
Abstract
This study aimed to investigate the clinical manifestations of pediatric clonazepam poisoning and to analyze treatment strategies based on its pharmacokinetic characteristics, thereby providing evidence for the clinical management of such cases. A retrospective analysis was conducted on four pediatric patients with clonazepam overdose admitted to our hospital between January 1 and December 31, 2024. Clinical data, including demographic information, clinical manifestations, treatment procedures, and outcomes, were collected and analyzed. Rescue strategies were evaluated in conjunction with the pharmacokinetic properties of clonazepam. All four children presented with varying degrees of dizziness, vomiting, and ataxia following clonazepam ingestion. Gastric lavage was promptly performed in all cases upon hospital admission. Cases 1 and 3 received the specific antidote flumazenil, while cases 1 and 2 underwent hemoperfusion and combined hemoperfusion–continuous venovenous hemofiltration therapy, respectively. All cases achieved complete recovery. Notably, in the two cases treated with hemoperfusion, plasma clonazepam concentrations declined more rapidly than the theoretical elimination time, suggesting that extracorporeal blood purification may facilitate drug clearance in cases of high-dose poisoning. Pediatric clonazepam poisoning is primarily characterized by dose-dependent central nervous system depression. In cases involving large doses or multiple drug overdoses, hemoperfusion may be considered on a case-by-case basis to help reduce plasma drug concentrations; however, further studies are required to confirm its clinical efficacy. Additionally, greater attention to adolescent mental health—particularly during puberty—and enhanced education on medication safety are essential to prevent such poisoning incidents.
Keywords
Introduction
Acute poisoning refers to a series of pathophysiological changes and clinical manifestations that occur when the body is exposed to toxic substances or a drug overdose within a short period. The condition is often complex and progresses rapidly, potentially leading to multiple organ dysfunction or failure, and in severe cases, can be life-threatening. 1 Children, as a particularly vulnerable population, are at high risk of acute poisoning due to their limited awareness of safety and self-protection. Poisoning can occur at any age during childhood. Studies have shown that, aside from cases involving self-administration of antipsychotic drugs, the highest incidence of poisoning occurs in children aged 1–3 years (54.2%) and 8–14 years (27.4%), with the preschool age group accounting for the largest proportion. 2 Pediatric acute poisoning is one of the most common emergencies in pediatric care, accounting for approximately 0.2–1% of daily visits to pediatric emergency departments, 3 with 4.6% of affected children requiring hospitalization or admission to intensive care units. 4 Over the past decade, the annual incidence of depression among children worldwide has reached 1.3%, and it increases sharply during adolescence and young adulthood, particularly in females. 5 In the United States, the prevalence of depression among adolescents aged 13–18 has been reported to reach 11.0%. 5 Intentional overdose is one of the most common methods of suicide in individuals with depression, and the incidence of drug poisoning among children with depression has been steadily increasing. Among these cases, benzodiazepine poisoning is the most frequently reported. 6
Clonazepam is a long-acting benzodiazepine with a duration of action of approximately 6–8 h. It possesses a relatively low molecular weight (315.76 g/mol), exhibits a high plasma protein-binding capacity of about 80%, and demonstrates high lipid solubility (log P ≈ 2.8), facilitating its wide distribution within the body. Clonazepam is primarily metabolized by the hepatic enzyme CYP3A4 and undergoes first-order elimination kinetics, with a reported elimination half-life ranging from 26 to 49 h. The therapeutic range of clonazepam is 0.02 to 0.07 μg/mL. 7 Clonazepam is commonly used in clinical practice to control epileptic seizures and treat anxiety disorders in children. Due to its sedative properties, clonazepam is also effective in alleviating mild to moderate emotional and neuropsychiatric symptoms, and is therefore often used as an adjunctive treatment for depression and anxiety. 8 As a central nervous system (CNS) depressant, accidental ingestion of clonazepam by children can result in serious adverse effects such as impaired consciousness and respiratory depression, and may even be life-threatening. In recent years, benzodiazepine poisoning has emerged as a significant issue in pediatric populations. The trend has been well-documented in poisoning case reports from the United Kingdom, and the number of pediatric exposures reported in the United States has been steadily increasing as well.9,10 Prompt and effective treatment is therefore critical in managing such poisonings. Flumazenil is currently the only specific antidote available for benzodiazepine poisoning. In addition to flumazenil administration, symptomatic and supportive care remains the mainstay of treatment. Because benzodiazepines exhibit high plasma protein binding and a large volume of distribution, extracorporeal blood purification therapy may be considered in cases of severe intoxication.11,12 Several reports have documented successful use of blood purification techniques in patients with life-threatening benzodiazepine overdose.11,13 This study reviews the clinical characteristics, treatment processes, and outcomes of four pediatric cases of clonazepam poisoning. By integrating these findings with the pharmacokinetic profile of clonazepam, we aim to summarize the clinical features and treatment strategies associated with clonazepam toxicity, providing valuable insights for clinical practice.
