
Abstract
Background
Following successful canalith repositioning procedures (CRPs), some patients with benign paroxysmal positional vertigo (BPPV) may experience residual symptoms. There is currently no consensus on whether these residual symptoms are related to the disease duration.
Objective
To examine the impact of BPPV duration on the persistence of residual symptoms following successful CRP.
Methods
A total of 102 idiopathic BPPV patients were enrolled and categorized into short-course and long-course groups based on the duration of the disease. The course of disease in the short-course group was less than or equal to 7 days. The long course of disease was longer than 7 days. All patients underwent swivel-chair-assisted CRP and were followed up 7–10 days after successful CRP. The Dizziness Handicap Inventory (DHI) questionnaire was administered to all patients before and after CRP.
Results
Before CRP, significant differences were observed between the two groups in total DHI score and its subdomains: Physical (DHI-P), Functional (DHI-F), and Emotional (DHI-E) (p < 0.05), indicating that long disease duration significantly affected all patient aspects. After CRP, significant differences remained in total DHI, DHI-P, DHI-F, and DHI-E scores (p < 0.05), with the long-course group consistently scoring higher. However, no significant differences were found in the changes in DHI scores across dimensions before and after CRP between the two groups.
Conclusion
The duration of BPPV did not influence CRP outcomes, but patients with a longer disease course were more likely to experience residual symptoms after successful CRP.
Keywords
Introduction
Benign paroxysmal positional vertigo (BPPV) is a prevalent peripheral vertigo disorder, constituting approximately 20%–30% of all peripheral vertigo cases. 1 According to the pathogenesis, BPPV is classified into canalithiasis and cupulolithiasis. Based on the direction of positional nystagmus, BPPV can be classified into posterior, lateral, and anterior semicircular canal types. 2 The roll test can induce horizontal nystagmus, and the duration is less than 1 minute, then the diagnosis is canalolithiasis. The roll test showed horizontal ground nystagmus with a duration of more than 1 minute, and the diagnosis was cupulolithiasis. The canalith repositioning procedure (CRP) is the most effective treatment for BPPV. However, some patients continue to experience balance disorders, including dizziness, unsteady gait, floating sensation, and instability while standing after successful CRP, despite the absence of positional vertigo; these are referred to as residual symptoms. 3 The incidence of residual symptoms ranges from 29.6% to 61%, though the underlying pathogenesis remains unclear,4,5 with possible hypotheses including: (a) abnormalities in vestibular function or the vestibular system 6 ; these dysfunctions cannot be detected, resulting in residual symptoms after CRP; (b) residual tiny otolith fragments in the semicircular canal after CRP, these fragments of otolith produce a constant, slight gravitational pull, insufficient to cause significant positional vertigo or nystagmus 7 ; (c) delayed central adaptation or compensatory response following CRP. 8 CRP can suddenly change the existing new balance, the center does not change with it; and (d) sympathetic nervous system disorder. 9
Some researchers suggest that residual symptoms may be associated with factors such as age,5,7 the number of repositioning maneuvers, 4 anxiety and/or depression,4,8 and osteopenia. 10 There is no definitive conclusion regarding the relationship between residual symptoms and the duration of BPPV.
This study examined the impact of disease duration on residual symptoms by comparing changes in different dimensional scores of the Dizziness Handicap Inventory (DHI) before and after successful CRP in BPPV patients. Our study found that patients with a long course of disease had higher DHI scores before and after treatment than those with a short course of disease.
Materials and methods
This study was a prospective case–control design. Patients diagnosed with BPPV were enrolled from the Department of Otorhinolaryngology—Head and Neck Surgery at Xinhua Hospital, affiliated with Shanghai Jiaotong University School of Medicine. The study was designed and conducted in accordance with the ethical standards of the Helsinki Declaration. The study was conducted from August 2021 to July 2022, following approval by the hospital's ethics committee (approval no. XHYY-2021-039). The reporting of this study conforms to STROBE guidelines. 11 All enrolled patients signed informed consent.
