
Abstract
Objective
To evaluate outcomes of cochlear implantation (CI) in patients with unilateral sensorineural hearing loss (USNHL) and explore effects and stimulation current in USNHL patients with bony cochlear nerve canal (BCNC) stenosis versus normal cochlear nerve canals.
Methods
A prospective study was conducted on 23 USNHL patients who underwent CI (MED-EL) from May 2019 to March 2023. Preoperative CT and MRI scans were performed to measure BCNC width. Subjects were divided into BCNC stenosis (BCNC-S) and BCNC normal (BCNC-N) groups. Hearing thresholds, speech recognition scores (SRS), sound localization ability, and auditory/musical abilities were assessed before and two years after CI. Differences were determined using Stata statistical software, with significance defined as p < .05.
Results
Eleven patients were diagnosed with BCNC stenosis. CI significantly improved SRS under noisy conditions (p = .027) and sound localization ability (p < .05), as well as auditory and musical quality (p < .05). No significant differences in outcomes were found between BCNC-S and BCNC-N groups. BCNC-S group had higher stimulation current than BCNC-N group.
Conclusions
CI provides similar improvements for USNHL patients with or without BCNC stenosis.
Significance
The findings will contribute to the understanding of cochlear implant outcomes in patients with USNHL and BCNC stenosis.
Introduction
According to the estimation of the universal newborn hearing screening program, about 1–2 in 1000 newborns suffer from significant hearing loss, with unilateral deficit accounting for one-third of all these subjects with permanent hearing loss. 1 Unilateral sensorineural hearing loss (USNHL) has been defined as the condition that one ear presents severe to profound deafness while the hearing threshold of the other side is normal or near-normal. 2 Many literatures highlighted the negative consequences of USNHL, including delayed auditory skills, difficulties in sound localization and speech understanding under noisy environment, and reduced hearing-related quality of life.2–4 With the growing awareness that sound input of both ears is essential for binaural hearing, treatments for USNHL has increased rapidly in recent years. 5
In the past, treatments for USNHL have mainly been focused on acoustic hearing aids, contralateral routing of signal (CROS) hearing aid and bone conduction hearing device (BCHD).6,7 Cochlear implantation (CI) have been used to improve hearing for bilateral deafness for over 40 years. The latest development is the application of this technology to USNHL, which was approved by the USA Food and Drug Administration in July 2019. 8 Many researchers have reported that CI can benefit USNHL patients significantly in various aspects, including speech perception both in quiet and noisy conditions, sound source localization, tinnitus, and patients’ subjective audiological outcomes, etc.4,9 In addition, a review of literatures reveals that the improvements brought by CI seem to be greater than what conventional options such as CROS and BCHD are able to achieve, which was superior to CROS specially in speech perception under noisy condition and sound localization.10,11 Above all, CI are currently considered the tool most likely to realize binaural hearing in adults and children who are affected by severe-to-profound USNHL.8,10
Early identification of hearing loss and understanding its etiology can assist with prognosis and counseling of families. 12 The etiology of congenital USNHL is less clear than that of bilateral sensorineural hearing loss, and although the specific etiology cannot be identified in most cases, the literature indicates a high incidence of inner ear malformation in congenital USNHL cases. Using CT and/or MR imaging techniques, the cause of USNHL was identified in 49% of patients, and the most commonly involved site was the labyrinth (29%), followed by the cochlear nerve (9%) and the brain (7%). 13 Bony cochlear nerve canal (BCNC) stenosis, first reported in 2000, can cause varying degrees of sensorineural hearing loss (SNHL), which may be an indicative of embryologic malformation of the cochlear nerve, 14 and is considered to be associated with up to 10% of pediatric hearing loss. 15 The diagnostic criteria for BCNC are mainly computed tomography (CT) imaging with a diameter of less than 1.5 mm threshold, and MRI findings of cochlear nerve hypoplasia. Although few articles based on bilateral BCNC who underwent unilateral CI indicated that CI can effectively stimulate the cochlea and bring satisfied improvement with a higher current, it's outcomes have not been fully elucidated because of small sample size or short-term follow-up.15,16 At present, there are no reports on the difference of cochlear stimulation current and the efficacy of CI in patients with SNHL caused by BCNC stenosis and unilateral deafness with normal BCNC.
In this study, we designed to analysis the auditory benefits of unilateral CI for patients affected by congenital USNHL, and also to explore the effects and stimulating current in USNHL patients with BCNC stenosis versus normal cochlear nerve canals.
Materials and methods
Ethical considerations
The study was approved by the Institutional Review Board of Peking Union Medical College Hospital (PUMCH; Beijing, China. Microtia genetics analysis. Protocol#: JS-795, approved at January 2016). We conducted our study in accordance with the Helsinki Declaration of 1975 as revised in 2024. All patients or guardians signed written informed consent.
