
Abstract
Odontogenic cysts are well-known maxillofacial pathologies with variable biological behaviour. Decompression has been widely used as a conservative, structure-preserving management strategy. This report presents a radiographic comparison of reduction patterns following decompression in two individual cases, one dentigerous cyst and one odontogenic keratocyst. Two patients presenting with cystic jaw lesions – one detected during radiographic investigation and the other presenting with progressive swelling – were managed using decompression as the initial treatment. Standardised radiographic measurements were performed, and the Standard Lesion Area Index and Percentage of Reduction were calculated at serial follow-up intervals. The dentigerous cyst demonstrated gradual reduction, achieving 94.4% shrinkage at 12 months and complete radiographic resolution by 44 months, with no radiographic evidence of recurrence. In contrast, the odontogenic keratocyst showed a more rapid initial reduction, with 58% shrinkage at 5 months, followed by a plateau at approximately 90% shrinkage by 24 months and radiographic evidence of recurrence at 44 months. Direct long-term radiographic comparison of dentigerous cyst and odontogenic keratocyst reduction following the same decompression protocol remains limited in the published literature. The literature synthesis indicated that decompression typically requires 8 to 24 months, with dentigerous cysts generally demonstrating more favourable radiographic responses than odontogenic keratocysts. Decompression and marsupialisation are non-definitive approaches, as definitive management requires subsequent enucleation of the lesions. These case-based observations suggest that decompression may be sufficient for selected dentigerous cysts, whereas odontogenic keratocysts require prolonged monitoring and are more likely to necessitate secondary surgical intervention. The findings should be interpreted cautiously in view of the very small number of cases.
Keywords
Introduction
Odontogenic cysts are distinct pathological entities confined to the oral and maxillofacial region, arising from epithelial remnants of the tooth-forming apparatus. In the fifth edition of the World Health Organization Classification of Head and Neck Tumours (2024), the odontogenic keratocyst, which was previously termed keratocystic odontogenic tumour in 2005, is currently classified among jaw cysts. This lesion is recognised as a locally aggressive developmental cyst, typically involving the mandible or maxilla and is characterised by a high tendency for recurrence. 1
In a United Kingdom population-based epidemiological analysis of 55,446 oral pathology samples, 7121 cases (12.8%) were identified as odontogenic cysts, with odontogenic keratocysts representing approximately 11.6% of these cases. 2 Epidemiological data demonstrate a bimodal age distribution, with incidence peaks in the third and sixth decades of life. A male predominance is consistently reported, with an overall male-to-female ratio of approximately 2:1, a disparity that appears less marked in White populations but exceeds 2:1 among Black individuals. 3
Multiple treatment strategies have been described in the literature, each associated with varying risks of recurrence and morbidity. Radical resection achieves the lowest likelihood of recurrence but is accompanied by considerable morbidity. In contrast, simple enucleation is associated with reported recurrence rates ranging from 17% to 56%, while the addition of adjunctive measures, such as Carnoy's solution or prior decompression, reduces recurrence to between 1% and 8.7%. 4 A multicentre study reported that enucleation combined with curettage or peripheral ostectomy was the most frequently employed approach, with an overall recurrence rate of approximately 9%. 5 Conversely, decompression or marsupialisation performed as sole interventions has generally been associated with less favourable long-term control. 5 A network meta-analysis suggested that enucleation with peripheral ostectomy and topical 5-fluorouracil may offer the most effective outcomes, although the quality of evidence was low to moderate, and no statistically significant differences were observed among several compared protocols. 6
Cyst decompression is a conservative surgical approach that reduces intracystic pressure by creating and maintaining a communication between the cystic cavity and the oral environment using a decompression device. 7 This technique facilitates gradual lesion shrinkage, promotes bone regeneration, and helps preserve adjacent anatomical structures. 7
The present report aims to compare radiographic reduction patterns following decompression in two individual cases, namely a dentigerous cyst and an odontogenic keratocyst, using radiographic change in lesion size as the primary outcome measure. This report addresses the following focused research question: ‘In patients with odontogenic keratocysts, what are the reduction rate (RR) and treatment duration following decompression or marsupialisation?’. Longitudinal radiographic comparisons of reduction dynamics between dentigerous cysts and odontogenic keratocysts following decompression are not commonly reported in the literature, particularly with extended follow-up beyond 2 years. By presenting two contrasting cases managed with an identical decompression protocol and followed for up to 44 months, this report provides a detailed comparative insight into lesion-specific reduction behaviour and long-term radiographic outcomes, thereby contributing additional case-based evidence to support clinical decision-making.
Case presentation
Case selection
This report presents a comparative of two patients; one diagnosed with a dentigerous cyst and the other with an odontogenic keratocyst. Both cases were initially managed using decompression, and longitudinal radiographic assessments were performed to evaluate treatment outcomes over time. Patient perspectives on the treatment experience were not obtained and are therefore not included in this report.
Radiographic evaluation
Digital panoramic radiographs were obtained for each patient at baseline (pre-operative) and at standardised postoperative follow-up intervals. For both cases, radiographic imaging was performed at 5-, 12-, 24-, and 44-month following decompression.
