
Abstract
Objective
This study aimed to systematically characterize the morphological patterns of proximal fibular fractures occurring concurrently with tibial plateau fractures.
Methods
Data were retrospectively collected from a Level-1 trauma center between January 2011 and January 2024 by querying hospital information and picture archiving and communication systems with keywords “tibial plateau fracture” and “fibular fracture” or “fibular head fracture.” Radiographic morphology was evaluated using standard anteroposterior radiographs and three-dimensional computed tomography (3D-CT), categorizing proximal fibular fractures into 13 predefined morphological patterns. Descriptive data, including fracture location, number of fragments, and degree of displacement, were recorded and classified. The distribution patterns of proximal fibular fractures were further correlated with the tibial plateau fractures, categorized according to the CT-based three-column classification system.
Results
A total of 223 eligible patients (123 males) were included in the analysis. Group I, II, and III proximal fibular fractures were observed in 63 (28.3%), 121 (54.3%), and 39 (17.4%) patients, respectively. Within group II, subtype II3p was the predominant fracture pattern, occurring in 61 patients (50.4%). Group I fibular fractures did not occur in tibial plateau posterior column or combined lateral and posterior column fractures. Group II fibular fractures were absent in tibial plateau lateral column or combined medial and lateral column fractures. Group III fibular fractures exclusively presented with combined lateral and posterior column or three-column tibial plateau fractures. Logistic regression indicated that group I proximal fibular fractures were significantly more associated with isolated medial column tibial plateau fractures, whereas group II fibula fractures were significantly associated with lateral-posterior and medial-posterior column tibial plateau fractures.
Conclusions
The morphological diversity observed in proximal fibular fractures underscores the complexity and heterogeneity of concomitant tibial plateau fractures. Further clinical and biomechanical investigations are warranted to elucidate the pathomechanics underlying comminuted fibular fractures associated with tibial plateau injuries.
Keywords
Introduction
Proximal fibular fractures constitute a common clinical entity, presenting either as isolated injuries or in conjunction with more complex knee or ankle trauma. Despite their prevalence, these fractures have often been overlooked in clinical assessment, resulting in insufficient characterization of their radiographic patterns in current orthopedic literature.1–3 Recent advances in the anatomical and biomechanical understanding of the posterolateral knee structures have underscored the clinical significance of proximal fibular fractures.3,4
The proximal fibula exhibits a distinct pyramidal anatomy, serving as an essential anatomical landmark for the fibular insertion points of key posterolateral corner (PLC) structures, including the fibular collateral ligament (FCL), popliteofibular ligament (PFL), and biceps femoris tendon.5–7 Given this anatomical configuration, the proximal fibula is critically involved in stabilizing the knee joint, particularly against varus loading, external rotation, and posterior tibial translation forces.7–9 Hence, comprehensive characterization of fracture patterns in this region is clinically important to better understand injury mechanisms and optimize therapeutic strategies.
Previous studies have offered valuable insights into specific fracture patterns such as arcuate fractures, correlating their radiographic features with the unique anatomy of the proximal fibula. 8 Our prior research similarly highlighted the frequent coexistence of proximal fibular fractures with tibial plateau fractures, prompting the development of a novel radiographic classification based on fracture location as visualized on plain X-rays. 1 Nevertheless, three-dimensional computed tomography (3D-CT) imaging has revealed substantially greater complexity and variability in proximal fibular fracture morphologies compared with traditional radiographic assessments. Thus, further in-depth morphological studies using advanced imaging modalities are warranted.
The present study addresses this knowledge gap by systematically evaluating proximal fibular fracture patterns using 3D-CT imaging. Specifically, we aimed: (1) to categorize proximal fibular fractures into defined morphological subtypes based on comprehensive 3D-CT analyses and anatomical considerations, and subsequently determine the distribution characteristics of these subtypes; (2) to investigate the associations between proximal fibular fracture morphologies and tibial plateau fracture subtypes according to the established CT-based three-column classification system. The findings of this study could facilitate a deeper understanding of knee injury patterns and serve as a reference for further clinical and biomechanical research.
