
Abstract
Objective
Cancer and other noncommunicable diseases (NCDs) are increasingly recognized as a global development challenge. The most recent UN high-level meeting on NCDs underscored insufficient progress toward the Political Declaration on NCDs. Key barriers—including gaps in situational analysis, priority setting, and budgeting—all hinge on localized cancer epidemiology data. The Global Burden of Disease (GBD) study is uniquely positioned to provide this essential information.
Methods
This study estimated global malignant tumor burden and trends across 5 socio-demographic index (SDI) areas and 21 regions from 1990-2021 and projected trends to 2041 using GBD 2021 data for 33 tumor groups.
Results
In 2021, there were 23.4 million (95% UI: 22.3-23.6 million) new cases, 9.8 million (9.1-10.5 million) deaths, and 251 million (235-268 million) DALYs attributable to malignant tumors, ranking them third globally for DALYs after respiratory infections and tuberculosis. Tracheal, bronchus, and lung (TBL) cancer was the leading cause of cancer mortality in both genders combined (15/21 regions) and in males (14/21 regions), while breast cancer led female mortality (12/21 regions). In high-SDI areas, malignant tumors ranked first for DALYs. TBL, colon and rectum cancer (CRC), and breast cancer comprised the top three DALY causes for both genders combined and for females; for high-SDI males, the top three were TBL, CRC, and pancreatic cancer. Projections to 2041 (Bayesian age-period-cohort [BAPC] model) indicated decreasing age-standardized incidence rates (ASIR) and case numbers for stomach and esophageal cancers. Conversely, rising ASIR and incidence numbers were projected for CRC, breast cancer, prostate cancer, lip/oral cavity cancer, multiple myeloma, thyroid cancer, and testicular cancer.
Conclusions
The cancer burden profile is strongly influenced by SDI level and gender, with high-SDI regions characterized by TBL and CRC, while lower-SDI regions face a higher burden from gender-specific and infection-related cancers. TBL cancer remains the dominant driver of cancer mortality worldwide, particularly among males. Breast cancer shows remarkable consistency as the leading female-specific cancer across most regions by both incidence and mortality.
1. Introduction
Malignant tumor is the second leading cause of the global health burden in considering absolute disability-adjusted life years (DALYs) in 2019. 1 The United Nations’ Sustainable Development Goals (SDGs), emphasized the urgency of diminishing the malignant tumor burden. The goal is to achieve a 33% reduction in premature mortality from noncommunicable diseases (NCDs) by the year 2030 through enhanced prevention, treatment, and fostering mental health and overall well-being. 2 To align with this SDG, nations must expedite their initiatives to alleviate the impact of NCDs, with a particular focus on malignant tumors.3,4
The Global Burden of Diseases (GBD), Injuries, and Risk Factors Study 2021 (GBD 2021) framework facilitates the standardized evaluation of malignant tumor burden across different regions and periods, focusing on metrics such as tumor incidence, mortality rates, and DALYs. The GBD 2021 provides a robust estimation of disease burden across a comprehensive and exclusive classification of diseases and injuries, allowing for a systematic comparison and prioritization of malignant tumors relative to other health conditions. By offering a detailed overview of variations in malignant tumor burden, the GBD 2021 can serve as a valuable resource for shaping cancer control strategies and interventions. 5
The GBD 2019 study provides comprehensive estimates: increased cancer prevention and control efforts are needed to equitably address the evolving and increasing burden of cancer across the SDI spectrum. 1 Our analysis adds distinct value by: (i)synthesizing the burden of all 33 malignant tumor groups (four more than previous major GBD cancer analyses) within a single comparative framework; (ii) performing the first comprehensive 20-year projections (to 2041) for this expanded set of cancers; and (iii)explicitly mapping the leading causes of cancer incidence and mortality across 21 GBD regions by gender, a detailed regional-gender ranking not provided in the primary GBD publications.
2. Materials and methods
2.1. Study design
In the GBD 2021 study, diseases and injuries were organized within a comprehensive nested hierarchy, in which neoplasms constituted a second-level category (https://vizhub.healthdata.org/gbd-results/). Malignant tumors were further classified into 33 third-level groups (e.g., liver cancer), five of which were subdivided into fourth-level groups (e.g., liver cancer due to hepatitis B). Although the GBD study recognizes that benign and in situ tumors contribute significantly to the overall cancer burden, the estimates presented in this article focus exclusively on malignant cancers and therefore do not include these categories at the third level. Similarly, since non-melanoma skin cancer (NMSC) has a higher incidence and lower mortality rate compared to other malignant tumors, this article provides estimates including and excluding NMSC. 1
2.2. Data sources
Examining trends from 1990 to 2021, the GBD 2021 study assesses mortality and disability from hundreds of diseases, injuries, and risk factors around the world. This database includes mortality and morbidity in 204 countries and territories, and these were categorized into 5 areas in terms of the socio-demographic index (SDI) and 21 GBD regions according to geographical contiguity 6 ; 288 causes of death; 371 diseases and injuries; 88 risk factors (https://vizhub.healthdata.org/gbd-results). The GBD NMSC estimates included squamous cell carcinoma and basal cell carcinoma. Because NMSC reporting was incomplete in many cancer registries, 7 GBD 2021 additionally incorporated data from the literature and clinical sources to estimate NMSC burden. 1 Our study was in accordance with the Helsinki Declaration of 1975 as revised in 2024.