Standardised radiographic reference points
Cyst dimensions were assessed using four standardised radiographic reference points. The Superior Point was defined as the most superior visible margin of the cyst, located near the alveolar crest. The Inferior Point referred to the lowest visible extent of the lesion, approaching the inferior border of the mandible. The Mesial Point was designated as the most anterior margin of the cyst, typically adjacent to the distal root of the nearest tooth. The Distal Point marked the most posterior extension of the cyst, often directed toward the mandibular ramus. These standardised reference points enabled consistent and reproducible measurement of the lesion's vertical and horizontal dimensions across serial radiographic follow-up.
Measurement definitions
Vertical Height was measured as the linear distance from the Superior Point to the Inferior Point, oriented perpendicularly to the occlusal plane.
Horizontal Width was defined as the distance between the Mesial Point and the Distal Point, measured along a line parallel to the occlusal plane.
Calibration and accuracy
To improve measurement precision, separate correction factors were applied for the vertical and horizontal dimensions due to potential non-uniform distortion in panoramic radiographs. Correction factors for each follow-up radiograph were calculated using the baseline radiograph as the reference standard. For dentigerous cyst case, the adjacent mandibular left second molar (LL7) was used as the reference structure. The horizontal correction factor (CFₕ) was calculated based on the mesiodistal crown width of LL7, while the vertical correction factor (CFᵥ) was based on the vertical height of the tooth, measured from the distal cusp tip to the apex of the root. These corrected values were applied respectively to the measured width and height of the lesion before calculating the Standard Lesion Area Index (SLAI). For odontogenic keratocyst case, the adjacent LL7 was excluded due to the presence of caries. Instead, the maxillary left second molar (UL7) was used for both vertical and horizontal calibration. The same method of deriving CFₕ and CFᵥ was applied using UL7. This strategy ensured that both height and width measurements reflected true anatomical proportions, allowing more accurate assessment of lesion size reduction.
Reduction rate assessment
To quantify the reduction in cyst size over time, the SLAI method, as described by Anavi et al., 8 was applied. This method calculates the estimated lesion area by multiplying the maximum vertical height by the maximum horizontal width, with both measurements recorded in millimetres. The resulting SLAI (in mm2) provides a reproducible approximation of the lesion's surface area. By converting the irregular shape of the cyst into a rectangular measurement, this method facilitates consistent comparison across follow-up radiographs: (SLAI = Maximum height (mm) × Maximum width (mm)). Percentage of Reduction (POR) is then calculated to determine the extent of shrinkage following decompression: (POR = ((Initial SLAI − Final SLAI) / Initial SLAI) × 100).
RR was also calculated by dividing the duration of decompression (in months) by the POR. This time-adjusted index offers a practical measure of the rate at which lesion size decreased during the observation period: (RR (months per % reduction) = Duration of decompression (months) / POR (%)).
Radiographic reduction response was classified according to the criteria proposed by Nakamura et al. 9 : (i) Good response: ≥80% reduction, (ii) Moderate response: 50 to 80% reduction, (iii) Poor response: <50% reduction. Measurements were performed using SCANORA® 5.2.6 software, with calibration based on stable anatomical landmarks to minimise the effects of image distortion. One examiner performed the measurements twice at two different time intervals to minimise any intra-observer discrepancy, and the mean of these repeated values was used for the final analysis. Two sets of measurements were obtained: the first using the standard black-and-white panoramic radiograph, as shown in Figure 1(a), and the second after applying the ‘Heatwave’ filter using the Canva AI application to enhance visual contrast of the lesion margin, as illustrated in Figure 1(b).

(a) It shows the original panoramic radiograph, while (b) it demonstrates the same image after applying the ‘heatwave’ filter using the Canva AI application to enhance the visual contrast of the lesion margins.
Case descriptions
Two patients with cystic lesions of the mandible associated with impacted mandibular third molars were included in this comparative case series. Both were managed initially with decompression and underwent standardised radiographic follow-up to assess lesion reduction over time. All demographic information, dates, and patient details have been fully de-identified in accordance with CARE case report guidelines. 10 Written informed consent for treatment and for publication of anonymised clinical, radiographic, and histopathological information was obtained from both patients. No formal patient-reported outcome measures were collected; outcomes were therefore assessed solely through clinical and radiographic evaluations. Adherence to decompression therapy was monitored through scheduled follow-up appointments, during which device patency and oral hygiene around the decompression stent were assessed, along with serial radiographic measurements. Both patients tolerated the decompression device well and did not report significant discomfort or treatment-related complications throughout the course of therapy. No adverse or unanticipated events occurred during the course of decompression therapy in either case. Both patients completed treatment without infection, device-related complications, or other clinically significant issues.
Case 1 (dentigerous cyst)
This case involves a female patient in her late thirties who presented with severe pain on the lower left side of the face, accompanied by a tingling sensation and radiating pain extending inferiorly, as well as restricted mouth opening. The patient was medically fit and well. Her psychosocial history was non-contributory, with no reported use of tobacco, alcohol, paan, or recreational drugs. She also reported no known allergies. Extra-oral examination revealed normal facial skin and symmetry, with no visible swelling or deformity. However, tenderness and pain were elicited in the left submandibular lymph node region. The parotid glands were unremarkable. Examination of the temporomandibular joint and muscles of mastication confirmed a limitation in mouth opening. Neurological assessment of the facial region revealed no abnormalities. Intra-oral examination indicated good overall oral hygiene. The labial mucosa, floor of the mouth, tongue, and both the hard and soft palates appeared normal. Tenderness and slight swelling were noted in the buccal mucosa adjacent to the lower left molars. Dental examination revealed that all third molars were clinically absent. Multiple restorations were present. The lower left second molar (LL7) exhibited purulent discharge, while the region of the missing lower left third molar (LL8) was tender to palpation.