The inclusion criteria were as follows: (a) all patients had primary BPPV, consistent with the 2017 clinical practice guidelines by AAO-HNSF 2 ; including posterior semicircular canal BPPV and horizontal semicircular canal BPPV; (b) all patients underwent successful CRP treatment, with success defined according to BPPV diagnosis and treatment guidelines as the disappearance of positional vertigo and nystagmus; and (c) presence of residual symptoms after successful CRP.
The exclusion criteria included: (a) light cupula or BPPV involving multiple semicircular canals; (b) secondary BPPV, such as that secondary to Meniere's disease, vestibular migraine, sudden deafness, vestibular neuritis, trauma, or surgery; (c) severe cardiovascular or cerebrovascular diseases; and (d) a history of using vestibular depressants, anti-anxiety drugs, or ototoxic drugs within the past 3 months.
We have identified the patient's information. All patients presenting with positional vertigo underwent Dix–Hallpike and roll tests to confirm the diagnosis of BPPV. Once BPPV was confirmed, patients received a DHI assessment followed by CRP treatment. After three sessions of CRP treatment, patients underwent the diagnostic positional test again. If the test result was negative (no positional vertigo and no positional nystagmus detected), the CRP was defined as successful. Conversely, if the positional test was positive (positional vertigo and nystagmus still detected), the CRP was defined as unsuccessful, and the treatment was repeated one day later. After three CRP sessions, the diagnostic positional test was performed again. If the test result was negative, the patient was included in the study. If the CRP was still unsuccessful after three sessions, the patient was excluded. On day 7 after successful CRP, the provocation maneuvers were given again, and patients with no vertigo or nystagmus were assessed for residual symptoms using the DHI questionnaire. If the patient was found to have positional vertigo and nystagmus by provocation maneuvers, we would exclude the patient again to avoid any impact on the study results due to recurrence or persistent symptomatic problems. After that, patients were divided into short-course and long-course groups based on the duration of BPPV. Differences in the scores across various DHI dimensions between the two groups were compared to determine the effect of BPPV duration on the occurrence of residual symptoms. A flowchart illustrating the research design is shown in Figure 1.

A flow chart describing the research design. BPPV: benign paroxysmal positional vertigo; DHI: Dizziness Handicap Inventory; CRP: canalith repositioning procedure.
Participants
A total of 102 BPPV patients were enrolled, comprising 31 males and 71 females. The patients ranged in age from 27 to 77 years, with a mean age of 56 ± 12.39 years and a median age of 59.5 years. The duration of the disease ranged from 1 to 30 days, with a mean duration of 8.73 ± 8.67 days and a median duration of 6.5 days. There were 55 patients with left ear involvement and 47 with right ear involvement. Of these, 56 had posterior semicircular canal BPPV, 27 had lateral semicircular canal BPPV, and 19 had cupulolithiasis. Anterior semicircular canal BPPV was not observed in this study. There were 66 patients in the short-course group and 36 patients in the long-course group (Table 1).
Demographics of all patients included in this study.

We used a 7-day threshold to classify the disease course: patients with an interval of 7 days or less between onset and CRP treatment were classified as the short-course group, while those with an interval of 8 days or more were classified as the long-course group.
CRP
Diagnosis and CRP methods. All patients underwent Dix–Hallpike and roll tests for examination and diagnosis. The diagnosis was confirmed by two doctors based on the manifestations of nystagmus observed during the positional tests. Posterior semicircular BPPV were diagnosed by Dix–Hallpike with torsional nystagmus. Lateral semicircular BPPV is diagnosed with ground-oriented nystagmus with a duration of less than 1 minute on roll test. Cupulolithiasis BPPV was diagnosed with an out-of-ground nystagmus that lasted longer than 1 minute on roll test.
We chose the CRPs according to the strongly recommended in the clinical practice guideline by AAO_HNS in 2017. 2 Patients with PSC-BPPV were treated with the Epley maneuver, and patients with geotropic or ageotropic type of HSC-BPPV were treated with the Barbecue maneuver or Gufoni maneuver, respectively. 2 The CRP could be repeated up to three times within the same session. The criteria for diagnosis and successful repositioning followed the 2017 clinical practice guidelines by AAO-HNSF.