2.3. Reporting standards
From 1990 to 2021, estimates were reported for 33 malignant tumor groups, 21 areas, and the SDI quintiles. Numbers of incidence, mortality, DALYs, percentage change, and their corresponding rates were reported per 100,000 population, along with 95% uncertainty interval (95% UI) according to the GBD algorithm. 8 DALYs were estimated by adding the years lived with disability (YLDs) and the years of life lost (YLLs). Also, age-standardized incidence rates (ASIRs), age-standardized mortality rates (ASMRs), and age-standardized DALYs rates (ASDRs) of malignant tumors were extracted. This descriptive analysis focuses on presenting estimates with uncertainty intervals for each demographic subgroup (including sex). While formal statistical tests comparing estimates between sexes (e.g., assessing the significance of rate differences) were not the primary aim, comparisons can be inferred by examining non-overlapping 95% uncertainty intervals, which provide a conservative indication of potential statistical significance. Uncertainty was propagated through each step of the cancer estimation process, with UIs representing the 2.5th and 97.5th percentiles of the distribution of 1000 draws at each step. 1 Ranking was sorted by DALYs. To predict the future trends of incidence and DALYs of different malignant tumor groups from 2021 to 2041, we used the BAPC 9 in the R software (version 4.4.2, including BAPC and INLA packages). This modeling approach was selected because it specifically accounts for how cancer rates are influenced by three key factors: a person’s age (Age), the time period of diagnosis (Period), and their birth year (Cohort). By separating these effects, the BAPC model provides a more nuanced and demographically grounded forecast than simpler time-series extrapolations. For forecasting absolute death numbers, we complemented the BAPC model with an ARIMA model, 10 a well-established statistical technique for predicting future values based on past data, to enhance the robustness of our mortality projections. All calculations were performed using R Studio, version 4.4.2 (R Project for Statistical Computing). The reporting of this study conforms to STROBE guidelines. 11
3. Results
3.1. Global estimates of total malignant tumor groups and burden of 32 malignant tumor groups (excluding NMSC) in 21 regions
Among the 22 disease and injury categories at Level 2 of the GBD cause hierarchy (Figure 1), malignant tumors represented the third largest cause of disability-adjusted life years (DALYs) globally, following respiratory infections and tuberculosis. In 2021, there were an estimated 23.4 million (95% uncertainty interval: 22.3–23.6 million) new cases of malignant tumors and 9.8 million (95% uncertainty interval: 9.1–10.5 million) deaths worldwide (Table 1). The ranking of the total absolute disability-adjusted life years (DALYs) for 22 level 2 disease types in the Global Burden of Disease (GBD) study of 2021 according to the social-demographic index (SDI) quintiles. Global incidence and deaths in 2021 for total malignant tumors (with or without NMSC) and 33 malignant tumor groups. Note. NMSC, non-melanoma skin cancer; UI, uncertainty interval; ASMR, age-standardized mortality rate; NA, not applicable.

Globally, the top 5 causes of DALYs related to malignant tumors for both males and females combined are tracheal, bronchial, and lung (TBL) cancer, accounting for 18.5% of total cancer-related DALYs; CRC accounting for 9.7%; stomach cancer accounting for 9%; breast cancer accounting for 8.2%; and esophageal cancer accounting for 5.2% (Figure 2). Ranking of malignant tumor groups by disability-adjusted life years (DALYs) in 2021 and percentage change from 1990 to 2021.
In 2021, tracheal, bronchus, and lung (TBL) cancer was the leading cause of cancer-related DALYs globally (46.5 million), with particularly pronounced mortality burden across regions. It ranked as the top cause of cancer mortality in 15 of 21 regions for both sexes combined, and was the leading cause of mortality among males in 14 regions. Colorectal cancer (CRC) contributed 24.4 million DALYs and was the leading cause of cancer incidence in 5 regions, though it did not rank first for mortality in any region (Table1 and eTable 1-6).
Breast cancer demonstrated a distinct epidemiological profile: while ranking third in global DALYs (20.6 million), it showed exceptional regional dominance in female-specific burden. It was the leading cause of cancer incidence in 18 of 21 regions for females, and the top cause of female cancer mortality in 12 regions (Table1 and eTable 1-6).
