
Abstract
Objective
To validate a serial multimodal ultrasound (MMUS) protocol for assessing dynamic tibialis anterior changes in detecting intensive care unit-acquired weakness (ICUAW) and to develop a diagnostic algorithm.
Methods
In a prospective cohort of 97 high-risk adults (mean age 60.7±13.7 years; 73.2% male; SOFA score ≥8 for ≥3 days), MMUS quantified structural (thickness, echogenicity), hemodynamic (perfusion grade, peak systolic velocity [PSV]), and mechanical (elastic modulus) parameters of the tibialis anterior at ICU admission (Day 1) and Day 7. ICUAW was diagnosed per American Thoracic Society guidelines. Serum biomarkers (IL-6, PCT, CRP) were correlated with sonographic changes. Diagnostic models were constructed using binary logistic regression and evaluated by ROC analysis.
Results
31 patients (32.0%) developed ICUAW. By Day 7, the ICUAW group showed greater structural deterioration (echogenicity progression: 54.8% vs. 16.7%, P < 0.001), hemodynamic changes (PSV: 7.60 ± 1.72 vs. 6.35 ± 1.78 cm/s, P < 0.001), and faster stiffness increase (elastic modulus rate: 14.1±12.3% vs. 5.4±6.0%, P < 0.001). Day 7 PSV correlated with IL-6 (r = 0.59), PCT (r = 0.50), and CRP (r = 0.68) (all P < 0.05). A 7-parameter model achieved an AUC of 0.917 (95%CI: 0.857-0.978) with an NPV of 92.4%.
Conclusion
Dynamic MMUS captures ICUAW pathophysiology. The proposed algorithm shows potential as a non-invasive bedside tool for early risk stratification, pending multicenter validation.
Keywords
Introduction
Intensive care unit-acquired weakness (ICUAW) represents a debilitating neuromuscular complication in critically ill patients, with reported incidence rates of 25–100% depending on diagnostic stringency.1,2 This syndrome independently prolongs mechanical ventilation duration by 1.5- to 3-fold, 3 increases mortality risk by 1.5–2.3-fold, 4 and raises long-term healthcare costs by 47% due to persistent functional impairment. 5 Early detection is clinically imperative, as timely rehabilitation interventions can reduce intensive care unit (ICU) stay and mortality 6 ; however, current diagnostic approaches face fundamental technical limitations in the intensive care environment. Established tools exhibit restricted utility: the Medical Research Council Sum Score requires patient cooperation—rendering it infeasible in over 65% of sedated individuals 7 —while its validity for global functional prognostication remains contested. 8 Electrophysiological studies demonstrate 28% false-negative rates attributable to electrical interference and tissue edema artifacts, 9 and although muscle biopsy provides definitive diagnosis, it carries a 5.7% complication risk. 10 Serum biomarkers such as neurofilaments further lack specificity for ICUAW subtyping. 11
Multimodal ultrasound (MMUS) emerges as an innovative engineering solution, enabling real-time quantification of three critical musculoskeletal domains: muscle biomechanical properties through shear wave elastography, 12 microstructural integrity via echogenicity and architectural analysis, 13 and microcirculatory dynamics using vascular density and perfusion velocity metrics. 14 While MMUS has been validated in chronic neuromuscular disorders, 15 its systematic application for dynamic ICUAW monitoring remains technically unexplored.
To address this gap, we selected the tibialis anterior (TA) muscle as our primary monitoring site. This choice was based on its distinct advantages in the ICU setting: (1) its distal location and non-weight-bearing status render it less confounded by dependent edema, which frequently obscures interpretation of quadriceps muscle architecture in critically ill patients 16 ; (2) it may serve as a “sentinel” muscle, exhibiting earlier signs of neuromuscular dysfunction due to its composition and innervation; and (3) it allows for facile, reproducible serial scanning with minimal patient manipulation, a crucial practical consideration in the ICU. While most prior studies have focused on the quadriceps, emerging evidence supports the utility of the TA in capturing ICUAW-specific pathology.17,18 Given these potential advantages of the TA over the quadriceps for ultrasound monitoring in the ICU, this study had two primary aims: first, to develop a diagnostic algorithm quantifying MMUS parameter evolution, and second, to engineer a real-time surveillance framework for critical care muscle pathology.