Case presentation
Methods
Study subjects
A retrospective analysis was conducted on the medical records of four pediatric patients with clonazepam poisoning who were admitted to Children's Hospital of Nanjing Medical University between January 1, 2024 and December 31, 2024. Case 1 was admitted in March 2024, case 2 was admitted in May 2024, case 3 was admitted in April 2024, and case 4 was admitted in May 2023.
Written informed consent for treatment was obtained from all patients’ guardians, and all patient information has been fully de-identified to ensure confidentiality. The reporting of this study conforms to the CARE guidelines. 14 This study was approved by the Ethics Committee of the Children's Hospital of Nanjing Medical University, China, on July 2, 2025 (Approval number: 202506034-1).
Data collection
All case information was obtained from the Hospital Information System. The following clinical data were collected: patients’ demographic information (including age and sex), underlying medical conditions, types and dosage of ingested drugs, time of presentation, clinical manifestations, diagnosis, time from ingestion to gastric lavage, use of specific antidotes, findings from auxiliary examinations, treatment procedures, clinical outcomes, and length of hospital stay.
Rescue strategies included the administration of specific antidotes, symptomatic and supportive therapy, and the use of extracorporeal blood purification.
Results
General information of the pediatric patients
Among the four children, one was male and three were female. Two children under the age of 2 accidentally ingested clonazepam, with the exact dosage unknown. The other two cases involved adolescent girls with varying degrees of depression who intentionally overdosed on clonazepam. Case 1 also had an overdose of lithium carbonate concurrently. Detailed information is presented in Table 1.
Clinical characteristics of pediatric patients with clonazepam poisoning.