Other significant contributors included stomach cancer (22.8 million DALYs) and esophageal cancer (13.0 million DALYs), though neither showed widespread regional dominance. Cervical cancer, while ranking lower in global DALYs (9.9 million), emerged as the leading cause of both incidence and mortality in 3 regions, highlighting its concentrated burden in specific geographical areas (Table1 and eTable 1-6).
The leading cause of malignant tumor incidence and mortality in 21 regions with gender-specific counts in 2021.
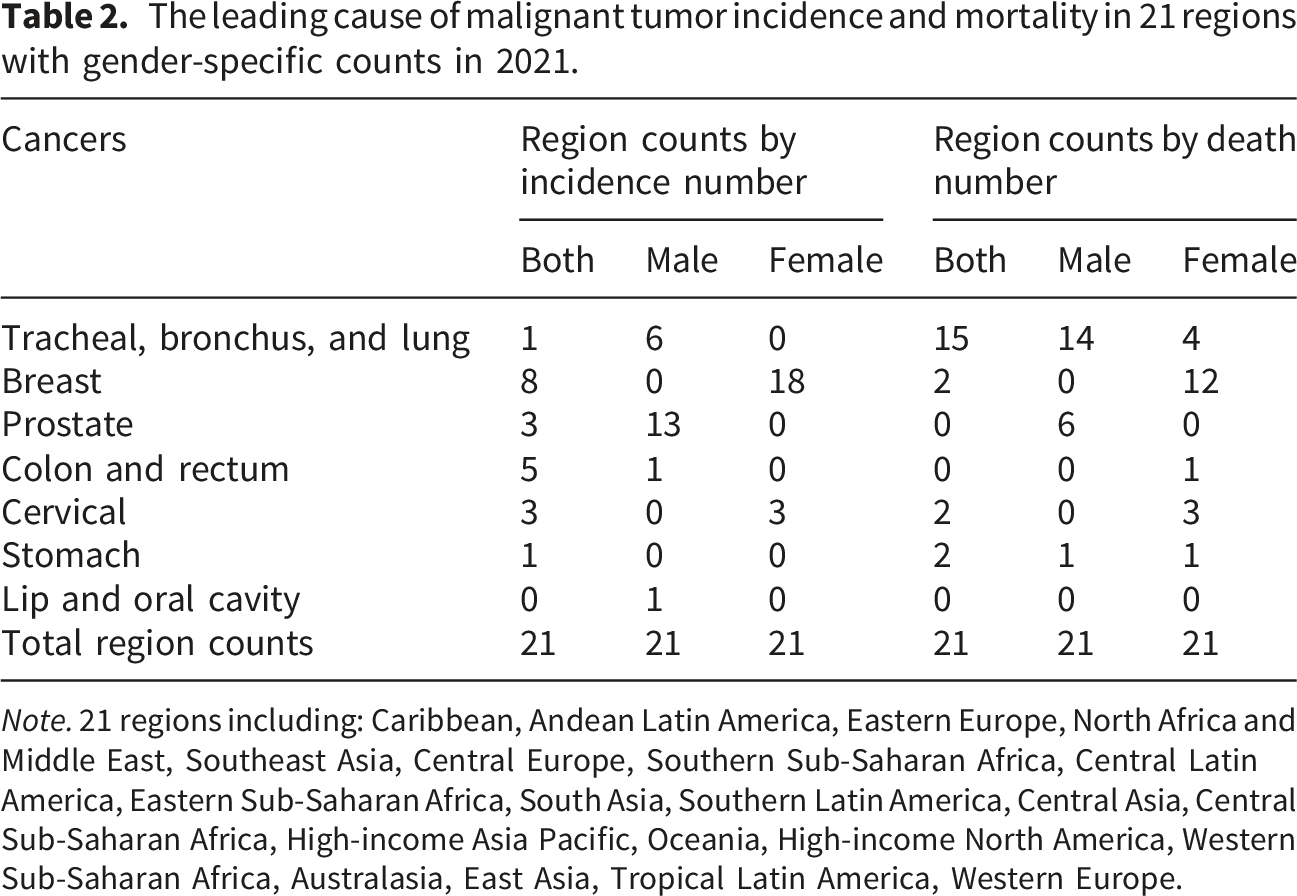
Note. 21 regions including: Caribbean, Andean Latin America, Eastern Europe, North Africa and Middle East, Southeast Asia, Central Europe, Southern Sub-Saharan Africa, Central Latin America, Eastern Sub-Saharan Africa, South Asia, Southern Latin America, Central Asia, Central Sub-Saharan Africa, High-income Asia Pacific, Oceania, High-income North America, Western Sub-Saharan Africa, Australasia, East Asia, Tropical Latin America, Western Europe.
Absolute death number of 33 malignant tumor types in 21 regions was demonstrated in etable8.
