
Abstract
Objective
To evaluate the influence of age, sex, and the need for intensive care unit admission on the clinical outcomes of patients with community-acquired pneumonia (CAP), considering the impact of comorbidities such as cardiovascular diseases, chronic kidney disease, and oncological conditions on the risk of complications and mortality.
Methodology
A multicenter retrospective cohort study was conducted in patients with CAP admitted to two tertiary-level institutions in Colombia between January 2010 and December 2020. A comorbidity map (comorbidome) was developed to reflect the prevalence of these conditions according to intensive care unit (ICU) stay, sex, and age.
Results
In a cohort of 3370 patients, the most frequent comorbidities were arterial hypertension (50.1%), anemia (31.8%), and chronic pulmonary disease (27.8%). Functional dependency showed the strongest association with mortality (OR 7.17; 95% CI 5.6–9.17), with significant differences in distribution and strength of association according to age, sex, and need for ICU admission.
Conclusion
This study demonstrated the high prevalence of comorbidities in patients with CAP in Colombia, highlighting arterial hypertension, anemia, and chronic pulmonary disease as the most common. The distribution of these comorbidities varied according to age and sex, although a very similar clinical profile was observed regarding the need for ICU admission.
Introduction
Community-acquired pneumonia (CAP) is one of the leading causes of morbidity and mortality worldwide, particularly in individuals with pre-existing conditions. The mortality rate is estimated to vary between 6.1% and 13%.1,2 In Europe, recent studies report an incidence of 14 cases per 1000 inhabitants, of which ∼50% require hospitalization, with an annual mortality of 0.7 per 1000 patients. 3 Additionally, it is calculated that 1.4 million people seek emergency services due to this pathology, resulting in 740,000 hospitalizations and ∼41,000 in-hospital deaths each year. 4 Thus, the presence of comorbidities plays a crucial role in the clinical evolution of CAP, as it increases the risk of complications and significantly contributes to mortality, reaching up to 22.9% at 30 days after diagnosis. 5
In a cohort study, Hespanhol and Bárbara 6 identified that high mortality from CAP is associated with the presence of comorbidities such as functional and mental deterioration, neoplastic diseases, chronic kidney disease, ischemic heart disease, and cerebrovascular disease, considering them independent risk factors for hospital mortality. Similarly, Corrales-Medina et al. 7 and their team highlight that a high percentage of patients with CAP have chronic conditions, with cardiovascular diseases being the most prevalent. These conditions increase the risk of serious complications, such as myocardial infarction, acute heart failure, and atrial fibrillation, which are associated with a significant increase in 30-day mortality.7,8
Independent studies conducted by Holter et al. 9 and Blanc et al. 10 have shown that elderly patients present a higher burden of comorbidities, including cardiovascular diseases, chronic obstructive pulmonary disease (COPD), and oncological pathologies, factors that significantly influence the prognosis of CAP. Patients admitted to the intensive care unit (ICU) with CAP often have comorbidities that affect both their clinical evolution and therapeutic decisions, unlike those with less severity. 11 On the other hand, there is mixed evidence regarding the impact of sex on the evolution of CAP, since, although the incidence is higher in men, mortality varies according to factors such as immune response and the presence of comorbidities. 12 These findings reinforce the importance of an approach that seeks the concomitant management with greater rigor of comorbidities that promote a more severe establishment of the disease, where early identification and management optimize therapeutic strategies and improve clinical outcomes, underlining the need for studies that deepen the interaction between comorbidities and this pathology.
Given the high morbidity and mortality of CAP and the wide variety of risk factors and comorbidities that can influence its evolution, and considering the gap in knowledge regarding the real impact of comorbidities on this pathology, with the aim of allowing a natural course of the disease that tends to have a lower probability of mortality outcome, we propose the creation of a comorbidome by subgroups. To address this gap, we conducted a retrospective cohort study to explore the prevalence and impact of comorbidities on CAP outcomes in Colombian patients. The objective is to identify the associations between CAP and comorbidities that may influence the outcome of 30-day mortality.
Methodology
A multicenter retrospective cohort study was conducted on subjects with CAP who were admitted to two tertiary care institutions in Colombia between January 2010 and December 2020. The main objective of this study was to describe the comorbidities most frequently associated with CAP and represent them in a comorbidity map (comorbidome) that reflects their prevalence according to ICU stay, sex, and age. The reporting of this study conforms to STROBE guidelines. 13
Eligibility criteria
Included subjects were adults over 18 years of age diagnosed with pneumonia according to the American Thoracic Society/Infectious Diseases Society of America (ATS/IDSA) 14 criteria, with the presence of acute respiratory symptoms, associated with radiological findings compatible with pneumonia, and requiring antibiotic management. Patients who did not have a clinical history, incomplete PSI score variables, or a diagnosis of nosocomial pneumonia during hospitalization were excluded.