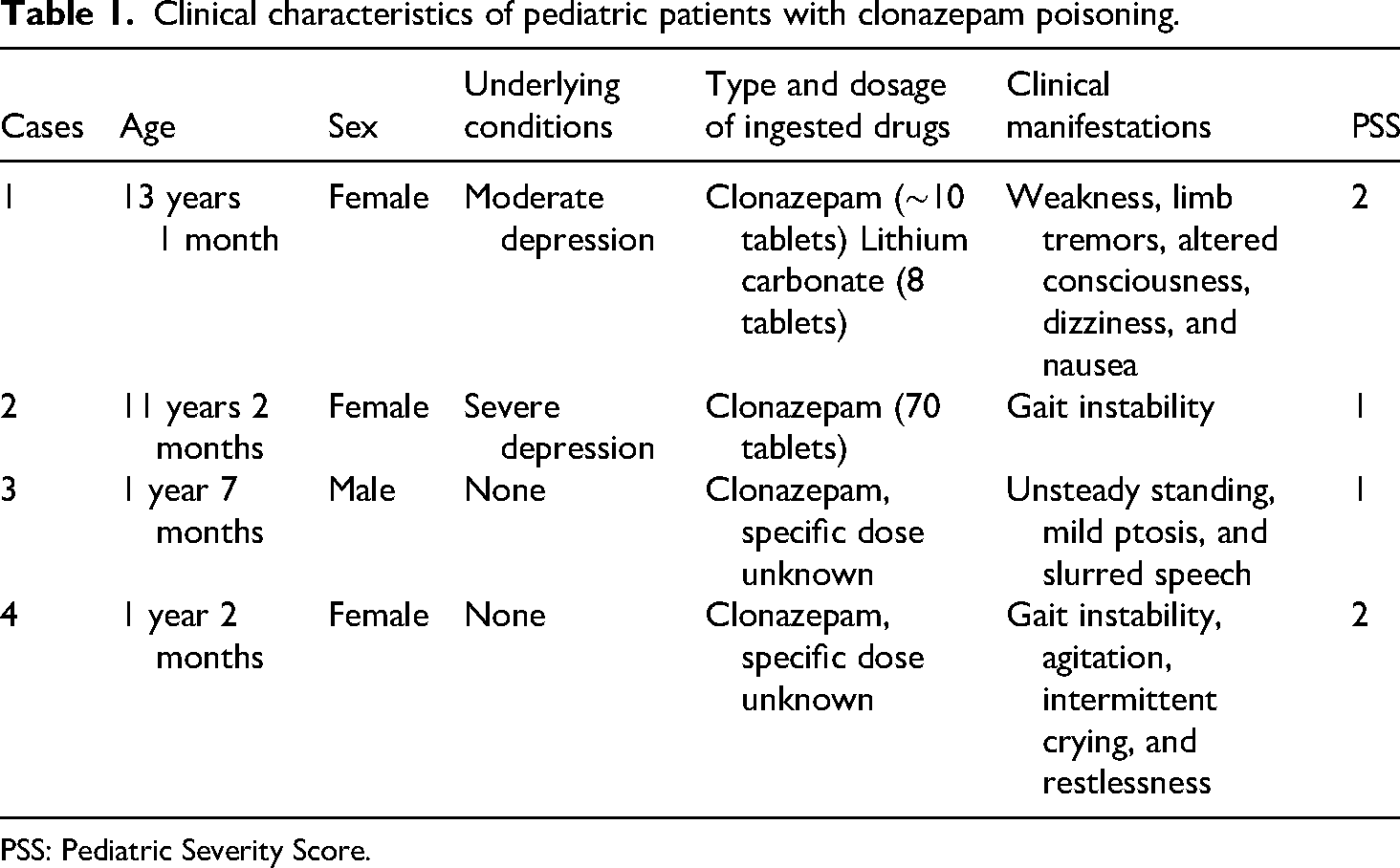
PSS: Pediatric Severity Score.
Clinical data of the pediatric patients
Clinical manifestations
All four children exhibited varying degrees of CNS depression within 1–2 h after clonazepam ingestion. Common symptoms included unsteady standing or gait (4/4), altered consciousness or psychiatric disturbances (3/4), and some patients also experienced limb tremors, dizziness, nausea, and speech disturbances. Case 4 showed signs of agitation or emotional instability. These clinical features were consistent with the known sedative, muscle relaxant, and vestibular effects of clonazepam. Upon admission, the Pediatric Severity Score for the four cases was 2, 1, 1, and 2, respectively. 15 Detailed clinical manifestations are summarized in Table 1.
Auxiliary examinations
Arterial blood gas analysis in case 2 revealed mild respiratory acidosis (elevated PaCO2). Blood biochemistry, complete blood count, cardiac injury markers, coagulation profiles, and liver and renal function tests were all normal ranges in all four patients.
Therapeutic drug monitoring
Serum clonazepam concentrations were monitored in all four cases after hospital admission. In cases 1, 2, and 3, the serum levels exceeded the therapeutic range, while case 4's level remained within the therapeutic window. Cases 1 and 2 underwent re-evaluation of serum clonazepam levels after blood purification therapy. In case 1, the post-treatment level was 53.9 μg/L, within the therapeutic range. In case 2, the concentration was 119.5 μg/L, still above the therapeutic range. However, due to significant clinical improvement, no further testing was performed. Based on the pharmacokinetic properties of clonazepam, the theoretical elimination half-lives were calculated as 66.6–195.4 h for case 1 and 40.7–118.7 h for case 2, respectively. However, after blood purification therapy, the actual elimination times were significantly shorter, 10.5 and 8 h, respectively. Details are presented in Table 2.