3.2. SDI burden in 2021
In the high-SDI area in 2021, TBL, CRC, and breast cancer were among the top 3 most DALYs for both genders and females. Accordingly, TBL, CRC, and pancreatic cancer were the top 3 most DALYs for males (Figure 3 and eTable7). However, TBL, CRC, and pancreatic cancer contributed the top 3 most absolute death in both genders (eTable8). Gender-specific rankings of 33 malignant tumor groups’ absolute disability-adjusted life years (DALYs) in 2021 in the Global Burden of Disease (GBD) study by 5 socio-demographic index (SDI) regions.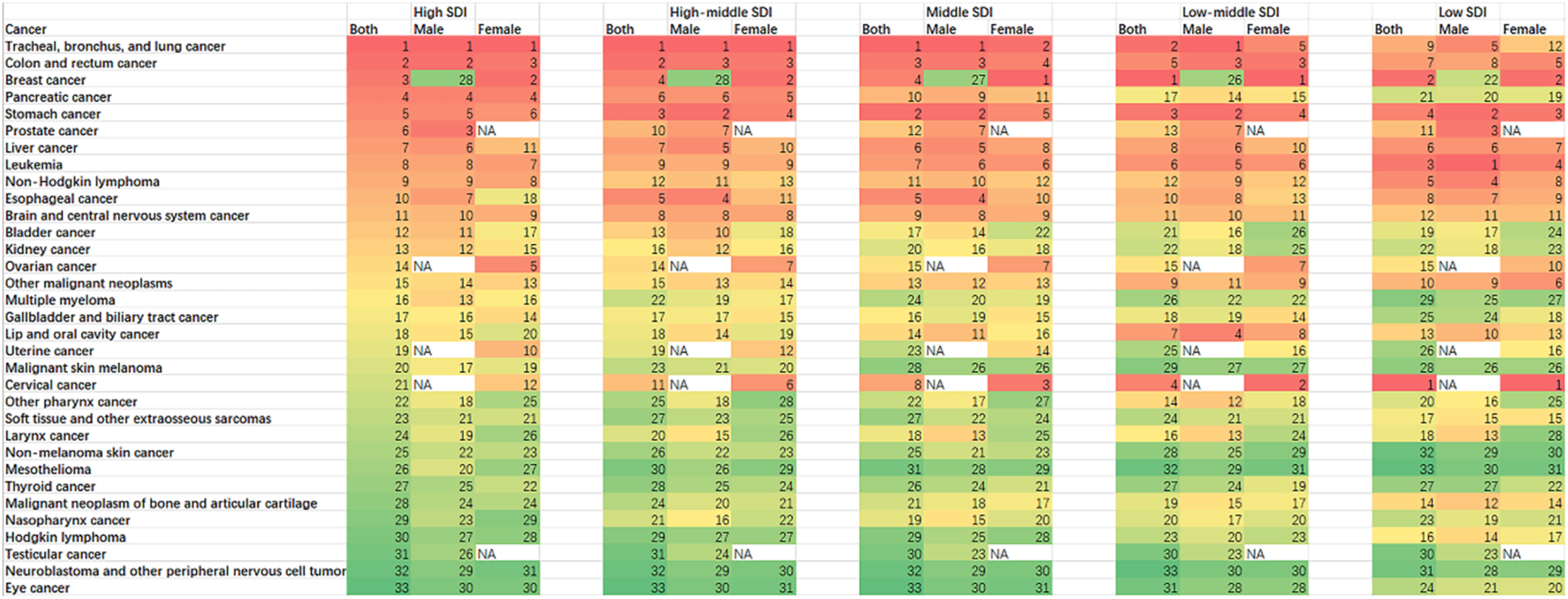
In high-to middle-SDI regions, tracheal, bronchus, and lung (TBL) cancer and colorectal cancer (CRC) consistently rank among the top three causes of cancer DALYs for both genders. Breast cancer is a leading cause among females in these regions, while pancreatic cancer ranks high for males in high-SDI areas (Figure 3, eTable7 and eTable8).
In low-to low-middle-SDI regions, female-specific cancers—notably breast and cervical cancer—emerge as dominant drivers of DALYs. Cervical cancer ranks highest among all cancers for females in low-SDI areas (Figure 3, eTable7 and eTable8).
A notable transition occurs in the low-SDI region, where the burden profile shifts considerably: cervical and breast cancers lead for both genders combined, and leukemia becomes the top contributor for males—marking a distinct pattern compared to higher-SDI settings (Figure 3, eTable7 and eTable8).
3.3. Prediction of 32 malignant tumor groups (excluding NMSC) for age standard incidence rate (ASIR), age standard DALYs rates (ASDR), incidence number and DALYs number globally
Further, we predicted the rate and number of 32 malignant tumor groups (excluding NMSC) in the next 20 years by using the BAPC packages of the R software.
