
Abstract
A longstanding sociological tradition of stigma research has highlighted its salience and consequences, both for children with disabilities and their parents. Yet, while it is recognised that forms of stigma are embedded in structural conditions and social context, understanding of how disability-related stigma plays out is overwhelmingly restricted to high-income countries. This is despite the fact that the prevalence of child disability is higher, and the associated economic and social challenges more severe in low- and middle-income countries (LMICs). This article advances sociological understanding of disability-related stigma and its consequences through thematic analysis of interviews with 22 mothers of children with disabilities in Nigeria. We analyse how their experience is embedded in the structural features of their society, an LMIC marked by high inequality, constrained state schooling, and an absence of disability support. We show how these conditions help perpetuate forms of felt stigma rooted in dominant cultural understandings of disability that serve to isolate mothers, and forms of enacted stigma typified by children’s educational and social exclusion. We further explore how mothers negotiate these attitudes and behaviours. Our findings show both concordance with and difference from existing sociological studies of disability-related stigma, demonstrating the relevance of attending to salient but under-researched settings.
Introduction
Disability is a key form of social stratification affecting 15% of the global population. Around 10–11% of children are disabled, with over half of them located in South Asia and sub-Saharan Africa (Olusanya et al., 2022; World Bank Group, 2011). Disability is associated with socio-economic disadvantage, lower educational attainment and increased poverty risks for both children and adults (Jones, 2021; Mitra et al., 2013; Mizunoya & Mitra, 2013; Spencer et al., 2015). These disadvantages are both shaped and compounded by stigma, discrimination and social isolation, which impact not only the well-being of children but also their future life chances (Chatzitheochari & Butler-Rees, 2023; Green et al., 2005; Haft et al., 2022; Stone-MacDonald, 2012; Thomas, 2021).
A longstanding sociological tradition of stigma research has highlighted its salience and consequential impact, both for children with disabilities and their parents. However, while it is recognised that stigma is embedded in structural conditions and social context (Scambler, 2018; Tyler, 2020), analysis of the relevance of different social-institutional contexts has been constrained by the limited range of countries studied. In particular, we have little understanding of how stigma plays out in low- and middle-income countries (LMICs).
This article contributes to the literature by extending understanding of the forms disability-related stigma takes to one LMIC, Nigeria, elucidating how they differ from or are similar to those in high-income countries, and how they are embedded in specific cultural and institutional features. West and Central Africa have the highest estimated child disability rates globally (15%) (United Nations Children’s Fund [UNICEF], 2021). In Nigeria, Africa’s most populous country, barriers to inclusion include stigma, misconceptions about disability, poverty and poor access to education (World Bank Group, 2020). Although Nigeria ratified the UN Convention on the Rights of Persons with Disabilities in 2007 and passed national anti-discrimination legislation in 2018, structural support remains weak. Despite this, academic research on childhood disability in Nigeria is scant, and little is known about how families experience and navigate these challenges.
Our study situates the accounts of 22 mothers of children with disabilities within the sociology of disability-related stigma and family life. We show that the Nigerian tendency to interpret disability in terms of spiritual causes (Ishola-Esan, 2016) strongly patterns the stigmatisation of mothers and children. Mothers are subject particularly to felt stigma, which merges shame and blame (Scambler, 2004), resulting in isolation compounded by economic strain. Such cultural scripts lead to an individualisation of responsibility, which aligns with the absence of institutional support. Children are subject more to enacted stigma, or discrimination, which limits their opportunities for education and participation.
While the individualised understanding of disability in a setting of inequality reflects certain emphases in studies of high-income countries (e.g. Scambler, 2018), the narratives within which these responses are embedded differ. Similarly, while the social ostracisation of children echoes findings on enacted stigma in high-income countries (e.g. Chatzitheochari et al., 2016), here it takes place in a context of widespread educational exclusion, rather than in the school setting. Our contribution to understanding disability-related stigma extends to how mothers negotiate it, where we see both similarities (such as recourse to biological explanations) and differences (such as reliance on spiritual interpretations) to features highlighted in sociological studies from high-income countries.
Background
Disability has both economic and social consequences for individuals and their families. These can interact, as economic precarity reduces the ability to deflect or challenge stigma, and social judgements on disability make it harder for parents to retain productive employment or children to sustain educational careers (Grech et al., 2023). In countries where disability support is minimal, economic context and existing power relations may reinforce stigmatisation (Eide & Ingstad, 2011). Yet, despite studies from both the perspective of children and their parents on the experience of disability (e.g. Blum, 2015; Green et al., 2005; Manago et al., 2017; Thomas, 2021), few sociological studies provide insight into how disability is experienced in LMICs, and whether the stigma related to mothering a child with disability interacts with these distinct contexts to reveal different manifestations.
Stigma and disability
Stigma remains a key sociological concept since Goffman’s (1963) influential work, which described stigma as something that marks individuals when they have ‘an attribute that is deeply discrediting’ (p. 3), and that evokes negative stereotypes. Stigma arises, he emphasises, relationally; and he draws attention to the importance of understanding its ‘structural preconditions’ (p. 1).
Goffman’s insights remain critical to our understanding of disability-related stigma, including that experienced by parents of disabled children. Such stigma applied to affiliated others Goffman termed ‘courtesy stigma’; and the exploration of courtesy stigma, including how parents resist and respond to it, has constituted an important strand of research on disability (e.g. Farrugia, 2009; Gray, 2002; Green et al., 2005; Manago et al., 2017; Thomas, 2021, 2024). According to Goffman, responses to stigma can include avoidance of social situations but also reformulating the stigmatised condition as a ‘blessing-in-disguise’. Both responses have been identified in literature exploring parenting of children with disabilities (e.g. Green, 2003; Thomas, 2024).