Variables
Information was obtained on demographic characteristics, vital signs, physical examination, and clinical outcomes. Comorbidities: systemic arterial hypertension, smoking, chronic heart failure, acute myocardial infarction, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, ulcerative disease, liver disease, diabetes mellitus, tumor, chronic kidney disease, dementia, hemiplegia, asthma, trauma, dependency, hematolymphoid neoplasia, connective tissue disease, immunosuppression, hypoalbuminemia, and anemia.
The evaluated groups were patients with and without ICU stay, older and younger than 65 years, men and women. The outcome variable is 30-day mortality. In order to reduce transcription biases, the data were verified by at least two members of the research group directly from the electronic medical record, and the personnel collecting the information had training for this purpose.
Sample size
To estimate the necessary sample size for this study, the formula by Machin et al. was used, and data from Hespanhol where a risk in exposed patients with chronic kidney disease of 28% and an odds ratio (OR) of 1.20 were found, for a confidence level of 95% and a statistical power of 80%, a minimum of 3069 subjects is required.6,15,16
Statistical analysis
Data were extracted directly from electronic medical records, which were reviewed in their entirety and extracted to the Research Electronic Data Capture (REDCap) electronic data capture software. They were then exported to Excel and analyzed with Python for the final analysis. Qualitative variables were summarized in count and percentage, quantitative variables in mean and standard deviation if their distribution was normal, median and interquartile range if their distribution was non-normal. Normality tests were performed using Kolmogorov-Smirnov. In the analysis of two independent samples, a chi-square test was used.
The prevalence of each comorbidity was calculated as a percentage, and an analysis of each one was performed in relation to the general population, patients who required ICU and those who did not, older and younger than 65 years, and male and female subjects. Univariate logistic regression was performed to evaluate the OR for each variable in subjects who were alive and patients who were dead at 30 days. A subsequent multivariate analysis was conducted on general characteristics, with their respective 95% confidence intervals, and a p < 0.05 was considered statistically significant.
To visualize the associated comorbidities, a comorbidome was created. This graph represents all comorbidities with associations, where the size of each bubble is proportional to the prevalence of the disease and the proximity to the center reflects the strength of the association. This strength was numerically quantified as the inverse of the OR (1/OR). 17 Statistical analysis was performed in Microsoft Excel, while data preparation and graphical visualizations were carried out using Python 3.12.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki of 1975 and its most recent revision in 2024. It is considered research without risk. It is considered research without risk, according to Law 8430 of 1993. 18 All privacy policies of the study subjects were respected.