Assessment of residual symptoms after successful reduction
All patients were evaluated using the DHI scale, as recommended in the BPPV diagnosis and treatment guidelines, 2 before treatment and 7–10 days after successful repositioning. All patients were followed up in face-to-face sessions. The DHI scale comprises 25 items that evaluate symptoms associated with dizziness or vertigo across three dimensions: Physical (DHI-P, seven items), Functional (DHI-F, nine items), and Emotional (DHI-E, nine items). Each item has three possible responses: “yes,” “sometimes,” or “no,” corresponding to scores of 4, 2, and 0, respectively. A score of 0 indicates the absence of residual symptoms. In this study, the scores for each domain and the total DHI score were calculated, with higher scores indicating more pronounced residual symptoms.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics 25.0 (Chicago, IL, USA) and Prism 9 (Version 9.4.1) for graphical representation. The chi-square test was employed for the analysis of count data. The scores for the DHI dimensions did not conform to a normal distribution, and their values are expressed as mean ranks. The non-parametric Mann–Whitney U test was applied for comparisons between groups, within groups, and before and after CRP treatment. Statistical significance was defined as p < 0.05.
Results
Comparison of clinical characteristics of the short-course group and long-course group
A total of 102 patients with BPPV were included in this study. Of these, 66 patients were classified into the short-course group, and 36 patients were classified into the long-course group. The mean duration of the short-course group was 3.54 ± 2.41. The mean duration of the long-course group was 18.22 ± 7.95. The differences in gender composition, age, BPPV type, and side distribution between the two groups were not statistically significant (p > 0.05). The distribution of cases by gender, age, side, and BPPV type in the two groups is presented in Table 2.
Comparison of demographic characteristics between the short-course and long-course groups.

Comparison of DHI scores between the short-course group and the long-course group
Before CRP, a statistically significant difference in DHI scores was observed between the short-course and long-course groups (35.4 ± 18.93 vs. 47.22 ± 23.28, p = 0.009). The long-course group had higher DHI scores, indicating more severe vertigo symptoms before CRP (see Table 3). The DHI scores differed significantly between the two groups after CRP (8.85 ± 15.20 vs. 24.89 ± 25.56, p = 0.002). The higher DHI scores in the long-course group suggest that these patients had more pronounced residual symptoms after CRP. The difference in DHI scores before and after CRP was not statistically significant. These results suggest that the duration of BPPV does not affect the overall effectiveness of CRP, but patients in the longer-duration group may experience more pronounced residual symptoms, as shown in Figure 2.
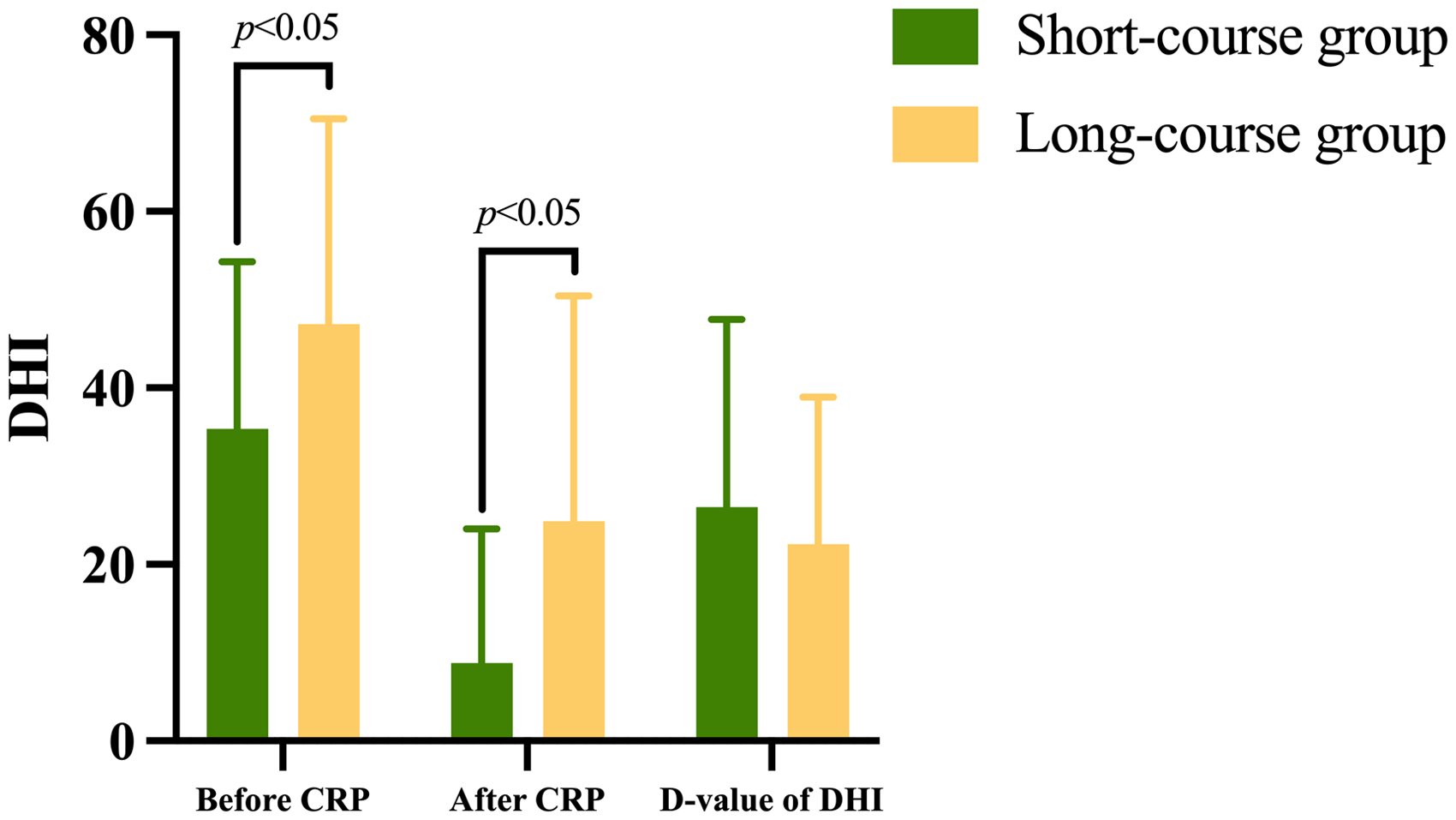
Comparison of total DHI scores before and after CRP between the two groups. Before and after CRP, the long-course group had a higher DHI score. The difference was significantly different.
Comparison of total DHI score before and after CRP.