Materials and methods
Study population
We conducted a prospective observational cohort study in the Intensive Care Unit of Chongqing Emergency Medical Center between March and June 2025. The reporting of this study conforms to the STROBE guidelines. 19 A prospective cohort of 97 critically ill adults (71 male, 26 female; mean age 60.7 ± 13.7 years, range 19–86) admitted to a tertiary ICU between March and June 2025 was enrolled. Inclusion required: (1) Sequential Organ Failure Assessment (SOFA) score ≥8 for ≥3 consecutive days within the first 5 ICU days, 20 indicating high-risk status; (2) mechanical ventilation with FiO2 < 0.6 and Positive End-Expiratory Pressure (PEEP) <10 cm H2O; and (3) written informed consent from patients or legal representatives. Exclusion criteria encompassed pre-existing neuromuscular disorders (e.g. spinal cord injury, Guillain–Barré syndrome), chronic corticosteroid/neurotoxic medication use, neuromuscular blockade within 24 h prior to assessment, limb fractures, active malignancies, or coagulopathies. This study was approved by the Institutional Review Board of Chongqing Emergency Medical Center, Chongqing, China (Approval No. 2025-32; date of approval: March 17, 2025). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, as revised in 2013. All patient data were de-identified to ensure anonymity and confidentiality. Conscious patients provided direct consent; for sedated patients, consent was obtained from legal representatives with documentation of deferred consent protocol.
MMUS protocol
Serial ultrasound examinations of the right TA (proximal third) were performed at ICU admission (day 1) and day 7 using a Canon Aplio i800 system (18L7 linear transducer, 5–18 MHz). The TA was chosen over the more commonly studied quadriceps due to its reduced susceptibility to edema, which provides a more reliable assessment of true muscle architecture and echogenicity, and its practicality for serial bedside monitoring in critically ill patients. 16
Standardized acquisitions included the following.
Structural parameters: Muscle thickness and pennation angle were quantified in B-mode perpendicular to the fascial plane. Echogenicity was graded using a validated 4-point scale (grade 1: homogeneous fascicles with preserved bone interface; grade 4: complete architectural disruption with bone cortex obscuration).
Hemodynamic parameters: Superb microvascular imaging (SMI) classified microvascular density via Szkudlarek's four-grade system, 21 with Doppler gain optimized to avoid aliasing. Peak systolic velocity (PSV) was measured in intramuscular vessels using pulsed-wave Doppler (angle correction ≤60°).
Mechanical properties: Supersonic shear wave elastography acquired Young's modulus (kPa) within muscle fascicles using a 10-mm region of interest, excluding septa and vessels. Five valid measurements (interquartile range/median ratio <0.3) were median-averaged per protocol.
Parameter deterioration definitions: Parameter deterioration was explicitly defined as an adverse change from ICU days 1 to 7 in the following TA parameters: worsened echogenicity, an increase in the 4-point echogenicity grade; reduced muscle mass, a decrease in thickness (mm); architectural disorganization, a reduction in pennation angle (degrees); worsened perfusion, an increase in the SMI grade; microvascular flow derangement, an increase in PSV (cm/s); and increased stiffness, an increase in Young's elastic modulus (kPa). Deterioration was assessed individually for each parameter; these parameters were subsequently analyzed both separately and in combination for the diagnostic model.
ICUAW diagnostic criteria
ICUAW diagnosis followed American Thoracic Society guidelines 11 and standardized protocols 15 : diffuse, symmetric limb weakness developing post-ICU admission; exclusion of alternative neuromuscular etiologies; objective confirmation via: for alert patients (Glasgow Coma Scale [GCS] = 15): handgrip dynamometry (cutoffs: <11 kg males, <7 kg females) and Medical Research Council Sum Score <48; for sedated patients: peroneal nerve conduction studies showing compound motor action potential amplitude <3 mV with electromyographic evidence of myopathy (short-duration, low-amplitude polyphasic potentials). All assessments were performed by neurologists trained in critical care electrophysiology, with ≥2-h sedation interruption prior to testing.