Critics of Goffman’s conceptualisation of stigma have argued, however, that its singularity and its breadth of potential applications reduce conceptual precision (Green et al., 2005). They also suggest that the focus on the ‘discredited’ risks locating the sources of stigma in impairment (and hence the disabled individual), rather than in the relationships within which it is expressed. It may tend to individualise the experience of stigma, neglecting a properly ‘sociological’ understanding of stigma which attends to the structural conditions creating it (Scambler, 2004, 2018; Tyler, 2020). Link and Phelan (1999) aimed to recover both a more specific and a more sociological conceptualisation. They identified the component elements of stigma as ‘labeling, stereotyping, separation, status loss, and discrimination’ (Link & Phelan, 2001, p. 363), while also emphasising the exercise of power as critical to its operation. The centrality of power for our understanding of stigma has also been stressed by Tyler (2020) and Thomas (2021). Thomas (2021) argues that stigma must be recognised as part of the social structures and power relations which engender institutional forms of hostility towards disability; while interpersonal expressions of stigma can demonstrate socio-cultural scripts that locate disability within a particular worldview.
For Link and Phelan (2001), potentially neutral acts such as ‘labelling’ can lead to social and material consequences for those stigmatised by the association of such labels with specific ‘stereotypes’. Separation, then, involves treating those with a particular label as part of a group and distinguishing them, while this in turn leads to status loss and results in discrimination at the individual and institutional level. These processes can be mapped through analysis of the experience of disability.
However, as they recognised, missing from this account were the emotional reactions of both stigmatiser and stigmatised, particularly shame (Link & Phelan, 2014). Shame is an emotion central to our understanding of the manifestation of and implicit violence associated with stigma (Tyler, 2020). While much contemporary discussion focuses on symbolic more than physical violence, this can downplay acts of actual violence accompanying stigmatisation (Meekosha & Soldatic, 2011). Sense of shame and risks of violence or exclusion align with the now regularly adopted distinction between felt and enacted stigma (Scambler & Hopkins, 1986; see also Scambler, 2004). Felt and enacted stigma impact both disabled individuals and, associatively, parents of disabled children for their implied responsibility for the disability (Manago et al., 2017). For Green et al.’s (2005) respondents, the ‘felt’ aspects were, however, most damaging: acts of discrimination could be called out or resisted; but internalisation and self-seclusion could set in train a vicious cycle.
One form of resistance to stigma is an emphasis on the biological (Thomas, 2024). Manago et al. (2017) discuss how medicalisation can be utilised by parents to both challenge and deflect stigma; and Farrugia (2009) points to its specific utility in deflecting stigma for parents of children with autism. The recourse to medical understandings of disability/impairment has been highlighted by Meekosha and Soldatic (2011) as particularly salient for disempowered or poor communities. They describe how marginalised mothers make claims on the basis of their children’s medical conditions, which helps them negotiate for resources. They argue that the distinction between disability and impairment that dominates the disability rights movement in the Global North may downplay the empowering potential for families in the Global South to be able to identify, and medicalise, impairments.
The interconnection between socio-economic position and stigma is a recurrent theme in the literature. But while greater socio-economic resources are found to offer some protection in the face of enacted stigma, several studies demonstrate how experiences of mothering, both negative and positive, crosscut socio-economic position (Blum, 2015; Green, 2003). The devaluation associated with stigma can impact economic well-being, creating economic pressures compounded by the additional costs typically associated with disability (Mitra et al., 2017); but this may prove less the case in environments which are already very poor (Chataika & McKenzie, 2013).
The importance of the voices of stigmatised individuals being heard to avoid misrepresenting their experience and further stigmatising them has been often stressed (Green, 2003; Thomas, 2024; Tyler, 2020). Existing empirical literature on stigma and child disability has paid attention to the voices both of parents (e.g. Blum, 2015; Thomas, 2021) and of children themselves (e.g. Chatzitheochari & Butler-Rees, 2023; McLaughlin, 2017). These include studies focused on those with specific conditions, for example Thomas’s (2021) study of parents of children with Down’s Syndrome or Gray’s (2002) research with parents of children with high-functioning autism; or where heterogeneity is part of the analysis of interest, such as Chatzitheochari and Butler-Rees’s (2023) study showing how disability-related stigma was moderated both by social class background and the nature of the impairment.
These central issues in understanding stigma and disability: the role of power and its institutional expression; the way labelling invokes stereotypes; the experience of shame and its relationship to material and symbolic violence; the relative impact of felt and enacted stigma on both those with disabilities and their parents, and the forms of response they invoke; the interaction between socio-economic circumstances and (defences against) stigma; and issues of voice and heterogeneity are all topics that have been investigated in relation to children with disabilities in high-income countries, particularly the US (Thomas, 2024). Yet we know little about whether the findings generalise to LMICs.
While stigma is viewed globally as part of the disabling environment that limits opportunities (UNICEF, 2021; World Bank Group, 2011), its expression varies cross-nationally (World Bank Group, 2020). Since stigma is shaped by social belief systems and cultural dynamics, economic environments and institutional structures, it merits investigation in contexts in which those features differ from the high-income Western countries whence most of our knowledge derives.
Disability and stigma in LMICs and the case of Nigeria
The limited research on the experience of disability in LMICs is particularly acute for Nigeria. Yet, this, the most populous country in Africa, situated in the region with the highest estimated rates of child disability (15%) (UNICEF, 2021), demonstrates distinctive institutional, cultural and organisational features that would be expected to shape the experience of disability-related stigma. Rich in resources and showing growth in per capita GDP and life expectancy over the past two decades, Nigeria remains marked by substantial inequalities (Mayah et al., 2017; Smith, 2024).
Poverty and disability are associated across the world (Eide & Ingstad, 2011); and poorer countries tend to have higher rates of disability (UNICEF, 2021). Nutritional insults, environmental dangers and uneven and costly out-of-pocket healthcare all contribute to higher rates of child disability. Some conditions that are rare in rich countries are more prevalent in LMICs: for example, cerebral palsy is twice as common in LMICs as in rich countries (McIntyre et al., 2022). Disability also increases poverty risks through reduced labour supply or extra costs (Mitra et al., 2017), or both. However, disability poverty gaps within LMICs (Mitra et al., 2013) tend to be greater in middle-income than in low-income countries (Banks et al., 2017; Pinilla-Roncancio & Alkire, 2021).