Patients and methods
Study design and patient selection
This study retrospectively analyzed clinical and imaging data from patients admitted with tibial plateau fractures to the Department of Orthopedics at Gongli Hospital, affiliated with the Second Military Medical University, from January 2011 to January 2024 continuously. Eligible cases were identified using the hospital information system (Ruijin, China) with search terms “tibial plateau fracture” combined with “fibular fracture” or “fibular head fracture.” The study was approved by the Institutional Review Board of Gongli Hospital, and all methods were performed in accordance with the relevant guidelines and regulations. Due to the retrospective nature of the study, the need for informed consent was waived by the Institutional Review Board of Gongli Hospital.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki, as revised in 2024. All patient data were fully de-identified prior to analysis, and no identifiable personal information was included in this study. Given that this was a retrospective study, the Institutional Review Board (IRB) of Gongli Hospital determined that ethical approval was not required for this study, and the need for informed consent was waived. The reporting of this study conforms to the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology). 10
Exclusion criteria included:
Fibular hairline fractures or displaced segments < 2 mm Pathological fractures secondary to severe osteoporosis or tumor involvement. Concomitant fractures of the femur or distal tibia. Unsatisfactory radiographic or CT imaging, including poor patient positioning, image quality, or incomplete radiologic documentation.
Imaging and data acquisition
Radiographic data, including standard anteroposterior (AP) and lateral X-rays, as well as 3D-CT scans, were digitally retrieved from the hospital's picture archiving and communication system (PACS, Centricity; Jinshida, China).
Morphological classification of proximal fibular fractures
Based on fracture line characteristics and comminution patterns observed on 3D-CT scans, proximal fibular fractures concomitant with tibial plateau fractures were categorized into 13 predefined morphological conditions (Figure 1). These conditions were classified into three main groups:

Thirteen hypothetical conditions on proximal fibula fractures.
Group I (avulsion fractures): Horizontal fracture line primarily indicating ligamentous avulsion. I1: Small avulsion fractures limited to the fibular styloid. I2: Superior cortical rim avulsions involving the arcuate ligament complex (classic “arcuate fractures”). I3: Fractures extending through metaphyseal bone without comminution.
Group II (cleavage and comminution fractures): Cleavage and comminution fractures of the fibular head, subdivided according to involvement of anatomical columns based on the model described by Takahashi et al.
6
(medial, lateral, and posterior columns; Figure 2): II1p: Single-column fracture (M, L, or P). II2p: Two-column fractures (M + L, M + P, or L + P). II3p: Three-column fractures involving medial, lateral, and posterior aspects.

The proximal fibular structure into three columns (the proximal lateral column constitutes the attachment area for the fibular collateral ligament and the biceps femoris tendon; the posterior column corresponds to the popliteofibular ligament insertion site; and the medial column comprises the tibiofibular articular surface).
Group III (fibular neck or shaft fractures): Fractures distal to the head involving the fibular neck or proximal shaft region: III1: Oblique fracture oriented from superomedial to inferolateral direction. III2: Horizontal or extensively comminuted fractures. III3: Oblique fracture oriented from inferomedial to superolateral direction.
Tibial plateau fractures were concurrently classified using the established CT-based three-column classification system described by Wang et al. 9 (Figure 3).