Inflammatory biomarker quantification
Serum concentrations of interleukin-6 (IL-6), procalcitonin (PCT), and C-reactive protein (CRP) were quantified on days 1 and 7 using chemiluminescent immunoassay (Roche Cobas e801). Fasting venous blood (5 mL) was centrifuged at 3000 × g for 10 min, with aliquots stored at −80 °C until batch analysis. Inter-assay coefficients of variation were <5% for all biomarkers.
Statistical analysis
All analyses were performed using SPSS 27.0 (IBM Corp.). The normality of continuous data was assessed using the Shapiro–Wilk test. Parametrically distributed data are reported as mean ± standard deviation (SD) and were compared between the ICUAW and non-ICUAW groups using independent (unpaired) Student's t-tests. Nonparametric data are reported as median (interquartile range) and were compared using the Mann–Whitney U test. Categorical variables were analyzed with χ2 tests or Fisher's exact test, as appropriate.
Binary logistic regression was employed to identify independent predictors of ICUAW. To ensure model robustness and minimize overfitting given the sample size, a forward stepwise selection procedure (with entry criteria of P < 0.05 and removal criteria of P > 0.10) based on the Akaike information criterion (AIC) was used to develop a parsimonious model. This approach resulted in a final model containing four predictor variables. With 31 patients developing ICUAW (events), the events-per-variable ratio was 7.75, which exceeds the commonly recommended threshold of 5 and indicates acceptable reliability for logistic regression.
Multicollinearity among the candidate predictors was assessed using the variance inflation factor (VIF), with a VIF <5 considered acceptable. The results of the logistic regression are presented as odds ratios (ORs) with 95% confidence intervals (CIs). The diagnostic performance of the model was evaluated using receiver operating characteristic curve analysis, and the area under the curve (AUC) was calculated. Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test. A two-tailed P < 0.05 was defined as statistically significant. No sensitivity analyses were performed to test the robustness of the logistic regression model due to the constraints of the sample size.
Results
Study population and participant flow
Between March and June 2025, 143 critically ill patients were screened for eligibility. A total of 46 patients were excluded: 23 for not fulfilling the inclusion criteria (primarily a SOFA score <8 or nonconforming mechanical ventilation parameters), 15 for meeting exclusion criteria (including pre-existing neuromuscular disorders or chronic corticosteroid use), and 8 who declined participation. Consequently, 97 patients were enrolled, yielding the final prospective cohort. All enrolled patients completed the 7-day follow-up assessment without any loss to follow-up, attributable to the closed ICU setting and short, fixed study duration.
Baseline characteristics
The baseline demographic and clinical characteristics of the 97 enrolled patients are summarized in Table 1. The cohort consisted of 71 males and 26 females with a mean age of 60.7 ± 13.7 years. No significant differences were observed at baseline between patients who developed ICUAW (n = 31) and those who did not (non-ICUAW, n = 66) regarding sex, age, height, weight, ICU or hospital length of stay, or initial SOFA score (all P > 0.05).
Comparison of baseline characteristics between ICUAW and non-ICUAW groups.

ICUAW: intensive care unit-acquired weakness; LOS: length of stay; SOFA: Sequential Organ Failure Assessment.
Note: Data are presented as n (%), mean ± SD, or median (interquartile range). Comparisons were made using the χ2 test, independent Student's t-test, or Mann–Whitney U test (Z-value reported), as appropriate.
Dynamic changes in muscle morphology and function
Serial ultrasound assessments revealed distinct patterns of muscle deterioration over the first week in the ICU. The proportion of patients exhibiting deterioration in muscle thickness, pennation angle, perfusion (SMI grade), and stiffness (elastic modulus) did not differ significantly between the ICUAW and non-ICUAW groups (all P > 0.05; Table 2). In contrast, a significantly greater proportion of patients in the ICUAW group showed progression in echogenicity grade (54.8% vs. 16.7%, P < 0.001). However, for the comparisons that were not statistically significant (e.g. muscle thickness and pennation angle), the observed effect sizes were small, and posthoc analyses indicated that the study was underpowered to reliably detect such differences (power <20% for these parameters). Therefore, the nonsignificant findings for these parameters should be interpreted as inconclusive rather than as definitive evidence of no difference between groups.