Radiographic examination
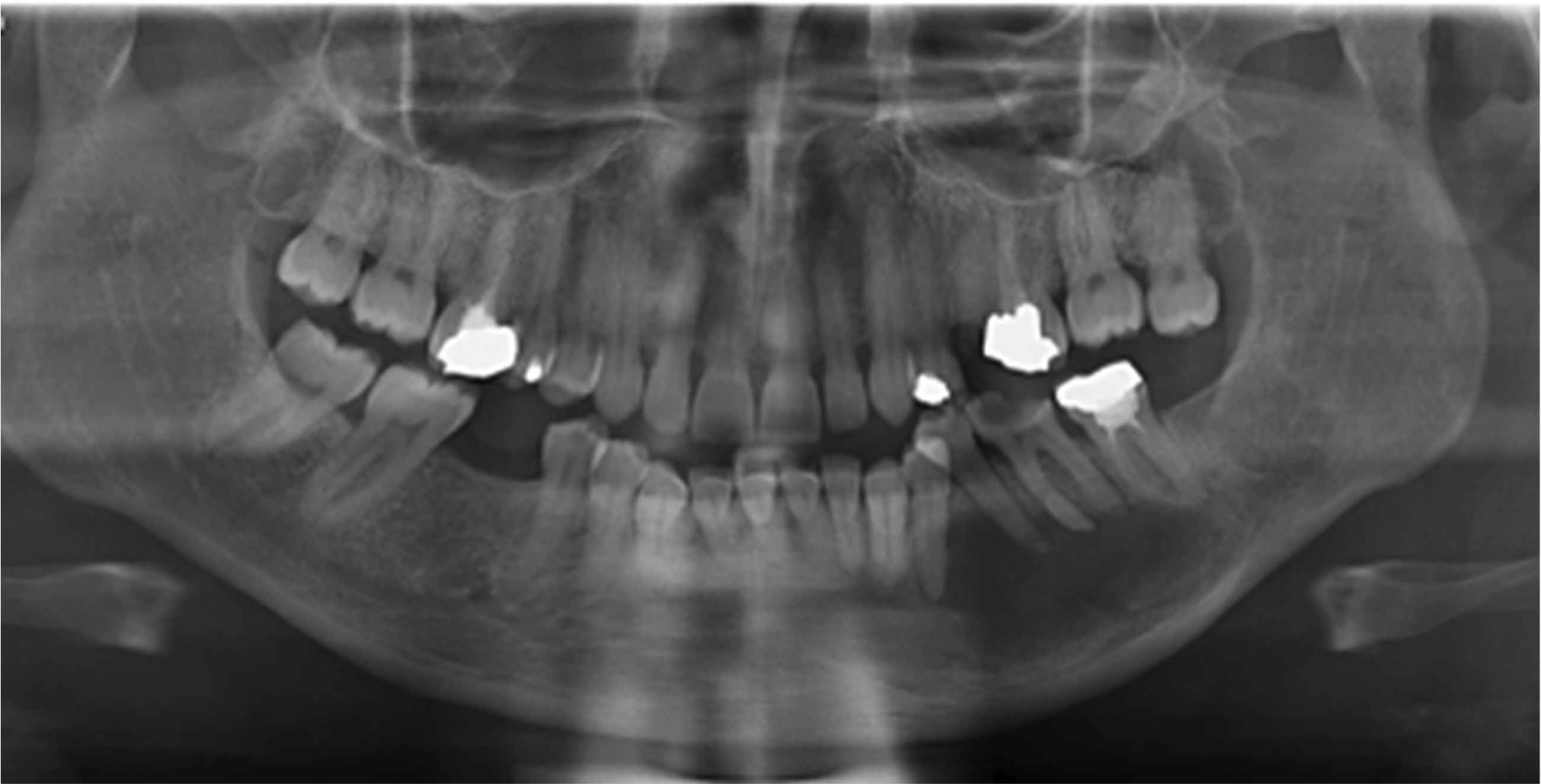
The panoramic radiograph, as shown in Figure 2, reveals an adult patient with missing upper right third molar (UR8) and lower right third molar (LR8), a distoangularly impacted upper left third molar (UL8), and a horizontally impacted lower left third molar (LL8). The LL8 is associated with a well-defined, unilocular, corticated radiolucency, consistent with a cystic lesion, which is attached to the crown at the cementoenamel junction. The lesion extends superiorly towards the ascending ramus and inferiorly to the lower border of the mandible, causing marked thinning of the mandibular cortex. There is no radiographic evidence of root resorption involving the adjacent lower left second molar (LL7). The inferior alveolar canal appears displaced inferiorly with partial loss of its cortical definition.

Pre-operative panoramic radiograph showing a horizontally impacted lower left third molar (LL8) associated with a well-defined, unilocular, corticated radiolucent lesion attached at the cementoenamel junction, consistent with a cystic lesion.
