
Abstract
The study aimed to analyze morphometric assessment of the mesorectal fat thickness and its correlation with body mass index in Chinese Han population. The anterior, posterior, right lateral, and left lateral mesorectal fat thickness were measured using MRI T2-weighted images. The mean distance from the rectal wall to the mesorectal fascia were 3.8, 8.4, 11.3, and 11.7 mm in anterior, posterior, right lateral, and left lateral portion, respectively. The mesorectal area, rectal area, mesorectal fat thickness area, and rectal height were 2395.3 ± 691.1 mm2, 709.6 ± 403.5 mm2, 1685.7 ± 525.3 mm2, and 9.1 ± 0.8 cm. BMI was found to be directly proportional to and statistically significant to the mesorectal fat area (p = 0.01). Since the mean mesorectal fat thickness was found to be <12 mm, T3d staged rectal cancer is less likely to be found in an average Chinese population that may affect the overall-survival and progression-free survival in rectal cancer patients. Anterior portion of the rectum was least thick compared to all other sides. Therefore, extra-caution should be taken in handling tumors on the anterior part of the rectum.
Introduction
The rectum is surrounded by loose perirectal tissue and the mesorectal fat. A thin enveloping visceral perirectal fascia binds the mesorectal fat within the mesorectal fascia (MRF). Rectal cancer is not only the third most common form of cancers but is also one of the leading causes of cancer related deaths in the world.1,2 The presence of tumor cells within 1 mm of circumferential resection margin (CRM) is associated with reduced overall survival and increased rate of local recurrence compared with uninvolved CRM.3–5 Involvement of CRM and MRF is highly influenced by the thickness of the mesorectal fat. The European Society for Medical Oncology (ESMO) guideline sub-classifies T3 rectal cancer into T3a (<1 mm), T3b (1–5 mm), T3c (5–15 mm), and T3d (>15 mm) according to the depth of mesorectal extension beyond muscularis propria. The depth of mesorectal extension alone has been shown to be an important independent prognostic factor in rectal cancer. 6 Mesorectal fat area has also been proven to be one of the useful predictors for the difficulty of robotic assisted laparoscopic total mesorectal excision (TME) surgery for rectal cancer.7–9 Regardless of the importance and popularity of the mesorectum, only a few morphometric studies have been performed to understand the differential thickness of mesorectal fat.
Due to the high sensitivity, reproducibility, accuracy and feasibility of MRI, it is considered as the choice of imaging modality in rectal cancer.10–15 The tumor height, local staging, and the depth of mesorectal extension can be predicted with high accuracy using MRI.16,17 The radiological landmark “sigmoid take-off” is the most commonly chosen definition for rectum 18 (Figure 1(a) and (b)). The sigmoid take-off identifies the junction of the sigmoid colon with the rectum; therefore, it is considered as the proximal end of the rectum. To ensure that the patient gets the optimum treatment, efforts have been made by the radiologists to convey accurate information about the tumor height and relation of the tumor with the MRF to the surgeons and oncologists.

(a) Sagittal view of rectal height using MRI and (b) axial view of rectum and sigmoid take-off using MRI.
Today, ESMO and/or NCCN guidelines are followed globally for the cancer management.19,20 These guidelines are mostly based on the European/American studies and their population. But there is evident difference in the fat deposition between the Asian and Caucasian population 21 ; this could be the result of differences in the body build, body habitus, physical activities, and energy intake.22,23 Since the Asians have comparatively small body build than Caucasians, we hypothesized the mesorectal fat to be lesser in Chinese Han population.
The purpose of the study was to analyze the morphometric mesorectum (i.e. the distribution of mesorectal fat) and its correlation with BMI and also to evaluate anthropometric definition (i.e. measured height) of rectum using high resolution MRI in Chinese Han population.
Methods
This retrospective study was approved by the Institutional Review Board and the requirement for formal informed consent was waived off from all patients. A consecutive cohort of 939 patients undergoing pelvic MRI scans from March 2016 to March 2018 at our institution were identified. The primary inclusion criterion was Han ethnic group Chinese patients admitted in our institution. The patients were excluded if presented with enlarged pelvic mass, prostrate, or uterus that affected the normal anatomy of mesorectum, history of abdominopelvic surgery, or radiation therapy prior to the MRI examination, history of other malignancies and patients treated as outpatient. The process of data collection and evaluation is shown in the flowchart below (Figure 2).

