
Abstract
Introduction
Worldwide, more than 460 million people suffer from disabling hearing loss. 1 Deaf or hard-of-hearing athletes represent a unique group within the global sports community.
Although deaf athletes may have reduced awareness of certain sport-related risks, their behavioral responses are comparable to those of hearing athletes. 2 While physiological differences exist between hearing and deaf athletes,3,4 deafness in itself does not inherently restrict athletic performance. 5 According to brain plasticity theories, the lack of auditory input can lead to compensatory adaptations, whereby other senses are processed more efficiently—a phenomenon known as cross-modal plasticity.6-8 In this context, parts of the auditory cortex may be repurposed for visual processing. 9 Numerous studies have shown that deaf individuals often outperform hearing individuals on visual tasks, particularly those requiring attention to stimuli in the visual periphery.10,11 Neuroimaging studies have further linked deaf-related structural and functional changes in the right temporal lobe to enhanced visual task performance outside of the imaging environment. 12
Like in the hearing population, many deaf or hard-of-hearing athletes participate in recreational sports, and some are involved in competitive sports. Integration into mainstream (hearing) sports remains a significant issue. 13 While deaf athletes can compete in regular competitions, there is often a lack of structural support and inclusive training environments. Events such as the Deaflympics, founded in 1924, are specifically tailored to deaf athletes, offering full linguistic and cultural accessibility and contributing to a high level of athlete satisfaction. 14
Elite sports for the deaf ensure equal opportunities in competition by taking into account specific sensory impairments. Since the 1960s, deaf sports in Germany have been included in the promotion of top-level sports as an independent sports organization. The German Deaf Sports Association (DGSV) is the German umbrella organization for sports for deaf and hard-of-hearing people. In total, 26 different sports are practiced on a national and international level. 15 Both contact and non-contact sports are represented. The range of sports is extremely diverse and includes, for example, football, handball, motor sports, tennis, swimming, athletics, darts, and chess. 15 With the acceptance into the DGSV squad, the athlete begins to be supported in his athletic activities and competitions in deaf sports on an international level. The athlete has the unique opportunity to belong to international elite of deaf sports and to receive financial support. In addition to the athletic qualification, a hearing loss of at least 55 dB pure tone average (average of hearing threshold levels at a set of specified frequencies: 500, 1000, 2000 Hz) in the better ear is a prerequisite for inclusion in the national squad of a sport and for participation in international competitions. 16 This hearing status must be officially certified by an Otolaryngologist using a form provided by the International Committee of Sports for the Deaf. 15 In competitions for deaf athletes, the use of cochlear implant (CI) speech processors is not allowed. Other hearing devices, such as hearing aids, are also prohibited to ensure equal conditions for all participants.
In the literature, most studies on deaf or hard-of-hearing athletes focus on comparisons with hearing athletes in terms of athletic performance or on athlete satisfaction with specialized sporting events such as the Deaflympics. To the best of our knowledge, we are the first to examine, within an interdisciplinary team of trauma surgeons and otolaryngologists, the provision of hearing systems among elite squad athletes and to evaluate their use, benefits, and potential drawbacks for the athletes.
Materials and methods
The reporting of this study conforms to STROBE guidelines. 17
Participants
In cooperation with the DGSV, all athletes, that are assigned to a squad (n = 170) were contacted online to complete a self-developed questionnaire. All participants provided online informed consent for the data analysis. The local ethics committee of the University Duisburg-Essen has approved the study (No. 20-9761-BO). The prospective clinical study is conducted in accordance with the Helsinki Declaration of 1975 as revised in 2024.
Questionnaire
A self-developed web-based questionnaire (LimeSurvey version 6.10.0 + 250106; LimeSurvey GmbH, Hamburg, Germany) was used, which had already proven its clinical applicability in previous modified versions by our study group.18-20 The questionnaire has been further expanded to include the domain of hearing.