Stigma plays a critical role in legitimising ideological and institutional arrangements that reinforce the perceived unworthiness of certain groups for state support (McLaughlin, 2017; Scambler, 2018), deepening their poverty, marginalisation and capacity to resist or make claims (Tyler, 2020). This entanglement of stigma and economic structures is especially acute in contexts like Nigeria, where education and healthcare are largely privatised (Smith, 2024); and where, despite being a 2007 signatory to the UN Convention on the Rights of Persons with Disabilities and having introduced national anti-discrimination legislation in 2018, there is an absence of disability-related social protection.
In high-income countries, educational systems label and segregate children with special needs, producing structural inequalities (Powell, 2003; Tomlinson, 2017). In LMICs, however, inequalities faced by children with disabilities manifest in access to schooling: of the estimated 240 million children with disabilities globally, around 120 million are out of school (UNICEF, 2021). Despite the expansion of primary education participation, Nigeria has an estimated 10.5 million primary-age children out of school (Baum et al., 2018), and has pronounced disability gaps in primary-school enrolment (Mizunoya et al., 2018). Structural barriers, including excessive fees, constrain access (Baum et al., 2018), exacerbated by exclusion through stigma or lack of adaptation. Despite policy commitment to inclusive education, there is a lack of practical implementation (Ajuwon, 2008). Teachers remain largely unaware of their responsibilities under the 2018 Act (Bamisaye et al., 2024), and parents report government reluctance to fulfil its obligations (Edward-Dibiana, 2023).
Institutional features of societies are also related to differences in values and norms. Chataika and McKenzie (2013) argue for a differentiated understanding of child disability in Africa, highlighting differences in social organisation and in cultural attitudes. They note the importance of extended families in care and support and more collective approaches to well-being. While such conditions are likely to have consequences for the stigmatisation of disability, it is unclear if they apply in Nigeria.
Stone-MacDonald’s (2012) study of a school in Tanzania highlights the relevance of local attitudes to the inclusion of children with disabilities. She paints a mixed picture where the children both are seen as a ‘gift from god’ and yet may be hidden away. Accounts of the causes of disability merge biology, contemporary religiosity and older beliefs in witchcraft. Yet her account focuses on interpretations from a phenomenological approach, rather than situating them within wider social structures. Spiritual interpretations of disability have also been cited for Nigeria (Ishola-Esan, 2016); but no connection has been made between dominant moral judgements and an institutional context that demonstrates very limited de facto recognition of the needs and rights of children with disabilities (Grech et al., 2023).
We address how these features of the Nigerian context shape the experience of parenting a child with disabilities, and reflect on how our findings speak to existing sociological research.
Methods and sample
Sampling and interviews
Our sample was accessed via a Facebook group comprising over 95,000 parents of children with disabilities in Nigeria. While the group does not cover the full range of parents of children with disabilities in Nigeria and will inevitably tend to identify those somewhat more engaged with disability issues, it nevertheless gave us access to a broad set of parents in different social and economic circumstances. We focused on mothers as they tend to have greater responsibility for the child, and the stigma associated with their disability (see Gray, 2002). We note, however, that those without internet access, digital literacy or an interest in online peer-support communities were not represented in our recruitment pool.
We selected the Facebook group as the source for our sample to facilitate voluntary recruitment and to avoid dependence on a gatekeeper, which might have impacted confidence in disclosure or led to different selection issues. Crucially, one of the researchers was a member of the group, as she has a child with disabilities, and this gave her approach credibility and elicited trust among those considering participating (cf. Green, 2003).
We achieved our target of 22 interviews, split between (a) those with children in private schools, (b) those with children in state schools and (c) those with children out of school. This stratification was intended to ensure diversity in the socio-economic position of parents and in the contexts in which disability plays out. At the design stage, we anticipated that differences in educational access might structure our findings, though in our analysis we found more commonalities than differences across the strata. The project was approved by the Ethics Committee of the London School of Economics and Political Science in October 2022.
Semi-structured interviews of around 60 minutes were conducted via the video-call function of WhatsApp, to suit the convenience and availability of respondents, and to help ensure diversity in location and circumstances across the sample. Small incentives were offered to offset any direct costs of participation, given high data costs in Nigeria, which helped to ensure inclusivity. A small gift for the child was given after the interview as a form of recognition. The researcher conducted interviews in the respondent’s preferred language. In Nigeria, it is common, irrespective of educational level, to switch between Nigerian Pidgin and Standard English, depending on context and relationship with the interlocutor. In interviews, the interviewer responded accordingly, allowing for fluid movement between linguistic codes in ways that supported rather than constrained the dialogue. This aided the development of rapport and helped to mitigate potential power imbalances between interviewer and interviewee. Nigeria is a country of over 500 languages and, despite the interviewers being fluent in a number of these, in two cases an interpreter was required. From the perspective of the interviewer, rapport was still maintained, and power imbalances were minimised.
Questions covered mothers’ perceptions of the causes of the disability; education; family relationships; financial implications; and perspectives on governmental support. The interviewer invited mothers to define their experience and describe any other challenges and benefits of parenting a child with disabilities. We note that in what follows we are reflecting mothers’ reports and interpretations of their child’s circumstances, which may differ from those felt or expressed by their child.