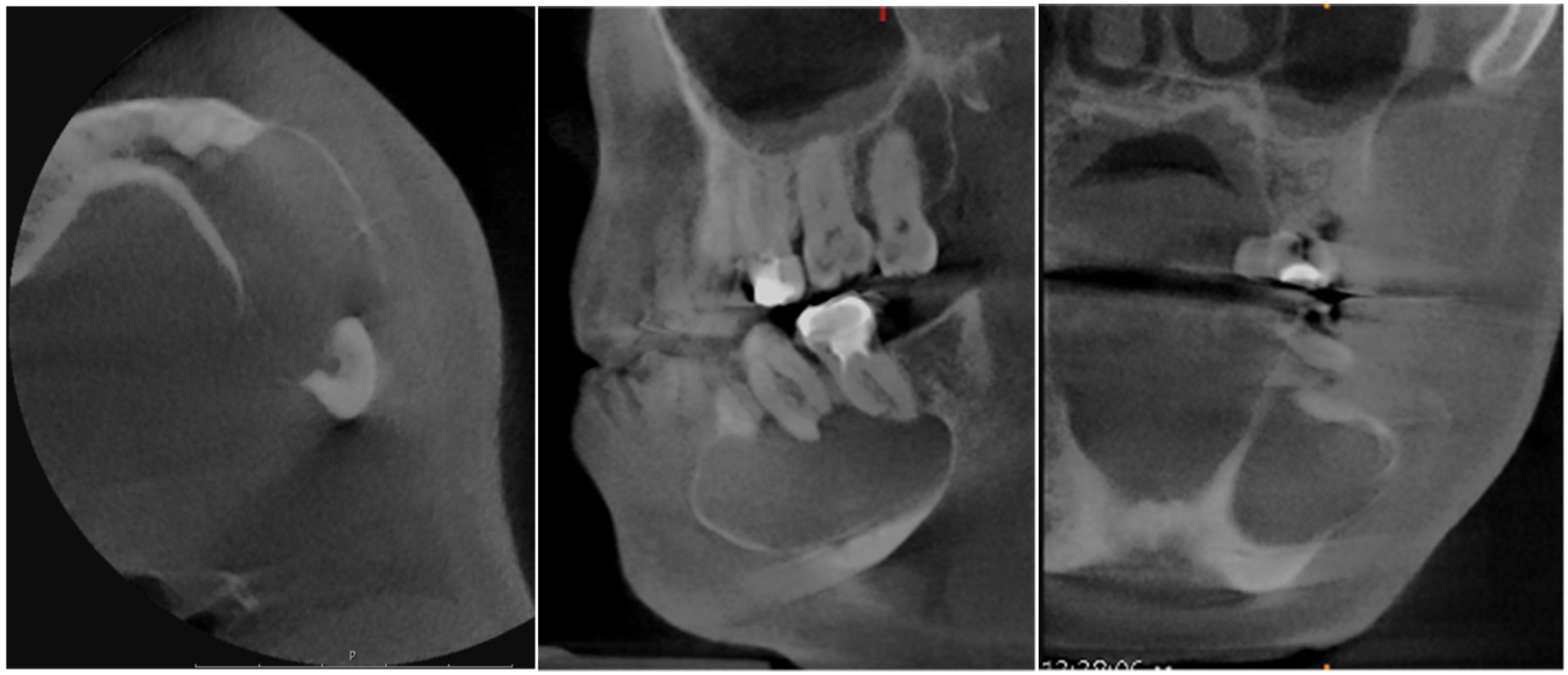
The pre-operative cone-beam computed tomography scan of the left posterior mandible, as shown in Figures 3, demonstrates a horizontally impacted and unerupted lower left third molar (LL8), associated with a well-defined, corticated, unilocular radiolucent lesion involving the pericoronal region, suggestive of a cystic pathology. The expansile nature of the lesion has resulted in posterior displacement of the LL8 towards the posterior border of the mandible, accompanied by buccal cortical dehiscence at the level of the apices and marked thinning of both the inferior and lingual cortices. The crown of LL8 lies in close proximity to the inferior alveolar canal, which is displaced inferiorly and slightly buccally, with partial loss of its cortical outline. Additionally, there is radiographic evidence of root resorption affecting the adjacent lower left second molar (LL7).

Pre-operative cone-beam computed tomography of the left posterior mandible demonstrating a horizontally impacted and unerupted lower left third molar (LL8) associated with a well-defined, corticated, unilocular radiolucent pericoronal lesion, suggestive of cystic pathology.
Histopathological report
Histological examination of H&E-stained sections revealed multiple cystic tissue fragments composed of granulation tissue, fibrous connective tissue, and areas consistent with dental follicle origin. The cyst wall is lined by a non-keratinised stratified squamous epithelium exhibiting significant inflammatory infiltration. The underlying connective tissue showed a dense chronic inflammatory cell infiltrate, with no features suggestive of ameloblastomatous change identified within the epithelial lining. These histopathological findings were consistent with a dentigerous cyst exhibiting secondary inflammation.
