
Abstract
Objective
This prospective study assessed the efficacy of the Cochlear™ Osia® 2 System compared to the previous Baha® Attract System in patients with mixed or conductive hearing loss (MHL/CHL).
Methods
In this prospective case-control study, 10 patients (2 men and 8 women) with MHL/CHL were implanted with the Osia® 2 System. Their audiological outcomes were compared with 13 patients (2 men and 11 women) who had previously been implanted with the transcutaneous Baha® Attract system. We compared the complications and compliance of the two groups. Also, in the Osia 2 System group, subjective satisfaction was assessed using the Korean version of the International Outcome Inventory for Hearing Aids (K-IOI-HA) questionnaire and the Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire.
Results
Complications such as poor magnetization, pain & infection, and abnormal noise were more common in the Baha Attract group, although not statistically significant. Also, the Osia 2 group exhibited better compliance. Subjective satisfaction was assessed using the K-IOI-HA and APHAB questionnaires with the Osia 2 group, revealing significantly improved scores in ease of communication, reverberation, background noise, and higher K-IOI-HA scores post-implantation. Postoperative-aided thresholds with both systems were significantly lower than preoperative-unaided thresholds, with the Osia 2 System demonstrating notably high satisfaction levels. Although both systems showed similar preoperative and postoperative word-recognition scores, the Osia 2 System provided greater audiological gain, especially at 2 kHz and 4 kHz frequencies. Additionally, the functional gain of both systems was comparable across all frequencies.
Conclusions
The Osia 2 System demonstrated high subjective satisfaction and improved audiological outcomes compared to the Baha Attract system in patients with conductive or mixed hearing loss. Its superior audiological gain, particularly at critical frequencies, along with better compliance, suggests it as a favorable option for this patient population.
Introduction
Conventional air conduction hearing aids (ACHAs), which we commonly use, are employed worldwide in moderate to severe hearing loss, and cochlear implants are used in severe to profound hearing loss. 1 Patients with moderate to severe hearing loss who do not benefit greatly from ACHAs or patients who cannot wear them for various reasons need to use implantable hearing devices, which are constantly under development, to meet their needs to improve their hearing and quality of life. 1 Bone conduction devices (BCDs) are instruments that convert sound into vibration through an osseointegrated implant in the skull, transmitting it directly to the cochlea without going through the external and middle ear. For this reason, BCDs are mainly applicable to patients with mixed or conductive hearing loss (MHL/CHL) and patients with single-sided deafness (SSD). 2 Compared to ACHAs, BCDs offer a distinct advantage in terms of speech recognition. Evidence suggests that patients with mixed hearing loss experience superior speech recognition with Baha devices compared to contemporary Behind-The-Ear (BTE) devices, particularly when the air–bone gap exceeds approximately 35 dB. 3 In addition, because an ear mold is not used and the device is attached to the temporal bone, it is useful in patients who cannot use ACHAs due to problems such as infection in the external or middle ear, or in patients with congenital ear deformities. 4
Baha® Attract (Cochlear™, Sydney, Australia) is a passive transcutaneous BCD that transmits sound waves across intact skin barriers to a passive implant magnet. In passive devices, hearing improvement is greatest in the low-frequency range. In the case of the Baha Attract, the performance gradually drops at frequencies above 3000 Hz due to soft tissue attenuation of external vibrations. 5 In currently available active BCDs since 2012, the sound processor (SP) remains outside of the body, but the vibrator itself is separated from the SP and located under the skin. With this design, a vibrator in direct contact with the skull generates vibrations transmitted through the skull to the cochlea. The Cochlear Osia® System (Cochlear™, Sydney, Australia) is a new active BCD system with transcutaneous connections between external processors and implants. The vibrator is piezoelectricity based and is fixed directly to a titanium screw integrated into the skull. In the Osia System, the surgically implanted titanium fixture (BI300) supports a piezoelectric actuator (OSI100), which includes a receiver simulator, receiving coil, and retention magnet under the skin.6,7
The Osia System is expected to show sufficient stability and effectiveness of the Baha Attract but also improved high-frequency hearing and better sound quality due to an active internal vibration system that can overcome soft tissue sound attenuation.5,8,9
Previous studies on the Osia System have shown good results in auditory evaluations and patient satisfaction surveys,6,7,10–13 especially regarding their auditory improvements over passive BCDs, such as Baha Attract, at high-frequency ranges.6,9 According to several previous studies, the new active transcutaneous Osia 2 System is expected to have many advantages over existing BCDs, but the number of subjects in these studies is still small. This study was designed to assess the subjective satisfaction with the Osia 2 System, evaluate the audiological improvements achieved with the Osia 2 System, and compare these audiological outcomes with those of the previous Baha Attract system in patients with MHL/CHL.