Characteristics of our sample
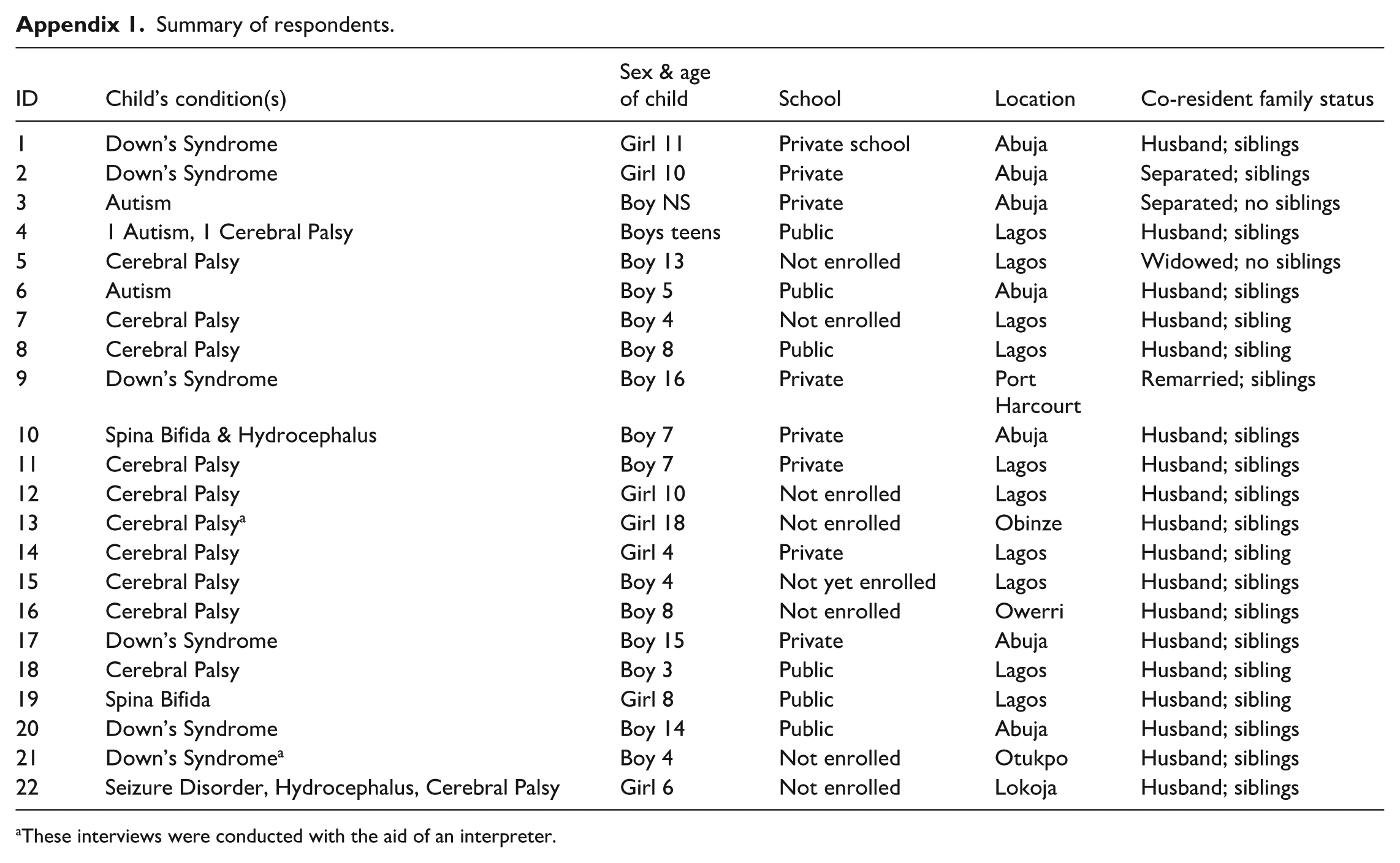
We did not aim to stratify by condition; though, in practice, the children predominantly had either Down’s Syndrome (6) or cerebral palsy (12), with smaller numbers with autism (3), hydrocephalus (2) and spina bifida (2): see Appendix. While we cannot compare systematically across these conditions, we remained alert in our analysis to possible differences; but found little evidence for distinctive patterns. The size and nature of our sample may, however, have reduced our ability to observe meaningful distinctions across conditions.
The age of the focal child ranged from 4 to 18, with most being under 12. The government Universal Basic Education programme runs from age 6, but school and nursery enrolment can occur earlier. Enrolment in education, and participation in private rather than state education, is heavily dependent on resources, thus school type also acts as a proxy for socio-economic context. No respondents identified themselves or the father of the child as having a disability, though this was not directly asked. Many Nigerians born before the 2000s live with undiagnosed conditions such as dyslexia or ADHD (Iwuagwu et al., 2022). Most respondents lived with their husband, which offered them a potential bulwark against stigmatising attitudes; but a small number were separated, sometimes as a consequence of the child’s disability – a point we return to. Most lived in Abuja or Lagos, urbanised settings that might have been expected to be less dominated by the traditional attitudes found in the rural contexts described by Stone-MacDonald (2012) and Chataika and McKenzie (2013). There was some additional regional variation, which respondents suggested had implications for opportunities and levels of support. In the Appendix, we provide summary sample details.
Analysis
We transcribed the interviews and employed thematic analysis of the data, following the six-stage process outlined by Braun and Clarke (2006). We adopted a realist approach to our analysis, and recognised that the themes were shaped by – though not identified with – the questions that constituted our interview schedule. We conducted initial familiarisation with the data and independently generated initial codes, before jointly collating those codes into key (selected) themes, supplemented by consultation of field notes. Consensus on the key themes was achieved iteratively through discussion, reflection and consideration of the study’s aims and conduct. We focus on the theme of stigma, which was expressed across the corpus. We examine how it was experienced by mothers and described as affecting children. We also explore how mothers framed their resistance to stigmatisation. We outline the ways in which the Nigerian experience aligns or contrasts with understandings of disability-related courtesy stigma from the high-income countries that dominate existing literature.