Number (percentage) of patients showing tibialis anterior deterioration between ICUAW and non-ICUAW groups during ICU days 1–7.

ICUAW: intensive care unit-acquired weakness; ICU: intensive care unit.
Note: Deterioration for each parameter was defined as follows from day 1 to day 7: reduction in muscle thickness: decrease in thickness (mm); worsened echogenicity: increase in the four-point echogenicity grade; decrease in pennation angle: reduction in angle (degrees); worsened perfusion: increase in the four-point superb microvascular imaging (SMI) grade; increased stiffness: increase in Young's elastic modulus (kPa). Comparisons of proportions were made using the χ2 test.
Day 7 discriminatory ultrasound parameters
While initial ultrasound parameters on day 1 showed no significant differences between the groups, pronounced disparities emerged by day 7. Patients with ICUAW demonstrated significantly worse muscle integrity across multiple modalities. This included greater structural deterioration (higher median echogenicity grade: 2.0 vs. 1.0, P < 0.001), more severe perfusion derangement (higher median SMI grade: 3.0 vs. 2.0, P = 0.012), elevated microvascular flow velocity (PSV: 7.60 vs. 6.35 cm/s, P < 0.001), and a markedly higher rate of stiffness progression (elastic modulus increase rate: 14.1 ± 12.3% vs. 5.4 ± 6.0%, P < 0.001). Changes in muscle mass reduction rate or pennation angle reduction rate remained nondiscriminatory (Table 3).
Comparison of multimodal ultrasound parameters between ICUAW and non-ICUAW groups.
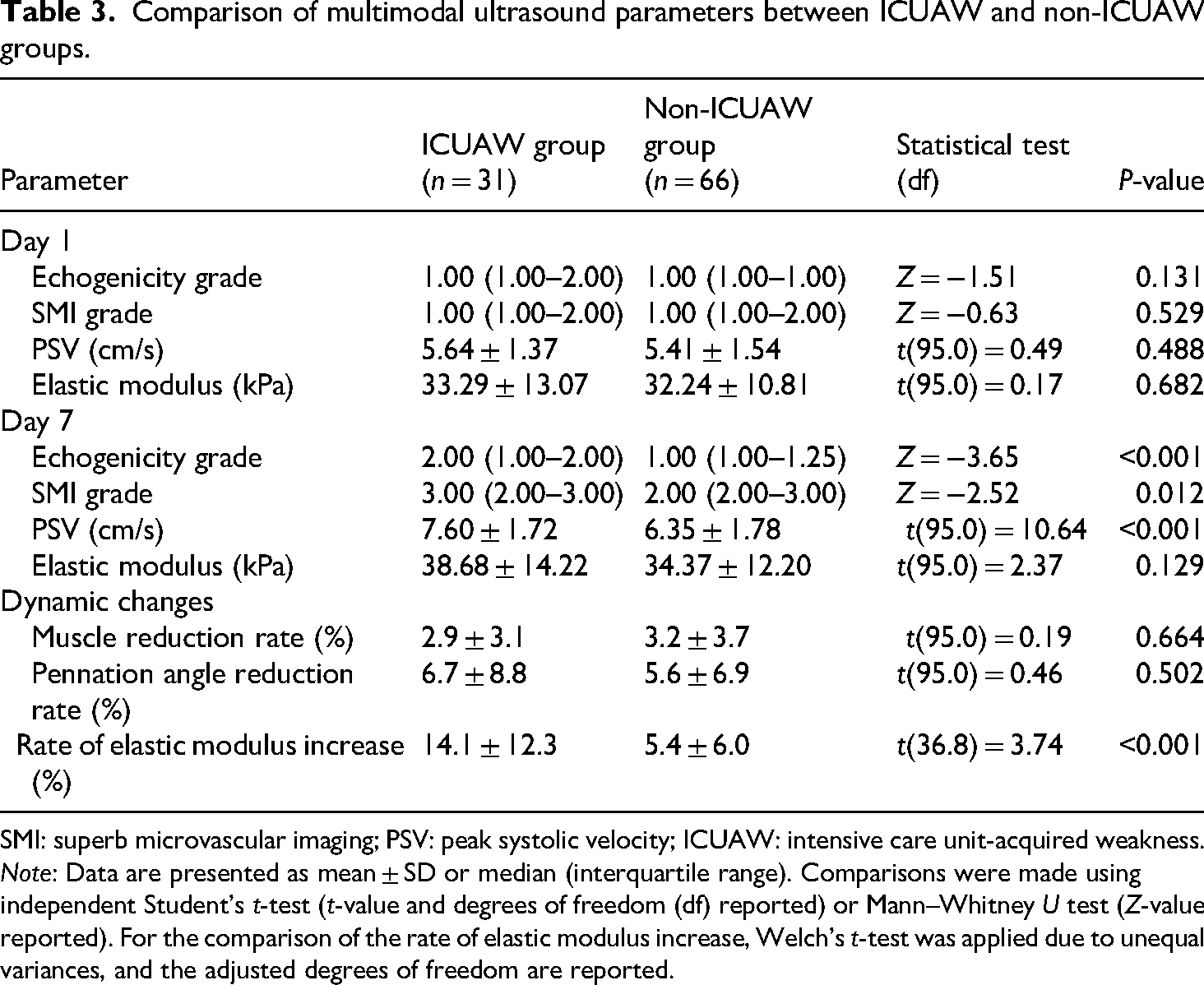
SMI: superb microvascular imaging; PSV: peak systolic velocity; ICUAW: intensive care unit-acquired weakness.
Note: Data are presented as mean ± SD or median (interquartile range). Comparisons were made using independent Student's t-test (t-value and degrees of freedom (df) reported) or Mann–Whitney U test (Z-value reported). For the comparison of the rate of elastic modulus increase, Welch's t-test was applied due to unequal variances, and the adjusted degrees of freedom are reported.
Correlations with systemic inflammation
Muscle perfusion status on day 7, measured by PSV, exhibited strong positive correlations with concurrent systemic inflammatory biomarkers (PCT: r = 0.50; IL-6: r = 0.59; CRP: r = 0.68; all P < 0.05). Furthermore, the change in muscle stiffness (rate of elastic modulus increase) showed a significant inverse correlation with CRP levels (r = −0.49, P < 0.05), indicating a potential link between systemic inflammation and tissue remodeling leading to increased stiffness.