Participants
This single center prospective study recruited Mandarin speaking patients with congenital USNHL who underwent unilateral CI surgery at PUMCH from May 2019 to March 2023. Patients were selected consecutively based on the following inclusion criteria: failed the hearing screening test at birth on one side, and later the hearing tests indicated profound congenital USNHL (affected side mean hearing threshold >80 dB HL and the other side is normal); with age 10–40 years old; performed preoperative CT and MRI evaluations; undergoing unilateral CI with a device manufactured by MED-EL; with no history of hearing aid using. The exclusion criteria were as follows: diagnosed with bilateral hearing loss; acquired USNHL due to infection or any other reasons; congenital UNHL of any clear etiology other than BCNC stenosis, such as cochlear malformations, acoustic neuroma, or auditory neuropathy, etc.; with any type of physical, psychological, or emotional disorder that would interfere with the ability to complete the tests; or incomplete data collection. The patients were divided into two groups according to the measurement of BCNC based on preoperative CT data, with dysplasia of the cochlear nerve shown on MRI (Figure 1). Subjects with BCNC < 1.5 mm were included in the BCNC stenosis (BCNC-S) group, while those with BCNC > 1.5 mm were included in the BCNC normal (BCNC-N) group.

Representative computed tomography images of the patient with left side bony cochlear nerve canal (BCNC) diameters: (a) The right side with BCNC = 1.6 mm normal; (b) The left side with BCNC = 0.9 mm; (c) The magnetic resonance imaging (MRI) shows the normal and the stenotic cochlear nerve; (d) MRI reconstruction of cochlea reveals bilateral cochlear nerves. (e) Picture of the surgery where cochlear electrodes are implanted into the round.
Device fitting
The CI was activated four weeks after surgery based on the postoperative CT data to realize an anatomic-based fitting, 17 with four maps set up for using. To obtain comfortable hearing levels, each fitting was adjusted based on the patient's behavioral responses. All subjects could choose their favorite map to use in their daily life and subsequently returned to undergo fitting 1, 3, 6, 12 and 24 months after activation. The detailed map-usage records as well as electrode stimulation current would be exported and analyzed at the 24th month fitting time, with all hearing tests and questionnaires finished under best-aided conditions. The mean stimulation current of electrodes 1, 6, and 12 (of the most commonly used program) between BCNC-S and BCNC-N groups were compared.
Hearing and speech evaluation
In both unaided and CI assisted situations, the speaker was placed one meter in front of the subject and the sound field thresholds of 0.25, 0.5, 1, 2, 3, 4, 6, and 8 kHz were tested in a soundproof chamber, respectively. In both quiet and noisy conditions, the percentage of speech perception was measured using a two-syllable test consisting of 10 lists, each containing 50 Chinese characters or spontaneous words. 18 In the noise-free test condition (0° azimuth), the signal is placed directly in front of each individual, and in the sound condition of 0° azimuth, both the signal and the noise are placed directly in front of the individual. The intensity required for the intelligibility score and the highest intelligibility score is assessed under quiet conditions. Under noise condition, the speech stimulus is set 65 dB SPL and the speech shape noise level is 60 dB SPL (signal-to-noise ratio +5). Average hearing thresholds were calculated at 0.5, 1, 2, and 4 kHz frequencies, and average speech perception results were analyzed after three repetitions in quiet and noisy conditions, which were all compared respectively.
Sound localization ability evaluation
Sound localization ability was evaluated with loudspeakers located as illustrated in Figure 2. The seven loudspeakers visible to the subject were placed 1 meter from their head at 30° intervals, from −90° to 90° in an azimuth. Since all participants had unilateral CI implants, the effect on the implantable side was balanced by defining the sound positions on the same and opposite sides of the implant as positive and negative, respectively. The LOC (v2.2.3) software was applied to generate white noise stimuli in random order, twice per Angle and six times per speaker at 65, 70 and 75 dB sound pressure levels, for a total of 42 presentations. During the test, participants had to sit up straight, look straight ahead and try to indicate which speaker the sound was coming from by listening. Participants are accompanied at all times by two experienced operators. If there is any significant head rotation, the test will be regarded as invalid and participants will be asked to repeat the test under the same conditions. The operator will record every reaction of the participant, while the LOC will automatically record the actual source. Responses more than 5 s after the stimulus will be judged as guesswork and excluded from statistical analysis. Patients were tested under both unaided and with unilateral CI. Percentages of accuracy (precisely/within a 30° deviation) for each presented angle and bias angles of unaided and CI aided are presented and compared. The root mean square (RMS) errors of different sides under both conditions are also evaluated.

Sound source test scene display diagram. Seven speakers were placed in front of the subject at −90°, −60°, −30°, 0°, 30°, 60°, and 90°. When the sound source is on the same side of the implant, the angle is defined as a positive number, and vice versa. Each participant was tested for both unaided and unilateral CI.
