work stressors, are related to workers’ well-being. Such approaches ignore broader sociological concerns, such as new forms of non-standard and temporary work, and the role of social class and household factors in labour market participation and consequent worker exposure to stressful job conditions.
Determinants of Flexible Work Arrangements
The increase in the availability of flexible working arrangements has been driven, in part, by demographic trends and legislative changes. There are more workers, particularly women, juggling the demands of employment with care responsibilities and a higher proportion of older workers seeking reduced hours working arrangements. Recent legislative changes in the UK have encouraged employers to offer more flexible working arrangements.
Although flexibility over working arrangements implies control over life decisions, there are structural constraints in gender, workplace culture and norms that could overshadow an employee’s apparent control over their working arrangements (Lewis et al., 2007). Women workers, especially those with caring responsibilities, are expected to combine work and family roles. Participation in flexible work arrangements is gendered and women are more likely than men to be involved in working arrangements that entail time flexibility and reduced earnings (Russell et al., 2009). Reduced hours working arrangements may just reflect such gender norms rather than real control over working schedules, and thus such arrangements may not have any actual effects on women’s levels of well-being or stress. It is also important to consider whether such flexible work arrangements are used, not just if they are available. Formal flexible work policies may be available in workplaces, but can be unevenly implemented across work units by supervisors, and may be selectively available to higher status workers (Kossek and Ozeki, 1998; Thompson et al., 1999). Workers in more routine occupations tend to have higher levels of managerial scrutiny than those in professional occupations, resulting in certain arrangements like flexplace, flextime and informal arrangements being more common among professional employees and those in senior positions (Kelly and Kalev, 2006). Requests for the use of such arrangements by higher skilled workers may be more readily accepted by employers (Brescoll et al., 2013), which may partly be due to greater trust placed in such workers, and their perceived potential to increase their productivity through the use of such arrangements (Lott and Chung, 2016). This leads us to RQ1: What are the determinants of the availability and use of different types of flexible working arrangements among UK employees? We hypothesise that workers in routine occupations use flexible arrangements less often than workers in professional occupations.
Work–Family Conflict and Its Consequences
The concepts of work–family conflict and role strain theory are central to research on flexible working arrangements and well-being. According to role strain theory (Goode, 1960), the demands of multiple roles can conflict when the individual is unable to meet the expectations of all roles and must consequently let go of some these roles. Work–family conflict is a specific form of inter-role conflict in which role pressures from work and family domains are mutually incompatible (Frone et al., 1992). Work–family conflict is associated with increased psychological strain, with higher levels of stress and lower levels of well-being associated with both work-to-family and family-to-work sources of conflict. Flexible work practices are meant to enable employees to achieve a more satisfactory work–life balance which should reduce work–family conflict. Across four meta-analyses of the association between flexible work arrangements and work-to-family/family-to-work conflict, greater flexibility was associated with lower conflict, although there was considerable heterogeneity in the reported associations (Allen et al., 2013).
There is potential for flexible working to result in the work intensification (Burchell and Fagan, 2004). Among professional workers in the UK private sector (Kelliher and Anderson, 2008), flexible workers reported higher levels of job satisfaction than their non-flexible counterparts, alongside the somewhat paradoxical outcome of work intensification. Some employees are prepared to increase the efforts they put in at work in return for their flexible working arrangements (Golden, 2001). Thus, high autonomy in the use of working hours may be linked to additional hours worked at home, and consequently higher work pressures.
Some of the debates around whether flexible work arrangements are good or bad for employee well-being are specific to the type of arrangement. Concerns about blurred boundaries between work and home roles mainly arise from flexplace arrangements. Negative career consequences are associated with part-time and other reduced hours working arrangements. Flextime arrangements such as non-standard work hours could be detrimental to mental and physical health. It is thus crucial to distinguish between types of flexible work arrangements. These debates lead us to RQ2: Are (different types of) flexible working arrangements associated with lower levels of stress? We hypothesise that employees who use flexible work arrangements have lower levels of chronic stress responses than employees who cannot or do not use such flexibility.
Theories of Social Stress and Allostatic Load
Inference from self-reported measures of work–family conflict may be biased by a number of cognitive, psychological and other measurement issues (Colombo and Ghislieri, 2008). These conflict or stress measures also conflate the stressor (the combination of work and family factors) with the stress response (the perceived conflict). This study moves away from psychological models of work–family conflict, and incorporates theories of social stress such as the stress process model (Pearlin et al., 1981) which distinguishes between different social stressors arising from the demands of work or family life, and stress reactions such as depression, low mood and well-being. Caregiving is a typical example of family stressors, which can interact with work demands to impact on a person’s well-being. Parents of young children are at particular risk of work–family conflict (Haslam et al., 2015). Working conditions that are not flexible to these family demands, such as long working hours, could adversely impact on a person’s stress reactions.
Measures of biological stress responses are increasingly being collected in social surveys. Perceived stress activates a physiological response that, if prolonged, leads to dysregulated cardiovascular, immune and endocrine functioning (McEwen, 2015). Stress hormones controlled by the neuroendocrine system influence the cardiovascular, metabolic and immune systems in attempts to compensate for dysregulated stress hormones (McEwen, 2015; McEwen and Stellar, 1993). Allostasis is the physiological process that enables recovery from social and environmental shocks and stressors (McEwen, 2000). Repeated stressful events arising from combinations of social and environmental stressors and major traumatic life events result in chronic stress, which in turn affects health (McEwen, 2015). Allostatic load is said to occur when a person’s biological systems do not adapt to or recover from repeated stressors, resulting in persistently elevated or altered levels of a number of biomarkers associated with the stress response, or ‘chronic stress’. The allostatic load model is thus a measure of cumulative wear and tear in a number of physiological systems. It has been consistently associated with poor health and the combined index consisting of all the biomarkers was a better measure for predicting mortality compared to each biomarker analysed separately (Castagné et al., 2018).
Inflexible work arrangements could have a direct effect on allostatic load, especially when combined with family responsibilities such as looking after young children. This leads us to RQ3: Is the combination of work and family stressors associated with higher levels of allostatic load? We hypothesise that the combination of longer working hours with childcare is associated with higher levels of allostatic load compared to those without childcare responsibilities. We will also examine whether flexible work can moderate the effect of work–family stressors on allostatic load, enabling those with the combination of work and family stressors to cope better in terms of their chronic stress responses. This leads us to RQ4: Is the use of flexible working arrangements associated with lower allostatic load among workers who combine childcare and longer working hours? We hypothesise that workers who combine childcare with longer working hours and who use flexible work have lower levels of allostatic load than those in jobs with similar work and family conditions without such flexible arrangements.