Flowchart for patient enrolment.
MRI technique and imaging acquisition
Pelvic MRI examinations were performed using 3.0T scanner (Discovery 750, GE Healthcare, Milwaukee, WI) with a 32-channel torso coil (phase-array body coil) in the supine position.
The following imaging sequences were used: sagittal T2 fast spin echo (FSE) (TR/TE, 5310/113 ms; matrix size, 320 × 320; slice thickness, 3 mm; intersection gap, 0 mm; and field of view, 250 × 250 mm2) and axial T1 fast spin echo (FSE) (repetition time [TR]/echo time [TE], 500/11 ms; matrix size, 320 × 224; slice thickness, 5 mm; intersection gap, 1 mm; and FOV 320 × 380 mm2), axial T2 FSE sequence (TR/TE, 4050/85 ms; matrix size, 320 × 324; slice thickness, 5 mm; intersection gap, 1 mm; and field of view, 380 × 380 mm2) together with oblique high resolution axial and coronal T2 FSE sequences (TR/TE, 5629/85 ms; matrix size, 448 × 314; slice thickness, 2 mm; intersection gap, 0 mm; and field of view, 200 × 200 mm2).
A computerized radiologic database was used for patient selection and image analysis. All images were evaluated using RIS workstation with a Coronis monitor. Measurements were made with mutual agreement between the two reviewing radiologists (10 and 4 years of experience in pelvic MRI). A third radiologist (with over 15 years of abdominal MRI examination experience) was invited to review the image whenever there was disagreement between the former two radiologists.
The distance was obtained in true axial plane at the levels of 5.0, 6.5, and 9.0 cm from the anal verge. The objective of selecting these three arbitrary levels was to measure the mesorectal thickness in lower, middle, and upper rectum. 24 Majority of the patients were found to have 9.0 cm as the least rectal height; therefore, this point was chosen to be end point of upper rectum. The height of the rectum was defined as the total length from the anal verge to the posterior end point of the rectosigmoid junction, “ the sigmoid take-off,” along the midline throughout rectum (Figure 1(a) and (b)).18,25
Mesorectal fat thickness and mesorectal fat area
The distance from the rectal wall to the MRF in the axial plane was considered to be the mesorectal fat thickness. Four readings were obtained at each level; namely: anterior, posterior, right lateral, and left lateral (Figure 3(a) and (b)). By employing the workstation specific software, the area of mesorectum was obtained using a mouse to draw a free hand region of interest (ROI) along the MRF and rectal wall that was determined by the naked eyes. At first, the total area within MRF was calculated and then the area of rectum along the outer border was calculated. Finally, the area of rectum was deducted from the total area to obtain the mesorectal fat area (Figure 4). To calculate the maximum area of mesorectal fat, level of 9.0 cm from the anal verge was chosen. Body mass index (BMI) was also noted and categorized using a cutoff value of 24 kg/m2 which is regarded as optimum BMI cutoff value in Chinese adults. 26

(a) Axial view of mesorectum using MRI and (b) axial view of mesorectum using MRI.

Axial view of mesorectal fat thickness using MRI.
Statistical analysis
The SPSS software package version 11.0 (SPSS, Inc., Chicago, IL) was used for statistical analysis for this study. Groups were compared using Student’s t test for continuous variables and the chi square test for categorical variables. The mesorectal area, rectal area, mesorectal fat thickness, and rectal height were all measured.
Results
A total of 549 axial MRI images were obtained to measure the mesorectal fat thickness. A total of 183 patients (36 female and 147 male) with the age of 57.26 ± 12.06 years at the time of MRI examination were included in this study among which 96 patients were histologically proven to have rectal carcinomas. The mean rectal height was 9.1 ± 0.8 cm. The mean rectal height was 9.1 ± 0.8 cm.