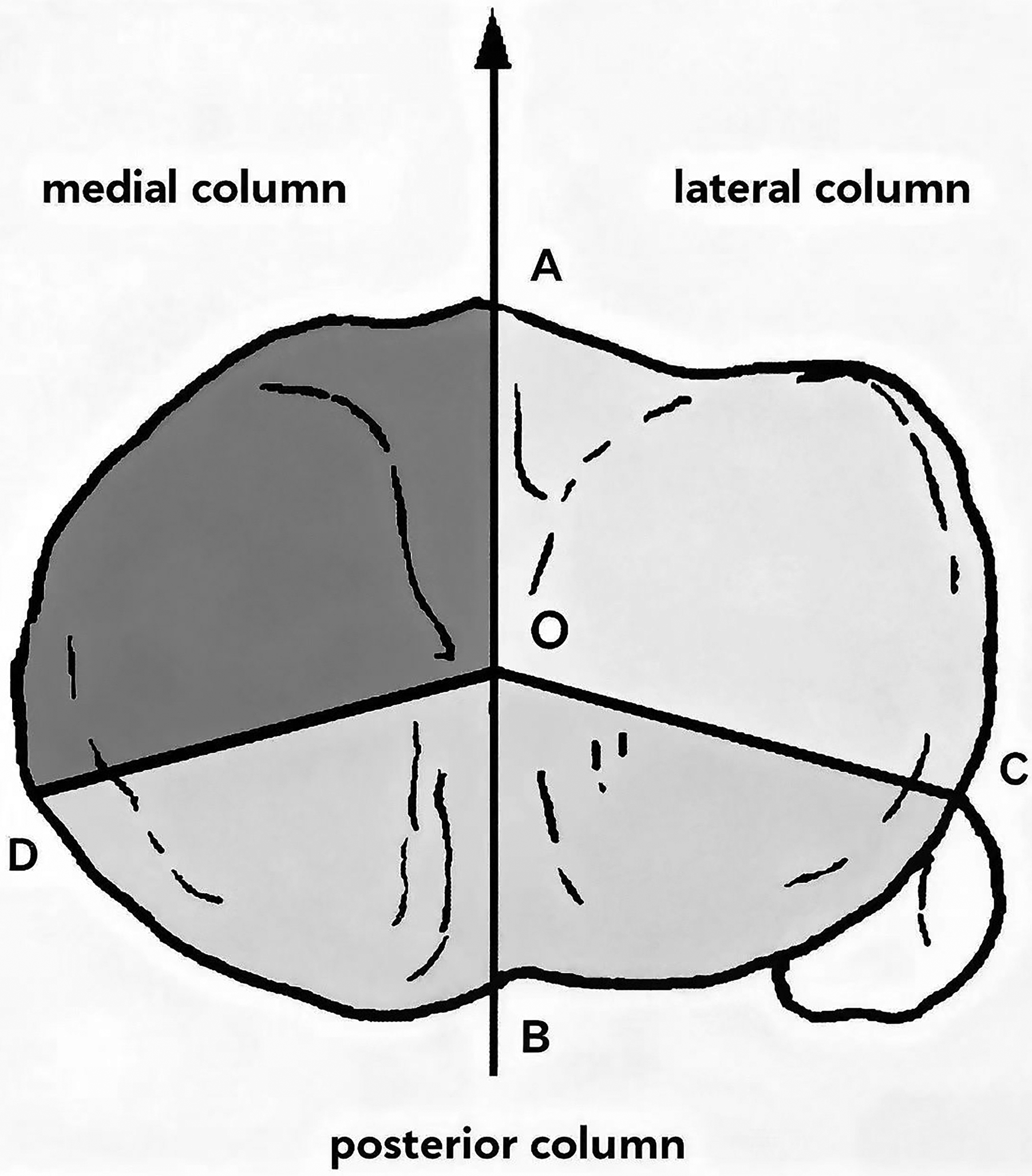
A ‘‘three-column’’ concept (Excerpt from Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma. 2010 Nov;24(11):683–92).
Reliability assessment and observers
To evaluate inter-observer reliability, two independent observers with differing expertise were recruited: an orthopedic trauma surgeon (Observer 1) with extensive clinical experience in fracture management, and a musculoskeletal radiologist (Observer 2) experienced in fracture imaging interpretation. Both observers were blinded to patient clinical outcomes and had no conflicts of interest.
Prior to evaluation, each observer was provided with detailed schematic illustrations and written instructions regarding the morphological classification system. In cases of disagreement, a consensus was reached through collaborative review and discussion. To quantify inter-observer agreement, Cohen's κ statistic was calculated for the classification of proximal fibular fracture morphologies (Groups I–III and subtypes). The overall κ value was 0.84 (95% CI 0.78–0.90), indicating excellent agreement between observers.