Materials and methods
Subjects
This study is a prospective study. However, for the control group, which consists of the Baha Attract implant cohort, data was collected retrospectively. The subjects of the Osia 2 implant study were Korean adults aged between 18 and 80 years with a history of middle ear surgery due to chronic otitis media, including cholesteatoma or congenital ossicular anomaly, who showed hearing improvement when using a Baha tester. The inclusion criteria of this study were (1) a bone conduction (BC) pure-tone average (PTA) of ≤55 dB hearing level (HL) and air–bone gap (ABG) of ≥25 dB HL in the operated ear, (2) maximum speech identification scores (PBmax) of ≥50% in the operated ear in speech audiometry, (3) a low expectation for hearing improvement through ossiculoplasty, and (4) an inability to obtain sufficient benefits from ACHAs or an inability to wear ACHAs due to changes in the shape of the ear canal or otorrhea. If a patient's anatomical structure was not suitable for the Osia 2 surgery, or if they did not consent to the procedure, they were excluded from surgery. To confirm the safety of the surgery, the postoperative complications were observed more than 6 months after surgery.
Surgical procedure
The Osia 2 implantation surgery was performed under local anesthesia, and the procedure is as follows. (1) The skin was marked using an OSI200 implant template to determine the incision site. (2) The skin thickness was measured and the retroauricular skin incision was made. (3) Using a guide drill and widening drill, a hole where the implant would be located was created, and the BI300 implant was inserted. (4) The internal implant (OSI2000) was fixed in place. (5) The subcutaneous tissue and skin were sutured. (6) A pressure dressing was applied for at least 24 h. After removing the compression dressing, a general therapeutic dressing may be used during the initial healing period. The Osia 2 SP device will be worn starting one-month post-surgery.14–17
Complications and compliance investigation
Six months following the implant surgery, we conducted an investigation into complications and compliance that arose post-surgery. We statistically compared all complications observed in both the Osia 2 implant group and the Baha Attract implant group, rather than focusing solely on a few specific issues. Additionally, we categorized patients’ compliance with device usage into four distinct groups:
“Full-used”: when the device was worn for more than 8 h, “Moderate-used”: when the device was worn for more than 2 h but less than 8 h, “Limited-used”: when the device was worn for less than 2 h, “No Use”: when the device was not used at all.
Questionnaires
The Korean version of the International Outcome Inventory for Hearing Aids (K-IOI-HA) questionnaire and the Korean translation of the Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire were utilized to evaluate the subjective impact and satisfaction associated with active BCHIs. All patients who received Osia 2 implants completed these questionnaires before surgery, at 3 months post-surgery, and at 6 months post-surgery.
The K-IOI-HA comprises a total of seven questions, utilizing a 5-point scale. A higher score indicates greater satisfaction with the hearing aid. An outcome measured by the K-IOI-HA is considered non-beneficial if the total score is ≤20 or if the mean score for the items is ≤2.9. Conversely, if the total score is ≥33 or if the mean item score is ≥4.7, the outcome indicates higher patient satisfaction. 18
The APHAB questionnaire consists of four detailed sections: ease of communication (EC), reverberation (RV), background noise (BN), and aversiveness (AV), totaling 24 questions. This questionnaire is widely utilized because it can predict the likelihood of success with a hearing aid before its use, compare different sound control capabilities of a hearing aid across various environments, and quantify the benefits of a hearing aid. With the APHAB, a lower score indicates reduced distress experienced by the patient. 19
Audiological assessment
The audiological assessment was conducted by a licensed audiologist in a soundproof audiometric booth using the AURICAL® Aud audiometer from Natus. For the sound audiometric examination, the non-implanted ear was masked using an ear plug and earmuff. Patients’ auditory function was assessed using pure-tone, speech, and sound field (SF) audiometry. Pure-tone audiometry was administered before the surgical procedure. For the group implanted with the Osia 2 device, SF audiometry, most comfortable loudness level (MCL), and word-recognition score (WRS) evaluations were performed preoperatively and at 1-, 3-, and 6-month intervals following surgery. In the cohort implanted with the Baha Attract device, these assessments were conducted preoperatively and at a follow-up period exceeding 6 months post-surgery.