Methods
Data
This study draws upon data from waves 2 and 3 of Understanding Society, the UK Household Longitudinal Study (UKHLS), a nationally representative household panel study, which began in 2009 recruiting over 60,000 adults in 40,000 households (Institute for Social and Economic Research et al., 2016). Further details of the study design are available elsewhere (Buck, 2008). In 2010–2012 (waves 2 and 3), adult respondents were invited to take part in a nurse health assessment interview, approximately five months after the main interview, which collected a range of physiological measures and blood samples (Institute for Social and Economic Research, 2014). There were 54,597 respondents at wave 2 with a full or proxy interviews of whom 35,937 were eligible for a nurse visit (Supplementary Figure S1). Nurse visits were only conducted on the UKHLS wave 2 General Population Sample, and Northern Irish participants were excluded. This sample reduced to 17,436 employees once those who were not in paid work or who were self-employed were taken out. A further 665 participants with missing covariates and missing auxiliary predictors of missing biomarkers were taken out of the analytical sample. This sample of 16,771 employees reduced to 9556 mainly because of a large number of refusals to the nurse visit, and then to 6025 when respondents with missing allostatic load measures were deleted.
Allostatic Load
The allostatic load index has previously been used in UKHLS to measure health-related effects of work stress and job quality (Chandola and Zhang, 2018). We used 11 available biomarkers measured in UKHLS that cover the systems involved in allostatic load: the neuroendocrine system (DHEA-S, insulin growth factor 1); the metabolic system (ratio of total to HDL cholesterol, triglycerides, HbA1c, creatinine clearance rate); the immune and inflammatory systems (clauss fibrinogen, C-reactive protein); the cardiovascular system (pulse rate, systolic and diastolic blood pressure) and the anthropometric system (waist-to-height ratio) – see Table S1 for more details. For calculating the creatinine clearance rate, we used the Cockcroft & Gault equation. Highest (sex-specific) quartiles of fibrinogen, C-creative protein and ratio of total cholesterol to HDL cholesterol, Triglycerides, HbA1c, systolic and diastolic blood pressure, and waist-to-height ratio were coded as 1 and the remaining quartiles as 0. The lowest quartiles of insulin growth factor 1, creatinine clearance rate and DHEA-S were coded as 1 and the remaining as 0. The allostatic load index was a sum of the 11 biomarkers with a maximum score of 11 (see Supplementary Figure S2 for the distribution). Respondents had to have at least one observation of a biomarker within a system to contribute to the overall allostatic load index. Eight of the 11 biomarkers were blood based, while three non-blood-based biomarkers were additionally collected during the nurse health assessment – pulse rate, blood pressure and waist-to-height ratio. Pulse rate and blood pressures were measured using the Omron Hem 907 electronic sphygmomanometer, with 5 and 10 mmHg added to diastolic and systolic blood pressures respectively, if the respondent was taking blood pressure medications. We used waist-to-height ratio as a replacement for waist-to-hip ratio to measure body fat distribution (Snijder et al., 2003). Participants provided biomarker data only on one occasion, either at waves 2 or 3.
Flexible Working Arrangements
At wave 2, employees were asked ‘If you personally needed any, which of the arrangements listed on the card are available at your workplace?’ The list of arrangements was grouped into:
Reduced hours arrangements, which included part-time, job-share and term-time working arrangements.
Variable and restructured hours (or ‘flextime’) arrangements, which included flexitime, annualised hours and compressed working week arrangements.
Other flexible working arrangements, which included working from home (‘flexplace’) and other informal flexible working arrangements.
Responses to each of these arrangements distinguished between their availability and use.
Work and Family Stressors
Each adult in households with resident children under the age of 18 was asked if they were mainly responsible for the child. A derived childcare variable was generated by the number of children aged under 15 for whom the adult survey respondent was mainly responsible. This was grouped into no children, one and two or more children (only 2.5% of the sample had three or more children). Hours of work in the respondents’ main job (hours normally worked per week) were grouped into gender-specific tertiles due to the very different distributions by gender (see Supplementary Figures S3 and S4). For men, this grouped into less than 37 hours/week, 37–40 hours/week and 40+ hours/week. For women, this grouped into less than 24 hours/week, 25–37 hours/week and 37+ hours/week.
Covariates
Working arrangements are influenced by socio-demographic and socio-economic characteristics like gender, ethnicity, age, marital status, parental status, education, occupation, family income and work hours, so we controlled for measures of these characteristics in all the statistical models. Age was grouped into 10-year age bands (with the exception of the youngest and oldest age groups) to take account of any non-linear associations with allostatic load. Ethnicity was grouped into ‘White British’ or ‘non-White British’ groups (most ethnic minority groups had small numbers). Marital and cohabiting status was grouped into never married, married or cohabiting or widowed/divorced/separated. Education was measured by the highest qualification attained (degree, other higher degree, A-level or equivalent, GCSE or equivalent, other qualification and no qualifications). Occupational class was measured by the five class version of the National Statistics Socio-Economic Classification (which reduced to four groups as there were no self-employed in the analyses). Household net income was grouped into quintiles in order to obtain similar proportions of people in each group. It is particularly important to distinguish between employees’ work hours and the use of reduced hours flexible working arrangements. While they are correlated (as part-time work is one of the reduced hours working arrangements), the question about flexible working arrangements was prefaced by employee choice, whereas work hours may be imposed by the employer. Hence in all the analyses, work hours in their main job are controlled for.
For RQ1, we additionally analysed the role of industry sector (primary and manufacturing vs service sector), private vs non-private business types and the number of employees (less than 25, 25–99 and 100 or more). For RQ2–4, in addition to controlling for socio-demographic, socio-economic and workplace factors, we also controlled for a range of health and behavioural factors that could affect allostatic load. These included longstanding illness or disability, medication use, physical activity (walking at least 10 minutes a day and moderate sports activity) and smoking status. We wanted to be conservative in our estimates of the association between flexible working arrangements and allostatic load and control for as wide a range of health and behavioural factors to reduce the possibility that any association between flexible working arrangements and allostatic load is confounded by health and behavioural factors.
Statistical Models
All the analyses were stratified by gender (or include gender as an interaction term) as working conditions and family responsibilities tend to be different for men and women. For RQ1, the three flexible work arrangements categorical variables were regressed on socio-demographic and socio-economic factors using multinomial logit models. For RQ2–4, allostatic load was regressed on flexible work arrangements and other work and family factors. As allostatic load is a count of biomarker risk indicators, negative binomial regression models were used to estimate the association with flexible work arrangements and work–family stressors after controlling for covariates. All the regression models used the longitudinal blood survey weights produced by the UKHLS team to make the analyses representative of the UK adult population. These survey weights explicitly take into account different factors resulting in missing UKHLS biomarker data for the nurse visit and blood sample outcomes (see Supplementary File for more details on handling missing data). Survey weighted model estimates assume that the data are missing at random. Additionally, we took account of the clustering of the individuals within primary sampling units and stratified sampling procedures.