Injury mechanism hypothesis development
Based on fracture morphology and clinical biomechanical principles, we developed a mechanism classification protocol:
Each PFF subtype was mapped to the corresponding tibial plateau column involvement using Luo's three-column model.
9
Statistical analysis
Data were initially collected and organized using Excel spreadsheets (Microsoft Corp., Redmond, WA), followed by independent verification for accuracy, completeness, and logical consistency. Verified data were then imported into Statistical Product and Service Solutions (SPSS, Version 20.0; SPSS Inc., Chicago, IL) for further analysis.
Descriptive statistical methods were employed to summarize the distribution of fibular fracture morphologies. Logistic regression analyses were subsequently conducted to determine associations between specific proximal fibular fracture patterns and the tibial plateau fracture subtypes according to the three-column classification system.
Results
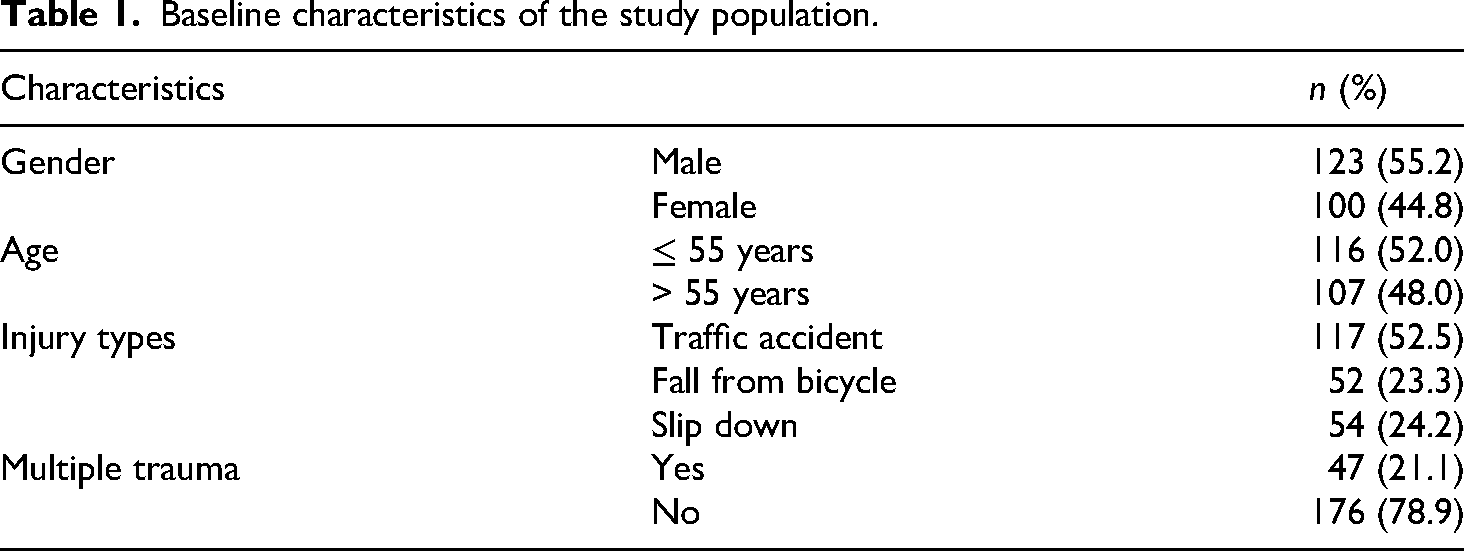
From January 2011 to January 2024, a total of 479 patient records were initially retrieved using the keyword “tibial plateau fracture.” Following further screening with additional keywords (“fibular fracture” or “fibular head fracture”), 285 records remained. After applying inclusion and exclusion criteria, 223 eligible cases (123 males, 100 females) were ultimately included in the analysis (Table 1).
Baseline characteristics of the study population.
Among these cases, proximal fibular fractures were categorized into group I (avulsion fractures, n = 63, 28.3%), group II (cleavage and comminution fractures, n = 121, 54.3%), and group III (neck or proximal shaft fractures, n = 39, 17.4%). Within group II, the most frequent subtype was II3p (three-part comminution), occurring in 61 patients (50.4%). Subtypes II1p(P), II2p(L + P), and III3 were not identified within our study cohort (Tables 2 and 3 and Figure 4).