TDM results in four pediatric patients with clonazepam poisoning.

TDM: therapeutic drug monitoring.
Treatment and outcomes
All four cases received gastric lavage and activated charcoal therapy. Three of them underwent these procedures within 4 h of admission. Case 1, who had co-ingested clonazepam and lithium carbonate, underwent lavage approximately 15 h post-ingestion. Following gastric decontamination, all cases received symptomatic and supportive care, including naloxone for arousal, omeprazole for gastric protection, lactulose to enhance intestinal motility, and intravenous fluid replacement. Cases 1 and 3 received benzodiazepine antagonist flumazenil. Additionally, both cases 1 and 2 underwent blood purification therapy without complications. After hemoperfusion, the consciousness of case 1 improved significantly, and plasma concentrations of lithium carbonate and clonazepam decreased markedly compared with pre-treatment levels, therefore, hemoperfusion was discontinued. Case 2 maintained a stable mental status after blood purification, and due to the short treatment course, the parents requested discharge for home observation. Case 1 underwent hemoperfusion for approximately 3.5 h, whereas case 2 received 8 h of hemoperfusion followed by continuous venovenous hemofiltration (CVVH). In case 2, two series of combined CVVH and hemoperfusion treatments were performed: the first session lasted 20 h and 20 min, and the second session lasted 19 h and 40 min. All patients showed clinical improvement and were discharged within 3 to 5 days. No neurological sequelae were observed during follow-up. Details are summarized in Table 3.
Treatment and outcomes in pediatric patients with clonazepam poisoning.

CVVH: continuous venovenous hemofiltration.
Discussion
Clonazepam is a representative benzodiazepine primarily used for the management of epilepsy and status epilepticus. 7 It has been widely prescribed for over four decades to treat seizures in both pediatric and adult patients, including severe childhood epileptic syndromes such as Lennox–Gastaut syndrome, absence seizures, and myoclonic seizures, as well as panic disorders in the United States. 16 Clonazepam exerts potent CNS depressant effects by enhancing γ-aminobutyric acid type A (GABA-A) receptor activity, thereby inhibiting neuronal excitability. However, it has addictive potential and is associated with rapid development of tolerance. 17
Acute poisoning can occur after ingestion of a large dose of clonazepam. Overdose of benzodiazepines is a relatively common reason for hospital admission in pediatric patients. 10 Symptoms of benzodiazepines poisoning typically appear within 4 h after medication. 18 The most common manifestations include somnolence, dizziness, slurred speech, confusion, and ataxia. 18 More than 90% of affected children develop ataxia, which is considered the most common symptom of pediatric benzodiazepine toxicity, while respiratory depression is less common and occurs in fewer than 10% of cases. 19 Children are more vulnerable to CNS depression due to the immaturity of hepatic enzyme systems, which leads to slower drug metabolism, reduced clearance, and prolonged elimination half-life. 20 Moreover, the high lipid solubility and large volume of distribution of clonazepam contribute to the prolonged duration of toxic symptoms. The CNS depressant effect is dose-dependent; because of their lower body weight, children may experience a relatively higher dose per kilogram, exacerbating the severity of intoxication. In addition, co-ingestion of other medications may further aggravate toxicity. 21 In the present study, the main clinical manifestations in the four pediatric patients included unsteady standing or gait, muscle weakness, altered consciousness, and emotional disturbances. These symptoms were consistent with the known pharmacological effects of clonazepam. Notably, case 1 had also taken a high dose of lithium carbonate, which may have contributed to symptoms such as limb tremors and confusion.