Results
The distribution of the different types of flexible working arrangements by allostatic load and key socio-demographic variables is shown in Table 1 (further details are shown in Supplementary Tables S2–S4). Unsurprisingly, more women than men made use of reduced hours flexible working arrangements. Mean allostatic load was higher among women who did not have any form of flexible work available. Among men, mean allostatic load was highest among men without access to reduced hours or variables hours flexible work, and also among men who used such work arrangements. Men who used reduced hours arrangements were on average at least 2.5 years older than men who did not have access to such arrangements. Among women, the age differences were not so marked. There were over twice as many women caring for two or more children (aged under 15) who used reduced hours arrangements than women who also cared for two or more children but did not have access to reduced hours arrangements. Almost no men were the main responsible adult for the care of two or more children. The use of reduced hours flexible working arrangements was much more common among those in the poorest income groups or those working in semi/semi-routine occupations, especially among men. In contrast, other flexible working arrangements (which included working from home) were more common among men and women in the most advantaged socio-economic groups.
Distribution of flexible work arrangements by gender.
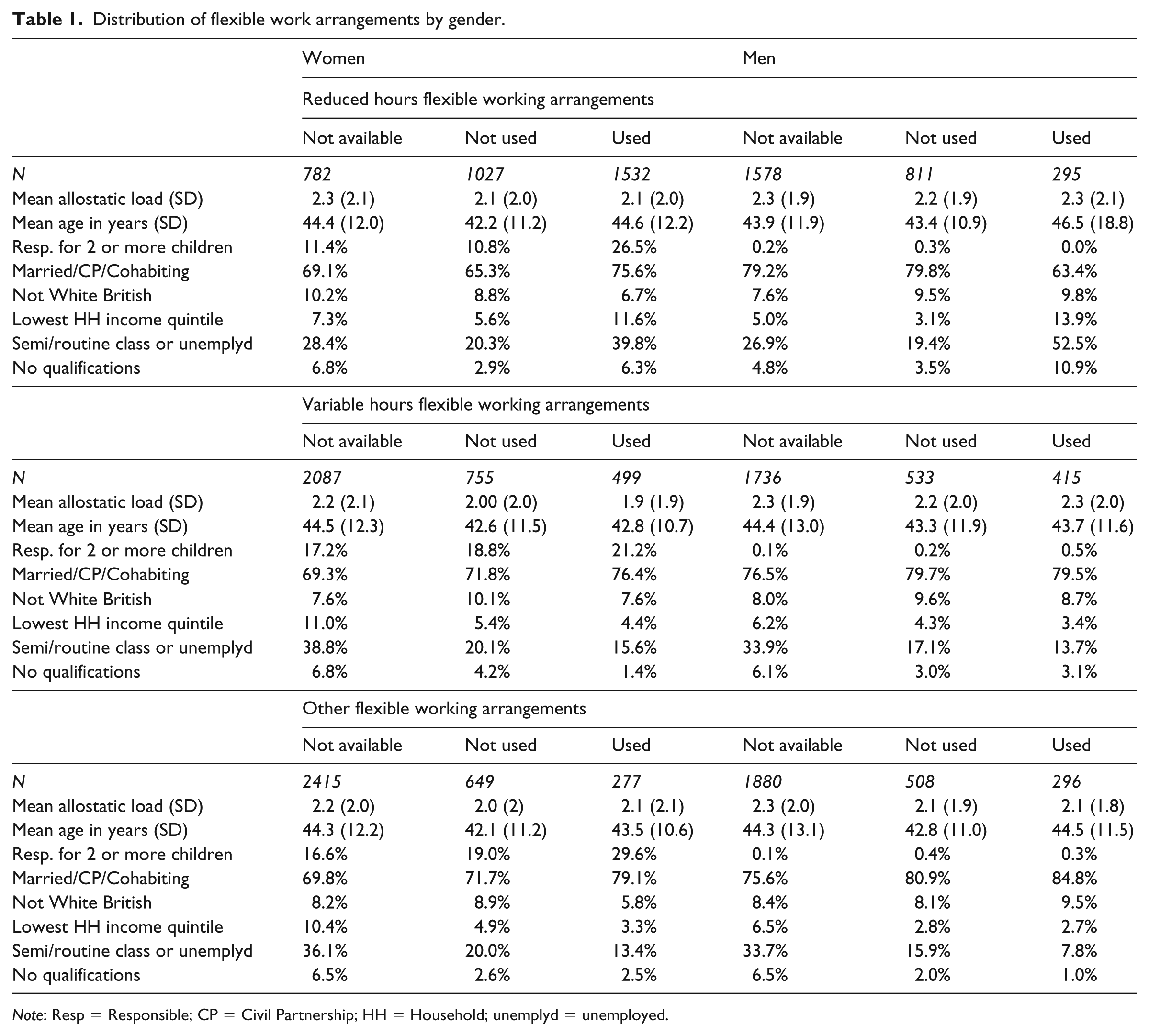
Note: Resp = Responsible; CP = Civil Partnership; HH = Household; unemplyd = unemployed.
RQ1 is examined in Table 2 which shows the relative risks (95% CI) of selected coefficients from the multinomial logit models predicting different types of flexible working arrangements (full model coefficients are in Supplementary Tables S5–S7). Both older men and women (aged 60+) tended to work in jobs where they made use of reduced hours arrangements – men aged 60+ were about three times more likely and women aged 60+ were twice more likely to use reduced hours arrangements compared to men and women aged under 30. Women who were responsible for the care of children under the age of 15 were four times more likely to make use of reduced hours arrangements compared to women who were not responsible for the care of children under 15. Professional men and women were least likely to make use of reduced hours arrangements compared with other occupational groups. Men and women working in large organisations employing over 100 employees tended to work in jobs where reduced hours arrangements were available.