Questionnaire
Two validated questionnaires were used to assess subjective auditory benefits, and face-to-face interviews were conducted to assess auditory and music appreciation abilities two years after CI activation.
The Chinese version of the Abbreviated Profile of Hearing Aid Benefit (APHAB-CH) questionnaire was used to assess perceived communication benefits with unilateral CI in different hearing situations. There are 24 items in this questionnaire, which involve hearing comfort in different living conditions, mainly divided into the following four dimensions with each including six questions: Ease of Communication (EC), assessing the ease of communication under favorable conditions; Reverberation (RV), assessing communication ability under high reverberation conditions; Background Noise (BN), assessing communication ability in noisy environments; and Aversiveness of Sounds (AV), assessing the unpleasant or harsh of environmental sounds in daily life. On each question in the questionnaire, subjects were asked to quantify how often this occurred: always (99%), almost always (87%), usually (75%), half the time (50%), sometimes (25%), rarely (13%), and never (1%), with the lower the percentage, the better the sense of hearing. 19
The Munich music questionnaire was used to evaluate the participants’ musical perception, sound quality and enjoyment of music. The questionnaire assesses the musical experience, including listening time, sound quality, instrument recognition, recognition of different components of music, past and present musical activities, and listening environment. Each item was scored on a 5-point Likert scale, with scores of 1, 2, 3, 4, and 5 indicating that the music was not important, little important, moderately important, important, and very important, respectively. 20
Statistics
Quantitative parameters were reported as means ± standard deviations (SDs), and qualitative parameters as frequencies (percentages). Random distribution of scores was assessed using nonparametric Friedman tests. Normally distributed qualitative data were compared by Pearson's coefficient analysis, and nonnormally distributed data by Kendall's tau analysis. All data were analyzed using GraphPad Prism software (v.6, GraphPad Inc., San Diego, CA, USA), with p-values <.05 defined as statistically significant.
Results
Participants
This study enrolled 23 patients, seven males and 16 females, with mean age of 16.6 ± 6.2 years (range, 11–36 years); 11 subjects were identified as the BCNC-S group while 12 were included in the BCNC-N group and their individual characteristics are reported as Table 1. The mean BCNC diameters of BCNC-S and BCNC-N groups are 0.98 ± 0.15 mm (range,0.8–1.2) and 1.80 ± 0.12 mm (range,1.6–2.0), respectively. Implant electrodes of appropriate length were selected based on preoperative CT evaluation, with 16(∼70%) patients implanted with FLEX 28 electrode arrays and 7(∼30%) with Standard electrode arrays. All of the patients underwent complete scala electrode insertion. The Patients’ characteristics and demographics were shown in Table 1.
Patients’ characteristics and demographics.

Note: BCNC-S: bony cochlear nerve canal-stenosis; BCNC-N: bony cochlear nerve canal-normal.
Greater benefits in speech recognition score in both BCNC-S and BCNC-N groups
Two years after CI activation, the mean hearing thresholds of the BCNC-S and BCNC-N groups were 20.5 ± 3.5 dB SPL and 21.8 ± 2.5 dB SPL, with unaided hearing thresholds of 23.2 ± 6.6 dB SPL and 25.0 ± 3.9 dB SPL, respectively. The mean frequency specific thresholds at 0.25, 0.5, 1.0, 2.0, 3.0, 4.0, and 8.0 kHz of different groups were shown in Figure 3. The mean speech recognition score (SRS) at 65 dB SPL unaided and with unilateral CI were 97.8 ± 1.3% and 98.7 ± 1.0% under quiet conditions and 65.0 ± 4.0% and 83.2 ± 2.6% under noisy conditions (signal-noise ratio +5), respectively. The results of different groups are compared and shown in Figure 4.