Clinical prediction models for ICUAW
To mitigate the risk of model overfitting given the sample size, we prioritized the development of a parsimonious model. A four-parameter model was selected using a forward stepwise procedure based on the AIC. Key day 7 ultrasound parameters were identified as independent features associated with ICUAW and were selected for inclusion in the predictive model. Increased muscle structural deterioration (OR = 13.93, P < 0.001), perfusion derangement (OR = 2.07, P = 0.026), and elevated microvascular flow (PSV; OR = 1.52, P = 0.020) were each strongly associated with the presence of ICUAW and contributed significantly to the predictive model. Multicollinearity diagnostics confirmed the stability of the regression coefficients, with all VIF values ranging between 1.0 and 1.3, indicating no multicollinearity among the predictors (for detailed VIF values, see Supplemental Table 1). This practical and parsimonious bedside model incorporating four parameters (muscle structure, perfusion, microvascular flow, and stiffness change) achieved a diagnostic accuracy of 77.3% with a high negative predictive value (NPV) of 86.4%. An exploratory comprehensive seven-parameter model was also constructed for comparative purposes, which further improved diagnostic accuracy to 84.5% and enhanced the NPV to 92.4% (Table 4).
Diagnostic performance of individual and combined parameters for ICUAW detection.

AUC: area under the receiver operating characteristic curve; CI: confidence interval; NPV: negative predictive value; PSV: peak systolic velocity (cm/s); SMI: superb microvascular imaging; ICUAW: intensive care unit-acquired weakness.
Diagnostic performance
The integration of MMUS parameters significantly enhanced the ability to detect ICUAW compared to any single metric alone. The combined seven-parameter model yielded an excellent AUC of 0.917 (95% CI: 0.857–0.978), substantially outperforming the best individual parameter (AUC ≤0.731). This combined approach, particularly model 2, optimized rule-out utility with an NPV of 92.4%, supporting its clinical application for reliably excluding ICUAW in patients with a low predicted probability.