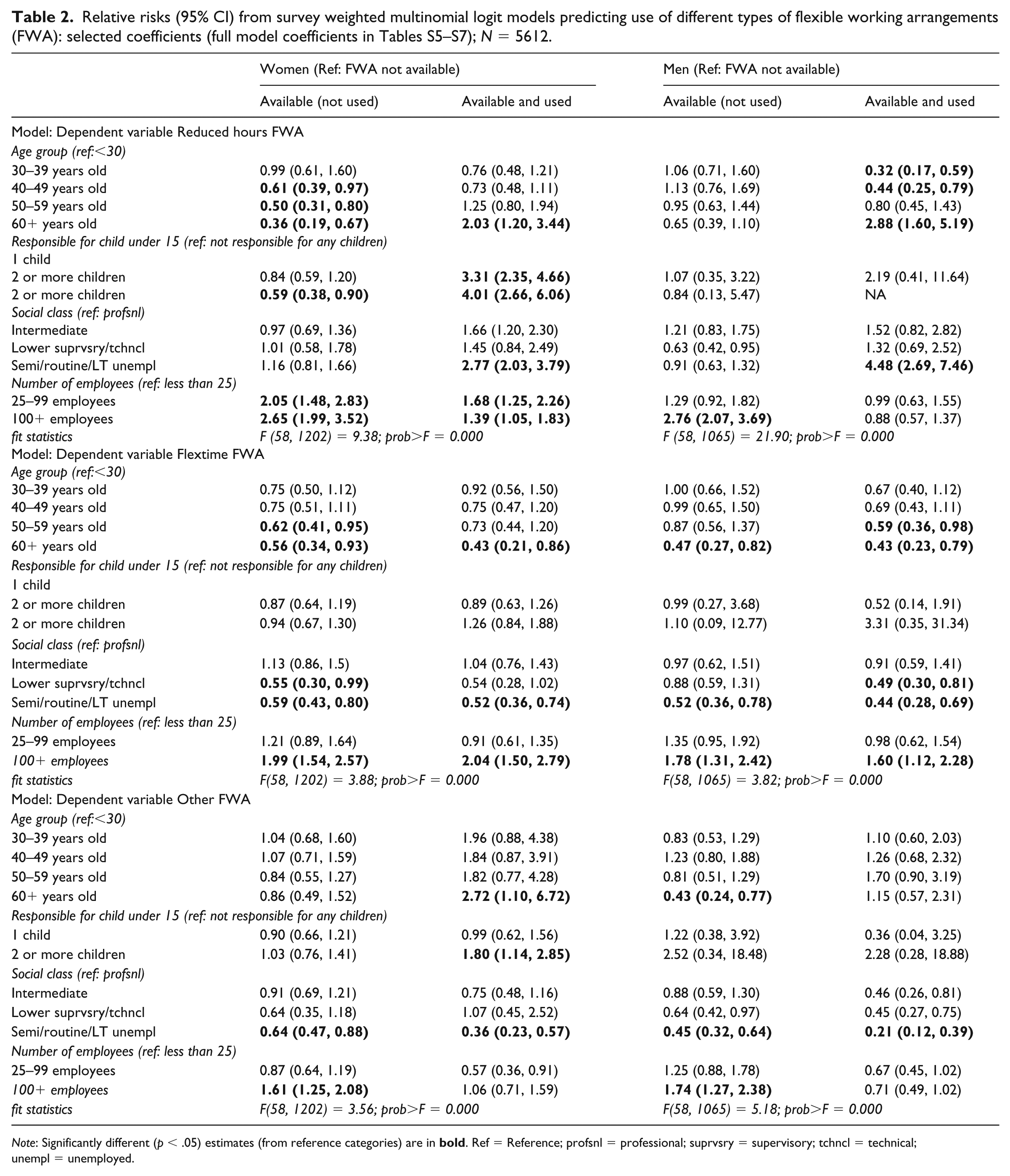
Note: Significantly different (p < .05) estimates (from reference categories) are in
For flextime working arrangements, older men and women were least likely to make use of such arrangements compared to younger workers. Furthermore, men and women working in semi-routine and routine jobs were also least likely to make use of flextime arrangements. Those working in service sector jobs and in large organisations were more likely to make use of flextime arrangements. For other flexible working arrangements, professional men and women were most likely to use such arrangements (which include working from home). Men and women with degree-level qualifications were most likely to be working in jobs with any flexible working arrangements and also to make use of such arrangements (see Tables S5–S7).
RQ2 is examined in Table 3 which shows the predicted allostatic load index by different types of flexible working arrangements. All the models controlled for age group, number of children, work hours, marital status, ethnicity, education, household net income, social class, duration in the job, smoking status, longstanding illness, physical activity and number of medications (see Table S8). When analysing both men and women together, only the use of reduced hours arrangements was significantly associated with lower allostatic load. Men and women who made use of reduced hours arrangements had around a 0.2–0.3 lower predicted allostatic load index than those who did not have such arrangements or did not use such flexible working arrangements. Just working in a job where such reduced hours arrangements were available was not associated with lower levels of allostatic load. There was no evidence that flextime working arrangements or other flexible working arrangements were associated with lower allostatic load. There was a significant interaction between flextime working arrangements and gender, but no such interaction for the other forms of flexible working arrangements. In the gender stratified analyses (not shown), there was some suggestion that the use of flextime working arrangements was associated with higher levels of allostatic load among men, but this was not statistically significant at the 5% level. Turning to the other predictors of allostatic load (Table S8), men and women with poorer health (longstanding illness or disability, or used more prescribed medications), with poorer health-related behaviours (current smokers or did less physical activity) and from more disadvantaged socio-economic backgrounds (lower household income, fewer qualifications or from ethnic minority groups) had higher levels of allostatic load.
Predicted allostatic load index from survey weighted negative binomial regression models controlling for covariates, by flexible working arrangements (FWA): UKHLS female and male employees (N = 5546).