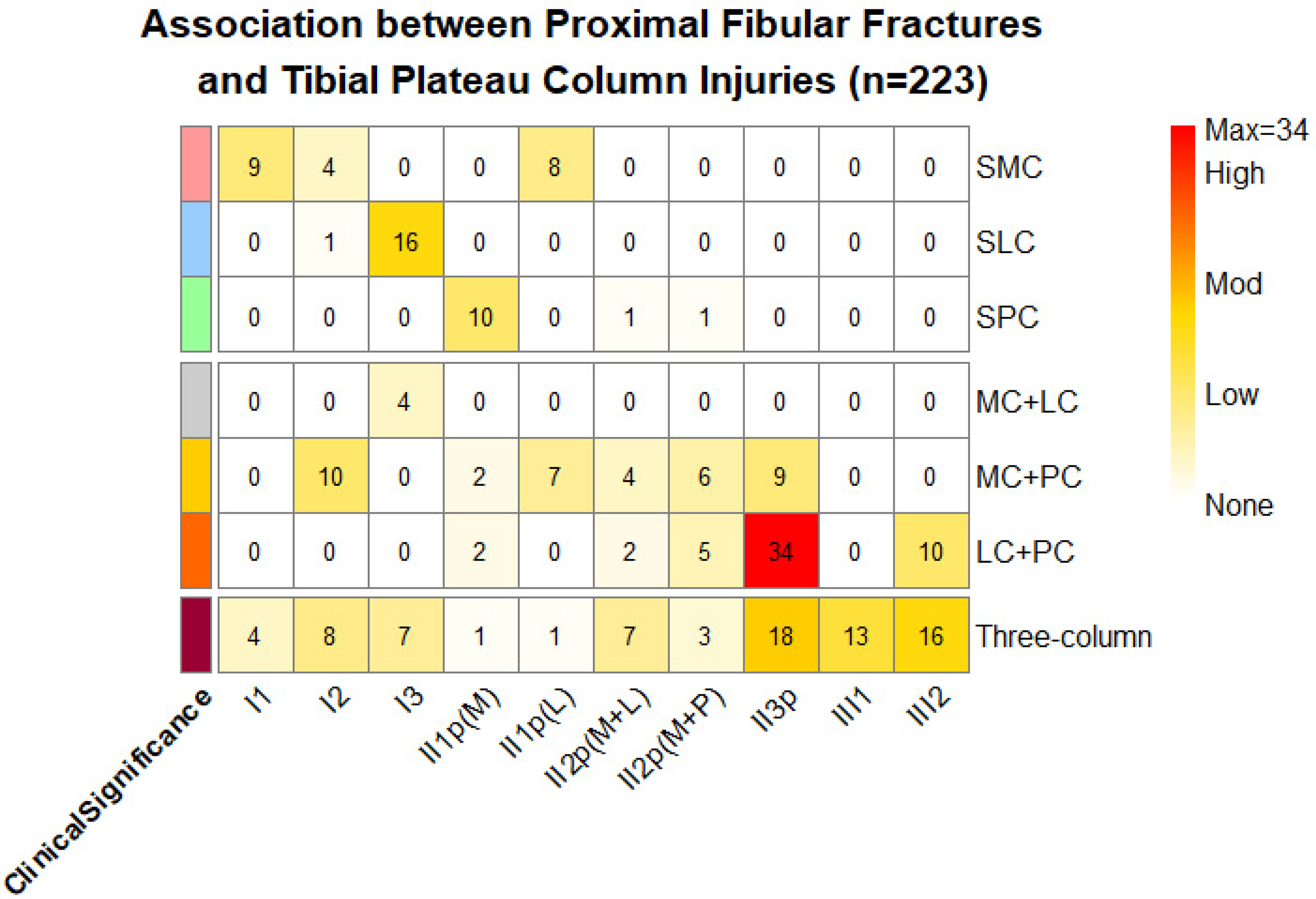
Heatmap of association between proximal fibular fractures and tibial plateau column injuries (n = 223).