Effective gain was calculated at each frequency of 0.25, 0.5, 1, 2, and 4 kHz as the disparity between the better bone conduction (BC) threshold of both ears and the air conduction (AC) threshold of SF audiometry in the implanted ear post-surgery. Functional gain was determined at each frequency of 0.25, 0.5, 1, 2, 4, and 8 kHz as the difference between the AC threshold of the implanted ear measured pre-surgery and the SF audiometry scores post-surgery. We assessed whether there was an auditory benefit at each frequency.
Statistical analysis
Statistical comparisons were conducted using Python 3.12.1 and GraphPad Prism 10.2.2. If the missing value was less than 10%, it was replaced with the mean if there was normality, or the median if there was no normality, and if it was more than 10%, it was removed. The normality of the data was tested using the Shapiro-Wilk test, and the equality of variances was tested using the Levene test. If the data showed normality, parametric methods such as paired t-test, independent t-test, repeated measures ANOVA, one-way ANOVA test with post hoc test, and chi-square test were used. In cases where normality was not shown or the parametric method could not be used due to reasons such as the ranking scale, the Wilcoxon signed-rank test, Mann-Whitney test, Friedman test, and Kruskal-Wallis test with the post hoc test were used. In addition, Fisher's exact tests were conducted on categorical data with a small number of samples. All statistics were expressed as mean ± standard deviations if normality was shown, median ± interquartile range if normality was not shown, and p-values < .05 were considered statistically significant.
Ethical considerations
This study follows the guidelines and principles of the Helsinki Declaration of 1975 as revised in 2013. All participating patients were provided written consent after a detailed explanation of the studies’ components and procedures in an independent space and were informed that they could revoke consent at any time they wanted. In accordance with ethical guidelines and to protect patient privacy, all patient details have been thoroughly de-identified before analysis. This study was approved by the Institutional Review Board (IRB) of Chonnam National University Hospital, South Korea, with the approval number CNUH 2022-033. (approved date: Feb. 14, 2022)
Results
Baseline characteristics of the subjects
As a prospective study, all surgeries were performed at Chonnam National University Hospital in South Korea, a single center, and were performed by one skilled ENT specialist (H. H. Cho). Ten patients (2 men and 8 women) with MHL/CHL underwent the Osia 2 implantation surgery from January 1, 2022, to December 31, 2022, and the follow-up period ranged from January 1, 2022, to June 31, 2023. Their ages ranged from 38 to 63 years old, with an average of 53.1 ± 7.4 years.
The Osia 2 group's audiological outcomes were compared with 13 patients (2 men and 11 women) who had previously been implanted with the transcutaneous Baha system (Baha® Attract). All patients who received Baha implantation were MHL/CHL, and the surgery was performed between September 2014 and January 2023. The patients’ ages ranged from 39 to 77 years, with a mean of 58.2 ± 12.0 years. There was no statistically significant age difference between the two groups (p = .262) (Table 1).
Patients’ demographics and characteristics.

Complications & compliance
In the Osia 2 implant group, poor magnetization was observed in 1 out of 10 patients (10.0%), whereas in the Baha Attract group, it was noted in 3 out of 13 patients (23.1%) (p = .604). Subsequently, within the Osia 2 group, no instances of pain, infection, or inflammation were reported during the 6-month outpatient follow-up. In contrast, in the Baha Attract group, 1 out of 13 patients (7.7%) experienced pain accompanied by inflammation. Additionally, 1 out of 10 individuals (10.0%) in the Osia 2 group reported difficulties wearing the device due to abnormal noise, while in the Baha Attract group, 3 out of 13 individuals (23.1%) faced challenges in wearing the device due to noise-related issues (p = .604). Abnormal noise refers to instances where wind noise is amplified or the sound of hair brushing against the implant is unpleasant. In such cases, we either reduced the high-frequency gain or advised the patient to gradually adapt to the sound.
Lastly, compliance with device usage was compared between the two groups. In the Osia 2 group, 6 out of 10 patients (60.0%) fell into the ‘Full-used’ category, and 4 out of 10 patients (40%) were classified under “Moderate-used.” In contrast, in the Baha Attract group, 12 out of 13 patients (92.3%) were “Moderate-used,” while only 1 out of 13 patients (7.7%) did not use the device at all. A statistically significant difference in compliance was observed between the two groups (p = .002) (Figure 1).