Results
From a total population of 7454 patients, inclusion and exclusion criteria were applied, resulting in an admission population of 3370 patients, with 3065 (90.9%) being alive and 305 (9.1%) deceased (Figure 1).
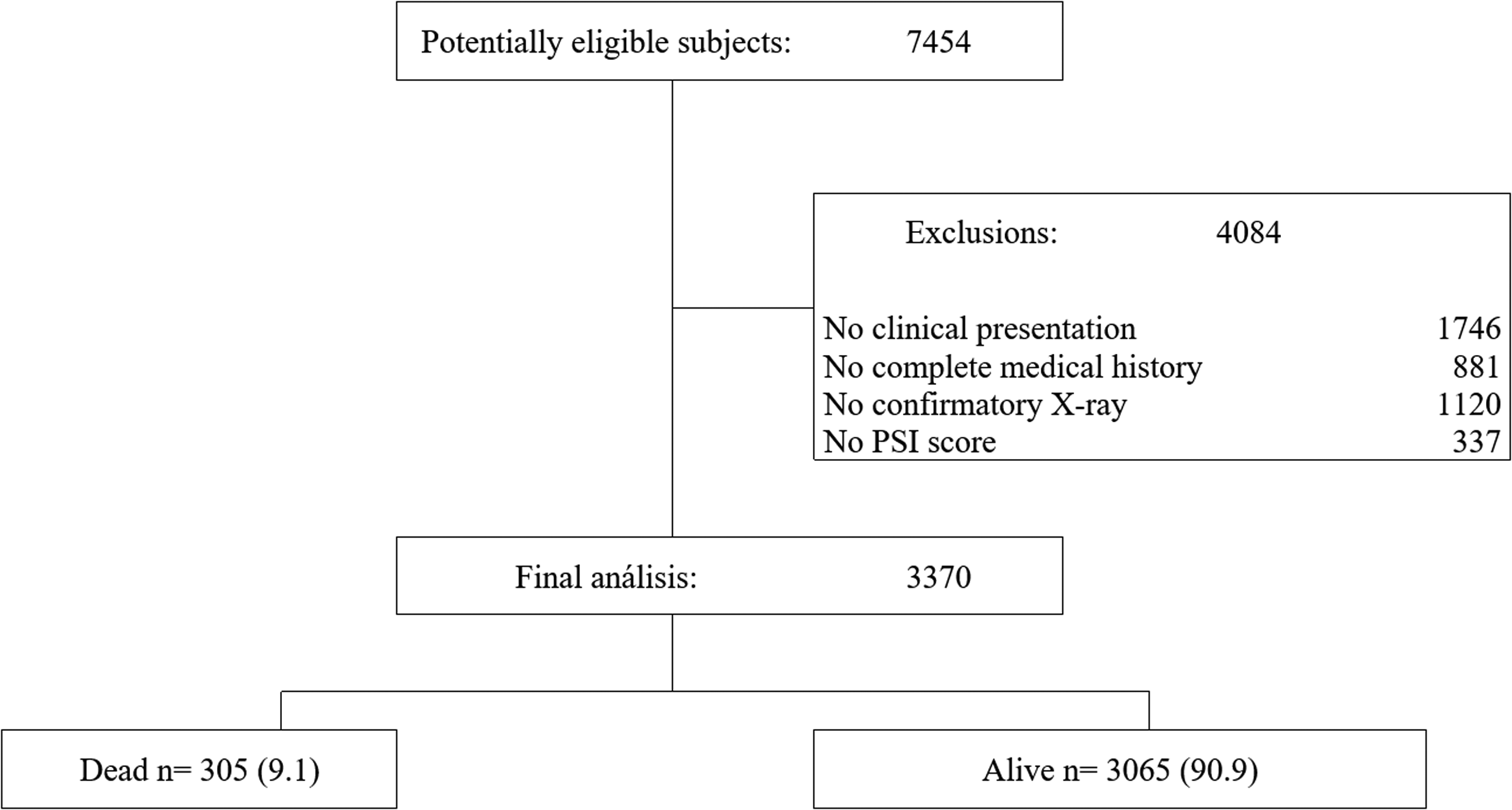
Flowchart of patient enrollment.
The average age of the population was 65.5 years (± 21.43). The deceased patients had a mean of 78.5 years (± 15.18), while the survivors had a mean of 64.2 years (± 21.54) (p < 0.001). 59.7% of the total population corresponded to male patients, with no statistically significant differences between the groups (p = 0.789). Patients who died had a significantly lower SpO₂/FiO₂ ratio upon admission (272.3 vs. 343.5, p < 0.001). Mortality was associated with higher rates of septic shock (35.4% vs. 7.5%), vasopressor use (22% vs. 7.2%), ICU admission (23.3% vs. 11.6%), invasive mechanical ventilation (22.6% vs. 7.6%), non-invasive ventilation (10.2% vs. 3.9%), and hospitalization (95.7% vs. 89.3%) (all p < 0.001) (Table 1).
General characteristics of the population.

m: average; ±: standard deviation; n: number; bpm: beats per minute; MAP: mean arterial pressure; bepm: breaths per minute; FiO2: inspired fraction of oxygen; SpO2/FiO2: ratio of oxygen saturation to the fraction of inspired oxygen.
Regarding vital signs, deceased patients presented a lower mean arterial pressure compared to survivors (84 ± 17 vs. 89 ± 14 mmHg, p < 0.001), a higher respiratory rate (23 ± 6 vs. 21 ± 5 breaths per minute, p < 0.001) and more compromised oxygen saturation (87 ± 9% vs. 89 ± 7%, p < 0.001). In relation to laboratory parameters, the deceased group showed a lower hematocrit (37 ± 7% vs. 40 ± 7%, p < 0.001), lower albumin levels (2.7 ± 0.44 g/dL vs. 2.9 ± 1.13 g/dL, p < 0.001) and higher BUN concentrations (35 ± 24 mg/dL vs. 24 ± 17 mg/dL, p < 0.001) (Table 1).
General population
In the general population (n = 3370), the most frequent antecedents were hypertension (50.1%), anemia (31.8%), and chronic pulmonary disease (27.8%). Among the deceased (n = 305), the most prevalent conditions were hypertension (66.2%), dependency (55.7%), and anemia (52.8%). Differences were observed in the frequency of multiple conditions between the deceased and survivors, with higher ORs for dementia (OR 4.71; 95% CI 3.58–6.2), dependency (OR 7.17; 95% CI 5.6–9.17), and hematolymphoid neoplasms (OR 3.10; 95% CI 1.61–5.97). In the multivariate analysis, dependency with an OR of 4.41 (95% CI: 3.23–6.03, p < 0.001), hematolymphoid neoplasms (OR 2.54; 95% CI: 1.18–5.46; p = 0.017), and dementia (OR 1.72; 95% CI: 1.23–2.40; p = 0.002) showed significant associations, with greater magnitude of effect (Table 2 and Figure 2).