Discussion
This prospective study suggests the potential of MMUS as a practical bedside tool for early detection of ICUAW, revealing a pathophysiological triad in the TA characterized by progressive muscle degeneration, microvascular dysregulation, and tissue stiffening. This triad aligns with and extends the current understanding of ICUAW pathophysiology beyond simple muscle mass loss.1,5 Crucially, these dynamic changes culminated in a diagnostic model with a high NPV of 92.4%, potentially offering clinicians a strategy to rule out ICUAW in low-risk patients.
Our findings identify a set of sonographic biomarkers that reflect the underlying pathophysiology of ICUAW, linking established disease mechanisms with a novel monitoring approach. Generalized immobilization effects—such as reductions in muscle thickness and pennation angle—occurred comparably in both the ICUAW and non-ICUAW groups, aligning with prior reports that fluid overload may mask atrophy. 16 This suggests such parameters reflect systemic critical illness burden rather than ICUAW-specific pathology. 22 In contrast, ICUAW patients exhibited selective structural deterioration, evidenced by a significantly higher proportion of patients with echogenicity progression and pronounced tissue stiffening. The progression in echogenicity, indicative of architectural disorganization and fibrofatty infiltration, 13 coupled with a 2.6-fold faster rate of increase in elastic modulus, strongly points toward active tissue remodeling and fibrosis as a core component of ICUAW pathology.23,24
The choice of the TA for monitoring, as opposed to the more extensively studied quadriceps, merits further consideration in this context. While quadriceps measurements, such as rectus femoris cross-sectional area, serve as excellent indicators of global muscle mass and have demonstrated predictive value for ICUAW, 25 their interpretation can be confounded by significant fluid shifts and edema in critically ill patients, 16 particularly affecting echogenicity and architectural assessment. In contrast, the TA, as a distal and nondependent muscle, is less susceptible to these confounding factors. Our findings of significant deterioration in TA echogenicity and elastic modulus specifically in the ICUAW group suggest that it may act as a more specific sensor for intrinsic muscle pathology, such as myofiber necrosis and fibrofatty infiltration, independent of fluid status. This complements the quadriceps-based approach, proposing that while the quadriceps may better reflect the “quantity” of muscle loss, the TA can provide superior insight into the “quality” of muscle deterioration, a notion supported by emerging literature. 26 In line with this notion, in our cohort, patients with ICUAW exhibited this selective structural deterioration in the TA, evidenced by a significantly higher proportion with echogenicity progression and pronounced tissue stiffening. These patterns correlate histopathologically with myofiber necrosis and fibrosis. 27
Strengthening this framework, we identified compensatory microvascular hyperperfusion in ICUAW patients, manifested through elevated SMI grades and PSV by day 7. The strong correlations between PSV and inflammatory biomarkers28,29 implicate inflammatory endothelial dysfunction as a key driver. This microvascular dysregulation, characterized by elevated flow velocity amid structural decay, may represent a maladaptive response to local tissue hypoxia and inflammation, a process increasingly recognized in critical illness myopathy. 30 Notably, the inverse association between elastic modulus changes and CRP implies inflammation actively remodels the extracellular matrix, bridging microcirculatory stress and macroscopic tissue decline. Our findings thus integrate microvascular and biomechanical alterations into a coherent pathophysiological narrative, supported by growing evidence of their interplay in muscle disease. 14
These insights translate into three clinical and methodological advances: first, focusing on the TA minimizes immobilization confounders inherent in proximal muscle monitoring. 21 Second, dynamic parameter tracking (e.g. stiffness progression rates) proves superior to static measurements for early ICUAW detection. Most significantly, our exploratory pragmatic diagnostic algorithm (model 2: seven ultrasound parameters) achieves high accuracy (AUC: 0.917) and an NPV of 92.4% in this cohort. The 17% improvement in AUC over single-parameter models suggests potential for efficient resource allocation by excluding low-risk patients while facilitating timely rehabilitation for high-risk cases (sensitivity: 83.9%). It is important to emphasize that the diagnostic algorithm derived from this study must be viewed as hypothesis-generating. While its performance in our cohort is promising, its generalizability and clinical efficacy are unknown. Prospective validation in large, multicenter external cohorts is an essential prerequisite before any consideration of its implementation as a bedside tool.