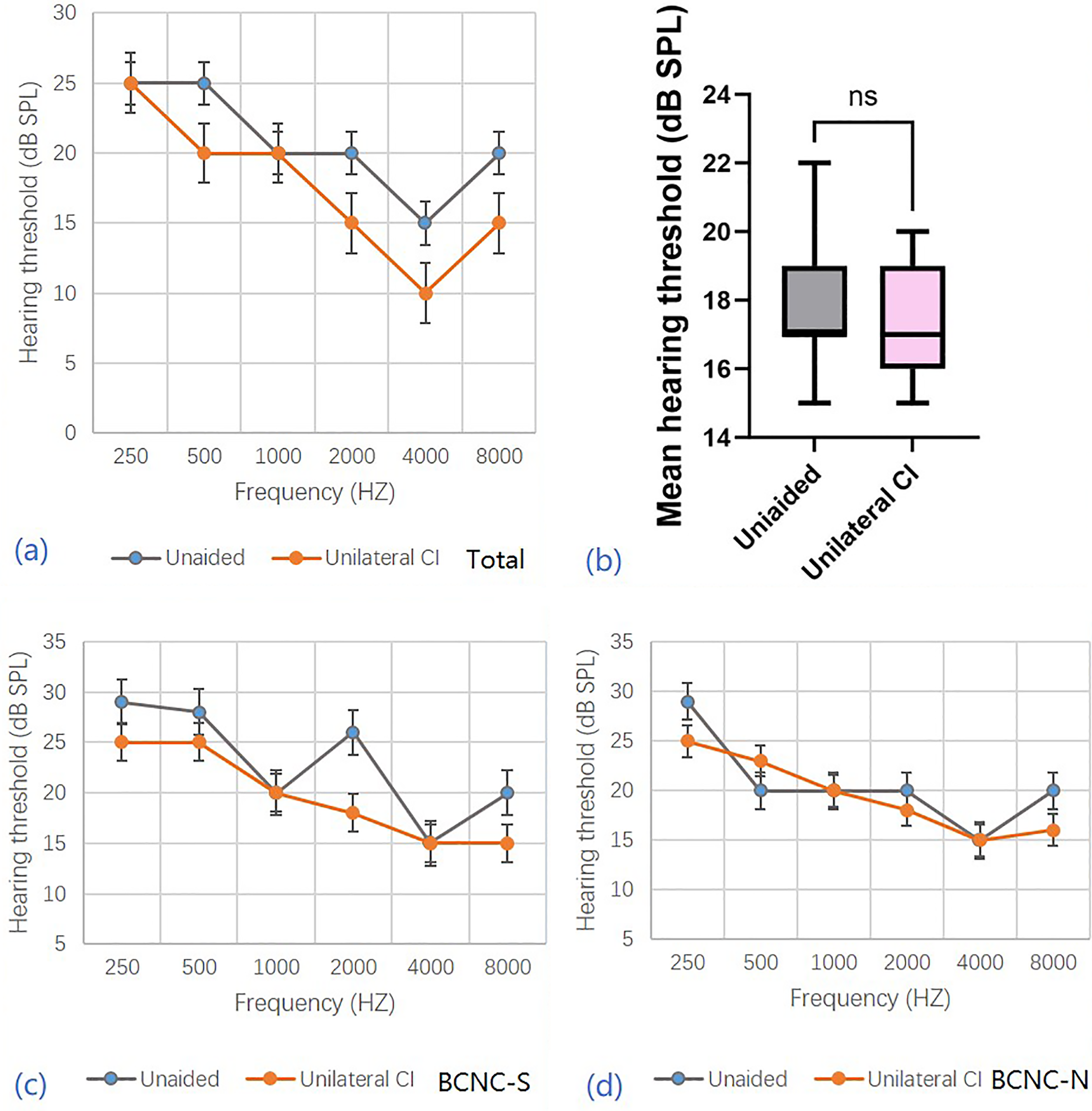
The frequency specific thresholds and the comparison of BCNC-S and BCNC-N groups unaided and with unilateral CI. (a) The frequency specific (0.25, 0.5, 1.0, 2.0, 3.0, 4.0, 8.0 KHZ) thresholds of all 23 subjects. (b) The comparison of mean hearing thresholds (0.5, 1.0, 2.0, 4.0 KHZ) unaided and with unilateral CI. (c) The frequency specific (0.25, 0.5, 1.0, 2.0, 3.0, 4.0, 8.0 KHZ) thresholds under unaided and unilateral CI conditions of BCNC-S group. (d) The frequency specific (0.25, 0.5, 1.0, 2.0, 3.0, 4.0, 8.0 KHZ) thresholds under unaided and unilateral CI conditions of BCNC-N group. Values represent mean ± standard error of mean.

The speech recognition scores (SRS) and its improvement both in quiet and in noise under different conditions. (a) The SRS in quiet under different conditions of different groups. (b). The SRS improvement in quiet of different groups. (c) The SRS in noise (signal-noise rate: +5) under different conditions of different groups. (d) The SRS improvement in noise (signal-noise rate: +5) of different groups.
The differences of mean hearing thresholds, SRS under quiet and noisy conditions unaided and with unilateral CI were investigated. The differences of SRS improvement between BCNC-S and BCNC-N groups were also analyzed. The mean hearing thresholds were better with the CI than unaided, but these differences were not statistically significant. The SRS both under quiet and noisy conditions were significantly better with unilateral than unaided (p < .05), while the differences of SRS improvement between BCNC-S and BCNC-N groups were not statistically significant (p = .84, p = .71, respectively). The mean stimulation current of electrodes 1, 6, and 12 (of the most commonly used program) was significantly higher of BCNC-S than BCNC-N group (Figure 5).

The comparison of stimulation current of electrodes 1, 6, and 12 (of the most commonly used program) of BCNC-S and BCNC-N groups. (a)The mean stimulation current difference. (b) The difference between means of two groups.