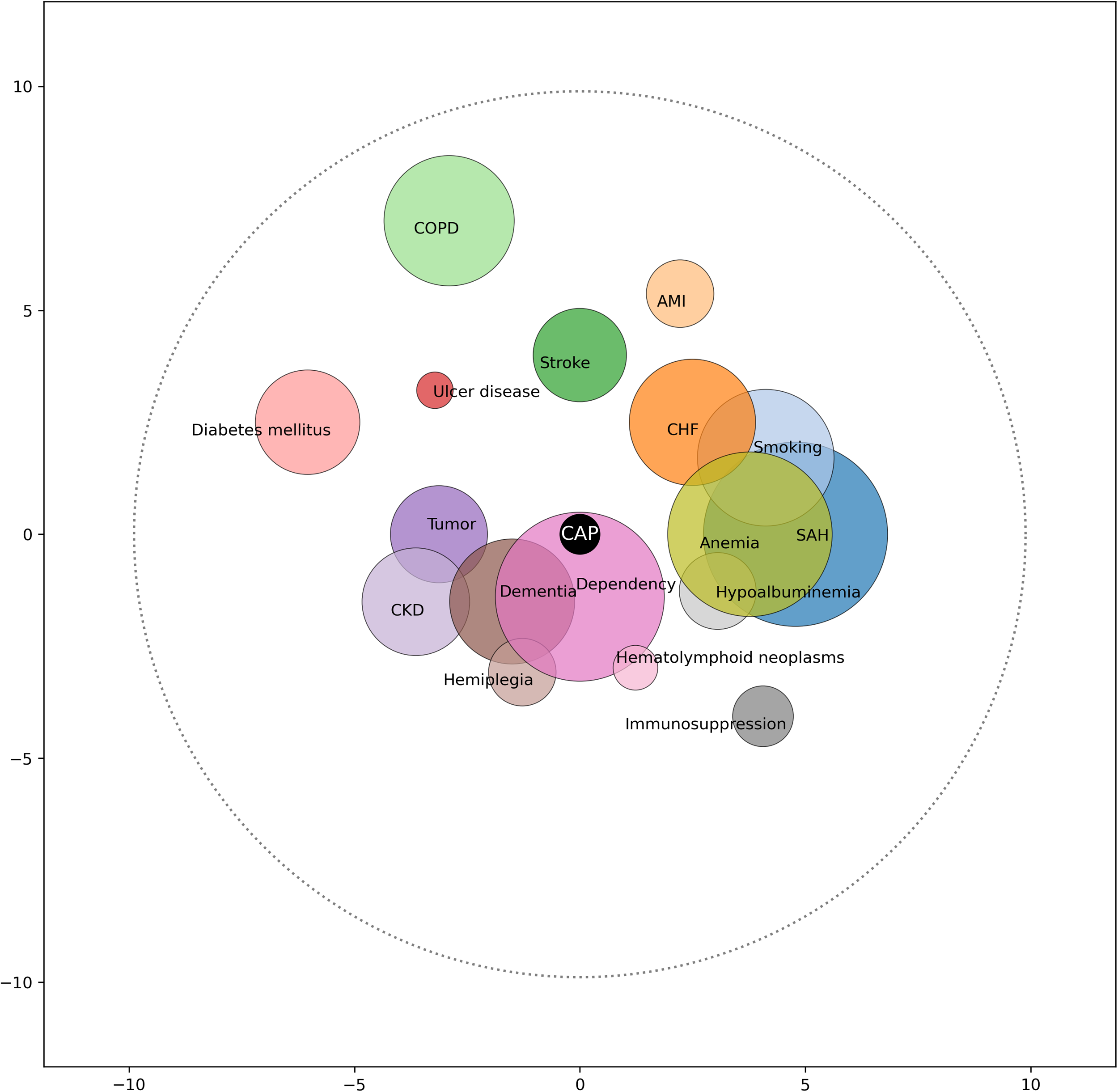
Comorbidome community-acquired pneumonia.
Background of the general population.

SAH: systemic arterial hypertension; CHF: chronic heart failure; AMI: acute myocardial infarction; PVD: peripheral vascular disease; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease.
Population over 65 years
In the population over 65 years with CAP (n = 2037), the most prevalent antecedents were hypertension (69.6%), chronic pulmonary disease (40.7%), and anemia (36.5%). In the group of deceased patients (n = 261), the three most prevalent conditions were dependency (60.5%), hypertension (73.6%), and anemia (54.8%). On the other hand, the factors with the strongest association with mortality were dependency (OR 5.87; 95% CI: 4.46–7.71), dementia (OR 3.41; 95% CI: 2.55–4.55), and hypoalbuminemia (OR 2.84; 95% CI: 1.86–4.35) (Table 3 and Figure 3).