Findings: The experience of stigma
Strikingly, almost all mothers explicitly described experiences of stigma affecting both their children and themselves. Only three did not use the term stigma directly, but their accounts nonetheless reflected the dynamics of ‘labelling, stereotyping, separation, status loss, and discrimination’ (Link & Phelan, 2001). In what follows, we trace the ways in which separation and status loss emerged from context-specific forms of stereotyping and mothers’ experiences of felt stigma, while also noting points of resonance with wider scholarship. We then examine how enacted stigma shaped the children’s lives. Finally, we turn to the strategies mothers employed to navigate and resist stigmatisation. Here too, their narratives reveal distinctive features, while also in some respects echoing existing accounts
Evil spirits and moral failings
Central to the experience of stigma among these mothers was a worldview that emphasised the spiritual causes of child disability. They gave consistent accounts of what they described as the ‘majority’ Nigerian view, both in general and as they had personally encountered it. This worldview located disability not in material or medical explanations but in spiritual ones: a child’s condition was attributed to actions that had exposed the family to malign forces or evil spirits, or to some form of moral or spiritual failing. A broader literature underlines how such beliefs are grounded in Nigerian epistemologies that position the spiritual realm as the base of society (Lazarus, 2019). Within this worldview, misfortune is often read as evidence of moral failing or spiritual neglect. The mothers in our study encountered this logic directly, with disability attributed to exposure to malign spirits or lapses in religious observance, reflecting this wider cultural script. This perspective partly echoes the community views described and rejected by respondents in Stone-MacDonald’s (2012) Tanzanian study. Unlike the Tanzanian study, however, our respondents were predominantly urban, contrasting with the rural settings identified by Chataika and McKenzie (2013) as sustaining such beliefs.
A striking feature of the stigma was its individualisation. The associative stigma experienced by mothers emphasised maternal responsibility for the child’s disability, casting it as evidence of her moral failings. In this sense, stigma weighed as heavily on the mother as on the child. Despite the apparent distinctiveness of the societal worldview described by our respondents compared to that in high-income contexts, the tendency to attribute responsibility at the individual level, in this highly economically unequal society, was comparable to that seen in capitalist settings structured by class relations (McLaughlin, 2017; Scambler, 2004, 2009).
Specifically, many mothers referred to having been told that the disability was due to them walking in the sun in the middle of the day while pregnant:
I remember when I was pregnant with my son in Lagos, some Yoruba women accosted and said, ‘Ah! It’s not good to walk in the sun when you are pregnant’, that some evil spirits roam around in the afternoon and when they see a pregnant woman like this that they could harm her. [#5] Some blame it on me, saying that it could be that I walked under the sun like about 1pm when I was pregnant. You know in my Yoruba ethnic group in Nigeria it is believed that walking in the sun while pregnant around that particular time in the day could be responsible for a number of challenging defects in a child. [#7]
Similar statements were also made by other mothers (e.g. #7, #14 and #20). Some mothers reported beliefs that located the source of the disability in lack of appropriate observance of prayer by the mother, or in her supposed immoral actions: ‘Some people say it’s because of some sins in the family, and I should do spiritual cleansing’ [#5]; ‘They blame me for my son’s condition, saying it is a curse on my family’ [#7]; ‘Some members of my immediate family believe the disability of my child is a punishment for whatever evil deed they thought I would have done’ [#12]. Again, the mother was being held individually accountable, exonerating others from communal or institutional responsibility. Only one of our respondents endorsed these views as a way of explaining her son’s disability:
I have a very strong belief that someone is responsible for my son’s condition. . . . Some evil people must have been responsible. Maybe they harmed him when I was pregnant by casting some spell on the pregnancy. [#21]
Comparable to some of the views reported in Stone-Macdonald (2012) of the role of God in determining disability, another mother considered that her child’s special needs must have been sent from God. She also drew on this faith to hope in his eventual recovery:
Some would tell you it’s medical; but as parents, when you look at it very well, you know that there’s a message God is trying to give you from this kind of situation. [#3]
However, despite the strongly expressed religious faith of many mothers, most did not understand their child’s disability as a consequence of spiritual or moral factors.
Apart from the mother cited above, by the time of the interview, no other mothers attributed their child’s condition to evil spirits, curses or moral failings on their part. However, some had for a while internalised this stigmatising view and accepted the marking-out of their child’s body as representing a personal failing that required atonement. One mother now bitterly regretted what she had put her child through as a result:
Sometimes I cry whenever I’m bathing my daughter and I see the scars inflicted on her by some of those native doctors, who used to cut her body with sharp blades because they wanted the purported demonic blood in her, responsible for her condition, to flow out for her to be healed. My daughter [has] suffered a lot of pain in our search for healing for her disability. When I was still ignorant, I took her to a lot of places where she went through a lot. [#12]
The close affinity of stigma with violence (Tyler, 2020) is vividly illustrated here, with the physical scarring that is the tangible evidence of that stigma. Another mother had initially accepted that her spiritual deficits had been responsible for her child’s disability and tried prayer and pilgrimage to correct this. But she subsequently changed her mind: ‘I thought it was a spiritual thing that could be resolved. . . . I was going from one mountain to another looking for miracles’ [#8]. A similar experience was described by #11.
This stigma that derived from such socio-cultural attitudes to disability was also, as with the assumption of caring responsibilities, highly gendered: it was the mother to whom the child’s disability should be attributed. Fathers were never mentioned as having been culpable for their child’s disability, nor needing spiritual atonement. Instead, the presence of a disability in the family could disrupt family relations. In two cases, mothers spoke of how the father separated from them as a consequence of their child’s disability; and others, whose husbands remained, assumed that the child was still their specific responsibility. This came through not only in terms of being the primary carer, but in acknowledging the virtue of fathers who continued to support them financially. One mother noted having ‘seen a lot of single mothers who were abandoned by their husbands because of their special children. So I appreciate my husband for not leaving me’ [#4]. This gendered moralisation of responsibility resonates with research on family breakdown in Nigeria, where divorced women face intense stigmatisation, often being blamed for the breakdown of their marriage and consequently excluded from opportunities to remarry (Lazarus et al., 2017). Such parallels underscore how stigma interacts with wider social hierarchies, and the tendency of the power relations inherent in disability stigma to promote a neoliberal understanding of experiences of disability (Scambler, 2018).
Literature from wealthy nations centres largely on mothers’ experiences and ‘battles’ (Thomas, 2024). Where fathers are included, findings are mixed regarding their perceived responsibility (e.g. Gray, 2002; Thomas, 2021), though rarely framed through a clear gendered lens around disability. Beyond fathers, Chataika and McKenzie (2013) show that extended family can serve as a support system, yet may also reinforce stigma, particularly mothers-in-law who view children with disabilities as a source of shame. In our sample, some relatives offered financial and emotional support: ‘My mum really tried for me . . . both financially and emotionally. Even currently, she still sends me money [#4]. Still, exclusion and isolation frequently extended to in-laws and even close kin.