Better sound localization ability with CI for USNHL
Direct comparisons of percentage of accuracy response, bias angle and RMS error for unaided and unilateral CI were shown in Figure 6. The percent accuracies for a precise answer for unaided and unilateral CI were 32.4 ± 2.1% and 46.7 ± 2.5%, respectively (p < .05, whereas the percent accuracies within 30° for were 39.8 ± 2.9% and 55.7 ± 3.4%, respectively (p < .05). The bias angles following unaided and unilateral CI were 49.9 ± 3.8° and 27.6 ± 2.1°, respectively (p < .05). The RMS errors unaided and with unilateral CI were 73 ± 2.9° and 61.2 ± 4.2°, respectively (p < .05). Differences of the above parameters between BCNC-S and BCNC-N groups were all not statistically significant (p > .05).

Sound localization ability measurements in unaided and unilateral CI. (a) Percentages of accuracy (precisely/within a 30° deviation) following unaided and unilateral CI, and (b) comparison between BCNC-S and BCNC-N groups under unaided condition and (c) with unilateral CI. (d) Bias angle of all subjects unaided and with unilateral CI, and (e) the comparison of BCNC-S and BCNC-N groups under unaided condition and (f) with unilateral CI. (g) RMS error following unaided and unilateral CI, and (h) comparison between BCNC-S and BCNC-N groups under unaided condition and (i) with unilateral CI.
Questionnaire results
All 23 patients completed the APHAB-CH questionnaire (Figure 7), with all reporting statistically significant benefits from the CI. EC and BN scores were better with the CI than unaided, whereas scores on the AV higher with CI than unaided and RV subscales did not differ significantly. The numbers of points did not differ between BCNC-S and BCNC-N groups (p > .05).
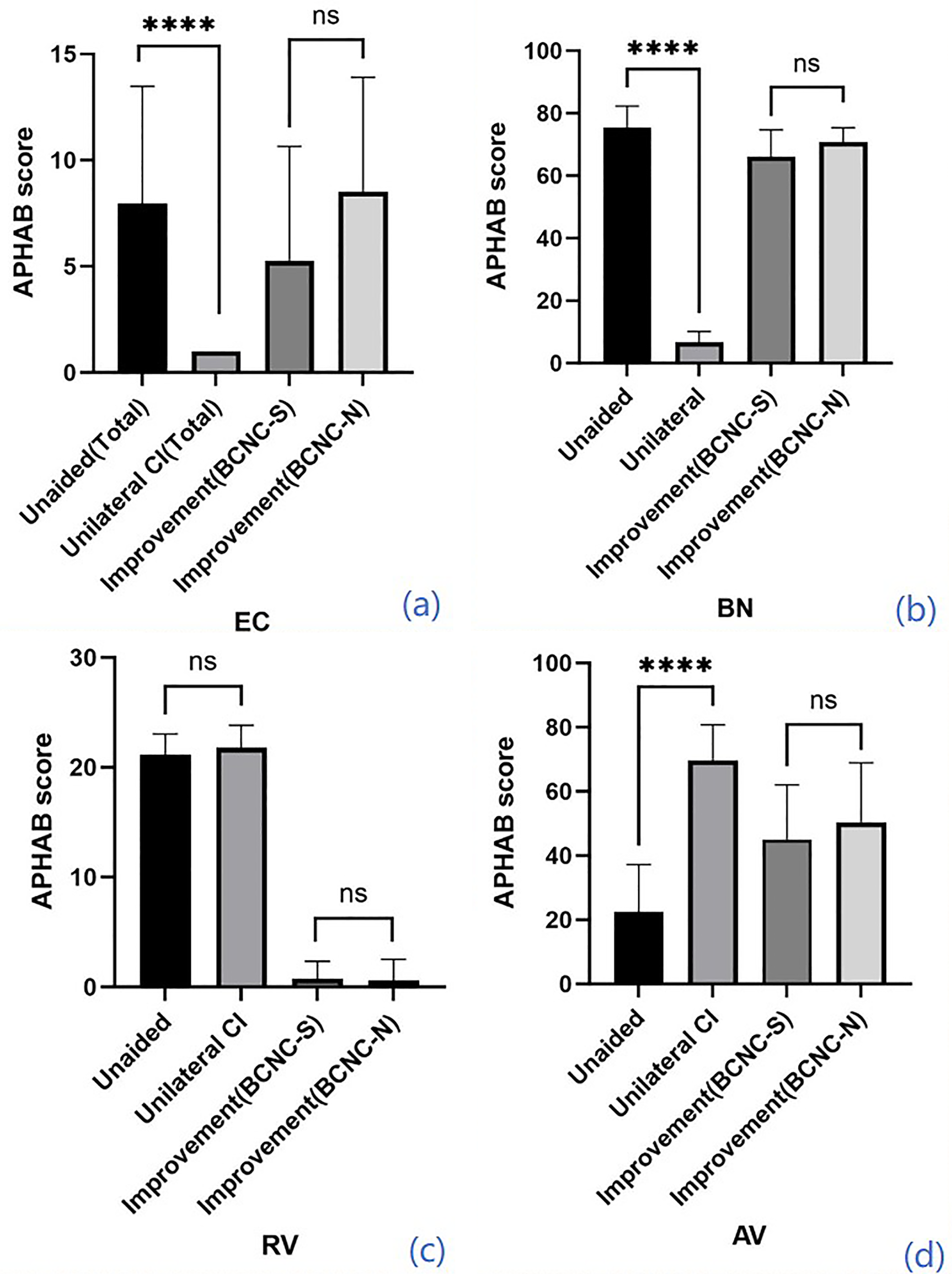
APHAB scores under different conditions (unaided, with unilateral CI) and the improvement comparison of different groups. Values are represented as mean ± standard error of mean for each subscales: EC, ease of communication; BN, background noise; RV, reverberation; AV, aversiveness. Lower scores indicate better functional results.