Comorbidome community-acquired pneumonia in patients over and under 65 years of age.
Background of the population by age.
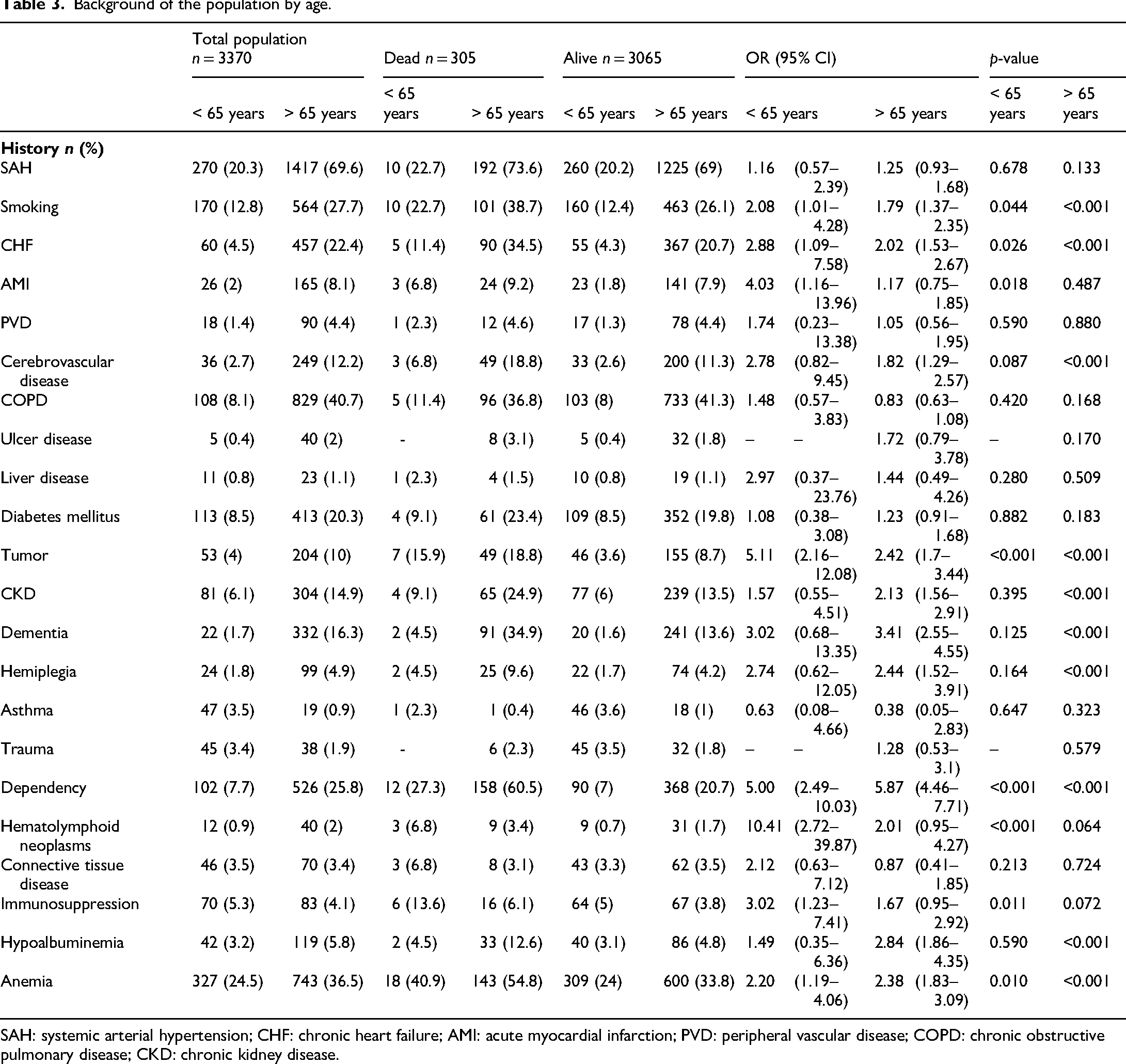
SAH: systemic arterial hypertension; CHF: chronic heart failure; AMI: acute myocardial infarction; PVD: peripheral vascular disease; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease.
Population under 65 years
In the population under 65 years with CAP (n = 1333), the most prevalent antecedents were anemia (24.5%), hypertension (20.3%), and smoking (12.8%). Among deceased patients, the most frequent were anemia (40.9%), dependency (27.3%), and hypertension (22.7%). Regarding the strength of association with mortality, the antecedents with the greatest impact were hematolymphoid neoplasia (OR 10.41; 95% CI: 2.72–39.87), solid tumor (OR 5.11; 95% CI: 2.16–12.08), and dependency (OR 5.00; 95% CI: 2.49–10.03) (Table 3 and Figure 3).