The negative attitudes to both mother and child led to a high degree of isolation: the separation that follows from stigma. Mothers expressed this vividly: ‘Sometimes I feel so alone, like nobody understands what I’m going through’ [#4]; ‘I can’t talk to anyone about it; people just judge you, and it’s very isolating’ [#11]; ‘sometimes I just feel like I’m at my breaking point’ [#13]; ‘The worst part is the loneliness; even my extended family doesn’t understand me’ [#19]; ‘Most times I just sit inside my room and cry’ [#21]. Such isolation was exacerbated by the limited resources at their disposal, though it could not be collapsed into their economic precarity.
Enacted stigma and child exclusion
If mothers were particularly affected by moral judgements and the impact of felt stigma, which had consequences for their sense of isolation and confidence (see Green et al., 2005), they also noted the deep challenges of the enacted stigma, or discrimination and exclusion, that their children faced. Their negotiations with educational institutions and hospitals about their children’s physical and cognitive challenges revealed high levels of exclusion. Despite policy commitment to providing primary education for all, mothers discussed how schools were typically reluctant to accommodate their children. One described how, at one school, ‘they would reject him because he can’t walk. We would go to another school and the story was the same’ [#4]. Others drew attention to the expectations that mothers would fund the additional support their child needed in school: ‘the school my child goes to, a mainstream school, he is in primary one; but . . . I have to get a teacher for him. I pay the teacher, and I still have to pay school fees, which is like four times what others pay’ [#11]. Some saw in these additional charges an exclusionary agenda:
Many schools don’t want to take children with special needs. And if you have the opportunity to get into any school that agrees to take them, you’ll pay triple what others pay. Is that not discrimination? [#8] The school head . . . agreed to register him but on the condition that his school fees would be 30% more. [#20]
Reports of schools rejecting their child, or, if accepted, requiring additional fees, were almost ubiquitous across the sample. Hence, while the quality of education within the school was also a concern (see Blum, 2015; Farrugia, 2009), the principal issue was access. A common refrain was the lack of inclusive education: ‘There is nothing like equal opportunity . . . inclusive education is almost non-existent in this country’ [#2]. While some noted regional variation in provision of (fee-paying) special schools, the lack of inclusive education was argued to be present in all areas.
It was not only education where additional payments created barriers for parents and were regarded as the norm. Health expenditures were typically large, and often out of reach even for those with some resources: ‘I also got to know that . . . there is medication that she can take that can facilitate her growth and everything. We did it for one month and we had to stop because it cost the family N150,000 for just one month’ [#1]. But in addition, medical costs appeared to attract a premium when sought for children with disabilities: ‘In Nigeria, if you take your child with special needs to any hospital and you want to run a test or have therapy session, you will pay through your nose. . . . Because he is a special needs child, they would increase the charges’ [#3]. A similar claim was made by #8. Mothers’ ability to provide the care they wished, and that they thought crucial, was thus severely constrained by economic exclusion.
Transportation was also difficult for many mothers, and another site of stigmatising exclusion of their child and humiliation for them:
Some public drivers, immediately they see you with a child with disability, they will just tell you they don’t carry ‘load’. Referring to the child as a load. They have said that to me a number of times. That’s part of the daily humiliation and discrimination we face as parents of people living with disability. [#8]
Another referred to the fact that ‘when we get to our bus stop, the way they will even fling the wheelchair down’ [#13]. The culture of blame that afflicted mothers thus extended to these forms of enacted stigma that characterised their day-to-day interactions with the disabling environment. Their lack of entitlement to services appeared to feed a culture that deprived them and their child of access and dignity (see Scambler, 2018).
Within school, stigma was also, on occasion, acted out through violence: ‘Sometimes my child comes back from school and say to me, mummy, my teacher hit me on my head and said I’m good for nothing’ [#8], reinforcing the link between stigma and violence (Tyler, 2020). Aggression, criticism or exclusionary behaviours, including ‘staring’ (cf. Gray, 2002; Farrugia, 2009), were also experienced in the wider social environment. A number reported the negative impact of such dehumanising treatment; and many emphasised the pressure to hide their child away in response to such exclusion [#2, #3, #7, #8, #9, #12, #18, #19, #22], even though they largely tried to resist it.
Mothers also spoke of schools excluding their child on the basis of complaints from other parents, reluctant to have their children ‘mingle’ [#20] with a child with disabilities. Underpinning this exclusion was a prevalent contagion model of disability that was a distinctive feature of their narratives. For example, one mother mentioned that ‘people would be avoiding him, because they felt that his disability was contagious’ [#4]; another noted that ‘some people think that this kind of disability is contagious’ [#11]; a third that ‘some relatives and neighbours . . . lock her out of their lives and homes as if her condition was contagious’ [#13]; while a fourth stated that ‘they avoided us as if my child’s condition was contagious’ [#21]. Reported across respondents, this reaction suggested that the understanding of disability as ‘contagious’ was general rather than condition-specific, at least for the conditions represented in our sample. Exclusionary complaints from other parents were all the more influential in private schools reliant on parental fees, which were in turn those schools that might have been expected to provide better adaptations and specialised support, demonstrating how socio-economic position cross-cuts the experience of parenting a child with a disability (see Blum, 2015).
Greater socio-economic advantage could clearly mitigate the exclusion caused by stigma when it is possible to buy into more accommodating environments, as noted by some mothers [e.g. #12, #13]. Class position and money could enable access to facilities and education for children with disabilities, as powerfully expressed by one relatively better-off mother: ‘Thank God that we are able to meet his basic needs, especially as it relates to his school’ [#10]; and as regretted by another financially struggling mother [#7]. However, in general, stigma was not itself conditioned by socio-economic position, with those across the financial spectrum pointing to the lack of inclusion or recognition and the extent of discrimination.