Comparison of DHI scores in different dimensions before and after CRP between the short-course group and the long-course group
Before CRP, statistically significant differences in DHI-P, DHI-F, and DHI-E scores were observed between the two groups (p < 0.05), suggesting that the longer course had a significant impact on patients (Figure 3). After CRP, statistically significant differences in DHI-P, DHI-F, and DHI-E scores were still present between the two groups (p < 0.05), with the long-course group showing much higher scores (Figure 4). This indicates that patients in the long-course group experienced more pronounced residual symptoms, including physical, functional, and emotional symptoms, after successful CRP (Table 4).
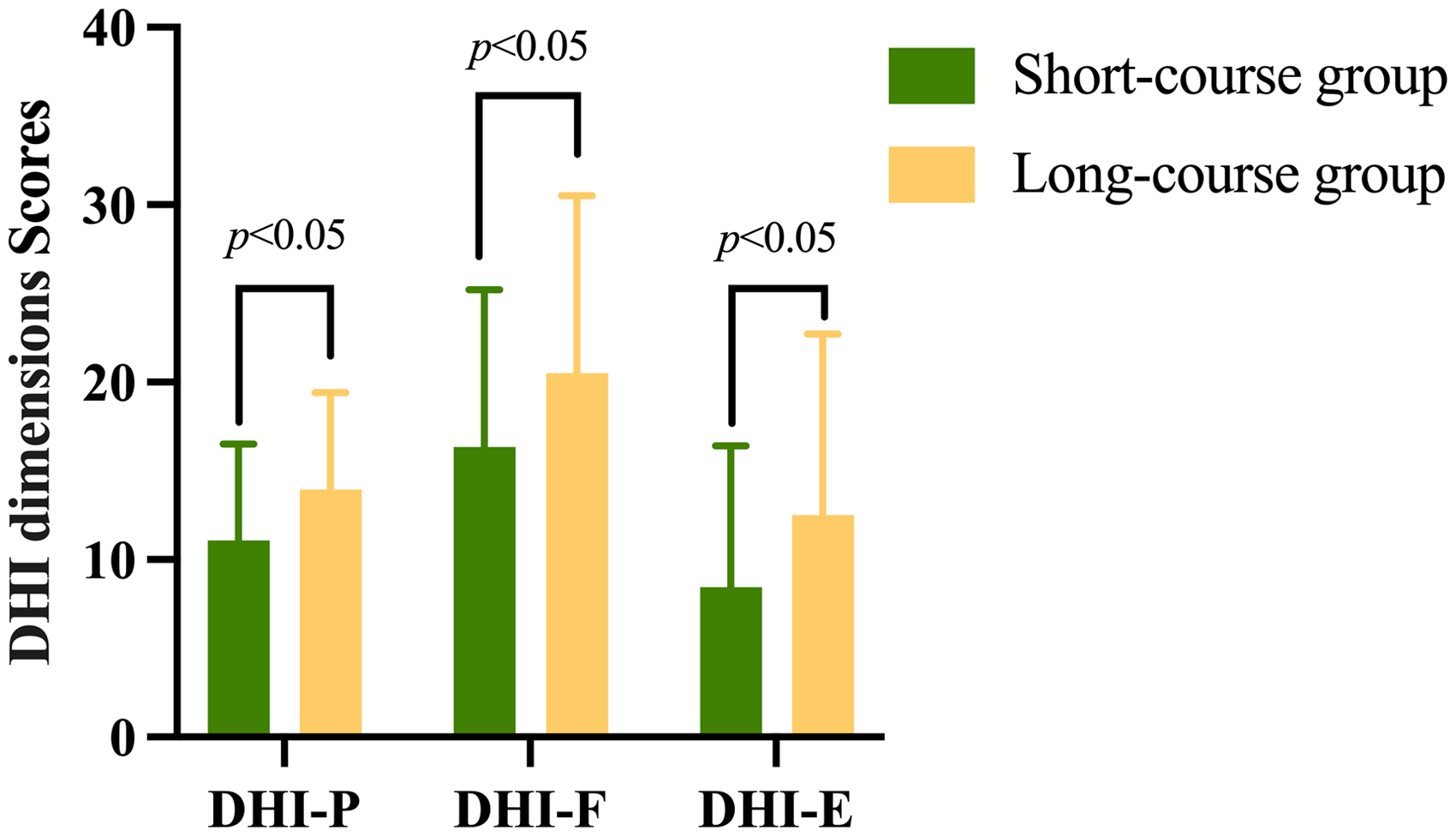
Comparison of different dimensions scores of DHI before CRP between the two groups. Before CRP, the scores of long-course group were much higher. p < 0.05 means statistically significant.

Comparison of different dimensions scores of DHI after CRP between the short-course group and the long-course group. After CRP, the scores of long-course groups were much higher; p < 0.05 means statistically significant.
Comparison of different dimensions scores of DHI before CRP between the short-course group and the long-course group.

The changes in DHI-P, DHI-F, and DHI-E scores before and after CRP were not statistically significant within either group (p > 0.05), as shown in Table 5. This suggests that while symptoms improved across different dimensions after CRP, the duration of the disease did not affect the extent of symptom reduction (Figure 5).