Case 2 (odontogenic keratocyst)
A male patient in his mid-50s presented with a chief complaint of a painless swelling in the lower left jaw region. He reported no pain or numbness associated with the swelling and had not experienced any discharge or infection-like symptoms. His past medical history was unremarkable; he had no known systemic diseases, was not on any medications, and reported no drug allergies. There was also no significant dental history of trauma or infection in the area of the lesion. On extra-oral examination, a slight fullness was observed over the left mandibular body region, but the overlying skin appeared normal and there was no obvious facial asymmetry. No cervical lymphadenopathy was detected. Intra-oral examination revealed a localised expansion of the buccal cortical plate in the region spanning from the lower left central incisor to the area of the first molar. The overlying oral mucosa was intact with no ulceration or sinus tract. On palpation, the swelling was hard (bony) in consistency, suggesting an intraosseous lesion. The teeth in the involved area (left mandibular incisors, canine, and premolars) were all firm and responded normally to vitality tests, indicating they were vital. However, the lower left first molar was carious (LL6), and the lower left second molar (LL7) had undergone endodontic treatment and was restored with a crown.
Radiographic examination
Panoramic radiograph in Figure 4 shows a well-defined radiolucent lesion in the left mandibular body with partially corticated margins. The lesion extends anteriorly from the region of the lower left central incisor to the area of the second molar posteriorly. It encompasses the periapical regions of the intervening teeth. The borders of the radiolucency are smooth and partially corticated. Although the roots of the adjacent teeth are displaced by the lesion, there is no evidence of significant root resorption.
Pre-operative panoramic radiograph demonstrating a well-defined radiolucent lesion with partially corticated margins within the left mandibular body.
A cone-beam computed tomography scan, as shown in Figure 5, was subsequently performed to further evaluate the lesion. The scan revealed thinning and mild expansion of the buccal cortical plate, without evidence of cortical perforation. However, a clear cortical perforation was observed in the lingual cortical plate.
Pre-operative cone-beam computed tomography of the left posterior mandible demonstrating thinning and mild expansion of the buccal cortical plate without evidence of buccal cortical perforation.
Histopathological report
Microscopic examination using H&E stain revealed a cystic lining composed of a thin, uniform layer of parakeratinised stratified squamous epithelium. The surface of the epithelium was characteristically corrugated, while the basal cell layer was well-defined, exhibiting palisading of columnar to cuboidal cells with hyperchromatic, basophilic nuclei-oriented perpendicular to the basement membrane. The fibrous connective tissue wall was relatively thin and showed no signs of inflammation. The epithelial-connective tissue interface was flat and smooth, with no evidence of budding, epithelial proliferation, or daughter cyst formation. No dysplastic changes or features suggestive of malignancy were observed in the examined sections, and the overall histopathological features were consistent with an odontogenic keratocyst involving the left mandible.
Decompression procedures
For both cases, decompression was performed under local anaesthesia. Anaesthesia was achieved through buccal infiltration and an inferior alveolar nerve block, using three cartridges (2.2 mL each) of Lidocaine 2% with 1:80,000 adrenaline. An envelope flap was raised along the alveolar crest with a single vertical releasing incision. Bone removal was performed using a round surgical bur to expose the cyst. An incisional biopsy of the cyst lining was taken to confirm the diagnosis histopathologically. Subsequently, a paediatric endotracheal tube was adjusted, inserted into the cystic cavity to maintain communication with the oral cavity, and secured using 3-0 silk sutures. The flap was repositioned and closed using 4-0 Vicryl sutures. Daily irrigation with saline was advised, and the patients attended regular follow-up appointments to monitor and evaluate the effectiveness of the decompression procedure. The decompression tube remained in place for 6 weeks, after which it was removed. By this stage, the opening created during the procedure had typically become lined with stratified squamous epithelium, forming a stable epithelialised tract. This epithelial lining helps maintain patency of the opening, allowing continued drainage and sustained intracystic pressure relief.
Treatment outcomes
As the radiographic images were not perfectly congruent, geometric distortion between the baseline and follow-up images was quantified in both the vertical and horizontal planes. Corresponding correction factors were derived for each dimension and applied to standardise measurements, thereby enhancing the accuracy and comparability of data obtained from multiple radiographic images. The calculated correction factors are summarised in Table 1.
Vertical (CFᵥ) and horizontal (CFₕ) correction factors used to standardise linear measurements between baseline and follow-up panoramic radiographs at 5, 12, 24, and 44 months for LL7 and UL7.

For the dentigerous cyst (Table 2), the baseline SLAI was 1320.00 mm2. A reduction to 761.31 mm2 at 5 months (42.34% shrinkage; RR = 57.76%; ∼8.47%/month) was classified as a poor response (<50%). By 12 months, the SLAI had decreased by 94.43% (RR = 5.57%; ∼7.87%/month), meeting the criteria for a good response (≥80%), which persisted at 24 months (96.54% shrinkage; RR = 3.46%; ∼4.02%/month). At 44 months, the lesion boundary was no longer visible, indicating complete radiographic resolution. For the odontogenic keratocyst (Table 3), the baseline SLAI was 2484.38 mm2. At 5 months, a 58.23% shrinkage (RR = 41.77%; ∼11.65%/month) was observed, representing a moderate response (50–80%). Subsequent follow-ups at 12 and 24 months demonstrated good responses, with reductions of 86.58% (RR = 13.42%; ∼7.21%/month) and 90.61% (RR = 9.39%; ∼3.78%/month), respectively. At 44 months, the SLAI remained reduced by 90.38% (RR = 9.62%; ∼2.05%/month), although radiographic evidence of recurrence was detected.
Longitudinal changes in corrected vertical height and horizontal width, surface lesion area index (SLAI), percentage of lesion reduction (POR), reduction rate (RR), and time-adjusted reduction rate following decompression of a dentigerous cyst from baseline to 44 months.