Benzodiazepine ingestion for more than 4 h may lead to recurrent or periodic coma due to delayed drug absorption. Therefore, gastric lavage should be performed as early as possible to remove any unabsorbed drug following benzodiazepine poisoning. 18 Administration of activated charcoal is only recommended within 1 h after oral intake of the toxic substance. 22 In this study, three of the four children underwent gastric lavage within 6 h of ingestion. However, case 1 developed more severe symptoms, which may be attributed to the longer time interval between ingestion and gastric lavage, as well as the combined intake of lithium. None of the four cases received activated charcoal within the recommended 1-h window.
Supportive care remains the cornerstone of treatment for acute benzodiazepine poisoning and includes close monitoring of vital signs, respiratory support, and fluid replacement therapy. In patients who develop significant consciousness impairment after charcoal administration, or are at risk of progressive neurological deterioration, airway protection should be ensured, and endotracheal intubation should be considered if necessary. Flumazenil, a structural analog of benzodiazepine with minimal intrinsic activity, is currently the only specific antidote available for benzodiazepine poisoning. It acts by competitively binding to the benzodiazepine site of the GABA-A receptor complex, thereby antagonizing the potentiating effects of benzodiazepines on GABA-mediated neurotransmission. This mechanism reduces receptor activation, closes chloride ion channels, and inhibits excessive inhibitory synaptic transmission, resulting in arousal and reversal of sedation. 23 Flumazenil has a short elimination half-life of approximately 50 min and is rapidly metabolized by the liver. In pediatric patients, the recommended dose of flumazenil is 0.01 mg/kg (not exceeding 0.2 mg per dose), with a maximum total dose of 1 mg or 0.05 mg/kg. In most cases, treatment is initiated with an intravenous infusion of 0.1–0.3 mg of flumazenil. The effect of a single administration typically lasts for less than 1 h. 24 Therefore, comatose patients receiving flumazenil should be closely monitored, and additional intravenous boluses or continuous infusions should be administered as clinically indicated. 25 However, its use in pediatric patients remains controversial, as several studies have reported adverse effects such as seizures. 26 Data from the US Food and Drug Administration Adverse Event Reporting System database from 2004 to 2023 revealed a significant association between flumazenil and neurological adverse reactions, including “withdrawal seizures” and “psychogenic epilepsy.” The risk was particularly elevated among patients with long-term benzodiazepine exposure. In that dataset, the median age of affected patients was 44 years old, and the primary routes of administration were “other routes” and intravenous injection, with a small number of cases involving subcutaneous administration. 27 Therefore, flumazenil should be used with caution and only after careful clinical evaluation, while symptomatic and supportive therapy remain the cornerstone of treatment. In our study, cases 1 and 3 received flumazenil to reverse the effects of clonazepam, and no adverse reactions were observed.
Although benzodiazepine overdose rarely results in death, large doses or concomitant use with other substances may lead to severe CNS depression and potentially life-threatening conditions. Therefore, when multiple drugs are ingested in overdose, a combination of therapeutic approaches should be considered to achieve optimal detoxification and clinical recovery. 17 In this study, case 1 had ingested both clonazepam and lithium carbonate. Considering the pharmacokinetic properties of these two agents, hemoperfusion combined with flumazenil administration appeared to contribute to clinical recovery, although causality cannot be confirmed. Previous studies have shown that hemoperfusion can be used as an adjunct to antidotal therapy, helping to shorten the duration of antidote use and intensive care unit stay, thereby improving prognosis. 28 However, extracorporeal therapies carry certain risks, including complications related to vascular access and anticoagulation-induced bleeding. 29 Moreover, blood purification may lead to excessive clearance of specific antidotes, potentially compromising their therapeutic effect. Therefore, prior to initiating blood purification, clinicians should comprehensively evaluate the patient's condition, the pharmacological characteristics of the ingested substances, and the urgency of treatment, balancing the risks and benefits. Flumazenil, with its high clearance and short half-life (∼50 min), often requires repeated administration to maintain efficacy, especially in poisonings involving long-acting benzodiazepines such as clonazepam. 28 Consequently, the impact of blood purification on the overall elimination of clonazepam may be limited. Nevertheless, hemoperfusion remains one of the preferred treatments for severe poisoning, 30 particularly for substances with small molecular weight, high lipid solubility, and strong protein-binding characteristics all applicable to clonazepam. While hemoperfusion can effectively reduce serum drug concentrations, it may be followed by a “redistribution phenomenon,” wherein the toxin re-enters the bloodstream from peripheral tissues, potentially leading to symptom recurrence. 