ASIR and incidence number showed rising trends in 7 and 19 malignant tumor groups, respectively; of which, colon and rectum cancer (rate, 36.04 to 38.97 and number, 2119417 to 2858829), breast cancer (rate, 34.46 to 44.67 and number, 2026608 to 3276457), prostate cancer (rate, 24.48-31.15 and number, 1286997-2081011), lip and oral cavity cancer (rate, 6.85-7.86 and number, 403077-576891), multiple myeloma (rate, 2.77-3.25 and number, 145852-217583), thyroid cancer (rate, 3.24-4.33 and number, 234518-373453), and testicular cancer (rate, 1.57-2.10 and number, 92770-154337) showed rising trends in both ASIR and incidence number from 2021 to 2041 (Figure 4, eFigure 1 and eTable10 including 95% UI). On the contrary, ASIR and incidence number showed decreasing trends in 10 and 2 malignant tumor groups, respectively; of which, stomach cancer (rate, 20.15-12.54 and number, 1185268-920043) and esophageal cancer (rate, 10.58-7.23 and number, 556431-483354) showed decreasing trend in both ASIR and incidence number (Figure 4, eFigure 1 and eTable10 including 95% UI). The rest 15 and 11 malignant tumor groups showed ambiguous trends respectively in ASIR and incidence number (Figure 4 and eFigure 1). Statistics and predictions of the 28/32 malignant tumor groups associated with ASIR and incidence number based on the BAPC model.
Most malignant tumor groups showed decreasing trends in ASDRs (21 malignant tumor groups) and DALYs numbers (6 malignant tumor groups), respectively. ASDRs and DALYs numbers showed rising trends in 2 and 9 malignant tumor groups, respectively; of which, other pharyxn cancer (rate, 51.34-54.24 and number, 2698340-3622510)and lip and oral cavity cancer (rate, 94.95-101.29 and number, 5583128-7429022) showed a rising trend in both ASDRs and DALYs numbers (Figure 5, eFigure 1). In addition, the rest 9 and 17 malignant tumor groups showed relative stable trends respectively in ASDRs and DALYs number (Figure 5, eFigure 1 and eTable11 including 95% UI). Statistics and predictions of the 28/32 malignant tumor groups associated with ASR-DALY and DALY number based on the BAPC model.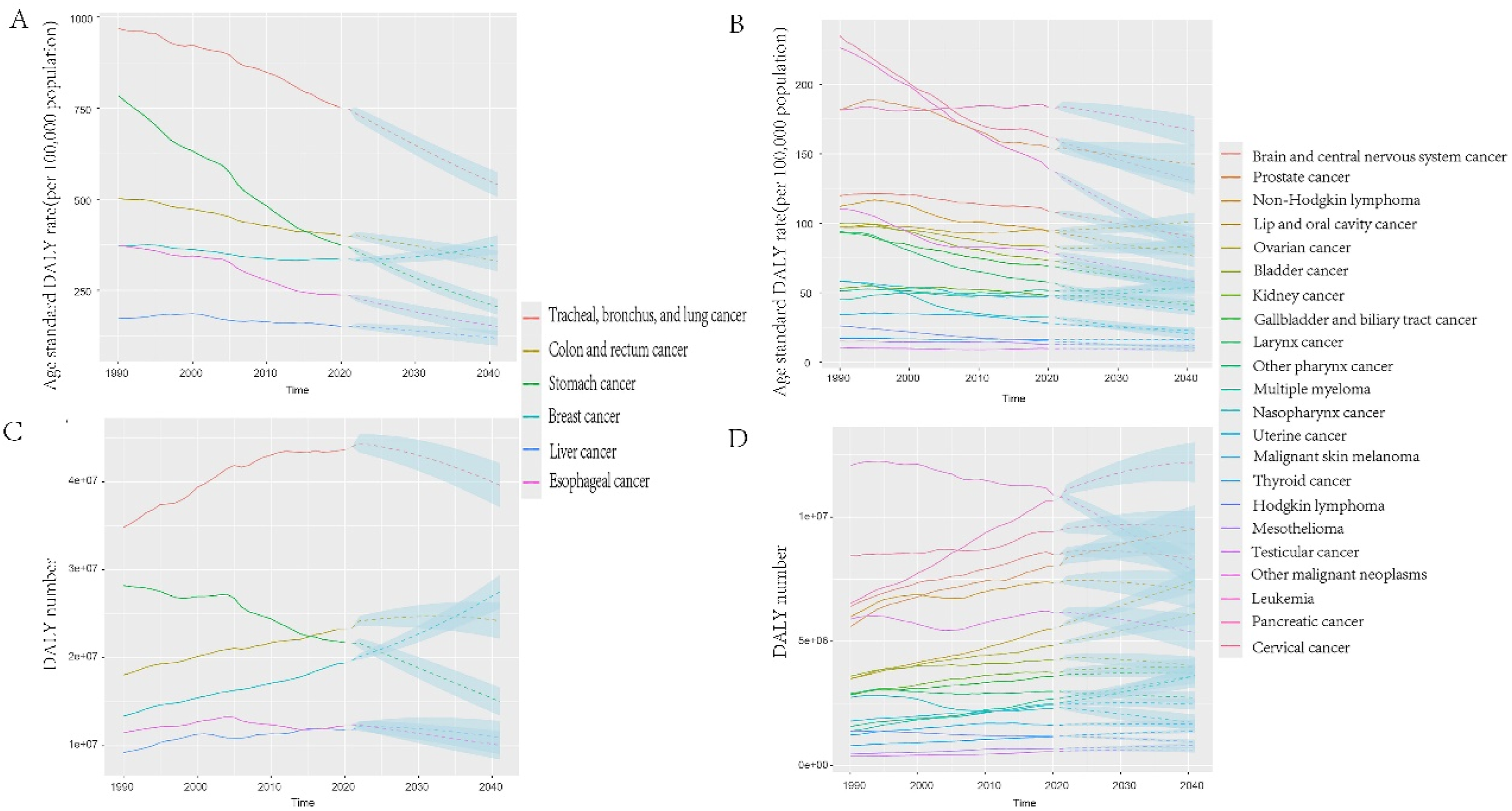
3.4. Prediction of 33 malignant tumor groups for absolute death numbers in 5 SDI areas
Comparing the BAPC model to the ARIMA model revealed that the majority of malignant tumor groups in high- and middle-SDI areas exhibited decreasing trends under the BAPC model; however, increasing trends were observed for most malignant tumor groups in these same areas (eTable9).
4. Discussion
The Global Burden of Disease 2019 Cancer Collaboration revealed that total malignant tumor groups were the second-highest cause of DALYs, deaths, and YLLs behind cardiovascular diseases. 1 The 2020–21 COVID-19 pandemic period placed an emphasis on mortality and DALYs of respiratory infections and tuberculosis, 12 led the total malignant tumor groups to the third-highest cause of DALYs in 2021 (Figure 1). Between 1950 and 2019, global age-standardised all-cause mortality rates per 100,000 population showed a broad decline. 12 A similar trend was observed in the age-standardised death rates (ASDRs) for malignant tumors, with 27 out of 33 groups exhibiting a decrease in percentage change, while the remaining 6 groups showed an increase (Figure 2).
The top four causes of DALYs among malignant tumor groups in 2021 were consistent for both sexes combined and remained unchanged from the rankings reported in 2019 (Figure 2) 1 : TBL, CRC, stomach, and breast cancer. Consistent with the study by Teng et al., 13 the burden of esophageal cancer continued to rise between 2019 and 2021, a trend likely attributable to population growth and aging. During this period, esophageal cancer also climbed in rank from the 6th to the 5th leading cause of cancer in terms of absolute DALYs (Figure 2).