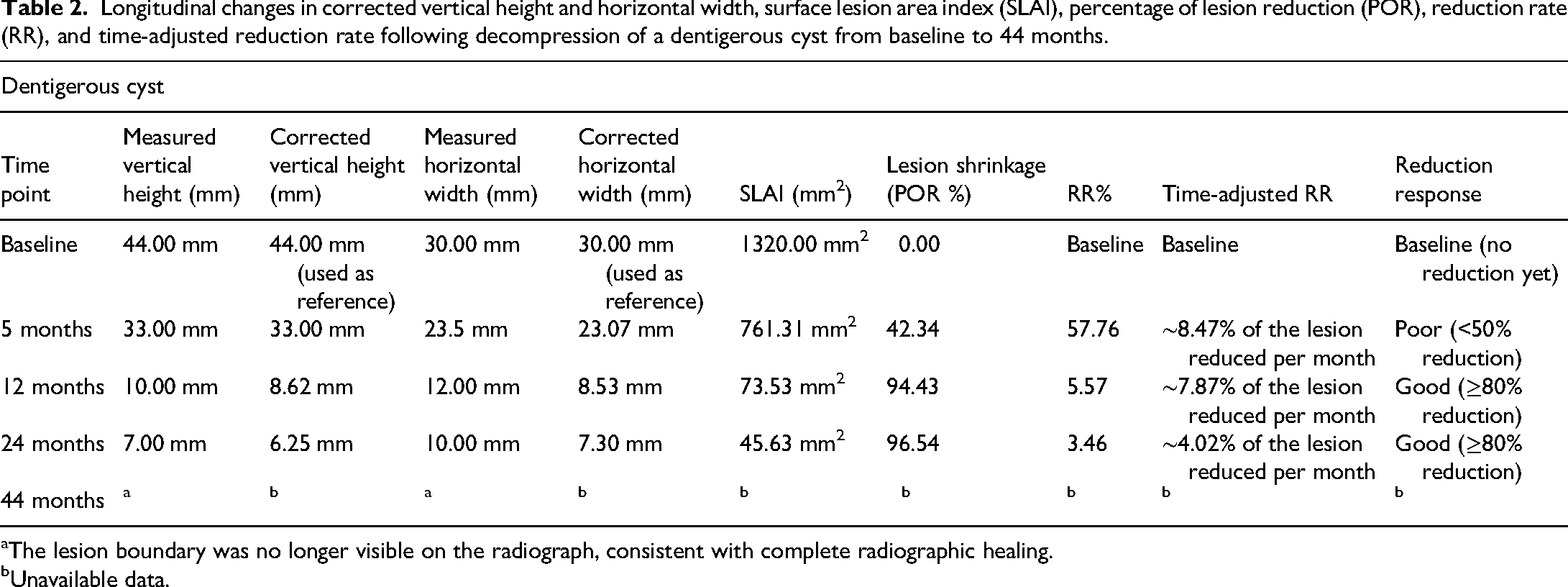
The lesion boundary was no longer visible on the radiograph, consistent with complete radiographic healing.
Unavailable data.
Longitudinal changes in corrected vertical height and horizontal width, surface lesion area index (SLAI), percentage of lesion reduction (POR), reduction rate (RR), and time-adjusted reduction rate following decompression of an odontogenic keratocysts from baseline to 44 months.

Evidence of lesion recurrence was observed on follow-up imaging at the 44-month interval.
Figure 6 depicts longitudinal changes in SLAI for dentigerous cysts and odontogenic keratocysts following decompression, over a 44-month observation period. By the 12-month interval, the dentigerous cyst had approached near-complete resolution and maintained minimal lesion dimensions thereafter. In contrast, the odontogenic keratocyst plateaued after 24 months, retaining a small residual lesion area at the final follow-up.

Longitudinal changes in surface lesion area index (SLAI) of the dentigerous cyst and odontogenic keratocyst from baseline to 44-month successive follow-up intervals following decompression.
Figure 7 illustrates the POR% for both lesions over a 44-month follow-up following decompression. The odontogenic keratocyst demonstrated a more rapid early reduction, reaching approximately 58% shrinkage by 5 months, compared with 42% for the dentigerous cyst. By 12 months, the dentigerous cyst had surpassed the odontogenic keratocyst, achieving over 94% reduction versus 86%, and maintained this high level of shrinkage through subsequent follow-ups. In contrast, the odontogenic keratocyst plateaued after 24 months at around 90% reduction, with no further substantial improvement by the 44-month interval.

Longitudinal change in percentage of lesion reduction (POR) for dentigerous cysts and odontogenic keratocysts following decompression.
Follow-up
Case 1: Dentigerous cyst
Case 2: Odontogenic keratocyst
Discussion
Based on evidence from the published literature, the first identified systematic review was conducted by Berretta et al. 11 to evaluate the effectiveness of marsupialisation and decompression techniques in reducing cystic jaw lesions. The review included 31 studies and aimed to critically appraise existing evidence regarding the outcomes of these conservative management approaches. The reported duration of marsupialisation or decompression varied widely, ranging from a minimum of 2.7 months to a maximum of approximately 23.5 months, with most studies reporting treatment periods of 1–2 years. The authors noted that marsupialisation and decompression were most commonly employed as preliminary treatment modalities, typically followed by a secondary surgical procedure. In the majority of included studies, lesion reduction was considered insufficient for these techniques to be used as definitive treatments. Furthermore, the authors highlighted substantial heterogeneity among the included studies and a lack of controlled clinical trials, limiting the strength of the available evidence and precluding firm recommendations for routine clinical practice.