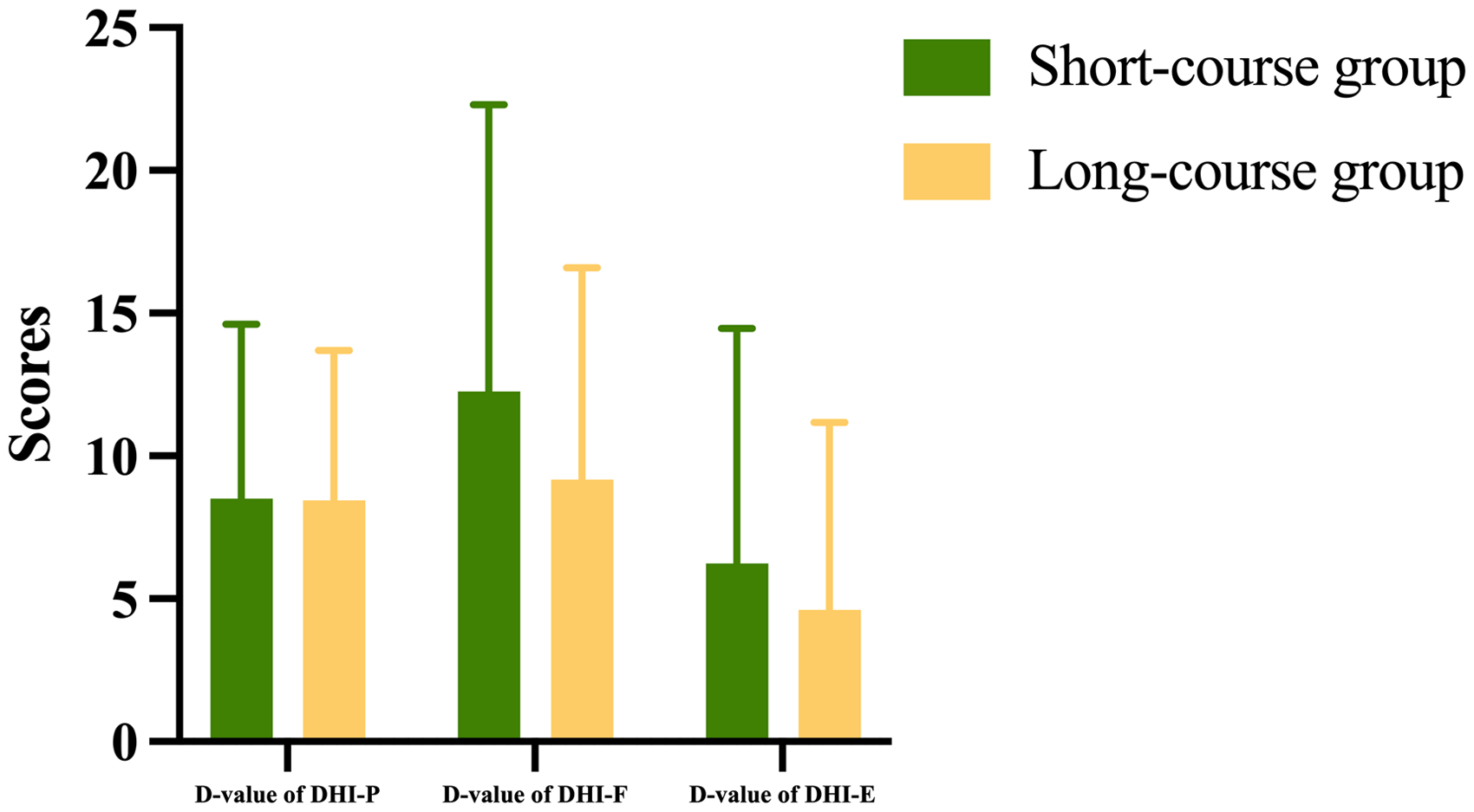
Comparison of difference in the scores of DHI-P, DHI-F, and DHI-E before and after CRP between the short-course group and the long-course group. p < 0.05 means statistically significant.
Comparison of the D-value of different dimensions of DHI before and after CRP.
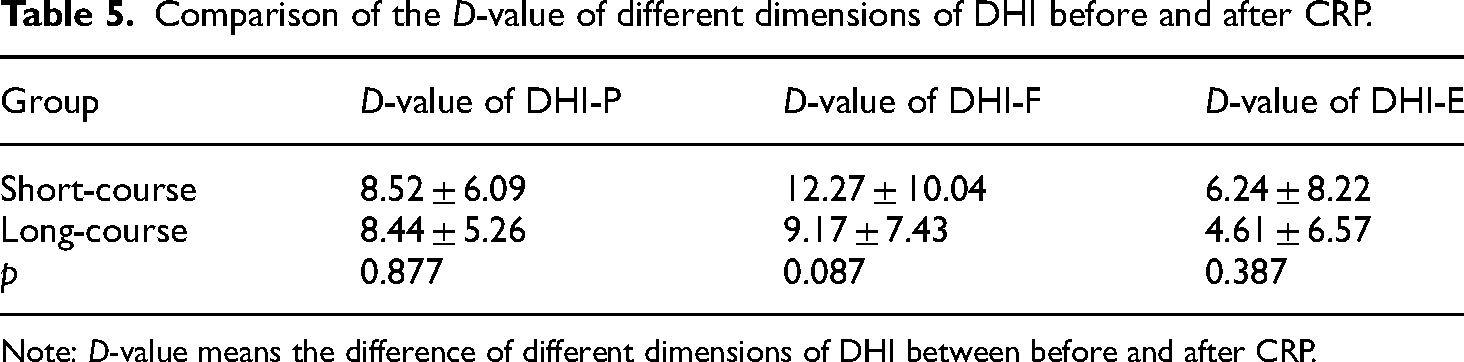
Note: D-value means the difference of different dimensions of DHI between before and after CRP.