Mean scores of music feeling in daily life under unaided and unilateral CI conditions were 2.57 ± 0.84 and 4.13 ± 0.69, respectively. Unilateral CI could bring better feelings about music and music habits than the unaided with scores being significantly higher (p < .0001) (Figure 8). Of two groups, the mean improvement didn’t differ significantly (p > .05).
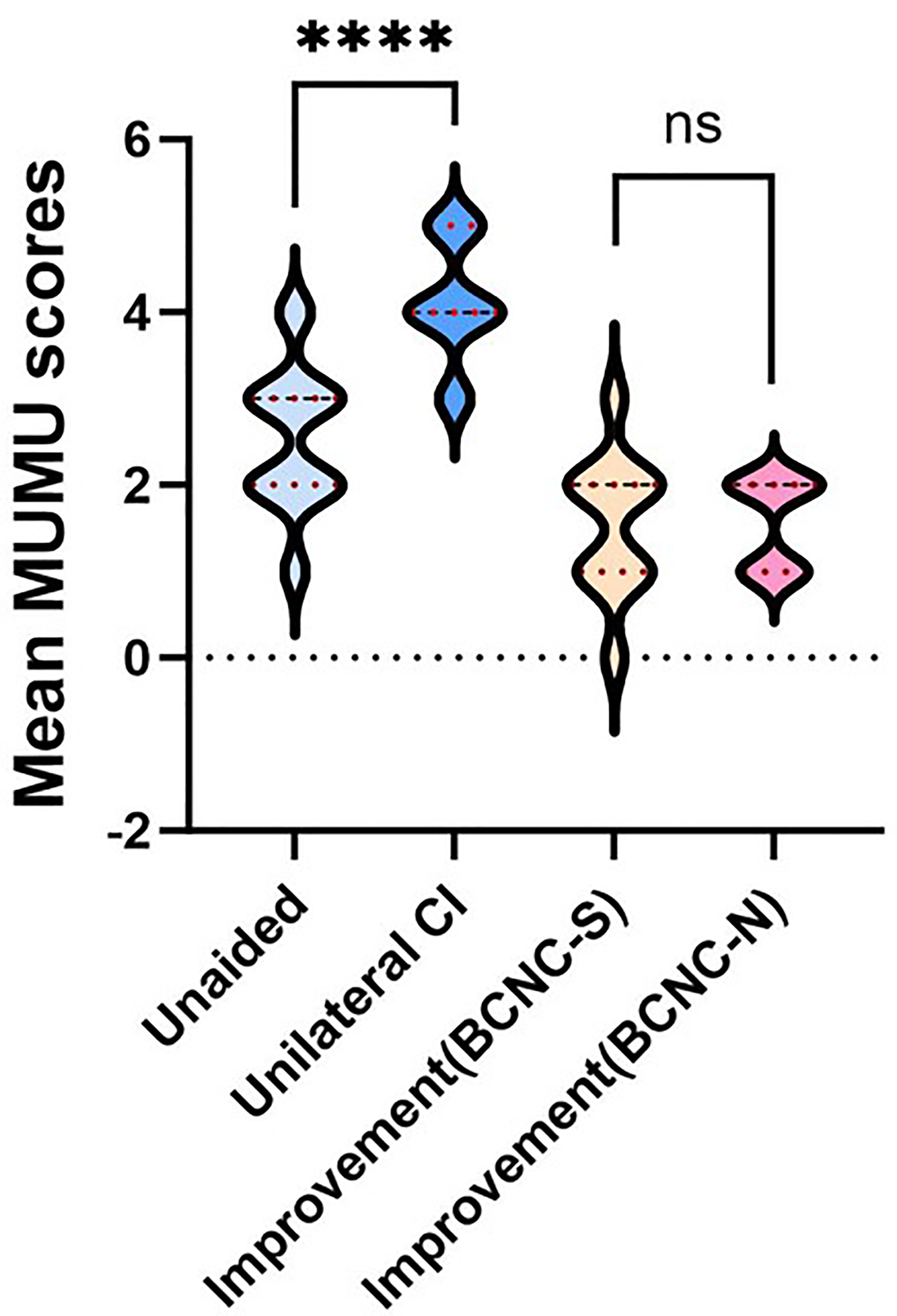
The mean MUMU scores under different conditions (unaided and with unilateral CI) and the comparison between BCNC-S and BCNC-N groups. Values are represented as mean ± standard error. Higher scores indicate better functional results.