The GBD database encompasses mortality and morbidity data from 204 countries and territories, categorized into 21 regions (Table 2). Based on death counts, TBL cancer ranked first in 15 of the 21 regions for both sexes combined and in 14 regions among males. In contrast, breast cancer was the leading cause of cancer mortality in 12 regions for females. Additionally, prostate cancer was the second most common cancer among men globally in 2020.6,14 Accordingly, in this study, prostate cancer ranked among the leading cancers in 13 of the 21 regions based on male incidence, and in 6 regions based on male mortality.
In 2021, though, COVID-19 increased the incidence and mortality of respiratory diseases, 12 total malignant tumor DALYs of the 22 diseases and injuries at Level 2 of the GBD cause hierarchy were still the first rank in the high SDI area (Figure 1). In areas with high SDI, the relative contribution of years lived with disability (YLDs) is greater, 5 which is part of DALYs number. And this is consistent with the fact that cancer screening,15,16 diagnosis,17,18 and treatment19,20 are usually more accessible in situations where SDI is increasing, thereby potentially improving survival outcomes and increasing the total DALYs number. In addition, many countries initially reported a decrease in newly diagnosed cancer cases during the height of the pandemic. This was largely attributed to the suspension of population-based cancer screening programs (e.g., for breast, colorectal, cervical cancers), reduced referrals from primary care, and patients’ reluctance to seek medical attention due to fear of infection and lockdown measures. 21
TBL, CRC, and breast cancer were among the top 3 most DALYs for both genders and females. Accordingly, TBL, CRC, and pancreatic cancer were the top 3 most DALYs for males in high SDI areas. Except for the low SDI area, TBL, CRC, stomach cancer, breast cancer, and cervical cancer ranked in the top 3 most DALYs accordingly in the other four SDI areas when taking gender into consideration (Figure 3). High-SDI countries have the oldest male populations; androgen receptor signaling in lung and pancreatic tissue accelerates malignant transformation in older men and interacts with tobacco carcinogens to increase mutation burden. 22 Smoking-attributable fractions for TBL cancer DALYs remain 70–75 % in high-SDI males despite decades of control programs. 22 Pancreatic cancer DALYs in the same quintile are 13.3 % attributable to smoking. 23
Our analysis identifies cervical and breast cancers as the leading causes of cancer DALYs among females in low-SDI regions, with incidence trends that are stable or rising. Hormonal milieu and reproductive factors significantly influence female-specific cancer risk patterns across the SDI spectrum. For breast cancer, the shifting reproductive trends now emerging in middle-SDI countries—characterized by earlier menarche, later age at first birth, and lower parity—elevate the lifetime duration of endogenous estrogen exposure, thereby increasing the risk of developing estrogen receptor-positive (ER-positive) tumors. 23
Our findings, stratified simultaneously by SDI and sex, suggest a strong joint effect of socioeconomic development and biological sex/gender in shaping cancer burden profiles. The divergent leading cancers for males and females in high-SDI settings, contrasted with the convergence towards infection-related and access-sensitive cancers in low-SDI settings, indicate that the impact of sex/gender is substantially modified by the developmental context.