Male population
In the male population (n = 2013), the most prevalent antecedents were hypertension (45.5%), anemia (35.4%), and smoking (27.5%). Among deceased patients, the most frequent were anemia (59.4%), dependency (52.2%), and hypertension (57.2%). Regarding the association with mortality, the factors with the strongest association were dependency (OR 6.55; 95% CI: 4.78–8.97), dementia (OR 4.03; 95% CI: 2.77–5.84), and hematolymphoid neoplasia (OR 3.66; 95% CI: 1.81–7.4) (Table 4 and Figure 4).

Comorbidome community-acquired pneumonia related to sex.
Background of the population by sex.

SAH: systemic arterial hypertension; CHF: chronic heart failure; AMI: acute myocardial infarction; PVD: peripheral vascular disease; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease.
Female population
In the female population (n = 1357), the most prevalent antecedents were hypertension (56.8%), dependency (20%), and chronic pulmonary disease (31.4%). Among deceased patients, the three most frequent conditions were hypertension (79.2%), dependency (60.8%), and anemia (43.2%). Regarding the association with mortality, the factors with the strongest association were dementia (OR 5.74; 95% CI: 3.81–8.63), dependency (OR 5.60; 95% CI: 3.99–7.91), and hemiplegia (OR 3.96; 95% CI: 2.08–7.54) (Table 4 and Figure 4).
ICU population
In the population admitted to the ICU (n = 428), the most prevalent antecedents were hypertension (50.5%), anemia (41.4%), and chronic obstructive pulmonary disease (31.5%). Among deceased patients, the three most frequent conditions were hypertension (67.6%), anemia (47.9%), and smoking (43.7%). Regarding the strength of association with mortality, the factors with the greatest impact were hematolymphoid neoplasia (OR 8.94; 95% CI: 2.09–38.31), immunosuppression (OR 3.09; 95% CI: 1.31–7.31), and chronic heart failure (OR 3.01; 95% CI: 1.68–5.39) (Table 5 and Figure 5).

Comorbidome community-acquired pneumonia related to intensive care unit admission.
Background of patients admitted and not admitted to the ICU.
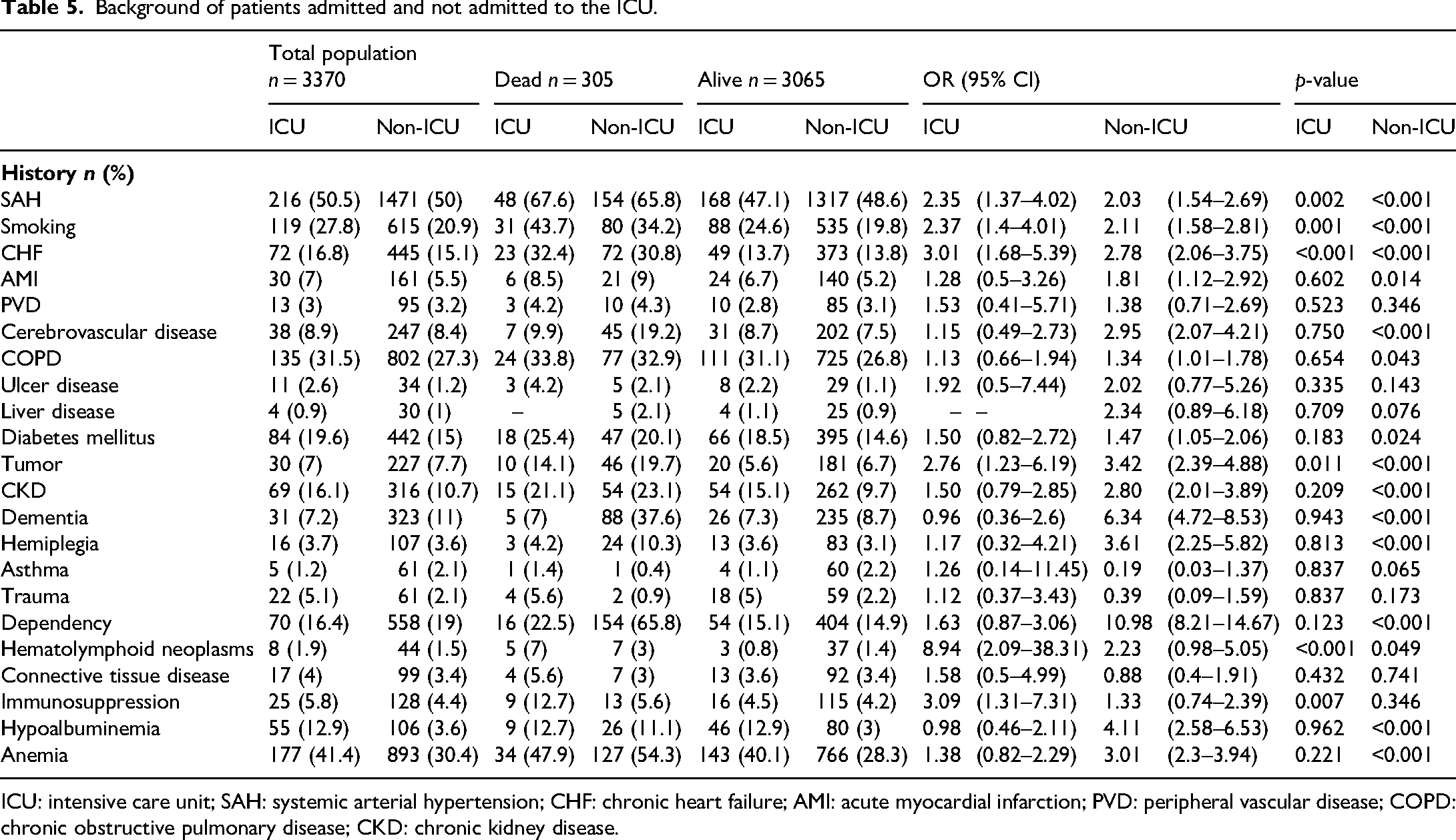
ICU: intensive care unit; SAH: systemic arterial hypertension; CHF: chronic heart failure; AMI: acute myocardial infarction; PVD: peripheral vascular disease; COPD: chronic obstructive pulmonary disease; CKD: chronic kidney disease.
Non-ICU population
In the population that did not require ICU admission (n = 2942), the most prevalent antecedents were hypertension (50%), chronic pulmonary disease (27.3%), and anemia (30.4%). Among deceased patients, the three most frequent conditions were hypertension (65.8%), dependency (65.8%), and anemia (54.3%). Regarding the strength of association with mortality, the factors with the greatest impact were dependency (OR 10.98; 95% CI: 8.21–14.67), dementia (OR 6.34; 95% CI: 4.72–8.53), and tumor (OR 3.42; 95% CI: 2.39–4.88) (Table 5 and Figure 5).
Discussion