30 In such cases, short-duration intermittent hemoperfusion sessions, combined with antidotal therapy (e.g. flumazenil), fluid resuscitation, and diuretics, may be necessary to promote drug clearance. 31 Case 2 had a history of single-episode polypharmacy overdose and presented with a large ingestion of clonazepam and poor mental status upon this admission. Based on the high risk of toxicity and overall clinical evaluation, combined treatment with continuous renal replacement therapy (CRRT) and hemoperfusion was initiated. CRRT is an extracorporeal blood purification modality that mimics renal function, offering continuous and gradual removal of fluid and solutes over a 24-h period. It has advantages such as hemodynamic stability, gentle solute clearance, and isotonic fluid removal, making it widely used in critically ill patients. 32 Current CRRT modalities include CVVH, continuous venovenous hemodialysis, continuous venovenous hemofiltration, slow continuous ultrafiltration, coupled plasma filtration adsorption, endotoxin adsorption, plasma exchange, and double filtration plasmapheresis. 32 In this case, the CVVH mode was selected, which is among the most commonly used approaches. CVVH removes excess fluid via ultrafiltration and uses convection transport for efficient solute clearance, particularly effective for middle- and large-molecule toxins. 33 Hemoperfusion may be used alone or in combination with CRRT. When applied in series, hemoperfusion enables the rapid removal of lipid-soluble, highly protein-bound substances, whereas CRRT facilitates the continuous clearance of middle-to large-molecule toxins. Previous studies have demonstrated that this combined regimen can help stabilize circulatory dynamics, shorten the duration of toxic symptoms, and improve patient outcomes. 34 Theoretically, this combined approach may provide a synergistic detoxification effect, potentially enhancing overall therapeutic efficacy, however, further clinical evidence is needed to confirm these findings. In contrast, cases 3 and 4 were younger and had milder clinical symptoms resulting from accidental ingestion. Given their stable vital signs and rapid clinical improvement with supportive care alone, blood purification therapy was deemed unnecessary in these cases.
In cases 1 and 2, plasma clonazepam concentrations were measured before and after blood purification therapy. Case 1's serum clonazepam level decreased from 165.0 to 53.9 μg/L over 10.5 h, while case 2's concentration dropped from 236.9 to 119.5 μg/L within 8 h. These findings demonstrate a marked reduction in serum clonazepam levels, suggesting the efficacy of blood purification in enhancing drug clearance in these cases. Clonazepam elimination in vivo follows first-order kinetics, 30 with a median clearance rate of approximately 0.42 mL/min/kg and an apparent volume of distribution ranging from 1.5 to 4.4 L/kg in children aged 2–18 years. Using the pharmacokinetic formula: t = log(C0/Cₜ) × (2.303/ke), where ke = Cl/Vd, 30 we estimated the theoretical time required for natural elimination of clonazepam to reach the post-treatment plasma concentrations observed in the two patients. For case 1, the theoretical clearance ranged from 66.6 to 195.4 h, and for case 2, from 40.7 to 118.7 h—both far exceeding the actual clearance durations of 10.5 and 8 h, respectively. These results suggest the potential clinical value of blood purification in managing severe clonazepam poisoning in children. However, the economic and logistical aspects of such therapy must be considered. Techniques such as hemodialysis or hemoperfusion are resource-intensive and costly, which may limit their accessibility and routine use in pediatric intensive care units, particularly in low-resource settings. While the observed clinical improvement indicates possible accelerated detoxification, our study did not include serial clonazepam plasma measurements to directly quantify elimination rates. Therefore, conclusions regarding faster clearance remain theoretical and should be interpreted cautiously. Larger studies with serial pharmacokinetic monitoring are warranted to determine whether blood purification truly enhances clonazepam elimination and to evaluate its cost-effectiveness and safety in pediatric populations. Moreover, in patients receiving chronic benzodiazepine therapy, rapid drug removal by hemoperfusion may precipitate withdrawal symptoms or seizures due to sudden reductions in plasma concentrations. Careful patient selection and close monitoring are therefore essential when considering extracorporeal blood purification in such cases. While therapeutic drug monitoring (TDM) can provide valuable pharmacokinetic information, routine TDM during blood purification may not be necessary outside of research settings. A more practical approach may be to perform sequential TDM prior to initiating extracorporeal therapy to identify patients with delayed drug elimination who are most likely to benefit from advanced detoxification strategies.