Of particular concern, recent progress in reducing age-standardized incidence and mortality rates seems concentrated in higher SDI locations, whereas these rates continue to trend upward in many lower SDI locations. 1 The observed increases in age-standardized rates in lower SDI quintiles coincide with several concurrent phenomena, including demographic aging, likely improvements in cancer diagnosis and death registration, and changing population-level exposures to metabolic, behavioral, environmental, and occupational risk factors. For instance, the shifting global patterns of smoking prevalence by SDI quintile represent a key risk association relevant to the cancer burden profile, 24 underscoring the ongoing need for enhanced tobacco control initiatives.25,26 Correspondingly, the ranking of the top three causes of cancer DALYs in low-SDI areas differed from other regions: for both genders combined, the leaders were cervical cancer, breast cancer, and leukemia; for males, leukemia, stomach cancer, and prostate cancer; and for females, cervical cancer, breast cancer, and stomach cancer (Figure 3).
Compared with 2019, there were four additional malignant tumor groups included in GBD 2021: malignant neoplasm of bone and articular cartilage, soft tissue and other extraosseous sarcomas, eye cancer and neuroblastoma, and other peripheral nervous cell tumors. Therefore, there were 32 third-level malignant tumor groups excluding non-melanoma skin cancer (NMSC). The BAPC model predicted that from 2021 to 2041, stomach cancer and esophageal cancer showed decreasing trend in both ASIR and incidence number. Compared with Western regions, East Asia bears a higher burden of stomach and esophageal cancer; however, a consistent decreasing trend in both cancers has been observed in this region. 27 In this study, colon and rectum cancer, breast cancer, and prostate cancer all exhibited an increasing trend in both ASIR and absolute incidence number, consistent with the findings reported by Bray et al. 28 Moreover, thyroid cancer, lip and oral cavity cancer, multiple myeloma and testicular cancer showed rising trend in both ASIR and incidence number (Figure 5, eFigure 1). We project a rising trend in both ASIR and incidence for thyroid cancer to 2041. This finding is consistent with the established paradigm of overdiagnosis described by Kitahara and Davies.29,30 Our projection suggests that without modifications in diagnostic practices, the epidemic of detected—though not necessarily lethal—thyroid cancer is likely to persist, particularly in regions with expanding access to ultrasound and biopsy. O’Sullivan et al. reported that the increase in oral cavity and lip cancer since 1990 was largely attributed to population growth and aging. 31
HPV vaccination demonstrates high effectiveness in preventing cervical cancer, especially when administered during early adolescence, which induces robust and durable immune responses. 32 The BAPC model also reveal a critical disparity: while cervical cancer age-standardized death rates (ASDRs) are decreasing globally and in high-SDI areas, the absolute number of deaths continues to rise in low- and middle-SDI regions. This finding directly aligns with and extends the 2023 study by Singh et al. 33 The predicted decreasing trend for cervical cancer age-standardized death rates (ASDRs) in high-SDI areas is temporally consistent with the rollout of HPV vaccination and screening programs in these settings. Therefore, combining our burden data with this established evidence for effective interventions, we suggest that strengthening prevention and early detection strategies for cervical and breast cancer should be a key consideration for health systems in low-SDI settings.
A key limitation in interpreting incidence trends, particularly in low- and middle-SDI regions, is the potential confounding effect of improving cancer surveillance infrastructure. The rising age-standardized incidence rates we observe for several cancers in these settings may partially reflect increased case ascertainment due to expanded access to diagnostic imaging, pathology services, and population-based registries, rather than—or in addition to—a genuine increase in cancer risk. Disentangling these contributions is challenging with aggregate data. Therefore, mortality and DALY rates, which are less susceptible to pure surveillance bias, may offer a more stable metric for tracking the underlying disease burden in contexts where health system capacity is rapidly evolving.