The second identified systematic review was performed by Yu et al., 12 focusing specifically on the efficacy and duration of decompression therapy in the management of odontogenic keratocysts. Eight studies were included in the quantitative analysis, with the primary objective of assessing volumetric changes and identifying factors influencing volume reduction during decompression. The pooled results demonstrated a mean volume RR of 58.5%, with an average decompression duration of approximately 258.6 days. Despite these findings, the authors emphasised that the overall quality and limited number of included studies constrained the robustness of the conclusions. They concluded that further well-designed, high-quality studies are required to better define the therapeutic effectiveness and optimal duration of decompression for odontogenic keratocysts.
Radiographic follow-up in this report adhered to the Faculty of General Dental Practice (UK) 2018 criteria, which recommend panoramic radiographs for monitoring cystic lesions such as dentigerous cysts and odontogenic keratocysts. 13 Routine cone-beam computed tomography is discouraged due to its significantly higher radiation dose, which can range from 11 µSv to over 1025 µSv, compared with 2.7 to 38 µSv for panoramic radiographs. 13 This approach reflects the need to balance diagnostic utility with radiation safety in long-term lesion monitoring.
The key findings of the current comparison between the two lesions revealed similar patterns of reduction. However, differences were observed in the POR, RR, and time-adjusted RR. The dentigerous cyst exhibited a slower initial response, with poor reduction at 5 months, but achieved a sustained good response by 12 months. It maintained ≥80% shrinkage thereafter and progressed to complete radiographic resolution by 44 months, with no evidence of recurrence as demonstrated in Figures 8 and 9. In contrast, the odontogenic keratocyst showed a more rapid early reduction, achieving a moderate response at 5 months and good responses from 12 months onwards. However, the overall rate of shrinkage declined over time, and radiographic evidence of recurrence was observed at the 44-month follow-up, as indicated in Figure 10.

Final follow-up panoramic radiograph of Case 1 (dentigerous cyst) obtained 44 months after decompression, demonstrating radiographic resolution of the lesion with no radiographic evidence of recurrence at the 44-month follow-up. The accompanying colour-mapped image is a visual enhancement generated using a Heatwave filter (Canva AI) to improve contrast perception and does not represent a diagnostic imaging modality.

Longitudinal outcomes of decompression for dentigerous cysts over the follow-up period, illustrating changes in lesion size and radiographic appearance from pre-operative assessment to the final follow-up.

Radiographic outcomes of odontogenic keratocysts following decompression. (a) Radiograph obtained at 24 months of follow-up. (b) Radiograph obtained at 44 months of follow-up. The white arrow indicates evidence of residual lesion development, as observed in Figure 10(b).
The literature review identified similar studies, despite the use of different methodologies. Song et al. 14 utilised cone-beam computed tomography to assess volumetric reduction at two time points, namely from the initiation of decompression to the final radiographic examination. Their results demonstrated no significant differences in either the absolute or relative speed of shrinkage between odontogenic keratocysts and dentigerous cysts. In contrast, the findings of the present report provide case-specific observations that reveal differences in the POR, RR, and time-adjusted RR between the two lesions, suggesting a potential variation in the biological response to decompression between odontogenic keratocysts and dentigerous cysts. Nevertheless, both the current report and the findings of Song et al. 14 concur that the rate of shrinkage progressively declined as the lesions became smaller.
Another study by Jeong et al. 15 reported that lesions with larger initial volumes exhibited higher RRs. In the present report, lesions with larger initial volumes likewise exhibited higher RRs. However, this effect was most evident during the early phase of decompression. The initial volumes were 1320.00 mm2 for dentigerous cyst and 2484.38 mm2 for odontogenic keratocyst. At the 5-month interval, the time-adjusted RR was approximately 8.47% per month for dentigerous cyst and 11.65% per month for odontogenic keratocyst, indicating a more rapid shrinkage in the larger lesions. However, this trend was not maintained at subsequent time points, suggesting that the effect of initial volume on the RR may be most pronounced during the early stages of decompression but not consistent throughout the whole decompression process.
Although differences were observed in the reduction outcomes of the two lesions, they demonstrated an almost identical trend of reduction, as illustrated in Figures 6 and 7. Accordingly, similar initial management strategies may be considered, although the long-term treatment outcomes were not equivalent between the two lesions.
One of the systematic reviews 11 reported that decompression is most often employed as a preliminary intervention and is typically followed by enucleation. However, this approach may not be applicable in all clinical scenarios. Findings from the present report suggest that, in this individual case, decompression alone was sufficient to achieve complete radiographic resolution of a dentigerous cyst over long-term follow-up. In this case, decompression resulted in complete lesion resolution, eliminating the need for subsequent surgery. These findings indicate that decompression may be sufficient in selected dentigerous cyst cases, although confirmation in larger series is required. In contrast, odontogenic keratocyst do not exhibit the same response, based on the current case, indicating that they should require additional or alternative interventions beyond decompression. In this case, secondary surgical intervention was considered following decompression to reduce the risk of recurrence. However, treatment decisions should be individualised and supported by larger clinical studies. In the present case, long-term follow-up revealed the development of a new lesion, highlighting the need for additional intervention after decompression in contrast to dentigerous cyst, which resolved completely without further surgery.