Responding to stigma
Mothers invoked various strategies of resistance to this stigma. Principal among these was an emphasis on asserting the biological origins of the disability. As discussed by Thomas (2024), reference to the biological is one means by which mothers try to deflect stigma or reshape negative attitudes. Its utility in deflecting courtesy stigma manifested in criticisms of parenting has been emphasised in studies on autism (Farrugia, 2009; Gray, 2002), particularly in relation to the child’s behavioural difficulties. But in this context, it was critical to defending against the implied shame and responsibility across the full range of conditions.
Linked to this emphasis on biological origins of disability was a focus on educating people about disability as the way to reduce stigma. However, emphasising education implies that a correction can be made at the individual level; and thus does not address structural causes (Scambler, 2004, 2018) or the power relations that shape the application of stigma (Tyler, 2020). Nevertheless, mothers argued that education had positively influenced and reshaped some local interpersonal relationships.
Mothers recognised that socially embedded stigma and its enactment in, for example, bullying of their children as they progressed through life was unlikely to disappear, even with greater education. Acknowledging pervasive societal discrimination, one mother explained how she felt it was important to prepare her son for it by sending him to a school that would ‘toughen’ him:
In the first week in the public secondary school, they stole his lunch money. Next time when I gave him money, he put it inside his socks so that it won’t be stolen. That’s practical life lesson . . . He was pushed down a number of times, people laughed at him; but he learnt a lot. That school toughened him. Was it not last week he was telling me, ‘mummy, thank you for making me to go to a public school. I was bullied but my experiences in that school made me more prepared to face the society.’ [#4]
Just as the expression of stigma was often conceived in spiritual terms, so responses attempting to manage it also invoked spiritual resources as forms of resistance. Thomas (2024) has talked about the reformulation of the child’s disability as a blessing (see Goffman, 1963); and there was an attempt by mothers to find a spiritual meaning in what had been represented to them as a spiritual evil.
Greeff and Loubser (2008), in their analysis of Xhosa speakers in South Africa, discuss how spirituality is embedded in responses to adversity across the life course in Africa more widely. Many mothers expressed the importance of their faith as a source of support, but spirituality also shaped their understanding of their child’s disability and their role as mothers. Their faith often offered a way to understand their situation and to push back against some of the negative imputations made against them. ‘I always tell myself that God must have seen something for Him to have given me my child. If not me, who? . . . There is a reason for everything’ [#10]. It also allowed them to assuage the guilt they often felt: ‘I have stopped blaming myself. God knows the best’ [#8]. Christianity could also be instrumental in supporting their rejection of suggestions that their child’s disability was caused by demonic forces: ‘I’m a strong Christian and I would not even consider such’ [#6]. Many also used the language of ‘special needs’ to highlight the ‘specialness’ of their child, simultaneously acknowledging the ways in which disability shaped his or her life, while asserting the child’s uniqueness and individuality (cf. Farrugia, 2009).
Finally, seen as offering some potential for structural change, many mothers promoted an advocacy approach. As noted, the women in our sample were more likely to be aware of and sensitive to disability issues due to their participation in the Facebook group. Mothers saw their role as modelling to the outside world the value they put on their child and the love they showed them in order to shift social attitudes. This is commensurate with moves away from ‘hiding away’ children with disabilities (Chataika & McKenzie, 2013). They explained that public demonstrations of pride and affection would communicate to those inclined to mock or stigmatise disability that their children merited love and inclusion. While such advocacy might not be expected on its own to change the wider social structures and power relations that rendered them victims of stigma; yet their modelling approach was potentially societal in reach, even if it originated with their individual behaviour. It offered a bottom-up approach to social change, in the face of institutional neglect of equality. One mother concluded her interview by urging:
The parents of children with special needs should not give up. I know how hard and distressing the struggle is, but . . . they should continue to give more care and more attention to their children because that’s when other people around can do the same to the children. If you let them know that this child is important to you, that this child is the love of your life, they have no choice. [#2]
This emphatic message on the value of children with disabilities presented a way forward for mothers to dispel the stigma they experienced through a positive formulation based in their maternal relationship but invoking universal values requiring societal recognition.
Discussion
Child disability is unequally distributed socio-economically and globally. Yet sociological understanding of its implications for children and their families, and in particular how stigma is experienced and engaged with, is partial and overwhelmingly investigated in high-income countries, particularly the US (Thomas, 2024). This is despite reports highlighting both the prevalence of child disability and the relevance of stigma in LMICs (UNICEF, 2021; World Bank Group, 2011).
Ours is the first study of the stigma faced by mothers of children with disabilities in Nigeria. It focuses on parents of children with a range of conditions, including those less frequently studied in rich countries, such as cerebral palsy. In this study, we give voice to those struggling to raise their children in a context where there are deeply judgemental attitudes to disability alongside an absence of economic support and educational opportunity, even by comparison with a number of other LMICs. This is despite the official endorsement by Nigeria of the UN Convention on the Rights of Persons with Disabilities, often honoured more in the breach than the observance (Grech et al., 2023). We shed light on the courtesy stigma mothers were subject to, and their accounts of the stigma enacted on their children.
Beyond the important element of voice, our study offers further specific contributions. We explored the extent to which stigmatising experiences were distinctive relative to the existing literature, or, conversely, whether they showed points of commonality.
One key distinctive feature of this context was the attribution of disability to spiritual causes that then allowed for a highly individualised form of moral blame and shame (Scambler, 2004). These prevailing ideas served to socially isolate mothers and often enhanced existing feelings of guilt, as well as, at times, being linked to violence against the child. These attitudes were accompanied by a high degree of enacted stigma, excluding children from opportunities, services and participation, which was often linked to contagion accounts of disability.
The specific nature of enacted stigma in limiting access to school was a striking and distinctive feature of the Nigerian context. There has been discussion of the implications of the move towards more neoliberal approaches to disability in rich countries (Chatzitheochari & Butler-Rees, 2023; Scambler, 2004, 2018; Thomas, 2021); but in our study, the highly devolved provision of education with a large low-cost private sector made mothers especially subject to market processes, enhanced by the understandings of disability as contagious and the conditioning of educational provision on the ‘consumer’ demands of other parents, who often held such views.