The questionnaire with n = 127 items (multiple choice answers) is divided into the following sections:
Demographic data
Gender, date of birth/age, height, weight Sport and injuries
General information about the sport (e.g. type of sport, squad status, participation in e.g. European Championships, World Championships) Training, injuries Hearing
Type of hearing loss (hard-of-hearing or deaf/congenital or acquired) and other symptoms (e.g. dizziness, tinnitus, surgery) Communication (e.g. in everyday life/training/competition/with coaches/with other athletes) Hearing systems (e.g. type of hearing system (hearing aid/CI), duration of wear in everyday life/training/competition, benefits) Perception (e.g. voice recognition of coach and teammates; hearing as a barrier in interactions; advantage of hearing aids/CI in sports)
Statistical analyses
Statistical analysis was performed using Microsoft® Excel® for Microsoft 365 (Redmond, WA, USA) and IBM® SPSS Statistics 25 software (IBM, Armonk, NY, USA). All values were tested for normal distribution using the Kolmogorov–Smirnov test. The two-tailed t-test was used for normally distributed data and the Mann–Whitney U test for non-normally distributed data. The Kruskal–Wallis test was used to determine differences between more than two groups.
Results
Athletes
Of the n = 7613 active athletes registered with the DGSV, n = 170 were assigned to a squad at the time of the study survey. Of these 170 contacted elite athletes, 105 completed the questionnaire lacking in many areas or not at all. These had to be excluded in the first step. Thus, a total of n = 65 questionnaires remained. However, n = 11 had to be excluded from the analysis due to insufficient or missing data in the section related to hearing. Consequently, data from 54 questionnaires were included in the final analysis (Figure 1).

Flow-chart: overview of participant selection and data inclusion.
The 54 participants (12 females, 42 males) have a mean age of 28.8 ± 10.5 years (min. 13/max. 62 years). Men (n = 42): mean age 30.48 ± 10.58 years; median 29.0 (min. 15/max. 62 years). Women (n = 12): mean age 22.92 ± 7.61 years; median 21.0 (min. 13/max. 43 years). In total, 16 out of 26 possible sports are represented. Most of the 54 participants are active in soccer or futsal (n = 13), n = 7 in handball, n = 6 in shooting, and n = 6 each in tennis and athletics, n = 3 table tennis. Golf, beach volleyball, and badminton are represented