Quantitative analysis
The mesorectal fat thickness at 5, 6.5, and 9 cm from the anal verge are shown in Table 1. Anterior part of rectum was the least thick amongst all three levels whereas the left lateral part was the thickest of them all on all three levels. The mesorectal area, rectal area, and mesorectal fat thickness area were 2395.36 ± 691.1 mm2, (95% CI 2258.2–2532.5), 709.6 ± 403.5 mm2 (95% CI 629.5–798.7), and 1685.7 ± 525.5 mm2 (95% CI 1581.4–1789.9), respectively (Table 2). The mean height of the rectum was 9.1 ± 0.8 cm (95% CI 9.01–9.35) ranging from 9.0 to 12.6 cm. The mesorectal fat thickness in male and female were 1722.9 ± 519.5 mm2 and 1516.0 ± 534.0 mm2, respectively (Table 3). Although the mesorectal fat thickness was comparatively lesser in the females, independent sample t-test revealed it to be statistically not significant (p = 0.79). The correlation between age and mesorectal fat thickness using independent sample test was statistically significant (p = 0.02, 95% CI 0.71–10.53). Similarly, the correlation between mesorectal fat thickness and BMI was also statistically significant (p = 0.010, 95% CI 1.29–10.10). Finally, using multivariate analysis, BMI was found to be statistically significant (p = 0.01, 95% CI 1.06–1.66) with mesorectal fat thickness. The measurements according to the BMI in the patient population are as shown in Table 3.
Morphologic assessment of mesorectal fat thickness at different levels of rectum.

Range, median, and standard deviation of the mesorectal fat thickness on anterior, posterior right lateral, and left lateral on 5, 6.5, and 9 cm from the anal verge along with overall measurements.
Distribution of rectal height and mesorectal parameters according to gender and BMI.
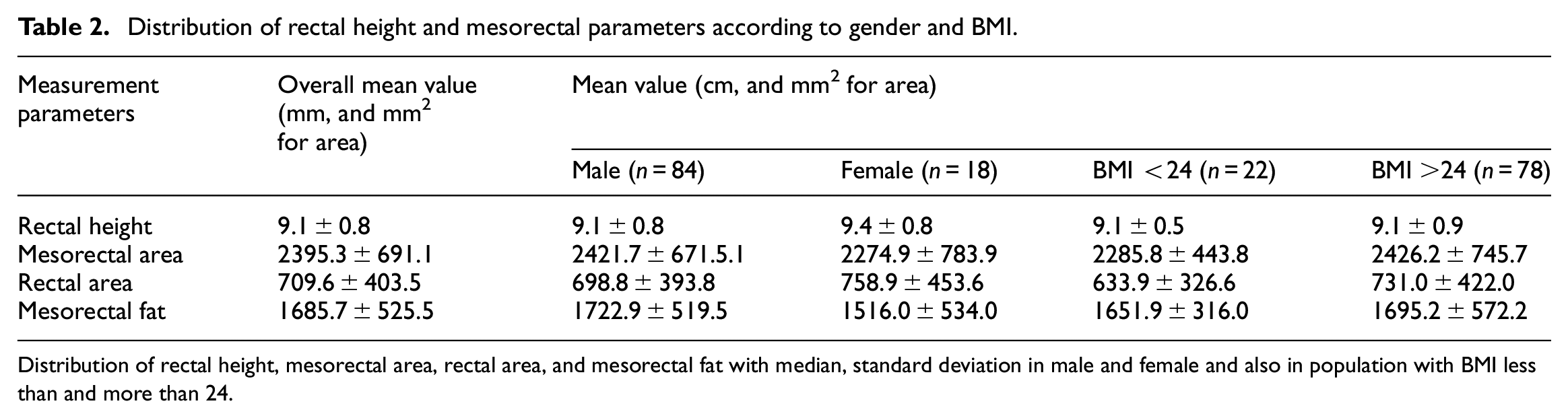
Distribution of rectal height, mesorectal area, rectal area, and mesorectal fat with median, standard deviation in male and female and also in population with BMI less than and more than 24.
Correlation of parameters with mesorectal fat thickness in overall population.