This study examines and analyzes the comorbidity profile of CAP in Colombia, graphically representing the relationships between concurrent diseases and their prevalence according to age group, sex, and need for ICU admission. In the general population, hypertension, chronic pulmonary disease, and anemia emerged as the most frequent comorbidities. The analysis revealed that anemia was the predominant condition among patients under 65 years of age. When examining differences by sex, ICU admission status, and those over 65 years, systemic arterial hypertension was consistently prevalent across groups. However, notable variations in disease prevalence were observed according to age and sex factors. Interestingly, patients requiring intensive care demonstrated a clinical profile similar to those who did not require ICU admission, suggesting that comorbidity patterns may not be strong predictors of ICU necessity in this population.
Hypertension emerged as the most frequent comorbidity in our study (50.1%), closely aligning with the 52% previously reported by Ibáñez-Prada et al. 19 in Colombian patients hospitalized for CAP. This consistency highlights a stable epidemiological profile in Colombia, likely attributable to dietary habits, sedentary lifestyles, and shared genetic predisposition. Anemia ranked as the second most prevalent comorbidity (31.8%), affecting both young and older adults, echoing findings by Doshi et al., 20 who associated this condition with increased severity and clinical complications, potentially linked to chronic inflammatory processes and adverse socioeconomic conditions. Chronic pulmonary disease was the third most common condition (27.8%), contrasting with Cavallazzi and Ramirez's 21 U.S. study that identified this pathology as the primary comorbidity (32%) in CAP patients. This discrepancy may reflect regional variations in environmental exposure and respiratory health patterns. The co-occurrence of these three comorbidities suggests a clinical profile with elevated cardiovascular risk and diminished ventilatory capacity, potentially contributing to greater hypoxemia and hemodynamic consequences.
When examining the population over 65 years, COPD showed higher prevalence in CAP subjects, while anemia was more frequent in younger individuals—a finding that diverges from international studies reporting lower anemia prevalence. 22 This difference likely stems from nutritional and physiological factors specific to our population. Colombia has documented a high prevalence of anemia (21.2%) among women of reproductive age, primarily attributed to iron deficiencies related to menstruation and insufficient micronutrient intake. 23 Consequently, this condition may manifest more frequently in younger cohorts from Latin American countries where social and nutritional inequalities are more pronounced. Collectively, these findings suggest that while younger patients typically present fewer comorbidities than older adults, certain conditions like anemia warrant particular consideration in patients with respiratory infections.