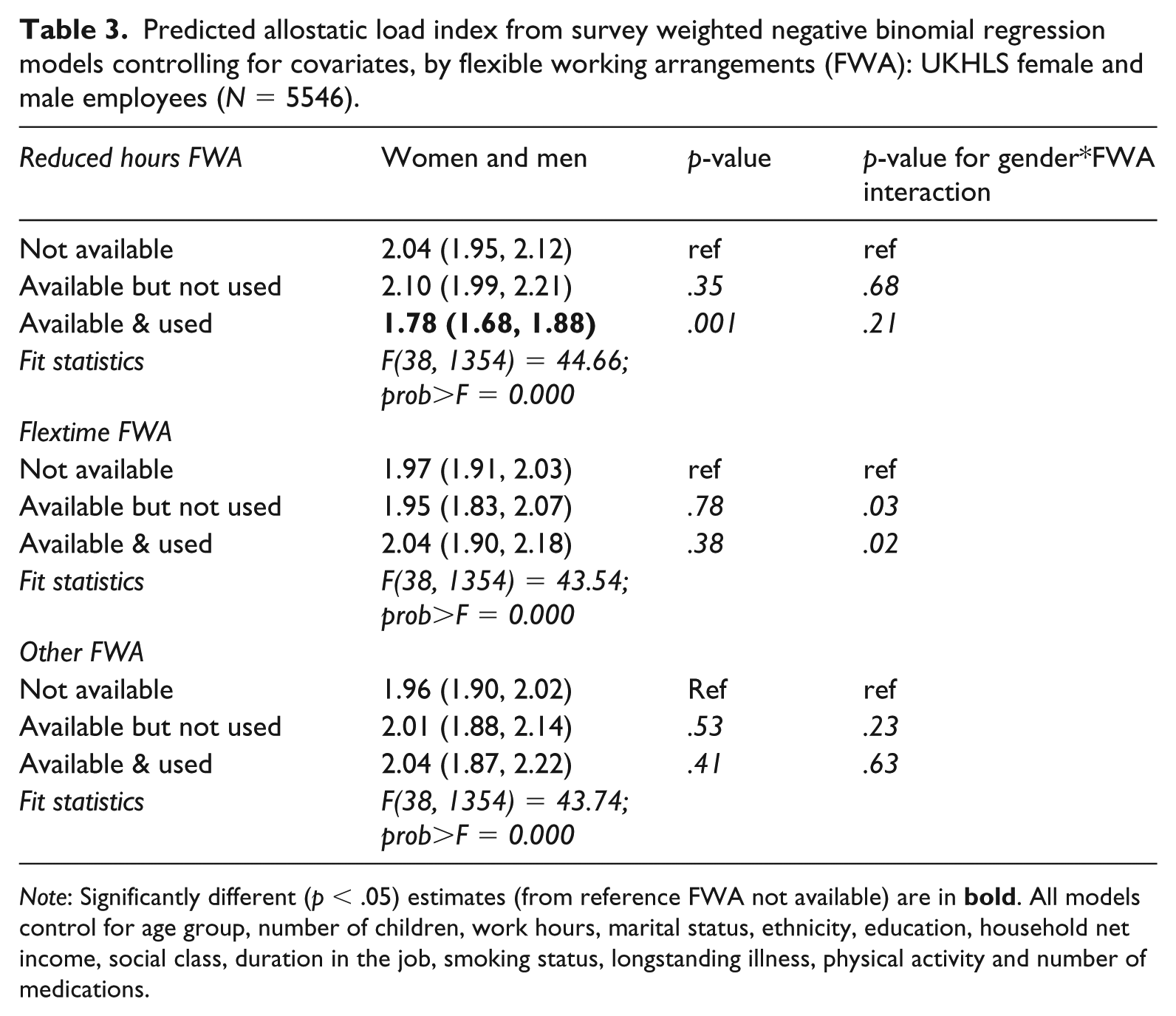
Note: Significantly different (p < .05) estimates (from reference FWA not available) are in
RQ3 is examined in Table 4 (full model coefficients in Table S9). The sample was restricted to women as very few men were the main responsible adult for childcare. There was a statistically significant interaction between working hours and childcare responsibility, and the predicted levels of allostatic load are displayed in Figure 1. This shows a clear pattern of increasing allostatic load among women who work 37 hours+ a week with greater childcare responsibilities. There was a difference of almost 0.8 units of the allostatic load index between women with no childcare responsibilities who worked 37 hours+/week and women caring for two or more children who worked 37 hours+/week. In contrast, there was no difference in the predicted levels of allostatic load among women who work less than 25 hours a week by their childcare responsibilities. This suggests that the combination of work and family stressors in terms of longer working hours and greater childcare responsibilities was associated with higher levels of chronic stress-related biomarkers.
Survey weighted negative binomial regression coefficients (95% CI) of allostatic load – UKHLS female employees (N = 3037); selected coefficients (full model in Table S9).
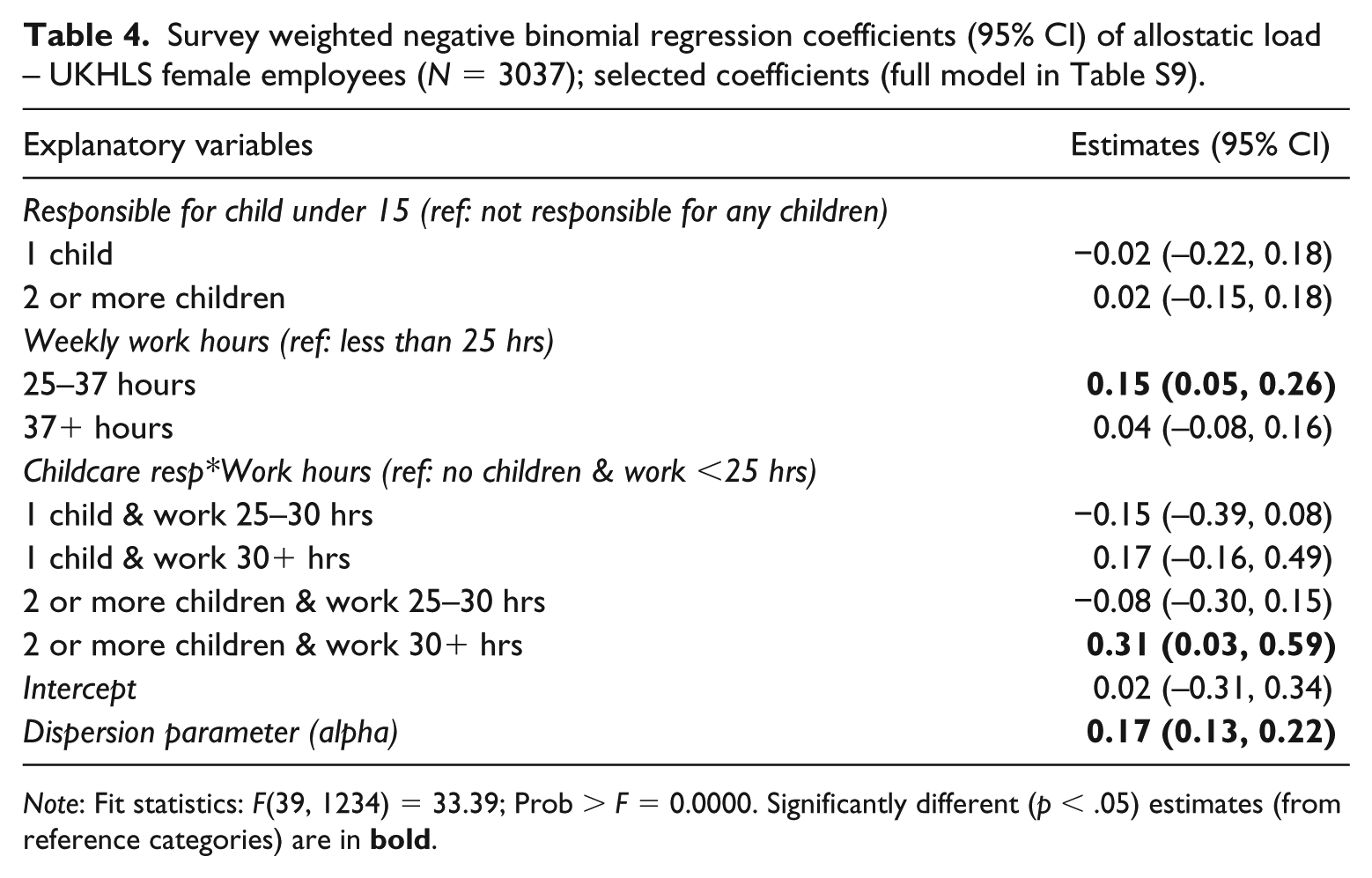
Note: Fit statistics: F(39, 1234) = 33.39; Prob > F = 0.0000. Significantly different (p < .05) estimates (from reference categories) are in
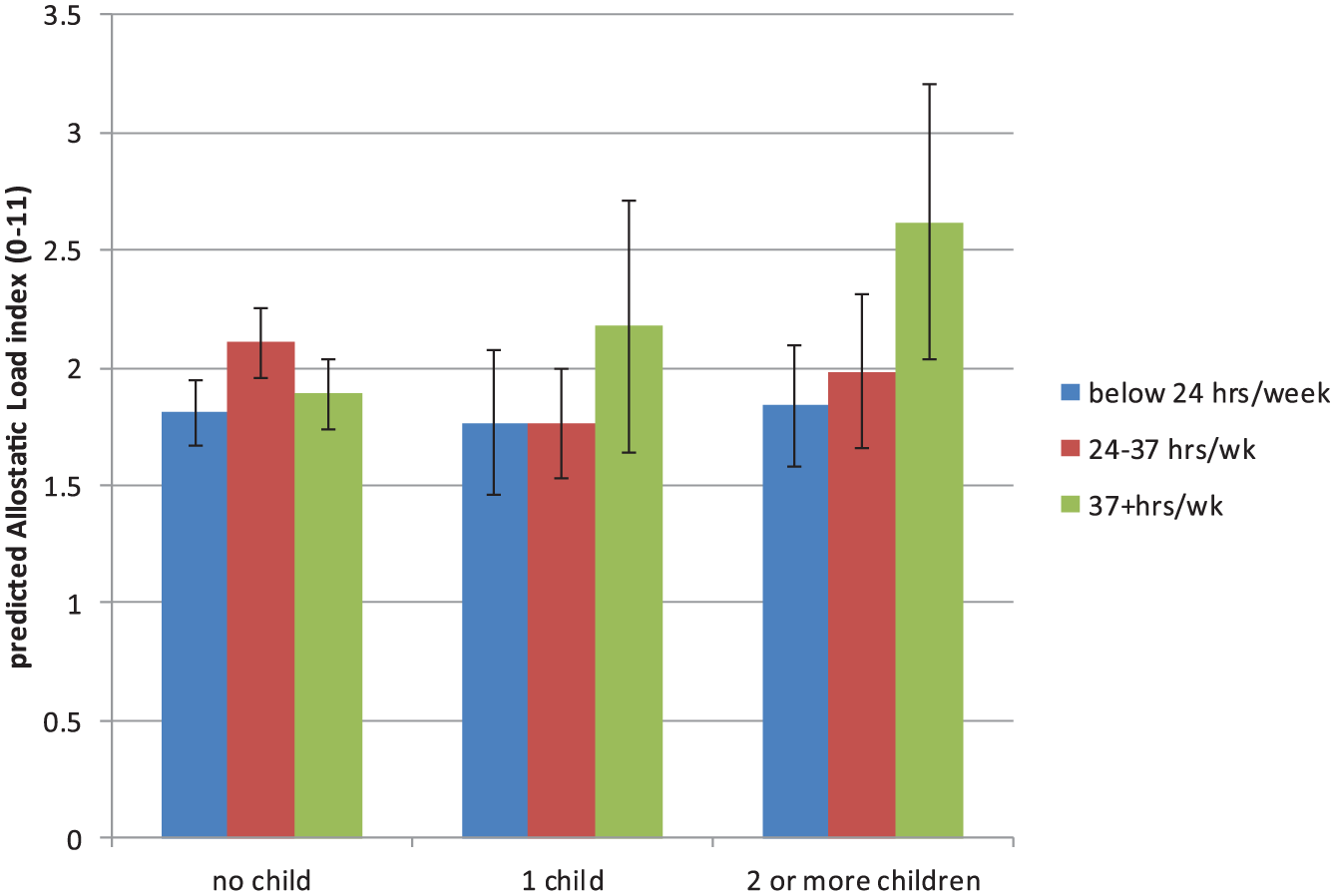
Predicted allostatic load index (and 95% CI) by weekly working hours and childcare responsibilities among women employees; estimated from Table 4.
RQ4 is examined in Table 5 (full model coefficients in Table S10). The sample was restricted to women working 25 hours/week or more as there was no association between greater childcare responsibilities and allostatic load among women working fewer hours a week. Furthermore, only reduced hours flexible work was examined as the other types of flexible work were not associated with allostatic load. The interaction between childcare responsibilities and reduced hours work was statistically significant and the predicted levels of allostatic load from this interaction are displayed in Figure 2. The figure shows that women who looked after one or more children and made use of reduced hours arrangements had lower levels of allostatic load than women who also looked after children and did not have access to such flexible working arrangements. There was a difference of almost one unit of the allostatic load index between women who made use of reduced hours flexible work and those without such arrangements, among women responsible for two children. Thus, among women who were exposed to the combination of work (longer working hours) and family stressors (childcare responsibilities), the use of reduced hours work arrangements appeared to reduce the association between the family stressor (childcare responsibilities) and allostatic load.
Survey weighted negative binomial regression coefficients (95% CI) of allostatic load – UKHLS female employees working 25+ hours a week (N = 2025); selected coefficients (full model in Table S10).