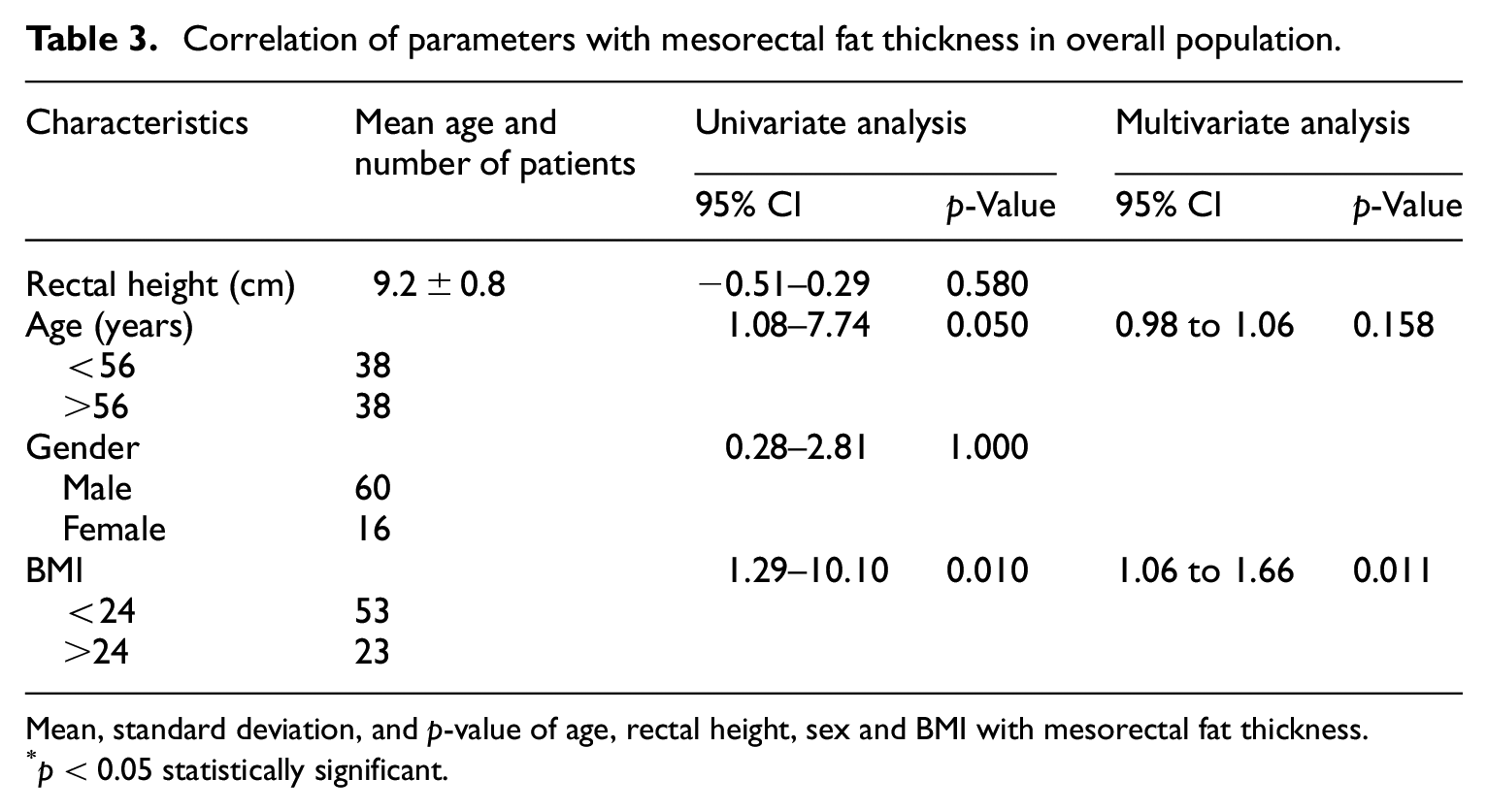
Mean, standard deviation, and p-value of age, rectal height, sex and BMI with mesorectal fat thickness.
p < 0.05 statistically significant.