Distribution of 223 proximal fibula fractures according to the three groups, 13 hypothetical conditions.

Distribution of proximal fibula fractures according to hypothetical conditions in the CT-based three-column tibial plateau fracture classification [deleted II1p(P), II2p(L + P), and III3 subgroups].

CT: computed tomography; LC + PC: lateral columns + posterior columns; MC + LC: medial columns + lateral columns; MC + PC: medial columns + posterior columns; SLC: single lateral column; SMC: single medial column; SPC: single posterior column.
Morphological associations between proximal fibular fractures and tibial plateau fractures, as classified by the CT-based three-column classification, revealed distinct patterns. Specifically, in this study, group II proximal fibular fractures did not occur in isolated posterior column fractures or combined lateral and posterior column fractures. Group III fibular fractures were exclusively associated with combined tibial plateau lateral-posterior column or three-column fractures.
Sensitivity analysis of exclusion criteria: To evaluate the impact of excluding small fibular fractures (<2 mm displacement), we performed a sensitivity analysis by re-analyzing the full dataset, including the 37 initially excluded cases. Fracture morphologies were re-classified using identical 3D-CT criteria. The re-analysis revealed a nearly identical distribution: Group I (27.7% vs. 28.3%), Group II (54.6% vs. 54.3%), and Group III (17.7% vs. 17.4%). Logistic regression results remained consistent with the primary analysis, with no significant changes in odds ratios (ΔOR < 10%). These robust outcomes suggest that the exclusion of minimally displaced fractures did not materially alter the study's primary morphological associations (Table 4).
Sensitivity analysis comparing morphological distribution with and without exclusion of fractures < 2 mm.

Logistic regression analysis utilized the “three-column” tibial fracture type as the reference category due to its comprehensive fracture spectrum. Results indicated a significantly higher likelihood of group I fibular fractures in isolated tibial plateau medial column fractures. Conversely, group II fibular fractures occurred most frequently with combined tibial plateau lateral-posterior or medial-posterior column fractures. Notably, group III fibular fractures were most commonly associated with tibial plateau three-column fractures in Table 3. The detailed results of the logistic regression analysis are summarized in Table 5.
The summary results of the significant dummy variables for the different fibular fracture conditions and 3D-CT tibia plateau classifications (“Enter” method).
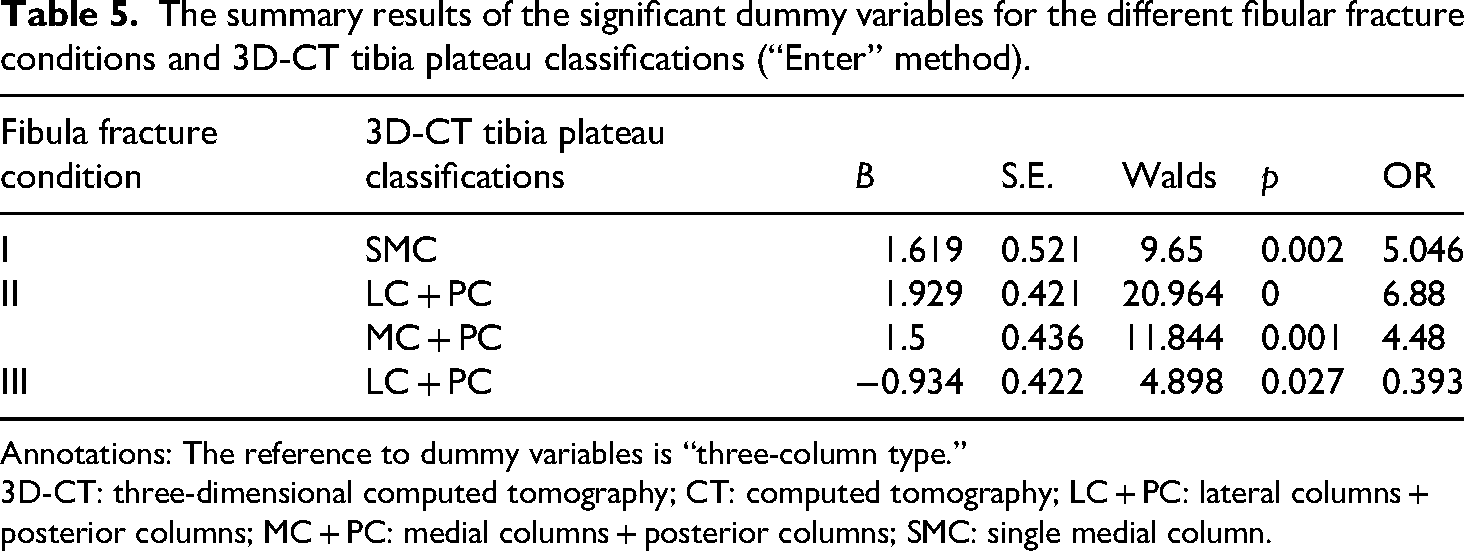
Annotations: The reference to dummy variables is “three-column type.”