Discussion
Taken together with the extant literature, the present study offers three principal contributions that refine our understanding of unilateral CI for children with profound USNHL. First, it corroborates and extends the accumulating evidence that restoring bilateral input through CI is superior to traditional routing devices. Earlier small-series reports21,22 already hinted at better speech-in-noise and sound-localization outcomes with CI, but lacked controlled comparisons across listening conditions. By systematically testing both quiet and spatialized noise, the current data confirm that the implanted ear supplies sufficient temporal and spectral cues to reestablish binaural summation and squelch. The observed gains in localization, variable yet consistently present, align with the adult findings of Mertens et al. 23 and underscore that only genuine bilateral stimulation—not CROS or BAHA—can overcome the head-shadow and binaural unmasking deficits inherent to USNHL.
Second, the study is the first to stratify pediatric CI outcomes by BCNC status. Previous imaging studies24,25 linked BCNC stenosis to cochlear nerve deficiency and predicted poorer performance, leading many programs to withhold implantation. The present results contradict this pessimism: children with BCNC stenosis achieved speech-recognition and localization benefits comparable to those without malformations, despite requiring higher stimulation currents. This parallels the recent bilateral-implant cohort of Zhang et al. 16 and suggests that higher charge densities can effectively recruit surviving neural fibers even when the canal is narrow. The implication is that BCNC stenosis should no longer be an exclusion criterion; instead, it should trigger closer audiological and radiological counseling while still permitting candidacy.
Finally, the findings reinforce the developmental imperative for early bilateral input. Earlier population studies associated untreated USNHL with high rates of grade retention and speech therapy; the current functional data provide a mechanistic explanation—deficient binaural hearing—and demonstrate that these sequelae can be mitigated by timely CI.
Functional hearing requires sound input from both ears
The use of neonatal hearing screening has made it possible for the identification of congenital UNHL immediately after birth, with estimation of the universal newborn hearing screening programs suggesting that around 1 to 2 in 1000 infants have significant hearing loss, with a unilateral deficit representing one-third of all the children born with permanent hearing loss.1,12 In the past, UNHL has gone untreated, either because patients perceive that this unilateral hearing loss has little impact on their lives, or because these subjects do not find satisfactory outcomes from existing treatment options. This causes many patients to experience significant hearing asymmetries in their daily lives. 26 However, recent research evidence overturns the notion that relying on one side of normal hearing is sufficient and highlights the importance of using both ears for sound input and developing binaural listening skills, which are critical for speech and language development, effective communication, and overall academic success. 12 Studies show that of all children with UNHL, about 35% fail at least one grade in elementary school, and more than 50% have learning or behavioral problems. Compared with their peers with normal hearing, children with UNHL are more likely to have impaired speech development and receive speech therapy. 27
The audiological dysfunction caused by UNHL consists of two main aspects, especially when the degree ranges from severe to profound. On the one hand, these patients lose the advantage of binaural hearing in specific communication tasks, resulting in a decline in speech recognition in noisy environments. One the other hand, normal hearing individuals primarily use interaural level difference cues and interaural time difference cues to localize sounds, however, in the absence of more effective binaural cues, severe to profound UNHL subjects use monaural cues for horizontal sound localization, and thus tend to have poor sound source localization. 28 In this study, we analyzed the hearing ability of 23 patients with profound UNHL, with the consistent finding that UNHL is poor in speech recognition (both under quiet and noisy conditions) and sound source location. In order to ensure a high quality of life, auditory intervention may be essential for these patients.
CI can improve UNHL's auditory perception and sound source localization ability
Interest in the management of UNHL has significantly increased in recent years. The reasons stem primarily from the growing awareness that functional binaural hearing requires sound input for both ears. Until the last decade, CROS or BAHA™ have been the primary rehabilitation options. These traditional intervention devices do not restore hearing in poor ears and do not enable true binaural input or binaural processing. Instead, these devices can only transmit signals received by the poor ear to the better ear. Although these arrangements improved sound awareness and head shadow effects, hearing was not restored to the poorer ears, and higher order binaural processing was not possible, and thus users continue to suffer from reduced understanding of speech in noise, poor sound localization. The finding that the contralateral path of the signal is not sufficient to force significant changes in sound localization or speech understanding, and that subjective ratings of performance or benefit are inconsistent, does reflect the underlying problem is a lack of genuine bilateral input.10,29 CI is the most recent treatment option for UNHL. Although it requires invasive surgery and adaptation may take longer, they are considered a safe and effective procedure. 29 Because CI is quite expensive and the cost has to be paid by the patient himself/herself out of pocket, it often requires careful consideration and decision-making. In this study, the patients tried on the soft band CROS and BAHA at the outpatient clinic, but they felt that they couldn't achieve satisfactory results. After understanding the working principles of CROS, BAHA and CI, the patients or their guardians eventually chose CI.