Discussion
The prognosis of rectal cancer is proportional to the depth of mesorectum invasion and involvement of MRF.3,27 Majority of currently available studies on rectum and rectal cancer specifically target cancer risk factors or post-treatment effects.15,28 Very few studies on the morphology of mesorectum are found; of which, majority of them are predominantly based on European population.29,30 The morphology of the mesorectum and mesorectal fat thickness in Chinese population still remains unclear. The average body-build, body habitus, height and weight between western and Asian populations have distinct variations. Today, a large number of Chinese populations have migrated and scattered in different parts of the world. Identification of mesorectal fat thickness in Chinese population is very crucial. It will facilitate the development of novel therapies and may result in better prognosis to currently available therapies among Chinese patients globally. To the best of our knowledge, this is the first study with such large sample size, describing the mesorectal fat thickness in Chinese population. This study adds to the knowledge of applied anatomy of mesorectum, mesorectal fat thickness and rectum height in Chinese population. The measurement we have described with the use of MRI may assist surgeons and clinicians to commence on personalized treatment strategy for China origin patients with rectal cancer.
In this study, we measured mesorectal fat thickness and the area of mesorectum. Adding four measurements in each three levels, the average mesorectal area, and mesorectal thickness were obtained. Some previous studies have used only a single point to measure the mesorectal fat area.29,30 We believe it is less convincing to use a single point to represent the whole mesorectal fat thickness of rectum. Therefore, to prevail over this issue, we choose single point from upper, middle, and lower rectum to average the mesorectal fat area. We believe the average mesorectal fat area obtained from all parts of rectum would be more accurate compared to a single point area. The average distance from the rectal wall to the MRF was 3.87, 8.48, 11.33, and 11.73 mm in anterior, posterior, right lateral, and left lateral portion respectively. The anterior portion of the rectum was least thick in all three levels; the study by Torkzad et al. also reported similar result with 3.03 mm in European population and is consistent with our findings. 30 A similar study by Wong et al. also reported that the anterior part was the least thick with 2.5 mm in T3 rectal cancer patients. 31 Although their results were consistent with our study, the overall mesorectal fat thickness was comparatively lesser in previous studies. Small sample size might have been the major contributing factor for such result in their studies.
In supine position, the anterior portion of the mesorectum gets compressed by the pelvic organ (uterus or prostate). Additionally, the available free space is also lesser in the anterior portion when compared with rest of the sides. These might be the reasons for the anterior portion to have the least thickness. As it approaches closer to the anal verge, the mesorectal fat gets thinner. Based on our data, we propose that the even the T3b tumors located on the anterior portion of the rectum have higher risk of MRF invasion compared with the same or even bigger sized tumor in any other portion of the rectum. Given that the same depth of tumor invasion on all sides of the rectum, the area with thin fat buffer may have poor prognosis compared with the area with thick fat buffer or we could even assume that the patients with thin mesorectal fat buffer may have poor prognosis compared with the patients with thick mesorectal fat buffer (Figure 5). The mesorectal fat in the lower rectum was thin when compared with mid and upper rectum. The risk of CRM involvement in the lower rectum is distinctly higher. Some previous studies have reported higher local recurrence with CRM involvement in the lower rectum, resulting in poor prognosis when compared with the mid and upper rectum.32,33

Schematic presentation of mesorectal fat thickness and rectal tumor.
Recently, the use of 5 mm as a cutoff value to differentiate early and advanced rectal cancer is highly accepted. 34 Some studies concluded that the tumors with distance of mesorectal extension >5 mm have poor prognosis compared with <5 mm.16,35 Many previous studies have investigated the prognosis of T3 subdivision using various cutoff points (4, 5, and 6 mm) and have concluded that the deeper the tumor invasion is, the worst the prognosis becomes.35–38 Among all of these studies mentioned above, only a few of them have mentioned MRF involvement status but none of them have included the mesorectal thickness or mesorectal fat buffer. We believe the prognosis and the survival rates obtained by considering the mesorectal fat thickness is more accurate. The MRF involvement status only describes the status at that certain time period, but the mesorectal fat buffer helps to predict the remaining mesorectal distance (distance of tumor edge to MRF) for MRF involvement in CRM-negative patients.
A previous study concluded that mesorectal size has no correlation with BMI. 39 But in contrast to the result, our study revealed a statistically significant correlation between BMI and mesorectal fat thickness. Obesity is considered as one of the crucial risk factors for many types of cancer, especially for colorectal cancer. 40 This also means that the risk of rectal cancer may increase in the patients with thick mesorectal fat buffer.