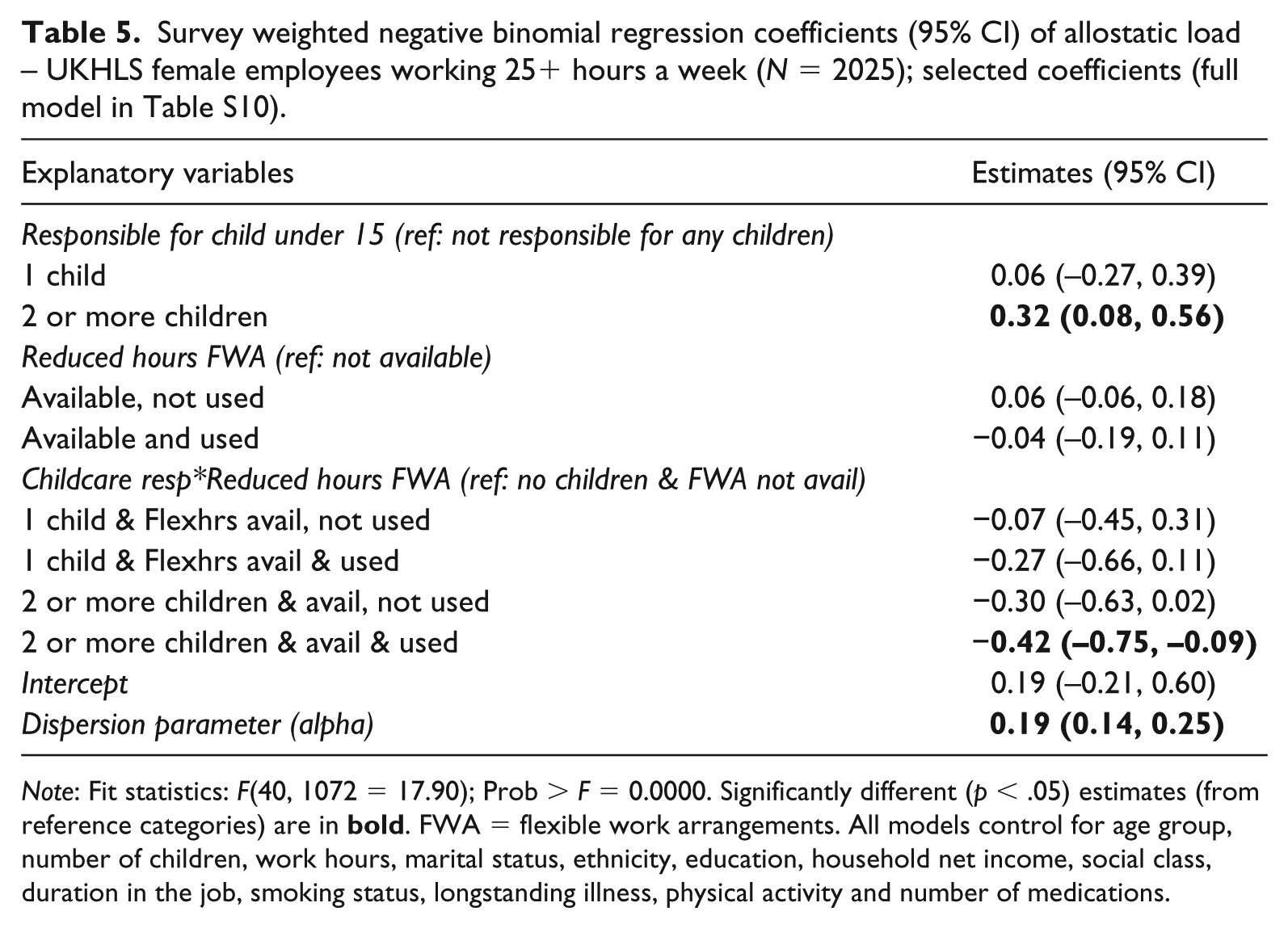
Note: Fit statistics: F(40, 1072 = 17.90); Prob > F = 0.0000. Significantly different (p < .05) estimates (from reference categories) are in
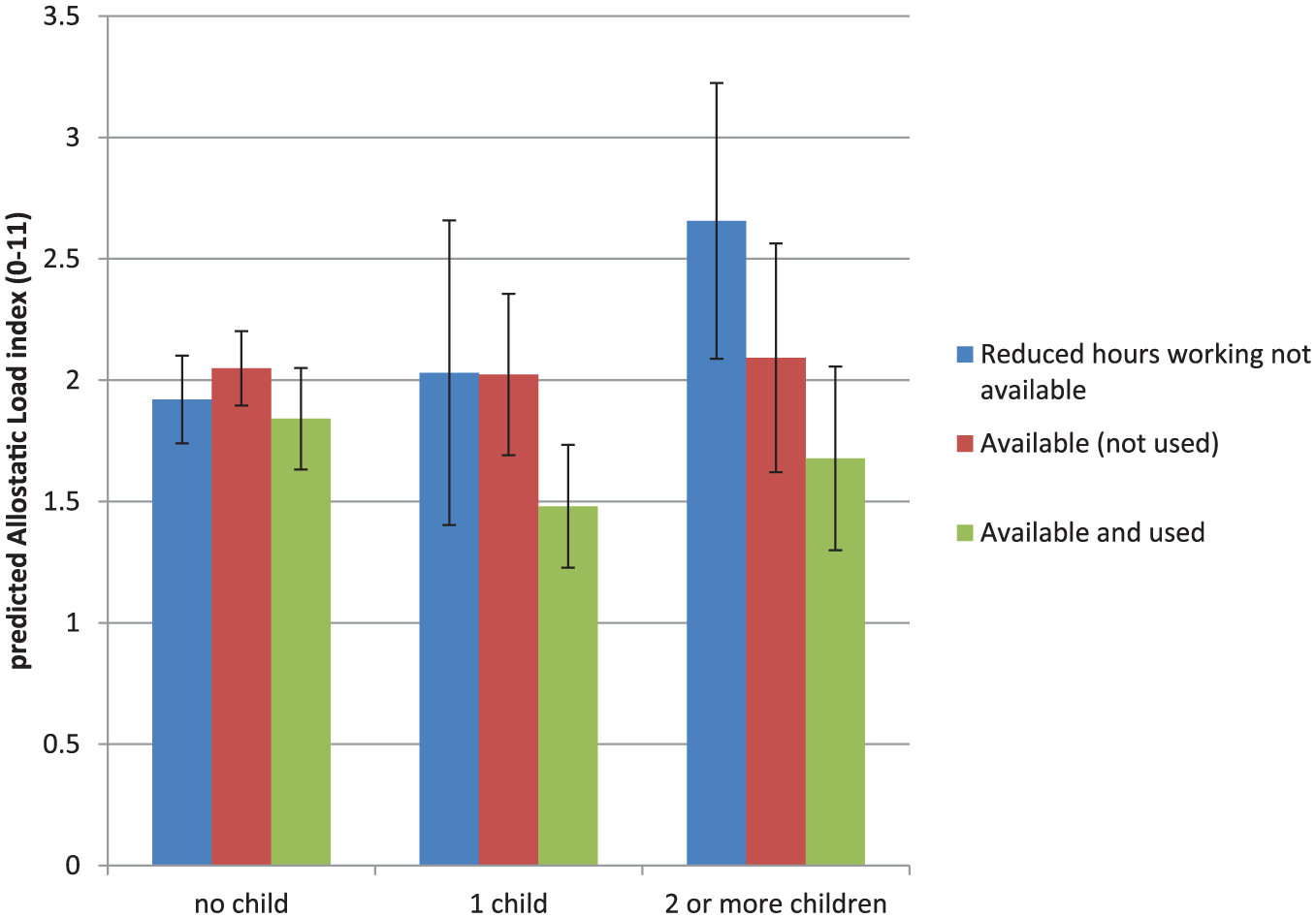
Predicted allostatic load index (and 95% CI) by reduced hours flexible working arrangements and childcare responsibilities among women who work more than 24 hours a week; estimated from Table 5.
We carried out a number of sensitivity analyses. We restricted the sample of women analysed in Table 5 just to women aged under 60 years and obtained very similar results. We explored reasons for missing biomarker data in the ‘Missing Data Analysis’ section in the Supplementary File and explored whether we obtained different estimates using different approaches to handling missing data. While similar patterns of associations between reduced hours flexible work and allostatic load were obtained from the complete case, survey weighted and multiple imputation models, the estimates derived from the survey weighted analysis and the multiple imputation model with survey weights were considerably larger (in absolute size) than those derived from the complete case or multiple imputation without survey weights.