In Nigeria, we see children with disabilities and their families being systematically left behind as drives towards universal basic education fail to accommodate them, and as informal social support breaks down, with no cash transfers to replace it. While existing literature documents the challenges that mothers face in obtaining rights and provision for their children (Blum, 2015; Green, 2003), Nigeria lacks a rights-based framework on which to draw. There is currently a move to amend the Discrimination Against Persons with Disabilities Act to promote greater inclusivity and equal opportunities for persons with disabilities. However, there is substantial scepticism about the effectiveness of such an amendment, particularly in the absence of wider societal change.
Some existing literature has focused on specific conditions or impairments, while a small number of studies has highlighted heterogeneity in experience across conditions, leaving the question of how far forms of stigma are specific to conditions somewhat open. Within the limits of our sample, we noted little systematic variation across the different conditions in terms of stigmatising beliefs and behaviours. The ‘discredited’ (Goffman, 1963) status of disability appeared to invite similar processes of shame and exclusion regardless of the specific condition. However, a more extensive study might be able to shed further light on this question.
There were a number of commonalities with existing studies. These included mothers’ formulation of the child as special and constituting a gift or blessing, and their stress on normalising their children’s behaviour and experience (see Farrugia, 2009; Thomas, 2024). Some mothers also claimed personal transformation as a result of caring for a child with disabilities in terms of their growth, development and assertiveness, despite the challenges. Yet, for many their experience was of continual struggle. Such a balance between celebration and struggle is also found in existing literature (e.g. Blum, 2015; Green, 2003; Thomas, 2024).
Their accounts also hint at the value of new forms of collective action that can be achieved, even for those so constrained, with social media praised as a source of information, companionship and, on occasion, financial resources. The mothers made a compelling case for the potentially transformative power of inclusive education. While much literature from Europe and North America has discussed how disability is constructed within the school setting (e.g. Powell, 2003), mothers recognised the significant socialisation potential of schools, despite the challenges in gaining access. The expansion of compulsory education in Nigeria, by increasing the possibilities for disabled and non-disabled children to interact, was seen as an important way to bring disability ‘out of hiding’ and shape a new understanding in the coming generations. Such a shift could potentially result in positive synergies through feedback effects on culture, institutions and policy, enabling disability rights to develop in a country where their absence is marked.
Conclusions
The impact of stigma on parents of children with disability is of longstanding sociological interest. Our study of stigma and child disability in Nigeria contributed to the sociological literature by extending our understanding not only of the forms disability-related stigma takes, but also how these relate to the specific cultural and institutional context in which they occur. We showed that the combination of lack of structural support and equal opportunities for children with disabilities, alongside a marketised health and education system, a highly gendered social organisation, and a worldview emphasising spiritual drivers, results in a highly stigmatising environment for mothers and children. The emphasis on individual moral failings and heavy financial burdens both limit mothers’ ability to make claims and reinforce existing structural power dynamics. Yet, the mothers in our study also demonstrate how their experience provides some potential for mobilisation and for reinterpretation of standard narratives to argue for social change and greater rights. Future research would benefit from considering the role and perspective of other actors involved in maintaining or transforming the status quo for families of children with disability, from investigating heterogeneity in the experience of stigma, and from studying whether LMICs with different institutional structures reveal similar or distinctive insights.
Footnotes
Appendix
Summary of respondents.
| ID | Child’s condition(s) | Sex & age of child | School | Location | Co-resident family status |
|---|---|---|---|---|---|
| 1 | Down’s Syndrome | Girl 11 | Private school | Abuja | Husband; siblings |
| 2 | Down’s Syndrome | Girl 10 | Private | Abuja | Separated; siblings |
| 3 | Autism | Boy NS | Private | Abuja | Separated; no siblings |
| 4 | 1 Autism, 1 Cerebral Palsy | Boys teens | Public | Lagos | Husband; siblings |
| 5 | Cerebral Palsy | Boy 13 | Not enrolled | Lagos | Widowed; no siblings |
| 6 | Autism | Boy 5 | Public | Abuja | Husband; siblings |
| 7 | Cerebral Palsy | Boy 4 | Not enrolled | Lagos | Husband; sibling |
| 8 | Cerebral Palsy | Boy 8 | Public | Lagos | Husband; sibling |
| 9 | Down’s Syndrome | Boy 16 | Private | Port Harcourt | Remarried; siblings |
| 10 | Spina Bifida & Hydrocephalus | Boy 7 | Private | Abuja | Husband; siblings |
| 11 | Cerebral Palsy | Boy 7 | Private | Lagos | Husband; siblings |
| 12 | Cerebral Palsy | Girl 10 | Not enrolled | Lagos | Husband; siblings |
| 13 | Cerebral Palsy a | Girl 18 | Not enrolled | Obinze | Husband; siblings |
| 14 | Cerebral Palsy | Girl 4 | Private | Lagos | Husband; sibling |
| 15 | Cerebral Palsy | Boy 4 | Not yet enrolled | Lagos | Husband; siblings |
| 16 | Cerebral Palsy | Boy 8 | Not enrolled | Owerri | Husband; siblings |
| 17 | Down’s Syndrome | Boy 15 | Private | Abuja | Husband; siblings |
| 18 | Cerebral Palsy | Boy 3 | Public | Lagos | Husband; sibling |
| 19 | Spina Bifida | Girl 8 | Public | Lagos | Husband; sibling |
| 20 | Down’s Syndrome | Boy 14 | Public | Abuja | Husband; siblings |
| 21 | Down’s Syndrome a | Boy 4 | Not enrolled | Otukpo | Husband; siblings |
| 22 | Seizure Disorder, Hydrocephalus, Cerebral Palsy | Girl 6 | Not enrolled | Lokoja | Husband; siblings |
These interviews were conducted with the aid of an interpreter.
Acknowledgements
The authors are grateful to the mothers who provided these insights into their experience. We are also grateful to the three anonymous referees for their detailed and constructive suggestions and to Daryl Martin and Carin Runciman for their editorial input, which has greatly strengthened this paper.
Funding
This research was supported by the LSE Department of Social Policy Titmuss Meinhardt Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.