3D-CT: three-dimensional computed tomography; CT: computed tomography; LC + PC: lateral columns + posterior columns; MC + PC: medial columns + posterior columns; SMC: single medial column.
Injury mechanisms by periprosthetic femoral fracture (PFF) subtype and tibial plateau column involvement.

Mechanism-fracture correlations revealed (Table 6)
:
Discussion
Recent biomechanical and clinical studies have emphasized the significance of the proximal fibula in maintaining the structural integrity and functional stability of the PLC of the knee. 9 The proximal tibiofibular joint, a critical anatomical structure, provides lateral stability to the tibial plateau and contributes to knee joint stability; however, its involvement often complicates the management of tibial plateau fractures. 9 Although proximal fibular fractures have been classified as AO subgroup 4F1, this classification predominantly addresses fracture localization and does not sufficiently reflect the detailed morphology or mechanisms underlying these fractures. 11
Takahashi et al., 6 through anatomical dissections and computer-assisted modeling, described the proximal fibula's characteristic pyramidal anatomy, which serves as a vital insertion site for the FCL, PFL, and biceps femoris tendon. The anatomical landmarks—such as the lateral prominence, fibular styloid process, anterior and medial cortical points—are consistently identifiable on 3D-CT imaging, facilitating precise fracture characterization. In our study cohort, comminution patterns of proximal fibular fractures displayed notable variability, likely influenced by tendon and ligamentous insertions at the medial, lateral, and posterior regions.
In our previous study, proximal fibular fractures were classified based solely on fracture line positions observed on plain radiographs. 1 However, 3D-CT imaging in the present study revealed a more complex fracture morphology. Therefore, our expanded hypothetical classification integrates both anatomical features and radiographic fracture characteristics to better delineate injury mechanisms.
Clinically, fractures classified within group I closely resemble the “arcuate fractures” described previously. 8 Such avulsion injuries typically result from varus stress mechanisms rather than direct axial loading from the tibial segment. Surgeons generally advocate operative fixation or ligament reconstruction in cases involving group I2 fractures (classic arcuate fractures) or certain comminuted group II fractures, given their direct impact on PLC stability.12,13 The presence of group I fractures in isolated medial column fractures, as well as complex multi-column fractures, suggests diverse trauma mechanisms, including compound injuries and multidirectional force applications.
In contrast, no cases categorized as subtype II1p(P)or II2p(L + P) were identified. Nor were group II fibular fractures observed in the tibial plateau, single lateral, or combined medial-lateral column fractures. Our analysis suggests that comminuted proximal fibular fractures (II2p and II3p) typically result from high-energy forces initiating at the proximal tibiofibular articulation and propagating posteriorly and laterally, ultimately breaching the cortical integrity and leading to extensive concomitant tibial plateau damage.