by two athletes each; karate, judo, bowling, alpine skiing, triathlon, motor sports, and marathon by one athlete each. All levels from junior to Deaflympics are represented. A total of 28% of the athletes are also supported by the Junior Elite Program and 33% are supported by the Olympic Training Center. Regarding their sporting activities, 87% of the athletes stated that they train in a regular club in addition to their training with the DGSV. In this context, 100% also participate in competitions with hearing athletes (Table 1).
Athlete demographics and participation (n = 54).

Hearing status and hearing systems
Of the 54 athletes, 79.6% had a congenital hearing loss, while 20.4% acquired hearing loss during their lifetime. In total, 50% of the individuals are totally deaf and 42% are hard-of-hearing. Four individuals (8%) have a single-sided deafness and a hearing loss in the contralateral ear. A total of 26% of the athletes report tinnitus, which is bilateral in 64% of the cases (Table 2).
Hearing status and use of hearing systems among athletes (n = 53–54).
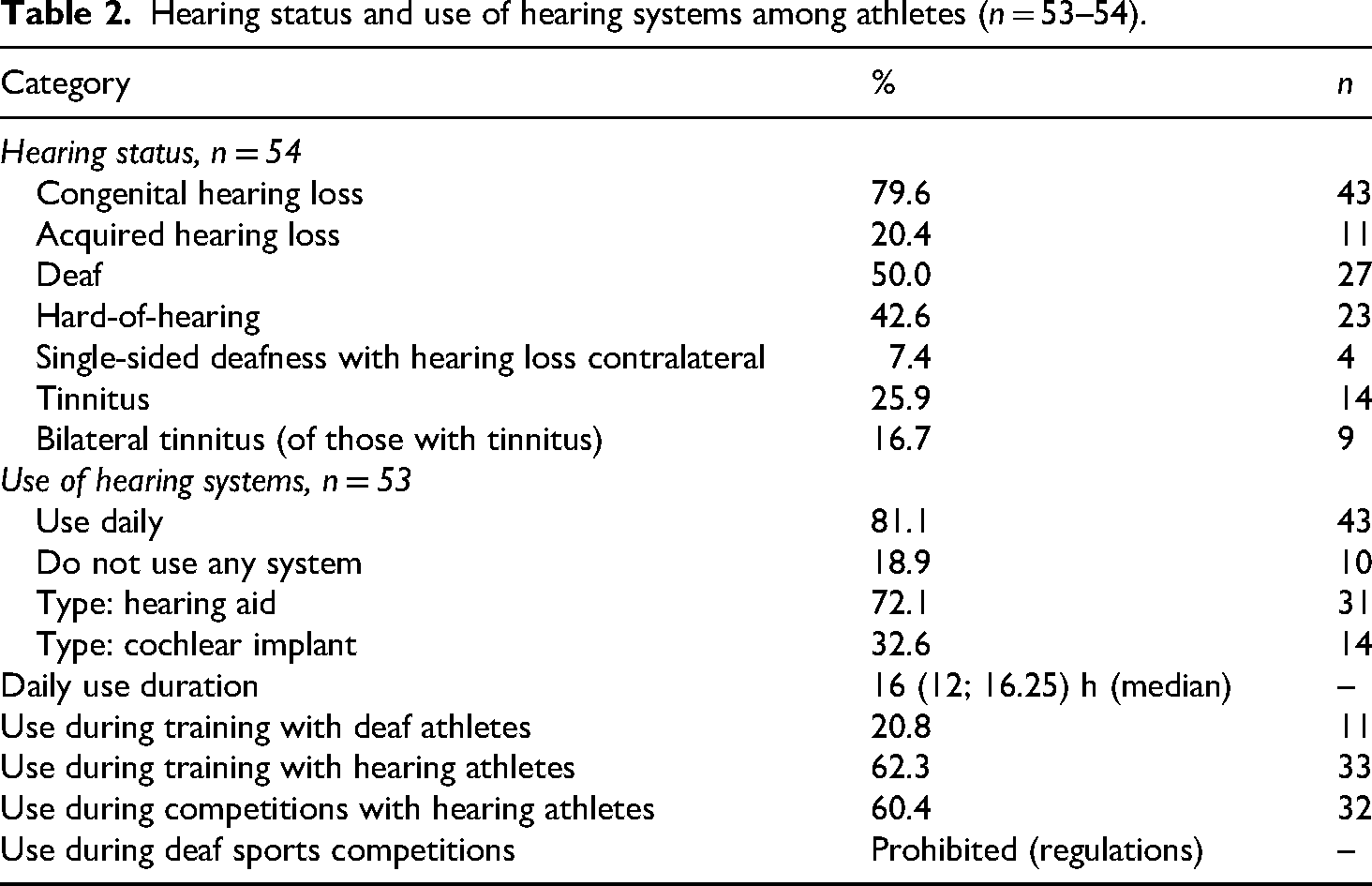
In total, 43/53 (81%) athletes report using hearing systems on a daily basis (n = 1 missing information in a questionnaire). Most common is the hearing aid (72.1%), followed by the CI (32.6%). A total of 19% do not use any hearing systems. The median time spent wearing their hearing devices is 16 (interquartile range (IQR): 12–16) h per day. Only 25% use these during training sessions with other deaf athletes, while 75% use their hearing device during training sessions with other hearing athletes. In deaf sports competition, the wearing of any hearing device is prohibited by the existing regulations in order to maintain equal opportunities. In total, 59% of athletes wear their hearing systems during competitions with hearing athletes. A total of 7.5% of athletes report regular or occasional dizziness. Of the athletes who wear hearing systems, 39.5% participate in contact sports and 60.5% in non-contact sports. Of the athletes who do not wear hearing systems, 40% participate in contact sports and 60% in non-contact sports.
Communication
Communication in everyday life, with the coach and other athletes is mainly through spoken language. In sport, this is followed by signing and lip-reading. Written communication with the coach and other athletes is less relevant than written communication in everyday life (see Figure 2).