Women demonstrated a higher burden of chronic non-communicable conditions in our analysis. This pattern correlates with frequent exposure to environmental factors, such as biomass fuel use for cooking in rural and semi-urban areas, which is associated with deteriorating lung function and increased vulnerability to respiratory infections like CAP. Additionally, we observed a high proportion of dependency among female patients, potentially explained by the “female morbidity paradox”—despite greater longevity, women experience increased disability and functional dependence, heightening their clinical complexity and vulnerability. While this aspect hasn't been directly addressed in previous CAP studies, it manifests in conditions such as dementia, where women show significantly higher prevalence. 23
A high prevalence of smoking was observed among men with CAP, potentially linked to the higher anemia rates identified in this group. Baskaran's meta-analysis demonstrated that smokers face twice the risk of developing CAP compared to non-smokers, with a clear dose-response relationship in heavy tobacco users. 24 Additionally, smoking has been associated with increased risk of iron deficiency anemia, as reported by Vivek et al., 25 who found that active smokers—especially long-term users—have a higher probability of developing this condition. This interaction between smoking, anemia, and CAP presentation suggests a complex pathophysiological vulnerability in male smokers, mediated by immunological alterations, chronic inflammation, and compromised tissue oxygenation.
Regarding pathologies in ICU versus non-ICU patients, we observed remarkably similar clinical profiles, suggesting that diseases may require hospitalization or intensive care depending on their clinical stages and severity rather than the specific comorbidity types. In our cohort, lower heart rate, mean arterial pressure, and body temperature in non-survivors may reflect more advanced stages of disease severity. These alterations can be indicative of systemic hypoperfusion, impaired thermoregulation, and a blunted physiological response to infection, all of which are associated with poor prognosis. However, these are not the only factors influencing care decisions, as conditions such as dementia, functional dependence, and multiple comorbidities have been described as determinants, often leading to less invasive interventions more focused on palliative care.26–28 This balanced distribution between critical and non-critical patients with similar comorbidity profiles aligns with findings from previous studies. 29
In Colombian patients with CAP, the high prevalence of hypertension, anemia, and chronic lung disease is consistent with international reports, where multimorbidity and functional dependence are strongly associated with increased mortality. Although regional variations exist in the classification and frequency of comorbidities, the overall risk pattern is widely supported by the literature.
Although our findings correspond with existing literature, this study has several limitations. Its retrospective design based on clinical records may introduce information biases in data collection, including coding errors, omission of relevant diagnoses, or variability in medical record quality—though this risk was mitigated through proper training of the research team. It is recommended that researchers consider conducting prospective studies or adding control groups in future work to mitigate the impact of these biases. Additionally, we were unable to classify comorbidity severity, limiting the precision of our comorbidome analysis. Important variables such as tumor stage, GOLD classification in COPD, subtypes of solid tumors or hematolymphoid neoplasms, and levels of functional dependence and treatment methods—all potentially significant prognostic factors—were not included in our analysis.
Conclusions
This study revealed the high prevalence of comorbidities in patients with CAP in Colombia, highlighting hypertension, anemia, and chronic pulmonary disease as the most common. The distribution of these comorbidities varied according to age and sex, with a similar profile observed in those requiring admission to the ICU. These findings highlight the need to develop protocols and policies aimed at recognizing high-risk CAP patients in order to guide interventions that may prevent mortality and improve clinical outcomes.
Footnotes
Acknowledgments
The authors are most thankful for the Universidad de La Sabana.
Ethical approval
The study was conducted in accordance with the principles of the current Helsinki Declaration, as well as local, regional, and international regulations pertaining to clinical research, including Colombian Law on Biomedical Research. Ethical approval was obtained from the Medical Ethics Committee of the Clínica Universidad de La Sabana, Chia, Colombia (approval number: 20220102 Date: 17/01/2022). Approval from the ethics committee waived the requirement for informed consent, in accordance with current regulations for retrospective studies.
Consent to participate
This is a retrospective database analysis study, and consent to participate is waived by the institutional review board.
Authors’ contributions
All authors contributed substantially to the study's conception and design. JSHP, ABG, EATQ, DDQ, and LMLN contributed to the drafting of the manuscript and data analysis. JDCC, MPVB, CMG, JFC, and JMMO participated in data collection and database management. PSM, ICQ, and AMV translated and edited the manuscript. VLF, TSE, and CFAM contributed to data analysis. All authors critically revised and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Universidad de la Sabana Grant (grant number MEDESP-41-2025).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are not publicly available due to privacy concerns and institutional restrictions. Access to the data is restricted and subject to the discretion of the Ethics Committee of Universidad de La Sabana.