Both cases 1 and 2 had a history of depression and developed poisoning as a result of intentional ingestion of large doses of medications prescribed for underlying psychiatric conditions. Notably, both patients were adolescents, an age group characterized by emotional sensitivity and susceptibility to interpersonal conflicts with peers or family members. The prevalence of depression among adolescents has been increasing in recent years, and self-harm behavior associated with depression during adolescence is often predictive of chronic, recurrent psychiatric disorders and physical harm in adulthood. 35 These findings underscore the urgent need for parents and society at large to pay greater attention to the mental health of adolescents. Early psychological intervention and counseling should be provided when signs of emotional distress are observed. In cases where depression is diagnosed, prompt medical treatment—including pharmacotherapy under medical supervision when necessary—is crucial to preventing serious consequences such as intentional drug overdose. In contrast, cases 3 and 4 were both under 2 years of age and experienced accidental ingestion of medications. Due to timely parental detection, both underwent gastric lavage within 2 h of ingestion and exhibited only mild poisoning symptoms. It is generally recommended that gastric lavage be performed as early as possible, ideally within 1 h of ingestion. However, in certain cases—such as delayed gastric emptying or ingestion of specific toxins—the lavage window may be extended to 4–6 h. In cases of severe poisoning with no specific antidote, gastric lavage may still be considered even beyond 6 h, based on clinical judgment. Given that most drug poisonings in infants result from inadequate supervision, these cases highlight the importance of caregiver vigilance. Proper medication storage and increased awareness among guardians are essential to preventing accidental pediatric poisoning.
Conclusion
This study summarizes four pediatric cases of clonazepam poisoning, providing insights into clinical management and emphasizing that early recognition and timely intervention are generally recommended in pediatric poisoning, based on clinical experience and prior references. According to the Chinese Expert Consensus on the Diagnosis and Treatment of Acute Poisoning, flumazenil, as the only specific antidote for benzodiazepine poisoning, plays a critical role in reversing sedation or coma in affected patients. 36 However, in cases with significantly elevated serum drug concentrations or combined drug overdose, flumazenil alone may be insufficient to reverse symptoms effectively. Under such circumstances, a combination of flumazenil administration with blood purification techniques can enhance drug clearance, shorten the duration of toxicity, and accelerate neurological recovery. The experience from these cases suggests that, in managing severe pediatric benzodiazepine intoxication, serum drug concentration monitoring, along with individualized blood purification strategies may be considered to optimize therapeutic outcomes and improve prognosis.
Footnotes
Ethical considerations
Written informed consent was obtained from the patients for publication of this case report. This study was approved by the Ethics Committee of the Children's Hospital of Nanjing Medical University, China, July 2, 2025 (Approval number: 202506034-1).
Consent for publication
The parents of the patients agreed to offer the clinical details and clinical images only for scientific research and publication.
Author contributions
Rong Zhuang drafted the initial manuscript, and reviewed and revised the manuscript.
Qin Zhang, Hongjun Miao, and Jin Xu discussed the topic and provided comments.
Wenjing Li critically reviewed the manuscript for important intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All patient information has been fully de-identified to ensure confidentiality.