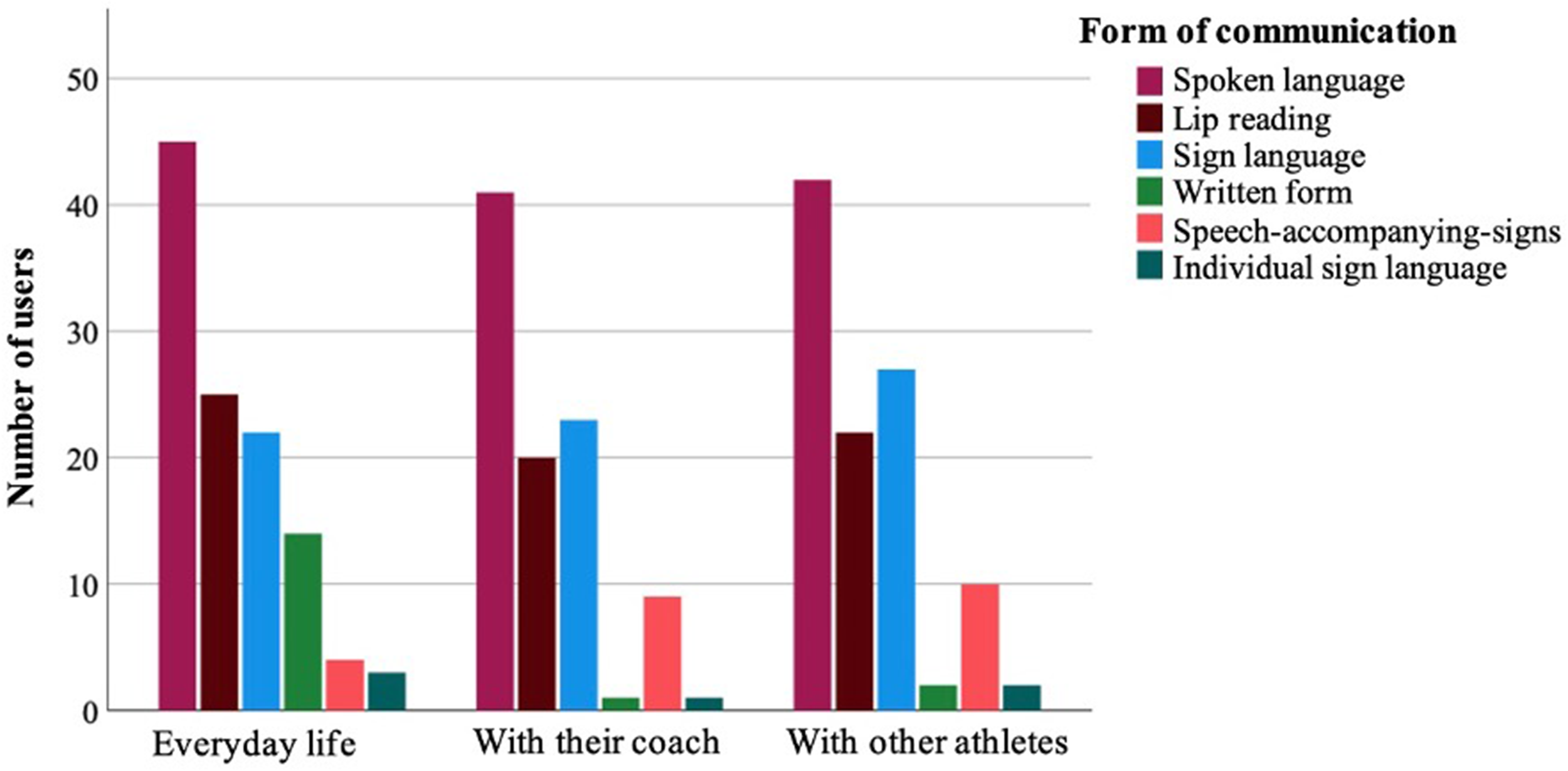
Preferred communication styles in everyday life and sports.
All athletes with hearing systems find them helpful in everyday communication. In total, 90% see a clear communication advantage in sports and 63% find them advantageous in noisy environments during sports.
Injuries
Athletes surveyed see little or no relationship between their hearing impairment and sports injuries they have suffered in the past. A total of 93% state that relationship does not exist or is unlikely.
With regard to injury incidence and downtime, comparative analyses were carried out between (1) athletes who generally use hearing systems and those who do not, (2) athletes participating in deaf sports who use hearing devices versus those who do not, and (3) athletes participating in mainstream (hearing) sports who use hearing devices versus those who do not.
A significantly higher number of work-related incapacities due to sports injuries is observed among athletes who do not use hearing devices (10/53) compared to those who do (43/53), with 0.32 incapacities/1000 training hours (median: 0.41 (IQR: 0.10–0.99)) compared to only 0.14 incapacities/1000 training hours (median 0 (IQR: 0–0.32)) (p = 0.02). No subgroup analysis was conducted for the individual sports due to the high degree of heterogeneity.