Although subtype III3 fibular fractures were not observed in this study, this fracture pattern is typically associated with lower limb rotational injuries such as Maisonneuve fractures involving the distal tibia or ankle injuries.12,13 The proximal fibula's stabilizing role, mediated by interosseous and ligamentous structures, primarily resists rotational rather than direct axial forces; thus, tibial plateau fractures associated with proximal fibular fractures typically occur due to combined varus or valgus loading with rotational components, rather than simple axial compression.14,15 Our study bridges fracture morphology to injury mechanisms for the first time in PFF-TPF complexes. Three key biomechanical relationships emerged: “Varus Stress -Group I,” “Axial Loading -Group II3p,” and “Rotational Force- Group III1,2.” The recent Schatzker-Kfuri classification (2022) offers enhanced mechanistic insights by correlating fracture morphology with injury vectors. 16 This system's emphasis on the “split wedge fragment” and articular rim continuity as biomechanical keystones aligns with our findings.
Based on our morphological study of proximal fibular fractures, we propose the following clinical management recommendations: For Type I avulsion fractures, which indicate potential posterolateral corner compromise, particular intraoperative attention should be directed toward medial plateau stability of the tibia. For Type II 3p comminuted fractures, meticulous restoration of axial alignment in the tibial plateau is essential. For Type III oblique fractures, assessment for proximal tibiofibular joint dissociation must be performed. This study establishes fracture-line morphology as an indicator of knee injury mechanisms—a strategy that adapts to diverse surgical settings while preventing critical complications such as ligamentous instability or dynamic malalignment.
Several limitations warrant consideration when interpreting these results. Firstly, this study was retrospective and conducted at a single trauma center, which may limit generalizability. Additionally, clinical follow-up data were limited, potentially restricting insights into functional outcomes. Secondly, the exclusion of 37 fractures with displacement <2 mm may theoretically overlook subtle PLC injury markers detectable only on MRI. However, our sensitivity analysis (reported in Results) demonstrated that including these fractures did not alter the morphological distribution patterns or key statistical associations. Nevertheless, clinically suspected PLC injuries warrant ancillary investigations (e.g. MRI or stress radiographs), particularly in cases with documented lateral instability. Moreover, patients with concurrent femoral or distal tibial injuries were excluded, possibly underestimating the complexity of proximal fibular fracture patterns. Prospective, multicenter studies with larger patient cohorts and comprehensive follow-up data are necessary to further clarify the associations and biomechanical mechanisms underlying proximal fibular fractures in the context of complex knee injuries. The detailed results of the logistic regression analysis are summarized in Table 4.
Conclusion
This study systematically delineated the morphological patterns of proximal fibular fractures associated with tibial plateau fractures, revealing significant fracture heterogeneity that indicates diverse trauma mechanisms and provides valuable insights for clinical decision-making. Our findings potentially elucidate certain morphological correlations between proximal fibular fractures and distinct tibial plateau fracture patterns. Further clinical investigations and biomechanical analyses are warranted to clarify the injury mechanisms and optimize therapeutic strategies for these complex fracture combinations.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251397508 - Supplemental material for Morphological study of proximal fibular fractures with concomitant tibial plateau fractures: An investigation of 223 cases
Supplemental material, sj-docx-1-sci-10.1177_00368504251397508 for Morphological study of proximal fibular fractures with concomitant tibial plateau fractures: An investigation of 223 cases by Yue Liu, Jinxia Yang, Renda Liu, Yunli He, Jiaqi Wang, Zhi Wang and Zisheng Ai in Science Progress
Footnotes
Acknowledgements
We would like to express our sincere gratitude for the support from Shanghai Pudong New Area Gongli Hospital and the relevant collaborative institutions.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Discipline Construction Project of Characteristic Clinic of Pudong New Area Health Commission (PWYts2018-03), Research Grant for Health Science and Technology of Pudong Health and Family Planning Commission of Shanghai (Grant No. PW2024A-13), Top-notch Talent Training Program of Pudong Gongli Hospital (No. GLRb2020-04), 2024 Gusau Health Talent Research Program (GSWS2023049), and the 2022 Suzhou Science and Technology and Development Project Healthcare Science and Technology Innovation Project (SKY2022168).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.