Discussion
Reduced hours flexible arrangements may be beneficial for employees’ levels of chronic stress. One of the limitations of a causal interpretation of this association is potential confounding by socio-economic factors, especially if more socio-economically advantaged workers are offered and make use of flexible work. However, the selection of workers into reduced hours flexible work was actually in the opposite direction. Contrary to our hypothesised association for RQ1, reduced hours flexible work was more common among socio-economically disadvantaged groups. In contrast, flextime, flexplace and informal arrangements were more common among more privileged social classes (which was in line with our hypothesis).
In relation to RQ2, we showed that UK employees who used reduced hours flexible arrangements had lower allostatic load than their peers for whom either such arrangements were not available or who did not use such flexible arrangements. This association remained statistically significant after controlling for a number of potential confounders (such as partnership and health status, ethnicity and socio-economic factors) and potential mediators (such as health behaviours like smoking and physical activity). The estimates from the models with and without the controls for potential mediators hardly changed, suggesting that there may be a direct effect of inflexible working hours on biological stress reactions that are not mediated through behavioural responses. The analysis of RQ3 showed that longer working hours (37 hours+/week) were associated with higher levels of allostatic load among women with greater childcare responsibilities. Our analysis of RQ4 showed how the use of such reduced hours arrangements appeared to moderate some of the association of family and work stressors with allostatic load. Among women responsible for the care of two or more children, there was a difference of almost one unit in the index (or an additional biomarker risk factor) between women with and without reduced hours working arrangements.
In our study, there was little evidence that flexplace or flextime working arrangements were associated with lower chronic stress responses. The suggestion that flexible working arrangements may not have any real effect on women’s well-being (Lewis et al., 2007) did not hold. Both women and men who made use of reduced hours arrangements had lower levels of allostatic load. This was not just a reflection of gender norms where women are more likely to work in part-time reduced hours jobs. First, we controlled for job hours in the analyses. Furthermore, in separate analyses, we analysed women working in jobs where their weekly working hours were 30 hours or more. Even in this group of women working longer weekly working hours, it was clear that reduced hours arrangements were associated with lower allostatic load.
These results confirm the expected associations arising out of role strain and work–family conflict theories, but go further by locating it within a broader sociological framework of work and well-being. Given the increasing availability of biomarkers related to stress and well-being in studies, we could be seeing greater amounts of sociological research that incorporates such biomarkers. However, there are considerable limitations in the use of such biomarkers. The operationalisation of allostatic load has been criticised (Johnson et al., 2017). There are a number of ways of constructing the index. In this study, we used the original method of constructing the index which sums up a number of risk biomarkers across a range of biological systems, with cut-off points for the risk categories determined by the distribution of the biomarkers within the sample. We did not use clinical risk categories for the biomarkers partly because not all the biomarkers have established clinical risk categories, and also because these clinical categories are not very relevant for younger populations. Another key criticism is that many allostatic load studies do not include neuroendocrine biomarkers, which is particularly worrying given that allostatic load is meant to reflect cumulative physiological dysfunction as a result of chronic stress. While the UKHLS does not have any measures of stress hormones, our measure of allostatic load includes measures of hormones related to neuroendocrine system. Another limitation of the use of biomarker data in surveys is the high proportion of missing biomarker data. As shown in Supplementary File S, allostatic load could be measured in only around 36% of employees in wave 2 of UKHLS. Our analyses of different approaches to handling missing biomarker data suggests that complete case estimates that ignore the pattern of missingness may be biased.
The main limitation of the study was that the biomarker data were only observed once, which meant we could not examine changes in allostatic load. Hence, it is hard to infer whether flexible working arrangements or other work and family stressors had a causal effect on allostatic load, because some other factors may have caused the reported associations. However, we did control for a wide range of factors, including demographic, socio-economic, job characteristics and health conditions. Baseline health was unlikely to be a confounder of the association between reduced hours flexible work and allostatic load. First, we controlled for a range of health measures and related health behaviours. Second, we distinguished between groups of employees for whom flexible arrangements were available but were not used. There could be a selection process of workers into jobs where flexible work is available. However, workers who used reduced hours flexible work had lower allostatic load than workers for whom such arrangements were available but were not used. Selection processes out of the labour market may also operate, with workers with childcare responsibilities who cannot work flexibly being selected out of the analysed sample. This selection process would have resulted in an underestimate of the association between reduced hours flexible work and allostatic load as the more stressed workers are more likely to leave work.
The study addresses some important limitations in the existing literature on flexible working arrangements and employee health by analysing the different types of arrangements, distinguishing between their use and availability by different socio-economic and demographic groups, separating out the stress response from work and family stressors, and analysing chronic stress-related biomarkers. Stress and the physiological response are one of the key concepts that link the social environment to biology. The use of biological data in social science research could be helpful in highlighting processes and mechanisms linking the social environment to well-being.
Supplemental Material
Supplementary_Tables_and_Figures – Supplemental material for Are Flexible Work Arrangements Associated with Lower Levels of Chronic Stress-Related Biomarkers? A Study of 6025 Employees in the UK Household Longitudinal Study
Supplemental material, Supplementary_Tables_and_Figures for Are Flexible Work Arrangements Associated with Lower Levels of Chronic Stress-Related Biomarkers? A Study of 6025 Employees in the UK Household Longitudinal Study by Tarani Chandola, Cara L Booker, Meena Kumari and Michaela Benzeval in Sociology
Footnotes
Acknowledgements
Understanding Society is an initiative funded by the Economic and Social Research Council and various government departments, with scientific leadership by the Institute for Social and Economic Research, University of Essex, and survey delivery by NatCen Social Research and Kantar Public. The research data are distributed by the UK Data Service.
Editor Note
This article was submitted by the author, Tarani Chandola, who is currently an editor of Sociology. The article followed the process as detailed in the BSA Terms of Reference. The article was edited by the Chair of the Board. The article underwent the journal’s usual peer review process with a minimum of two peer reviewers. During the process the author had no access to information regarding the article beyond that available to all authors.
Funding
This work was supported by the Economic and Social Research Council (ESRC ES/J019119/1, ES/M008592/1, ES/L008351/1).
Supplemental material
Supplemental material for this article is available online.
![]() ). Tarani’s research is primarily on the social determinants of health, focusing on health inequalities and psychosocial factors, and the analysis of longitudinal cohort studies. Much of his research is on stress at work, and its effects on health and related biomarkers.
). Tarani’s research is primarily on the social determinants of health, focusing on health inequalities and psychosocial factors, and the analysis of longitudinal cohort studies. Much of his research is on stress at work, and its effects on health and related biomarkers.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.