In deaf sports training, the injury rate is 3.93/ 1000 training hours among athletes not using hearing devices (median: 1.21; IQR: 0.29–6.00), compared to 1.10/1000 training hours among users (median: 0.49; IQR: 0.00–2.14), with a p-value of 0.09. The total duration of sports-related incapacities is significantly longer in the group of athletes who did not use hearing devices during deaf sports training, with 2.29 weeks/1000 training hours (median: 1.47; IQR: 0.13–4.12), compared to 0.96 weeks/1000 training hours among users (median: 0.00; IQR: 0.00–2.47), with p = 0.045.
In mainstream (hearing) sports training, athletes without hearing aid/CI exhibit an injury rate of 4.66/1000 training hours (median: 1.05; IQR: 0.12–13.45), compared to 2.19/1000 training hours among athletes using hearing devices (median: 0.87; IQR: 0.14–2.35), with a p-value of 0.54. Although this difference is not statistically significant, the data suggest a halving of the injury rate associated with hearing device use during training in hearing sports.
Discussion
According to the World Report on Hearing by the World Health Organization, over 430 million people worldwide will require rehabilitation for hearing loss during their lifetime. 1 Hearing aid provision is typically the first step in auditory rehabilitation. When hearing aids no longer provide sufficient benefit—especially in cases of severe to profound hearing loss—cochlear implantation may be considered to further improve hearing outcomes. Across Europe, approximately 500,000 people use CIs, with around 60% being adults and 40% children. Each year, about 25,000 European citizens receive a CI. Globally, the total number of CIs in use is estimated at around 1 million. 21 Several countries around the world have already successfully established medical CI registries. The national German CI registry, established in January 2022, documenting a total of 2292 cochlear implantations performed during that first year. 22 It should be noted that the current registry data do not yet fully capture the actual number of implantations, as not all clinics have reported their data so far. Comprehensive hearing care not only supports auditory, speech, and language development, but also enhances quality of life and helps prevent social isolation.23,24 Moreover, it has shown significant benefits for individuals with dementia.25,26
To our knowledge, this is the first study to systematically examine the benefits of hearing aids and CIs in elite athletes engaged in competitive sports. In our cohort, 81% of athletes were fitted with hearing aids or CIs, reflecting a notably high level of hearing care within elite squads. In contrast, the HÖRSTAT study reported a 16% prevalence of hearing impairment in the general German population, with only 6.5% using hearing aids. 27 Similarly, the Gutenberg Health Study found that although 34.5% of participants had hearing loss and 47.4% met the criteria for bilateral hearing aid use, only 7.7% were actually using them. 28 Our athletes reported wearing their hearing aids or CIs for a median of 16 h per day. The number of studies including age-matched comparison groups is very limited, as most research focuses either on children or older adults, particularly with regard to processor or hearing aid wearing time. The reasons for this are likely related to the timing of implantation. The vast majority of patients receive implants either in early childhood due to congenital deafness or at an older age due to acquired deafness. Only a small proportion is newly implanted at the age of our athletes.
It has been shown that the highest speech recognition outcomes are associated with more than 10 h of daily CI use in adults. 29 A retrospective cross-sectional analysis of data logs from 1501 Cochlear Nucleus 6 users (aged 0–96 years) revealed that CI users have an average daily device use of 10.74 h across all users and 11.3 h among adults aged 18–64. 30 At older ages (median age: 73 years), the average wearing time for single-sided or bilaterally fitted CI users was found to be 10.35 h/day. 31 The length of time that a hearing aid or CI is worn varies greatly from person to person. Longer hearing aid use tends to be associated with greater hearing loss. In particular, patients who derive a high benefit often use it longer than the average. This can be assumed for our athletes. In addition, it should be noted that our results with 16 h of daily use are based on a self-report and not on an objective measurement (e.g. data logging) and may therefore differ slightly from the actual use. These findings align with those of Holder et al., who reported that participants self-reported an average CI use of 13.0 h per day, whereas objective data logging indicated a significantly lower average of 10.4 h per day—a difference of 2.6 h (p < 0.0001). 32
Athletes with hearing loss communicate differently during competition and training than those with normal hearing. Spoken language is the most common form of communication used by the athletes we surveyed, both in everyday life, and with coaches or other athletes. However, sign language and lip reading are also commonly used. These forms of communication have played and continue to play a role not only within the deaf community, but also in official competitions where hearing aids/CIs are not allowed. 16 Sign language allows deaf or hard-of-hearing people without hearing devices to communicate with each other. At the Deaflympics, which have been held since 1924, and at the World and European Championships, most deaf athletes have used sign language, at least in the past. A study of collegiate athletes showed that deaf athletes preferred to communicate with their coaches using sign language, while hard-of-hearing athletes preferred spoken language. 33 Athletes’ satisfaction during competitions depends to a large extent on communication. 14 Since individuals with hearing loss are at greater risk of misunderstandings, it is essential to reduce communication barriers. In this context, sign language coaches can play a supportive role.