Discussion
In this study, we found that patients with a long course of disease had higher DHI scores before and after treatment than those with a short course of disease.
Studies have shown that the DHI scale can quantify the impact of vestibular disease on quality of life 12 and predict the risk of residual symptoms after CRP treatment. Higher DHI scores prior to repositioning are significantly correlated with an increased risk of residual symptoms after treatment.13,14 We compared the total DHI scores of patients with different durations of BPPV before and after CRP. The results showed that patients in the long-course group had significantly higher DHI scores before CRP compared to those in the short-course group (Figure 2). This statistically significant difference indicates that patients with a longer course of BPPV are at a greater risk of residual symptoms after CRP. After CRP, we further compared the total DHI scores of the two groups. The long-course group had significantly higher scores than the short-course group, suggesting that patients with a longer disease duration exhibited more pronounced residual symptoms after CRP. Therefore, we conclude that a longer duration of BPPV before CRP is associated with a higher probability of residual symptoms after CRP. This finding is consistent with the study by Teggi et al., 3 which demonstrated that residual symptoms are associated with the duration of BPPV, with a longer disease duration before CRP linked to a higher risk of residual symptoms after CRP.
We further compared the DHI scores across each dimension between the two groups before CRP. Before CRP, patients in the long-course group had significantly higher scores across all three DHI dimensions compared to the short-course group (Figure 3). This indicates that a longer duration of BPPV before CRP is more likely to adversely affect a patient's physical activity, social functioning, and psychological state. Previous studies have found that the longer the duration of BPPV, the higher the level of anxiety exhibited by patients, and the longer the duration of residual symptoms. 15 A meta-analysis suggested that psychological factors play a particularly important role in the development of residual symptoms. 16 Some studies have also observed that residual symptoms are more prevalent among patients with anxiety disorders.4,17 Our study further indicates that a longer duration of BPPV before CRP increases the likelihood of patients developing psychological problems, such as stress, anxiety, or depression. Some patients with psychological stress develop phobic postural vertigo after BPPV. 18 Some authors have suggested that psychological evaluation and treatment of BPPV patients before CRP may improve therapeutic outcomes and reduce the occurrence of residual symptoms. 17
After CRP, patients in the long-course group had significantly higher DHI scores across all dimensions compared to those in the short-course group (Figure 4). It can be concluded that residual symptoms were more pronounced in the long-course group after successful repositioning. These symptoms manifested not only in physical activities but also in various aspects of social functioning and psychology, leading to an increased risk of falls and fear of falling. Consequently, patients tended to reduce their daily and social activities. Psychosomatic symptoms, such as anxiety and fear, may persist after successful repositioning and could lead to chronic subjective dizziness. 19 Previous studies have found that most residual symptoms resolve within 3 months of BPPV onset, 3 which is inconsistent with the diagnostic criteria for PPPD, but about 12.5% of patients with residual symptoms develop PPPD. 20 It may have something to do with anxiety. 21 Compared with VM and MD, the conversion ratio of BPPV to PPPD is low. And PPPD is more common in patients with the first episode of BPPV. 22 Therefore, Martellucci et al. 23 suggested that resuming daily physical activity as soon as possible after CRP might reduce the occurrence of residual symptoms. Faralli et al. 8 concluded that prolonged vertigo before CRP treatment might have a psychological impact on residual symptoms. This finding also prompts us to focus not only on the recovery of physical and social functioning in patients with a longer duration of BPPV but also on their psychological status and the remission of residual symptoms after repositioning treatment. Some authors believe that anxiety can cause patients to lose confidence and interfere with daily life, 14 and that anti-anxiety treatment can help patients return to their daily activities more quickly. 24
Seo et al. studied 44 patients with BPPV, dividing them into non-RD and RD groups based on the 1-week post-CRP review results. They found no statistically significant difference between the two groups regarding the duration of symptoms and disease. 16 Additionally, Babac et al. 25 retrospectively analyzed the outcomes of 400 BPPV patients treated with manipulative repositioning and found that the duration of the disease did not affect the prognosis. In this study, we compared the differences in total DHI scores and the scores of each dimension between the two groups before and after CRP. The results indicated that these differences were not statistically significant, suggesting no difference in the improvement of vertigo symptoms between the two groups after CRP (Figure 5). These results suggest that the duration of the disease does not affect the efficacy of CRP, consistent with previous findings.15,19 However, their studies did not focus on whether patients experienced residual symptoms after CRP treatment.