The optimal duration of decompression remains debated; however, evidence from the systematic review suggests a relatively consistent treatment timeframe. Reported durations of marsupialisation/decompression ranged from 2.7 to 23.5 months, with the majority of cases requiring approximately 1–2 years of treatment. 11
Similarly, another systematic review demonstrated a mean decompression period of approximately 258.6 days (around 8.5 months), thereby reinforcing the variability but also suggesting a predictable treatment window. 12 These findings collectively emphasise that the required duration is influenced by lesion type, biological behaviour and initial lesion size. The results of the present report align with these observations, further demonstrating that the treatment duration varies depending on the cystic lesion type.
In the present case, the dentigerous cyst demonstrated more rapid regression than the odontogenic keratocyst, requiring approximately 5 to 12 months to achieve about 90% reduction in size, with a maximum of 24 months to attain over 95% shrinkage. By contrast, odontogenic keratocysts required a considerably longer duration up to 24 months to reach a similar 90% reduction.
Furthermore, long-term follow-up in the current report provided additional insight into these differences. At 44 months, the dentigerous cyst was no longer detectable radiographically, indicating complete healing following decompression. In contrast, despite substantial shrinkage, the odontogenic keratocyst exhibited evidence of recurrence at the same follow-up interval, which is consistent with the known aggressive biological behaviour of odontogenic keratocysts reported in the literature. 16 Taken together, these observations highlight the potential influence of lesion type on reduction patterns following decompression.
In the present case-based comparison, dentigerous cyst achieved satisfactory shrinkage within a relatively shorter timeframe. In contrast, the odontogenic keratocyst require prolonged monitoring, extended decompression and a secondary surgical procedure due to its more resistant biological profile. From a clinical perspective, secondary surgical intervention in odontogenic keratocysts may be considered when one or more of the following criteria are present: (i) plateauing of lesion reduction despite an adequate decompression period, typically beyond 12 to 24 months; (ii) persistence of a substantial residual lesion on radiographic follow-up; (iii) radiographic features suggestive of recurrence; and (iv) lack of progressive cortical bone regeneration. In the present case, secondary surgery was planned following radiographic evidence of lesion persistence and subsequent recurrence at long-term follow-up. These criteria may assist clinicians in determining the appropriate timing for definitive surgical management following decompression.
The present report is limited by its very small sample size, comprising only two patients, and therefore the findings must be interpreted strictly as case-specific observations rather than population-level evidence. While radiographic assessment is valuable for monitoring dimensional changes, it does not fully capture the biological behaviour of cystic lesions or subtle histopathological changes that may influence recurrence. In addition, differences in patient-related variables, such as age and lesion location, may have affected the rate of reduction observed.
Although the systematic review component provides a broader contextual framework, the substantial heterogeneity in study design, imaging protocols, and outcome measures across the included literature limits the ability to define a definitive timeline for odontogenic keratocyst reduction following decompression or marsupialisation. To strengthen the evidence base, well-designed prospective trials with larger cohorts and standardised protocols are required, alongside long-term follow-up, to clarify treatment effectiveness in different types of cysts.
Despite these limitations, the study's strengths include its extended follow-up period, standardised radiographic assessment across both cases, and direct comparison of two distinct cystic lesions managed with an identical decompression protocol, which provides clinically meaningful insight into lesion-specific reduction behaviour.
This report is presented as a focused case-based comparison and is not intended to provide generalisable conclusions. The observations reflect individual lesion behaviour and serve to illustrate potential differences in reduction dynamics following decompression. Broader clinical inference would require validation through larger case series or prospective cohort studies.
Conclusion
This report demonstrated that decompression is a useful conservative approach for managing cystic jaw lesions, although treatment outcomes appear to vary according to lesion type. In the present cases, dentigerous cysts achieved complete radiographic resolution and showed no evidence of recurrence or requirement for secondary surgery during long-term follow-up. In contrast, the odontogenic keratocysts exhibited an initially rapid reduction that plateaued at approximately 90% shrinkage by 24 months, followed by radiographic evidence of recurrence at 44 months, necessitating additional intervention.
These case-based observations suggest that decompression may be sufficient in selected dentigerous cyst cases, whereas odontogenic keratocysts require prolonged monitoring and are more likely to require secondary surgical management. Importantly, this study is not intended to support generalisable clinical conclusions but rather to provide detailed longitudinal observations of two individual lesions. Larger prospective studies with standardised protocols and extended follow-up are required to clarify reduction dynamics, refine treatment timelines, and define the optimal role of decompression in different odontogenic cysts.
Key clinical message
Decompression is an effective conservative treatment for cystic jaw lesions, with outcomes varying by type. Dentigerous cyst resolve completely and faster, without recurrence or secondary surgery. Odontogenic keratocyst show initial shrinkage but plateau, with recurrence. Long-term follow-up and potential further intervention are essential for keratocysts.
Footnotes
Informed consent statement
Written and verbal informed consents were obtained from the patients for the publication of the anonymous data.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data concerning this article may be requested from the corresponding author for reasonable purposes.
Institutional review board statement
Not applicable.