With the introduction of newborn hearing screening in many countries, including Germany in 2009, hearing loss is being detected earlier.34,35 This leads to earlier provision of hearing aids and implantation of CIs. As a result, more and more deaf or hard-of-hearing children are able to attend mainstream schools, where sign language is not taught. Less than 10% of children with hearing loss or deafness have one or two deaf parents, which means that sign language is probably not used in all families. 36 Thus, more and more children have less and less contact with sign language, and whether or not they learn it is left to their parents. In the future, this may lead to athletes feeling excluded in special situations, such as deaf competitions, because they are not fluent in sign language. 13 Since the early implantation of CIs in children has only been performed for a few years and parents are increasingly educating their deaf or hard-of-hearing children in spoken language, without using sign language, it remains to be seen how the use of sign language will develop in the next few years in everyday life and within the deaf community or at deaf sports events.
The athletes surveyed see little or no connection between their hearing impairment and sports injuries they have suffered in the past. Hearing loss has been shown to be associated with poor balance and postural control.37,38 However, participation in sports seems to improve balance and gait in hearing-impaired children and adults. 39 As we were studying competitive athletes, the balance in our cases is very well optimized by regular training. Only 7.5% of the athletes (4/54) we surveyed report regular or occasional dizziness. They practice golf, soccer, and athletics. The individuals included in our study experienced a relevant number of injuries to all parts of the body, resulting in significant time off work, incapacity to work and medical consultations. 18 Although our sample size is relatively small, the data suggest a potential protective effect of wearing a hearing aid or CI with respect to sports injuries. This can be compared to traffic-related injuries among pedestrians and passengers, where more accidents occur with a higher degree of hearing loss.40,41 However, these real-world data in a small cohort would need to be revalidated in a larger number of cases.
Limitations
This study has several limitations. First, the relatively small sample size may limit the generalizability of the findings. The voluntary participation introduces the possibility of selection bias, as those who chose to respond may differ systematically from those who did not, particularly regarding their use of hearing systems. Additionally, the data are based on self-reported information, which may be subject to recall bias or social desirability bias—especially in reporting hearing aid or CI usage durations. Objective verification of device usage (e.g. data logging) was not performed.
The questionnaire design, while interdisciplinary and comprehensive, may not fully capture the nuanced experiences of all athletes, especially across different types of sports or communication methods. Finally, while the study focused on elite athletes, the findings may not apply to recreational athletes or younger individuals with hearing loss who are still in early training phases.
Conclusion
This interdisciplinary study is the first to systematically investigate the use and perceived benefits of hearing devices among elite deaf and hard-of-hearing athletes in Germany. The results show a high rate of hearing aid and CI use, with a median daily usage of 16 h. Athletes reported clear communicative advantages in both everyday life and during sports activities—especially in mixed training environments with hearing athletes.
A significantly higher number of work-related incapacities due to sports injuries is observed among athletes who do not use hearing devices, indicating a potential protective effect. Although such devices are prohibited in official deaf competitions, their role in training and communication highlights their broader value beyond auditory rehabilitation alone.
These findings emphasize the importance of personalized hearing care and inclusive training settings in elite sports. Future research should include larger cohorts and objective data collection (e.g. device data logging) to validate these initial findings and inform evidence-based recommendations for athletes with hearing loss.
Footnotes
Acknowledgments
We used AI (ChatGPT) for language improvement.
Ethical approval
The local ethics committee of the University Duisburg – Essen has approved the study (No. 20-9761-BO).
Informed consent
Online informed consent is given by all participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will be shared upon reasonable request.