The hypothesized mechanism by which patients with long-course BPPV are more likely to develop residual symptoms after CRP involves the prolonged presence of free otoliths in the semicircular canal. This may alter the lymphatic fluid microenvironment within the membranous labyrinth, damaging the vestibular hair cells of the semicircular canal jugular crest. As a result, abnormal peripheral vestibular function occurs, causing the central vestibular system to take longer to compensate, ultimately leading to residual symptoms after CRP. Long-term otolith loss may also affect the function of the otolith organ, making the patient more susceptible to residual symptoms. Prolonged otolith deficiency may also impact utricular function, further predisposing patients to residual symptoms.
There are also some limitations to this study. Firstly, the follow-up period is short and should be extended to better assess the persistence of residual symptoms. Secondly, this study is a single-center study, and further multi-center prospective, randomized, controlled studies are needed to provide more reliable clinical evidence. Thirdly, for the posterior semicircular BPPV, we chose Epley repositioning. Studies have shown that compared with Semont repositioning, Epley repositioning reduces dizziness faster after treatment. 26 At present, there is no literature to show whether the two CRP methods have different effects on residual symptoms. In the later stage, we need to further select posterior semicircular duct BPPV patients and group them according to different reduction techniques to compare residual symptoms after reduction between the two groups. Finally, we did not assess vestibular function in patients with residual symptoms, nor did we examine whether there was a relationship between pre-CRP abnormal vestibular function and residual symptoms after CRP in BPPV patients. Future studies should investigate the full vestibular function of BPPV patients prior to CRP and examine the association between pre-CRP vestibular function and the development of residual symptoms after CRP. If CRP is not effective, we do not rule out central-positional nystagmus, 27 which is outside the scope of our study.
Conclusions
In conclusion, the risk of residual symptoms after successful CRP is associated with the duration of BPPV prior to CRP. The longer the duration, the greater the risk of residual symptoms, which can manifest in physical, social, and psychological aspects. If residual symptoms develop after successful CRP, it is important to provide not only vestibular rehabilitation or medication to improve physical and social functioning but also psychological support to alleviate anxiety.
Footnotes
Authors’ contribution
Jun Yang, Shuna Li, and Jianyong Chen contributed to the study design and manuscript revision; Lixin Gu and Jianyong Chen performed CRP; Jiali Shen, Jin Sun, and Lu Wang collected and collated data. Lixin Gu, Dekun Gao, and Xiaobao Ma contributed to the statistical analysis and manuscript draft. Yulian Jin, Xiangping Chen, and Qing Zhang devoted the study proposal. All authors helped to perform the analysis and to revise the manuscript with constructive discussions.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to the privacy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Ethics Committee (Xinhua Hospital Affiliated with Shanghai Jiaotong University School of Medicine) (approval number/protocol number XHYY-2021-039). The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association's Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant Nos. 82171135, 82371140, and 82230035) and the Shanghai Jiaotong University Medical-Industrial Intersection Key Project (Grant No. ZH2018ZDA11).
Informed consent
Written informed consent was obtained from each participant/patient for study participation and data publication.