There have been considerable debates over the measurement of exact height of the rectum. The variation of haustral convergence, body size, curvature of rectum, and sex may influence the rectal height. Radiologically, with the use of MRI, the anal verge, point of peritoneal reflex, and rectosigmoid junction “sigmoid take-off” is clearly seen; which benefits the rectal height measurement. Wide variations in the rectum height ranging from 12 to 19 cm have been reported in literatures.41–43 When compared with those reports, the height of rectum in our study population varied distinctly. The average rectal height was 9.2 ± 0.8 cm (ranging from 9.0 to 12.6 cm). American, 44 Dutch, 45 and German 46 studies used the distance of 12, 15, and 16 cm from the anal verge respectively for the rectum. However, in our study population the rectum had ended before these landmarks in about 98% of the patients. As mentioned above the difference in body build, energy intake, and physical activities might be the probable cause. In our study, the average mesorectal fat area was 1722.9 ± 519.5 mm2 in males and 1516.0 ± 534.0 mm2 in females. In previous studies, the average mesorectal fat thickness area was 2562 ± 770 mm2 in male and 1842 ± 830 mm2 in females.7,29 In agreement with previous studies, similar difference of mesorectal fat area between different sexes was observed in our study, however, when compared with previous studies we found a distinctly lesser average mesorectal fat area. There are some relevant previous studies aimed to study the mesorectal fat thickness but were not race or ethnic specific.29,30 Case reports and small sample size were major limitations of the previous studies.29–31,39 To overcome this pitfall, we enrolled large number of patients compared with previous studies and conducted an observational study.
There are some limitations in our study that warrants few considerations. First, given the retrospective nature of this study, some potentially helpful data were not collected at the time of examination and are thus omitted from the data set. Second, the study is not a large-scale randomized trial and comprised data from only one center. But in our defense, the aim of this study was to understand the maximum potential mesorectal fat thickness in specific race of population.
The findings from our study are very crucial to the current rectal clinical practice. The current treatment guideline for rectal cancer is based on the American and European population. The purpose of this study was not to criticize the current treatment guidelines but to encourage adopting personalized treatment as the variation of mesorectal fat thickness could be observed within the Chinese population. This study may facilitate the development of novel therapies and result in better prognosis to currently available therapies in Chinese population. In future, multicenter studies with large population may support our results and provide additional evidences. The studies investigating mesorectal fat thickness to predict prognosis in rectal cancer and also treatment effects in variety of mesorectal fat thickness in rectal cancer might result in new perspective for mesorectal fat thickness and treatment modality for rectal cancer. Also, the correlation of BMI and mesorectal fat thickness has opened the door for new research. As mentioned above, some previous studies concluded obesity or overweight as a risk factor for colorectal cancer. If so, does the incidence of rectal cancer increase in the patients with thick mesorectal fat? This might be the aim of our future study.
In conclusion, mesorectal fat thickness and the height of the rectum are important parameters from the surgical standpoint. Preoperative determination of the accurate mesorectal fat thickness and rectal height may lead to more accurate surgical qualification in rectal cancer treatment. The T3d staged (>15 mm) rectal cancer is less likely to be found in an average Chinese population. This may result in the variation in the overall-survival and progression-free survival rates in Chinese patients. Anterior mesorectal fat is least thick in all three levels. Even T3b (1–5 mm) tumors located on the anterior portion of the rectum have higher risk of MRF invasion compared with the same or even bigger sized tumor in any other portion of the rectum. In this era of precise medicine, such results might encourage us to develop novel treatment and management strategy in Chinese origin patients.
Footnotes
Author contributions
Dr. Tripathi Pratik developed the original idea and the protocol, abstracted, and analyzed data, wrote the manuscript. Dr. Yucheng Hai, Dr. Zhen Li, Dr. Yaqi Shen, Dr. Xuemei Hu, and Daoyu Hu contributed to the development of the protocol, abstracted data, drafted, and revised the manuscript. All authors are in agreement with the content of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the [National Natural Science Foundation of China] under Grant [number 81571642]; [National Natural Science Foundation of China] under Grant [number 81701657]; [National Natural Science Foundation of China] under Grant [number 81771801]; and [National Natural Science Foundation of China] under Grant [number 81801695].