TBL cancer remains the dominant driver of cancer mortality worldwide, particularly among males.
Breast cancer shows remarkable consistency as the leading female-specific cancer across most regions by both incidence and mortality. While several cancers contribute significantly to global DALYs, their regional dominance patterns vary substantially, reflecting different epidemiological transitions and risk factor distributions.
The regional rankings in Table 2 are not random but largely stratify along the SDI gradient we describe. The high-SDI pattern (TBL/CRC/breast) is evident in Western Europe and High-income Asia Pacific, while the low-SDI pattern (cervical/breast/prostate with infection-related cancers) is clear in Sub-Saharan Africa and parts of South Asia. This reinforces that SDI is a powerful, though imperfect, predictor of a region’s cancer profile.
The distinct patterns of cancer burden across SDI quintiles, genders, and specific cancer types, as detailed in this analysis, necessitate equally nuanced policy responses. Moving beyond a “one-size-fits-all” approach, we propose the following priority considerations for future policymaking: In high-SDI regions, policy should sustain progress against TBL cancer (notably in males) and colorectal cancer through robust tobacco control and optimized screening, while addressing rising burdens like pancreatic cancer. In low- and middle-SDI regions, foundational investments are critical: scaling up vaccination and implementing feasible, cost-effective early detection to counter the high burden from infection-related and gender-specific cancers. A cross-cutting priority is strengthening cancer surveillance, as improved diagnosis and registration may partly explain rising incidence rates in these settings, making mortality and DALY rates vital for tracking true burden.
This study had some limitations, providing opportunities for improvement in future GBD iterations. First, the analysis heavily relied on the GBD database which whose accuracy is constrained by the availability of national registry data. The GBD addresses these data limitations through data-seeking efforts, data processing corrections, and modeling approaches that incorporate geospatial and temporal smoothing. 1 Second, the forecasting model used in this study was the BAPC model and ARIMA model. The Nordpred model was not used. 9 Third, this study did not incorporate the COVID-19 pandemic with global cancer morbidity and mortality, as a previous study did. 12 Fourth, while our analysis descriptively reveals distinct cancer burden patterns by SDI and sex through stratified presentation, we did not perform a formal statistical test for interaction between SDI and sex in a multivariate model. Such an analysis would quantify the significance and strength of this modifying effect and represents a valuable avenue for future research.
5. Conclusions
This study confirms that the global cancer burden is stratified by socioeconomic development (SDI), gender, and cancer type. High-SDI regions are dominated by lung (TBL) and colorectal cancers, while lower-SDI regions face a greater burden from gender-specific and infection-related cancers. These disparities demand divergent strategies: advancing precision management in well-resourced settings versus building foundational prevention and early detection where resources are constrained. Lung cancer remains the leading driver of mortality, especially among males, necessitating reinforced tobacco control. The dominance of breast cancer in females and the heavy burden of cervical cancer in low-SDI areas are critical targets for gender-sensitive prevention. Future efforts must leverage these specific insights to allocate resources efficiently and implement context-appropriate interventions.
Supplemental material
Supplemental material - Burden of 33 malignant tumor groups in 5 socio-demographic index areas and 21 regions from 1990 to 2041
Supplemental material for Burden of 33 malignant tumor groups in 5 socio-demographic index areas and 21 regions from 1990 to 2041 by Chengyun Dou, Yidan Sang, Lirong Huang and Chuangjie Cao in Science Progress.
Footnotes
Acknowledgements
This study was generously supported by Jingding Medical Tech, to whom we extend our sincere gratitude. We especially thank them for providing authorization and technical support for the JD_GBDR software. The team at Jingding Medical Tech offered invaluable assistance in data processing.
Ethical considerations
GBD data made available for download on IHME Websites can be used, shared, modified or built upon by non-commercial users in accordance with the IHME FREE-OF-CHARGE NON-COMMERCIAL USER AGREEMENT (![]() ). The GBD study is based entirely on publicly available databases and does not require clinical ethics approval.
). The GBD study is based entirely on publicly available databases and does not require clinical ethics approval.
Consent to participate
The GBD study is based entirely on publicly available databases and does not require clinical ethics approval.
Author contributions
Chuangjie Cao and Chengyun Dou: Conceptualization, Supervision, Writing-review & editing; Lirong Huang: Draft preparation, Software; Yidan Sang: Statistic analysis, Data Preparation and Curation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was funded by Hunan Natural Science Foundation, NO. 2025JJ70166 and NO. 2025JJ70165.
Declaration of conflicting interests
All authors hereby attest that they do not have any conflicts of interest related to this article.
Data Availability Statement
Research data and other items supporting the results in this article are available upon reasonable request to the corresponding author.
IRB approval
Institutional Review Board (IRB) approval: We have checked this with our review board and received exemption.
Supplemental material
Supplemental material for this article is available online.