In 2010, Arndt et al. conducted a study comparing CROS/BAHA™ with cochlear implants as a treatment for UNHL. They found that in patients with UNHL, cochlear implants not only performed better, but they also performed better compared to traditional CROS/BAHA™. The results of this study are encouraging and have generated great enthusiasm for the use of cochlear implants in UNHL. 21 Cochlear implants were originally developed to help patients with bilateral deafness. In recent years, more and more scholars have studied the effectiveness of cochlear implants in improving speech perception in patients with unilateral deafness. 27 In 2017, Finke et al. 22 studied 48 patients and found that speech perception was significantly improved in both quiet and noisy environments. In 2018, Doge et al. 30 reported that a majority of patients (eight out of 11) showed a tendency to improve speech perception in complex noise. In this study, the SRS both under quiet and noisy conditions are improvement significantly. For subjective questionnaire evaluation, the AV scores, representing the level of dislike for the sharp sounds of life, such as car horns, construction sites and so on, are higher with CI than unaided. This may be due to long-term adaptation to monaural listening, which takes longer to adapt to these more uncomfortable sounds, or to the transition by choosing a lower stimulus program.
Besides, improved sound localization with CI is a key advantage over traditional CROS hearing aids and BAHA treatment options. Sound source localization is generally improved after CI in patients with SNHL, but the degree of improvement varies from study to study due to the complicating factor that the number of speakers, placement of speakers, spacing between speakers, and other details differ between studies. 23 In this study, all patients obtained different degrees of improvement in sound source localization ability.
CI could bring satisfied results for patients with USNHL due to BCNC stenosis with higher stimulation current
The cause of congenital USNHL is much less clear cut than bilateral sensorineural hearing loss, and although the specific cause is not often identified, the literature suggests a high incidence of inner ear malformation in cases of congenital USNHL. Identifying inner ear malformations is critical to elucidating the underlying pathology, providing key information on possible progression of hearing loss or contralateral involvement, and providing advice and treatment tips. In fact, among other factors known to influence the outcome of cochlear implants, the choice and degree of benefit of cochlear implants depends on neuronal health and the presence of inner ear malformation. Aplasia or hypoplasia of the auditory nerve is the primary concern, due to the possibility of compromising nerve stimulation through electrical impulses delivered by the cochlear implant. 25
The BCNC is located between the base of the inner ear canal and the base of the cochlea. It allows nerve fibers to extend from the cochlear nerve to the spiral ganglion. The width of the BCNC is measured in the middle section between the inner edges of its bone wall. Thus, narrowing of the BCNC may lead to functional or anatomical disturbances of the cochlear nerve (CND). In fact, axial plane BCNC width less than 1.4 mm is associated with CND. One study found such a narrow BCNC in approximately 60% of patients with USNHL. The literature reports that children with BCNC stenosis are generally considered poor candidates for cochlear implant surgery, and only a minority of children implanted with CND achieve good results. 24 Zhang et al. reported their experience with a series of patients with bilateral BCNC stenosis who underwent unilateral CI for hearing rehabilitation, finding that these patients under best aided condition generally derived significant benefit from unilateral CI with approximated results seen in CI performed in congenitally deaf peers without BCNC stenosis. 16 In this study, we are the first to compare the outcomes of unilateral CI for USNHL with and without BCNC stenosis.
Limitations
The study's sample size (n = 23) was determined by consecutive clinical availability rather than an a-priori power calculation; therefore, the null findings between BCNC-S and BCNC-N groups may reflect type-II error. The relatively short follow-up (24 months) and the heterogeneity of speech-processor programming strategies were not controlled for, potentially influencing stimulation-current comparisons. Additionally, the single-centre design and the absence of randomization limit generalizability and control for selection bias.
Conclusion
CI could improve the hearing and sound localization ability for USNHL patients with and without BCNC stenosis. USNHL due to BCNC stenosis could achieve approximated benefit from unilateral CI with congenitally deaf peers without BCNC stenosis.
Footnotes
Author contributions
XWC conceived the study and acted as head surgeon for the Cochlear performed in this study. XMF designed and conducted the study. XMF and TYY analyzed the data and draft the manuscript. FYZ, WG, RZG and YF participated in the literature search, data collection and data analysis. XWC obtained the funding. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant to Xiaowei Chen from the General Programs of the National Natural Science Foundation of China (Grant No. 81974143) and by a grant to Xinmiao Fan from the Beijing Natural Science Foundation (Grant No. 7244382).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.