Despite the model's promise, its single-center design and focus on the TA warrant validation in quadriceps-dominant assessments. Addressing these priorities, future work should: (1) conduct multicenter algorithm validation; (2) establish histopathological correlates for ultrasound markers (e.g. echogenicity vs. fibrofatty infiltration); and (3) integrate electrophysiological biomarkers to differentiate axonal and myopathic ICUAW subtypes.
Limitations
Our study has several limitations that should be considered. First, the sample size, particularly the number of patients who developed ICUAW (n = 31), results in a low events-per-variable ratio and limited statistical power, as confirmed by posthoc analyses. Although we employed strategies to mitigate overfitting (e.g. VIF analysis, stepwise selection), the comprehensive seven-parameter model must be considered exploratory and requires external validation before clinical application. Furthermore, the lack of sensitivity analyses due to sample size constraints means the robustness of our model to alternative analytical approaches could not be assessed. Second, the single-center design and recruitment restricted to invasively ventilated patients with high illness severity may affect the generalizability of our findings to other ICU populations. Third, the focus on a single muscle (the right TA) without bilateral assessment means we cannot comment on potential asymmetry or the behavior of other muscle groups, such as the quadriceps. Fourth, the 7-day follow-up period, while suitable for capturing early dynamic changes, provides no insight into the long-term trajectory of muscle recovery or its correlation with patient-centered functional outcomes. Finally, the pathophysiological interpretation of our findings is constrained by the inability to differentiate between axonal and myopathic ICUAW subtypes, as this distinction requires advanced diagnostic techniques beyond our study's scope.
Conclusion
MMUS captures ICUAW's pathophysiological continuum—from microcirculatory stress to irreversible structural decline. By transforming these insights into a proposed methodology, our study lays the groundwork for a potential shift in ICUAW detection from retrospective diagnosis to early identification of the disease, contingent upon successful external validation. This advances critical care beyond isolated muscle mass evaluation, which could potentially enable earlier rehabilitation initiatives and more optimized resource utilization, pending validation of our findings.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251409993 - Supplemental material for Dynamic tibialis anterior ultrasound monitoring reveals a multimodal ultrasound signature for intensive care unit-acquired weakness: A prospective cohort study
Supplemental material, sj-docx-1-sci-10.1177_00368504251409993 for Dynamic tibialis anterior ultrasound monitoring reveals a multimodal ultrasound signature for intensive care unit-acquired weakness: A prospective cohort study by Jing Chen, Jingjing Yin, Xiaoling Hu, Yuxia Li, Yan Zeng, Yan Du and Jie Zhu in Science Progress
Footnotes
Acknowledgments
The authors gratefully acknowledge the nursing staff and colleagues in the Intensive Care Unit of Chongqing Emergency Medical Center for their invaluable assistance in patient recruitment and data collection. We also thank the patients and their families for their participation and cooperation in this study. This work was supported by the Chongqing Science and Health Joint Medical Research Project (Grant Number 2025QNXM015). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors acknowledge the use of a large language model (DeepSeek) solely for the purpose of language polishing and improvement during the manuscript preparation. The authors take full responsibility for the entire scientific content, data analysis, and conclusions presented in this work.
Author contributions
Jing Chen: conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and funding acquisition.
Jingjing Yin: investigation, resources, data curation, and writing—review and editing.
Xiaoling Hu: investigation, resources, validation, and writing—review and editing.
Yuxia Li: investigation, resources, and writing—review and editing.
Yan Zeng: investigation, resources, and writing—review and editing.
Yan Du: methodology, software, validation, and formal analysis.
Jie Zhu: conceptualization, methodology, supervision, project administration, and writing—review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chongqing Science and Health Joint Medical Research Youth Project (Grant No. 2025QNXM015), which does not mandate public data deposition.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
De-identified ultrasound metrics, analysis code, and protocols can be requested from the corresponding author (
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.