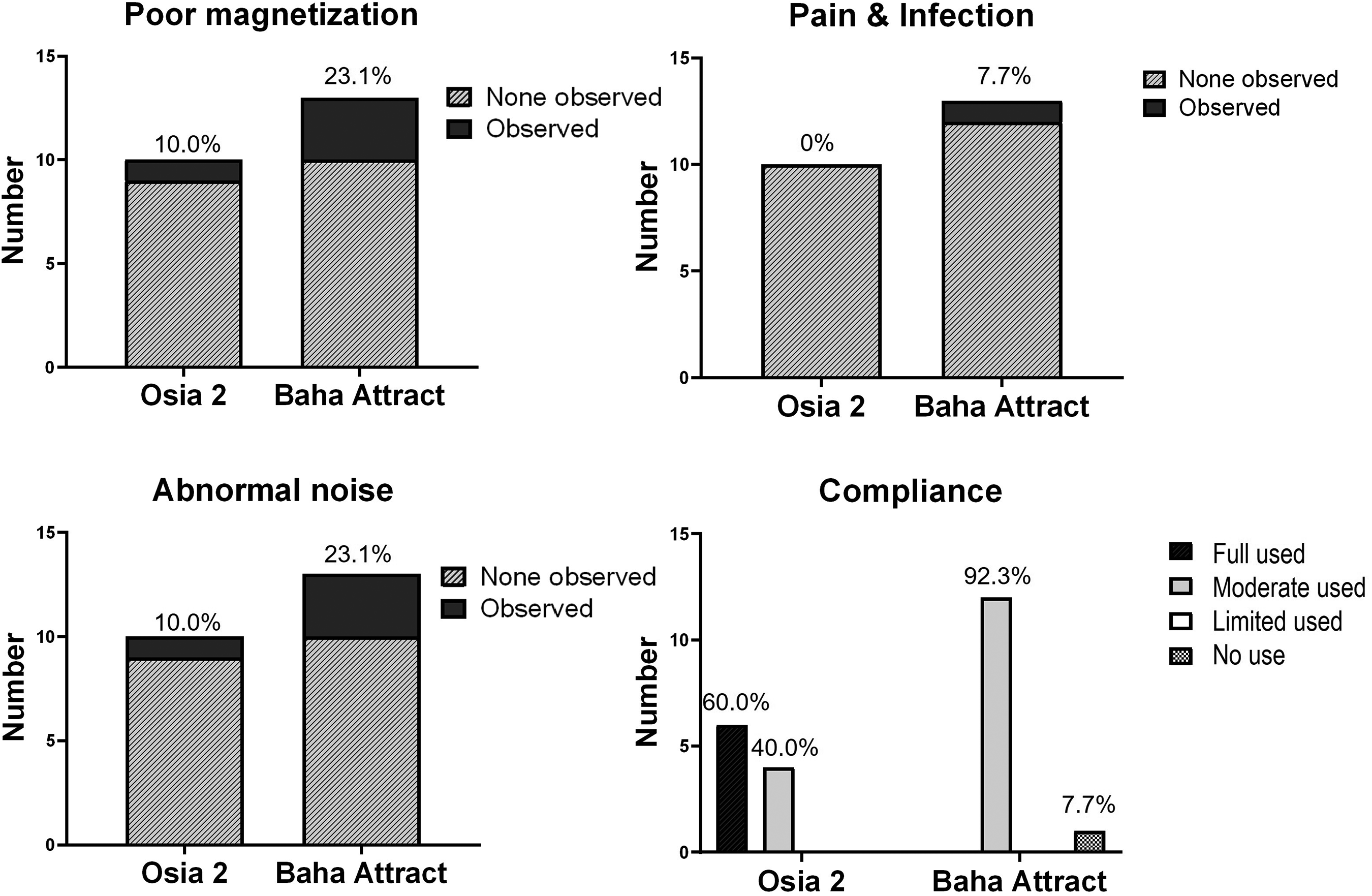
Comparison of the number of complications and compliance between the Osia 2 implantation group and the Baha Attract implantation group. There was no statistically significant difference in poor magnetization, pain & infection, and abnormal noise between the two groups (p = .604, p = 1.000, p = .604). However, there was a statistically significant difference in compliance between the two groups (p = .002).
Questionnaires
In the K-IOI-HA questionnaire, with the hearing aid in use, the average preoperative score for patients with the Osia 2 implant was 20.7 ± 7.7. When using the Osia 2, the average score at 3 months post-surgery was 29.0 ± 4.4, and at 6 months post-surgery, it was 28.7 ± 4.7. Upon comparison across the three time points using post hoc analysis, a significant difference was found between the preoperative score and the score at 3 months, as well as between the preoperative score and the score at 6 months (p = .016, p = .039). However, there was no statistically significant difference between the 3-month postoperative group and the 6-month postoperative group (p = 1.000, Figure 2).
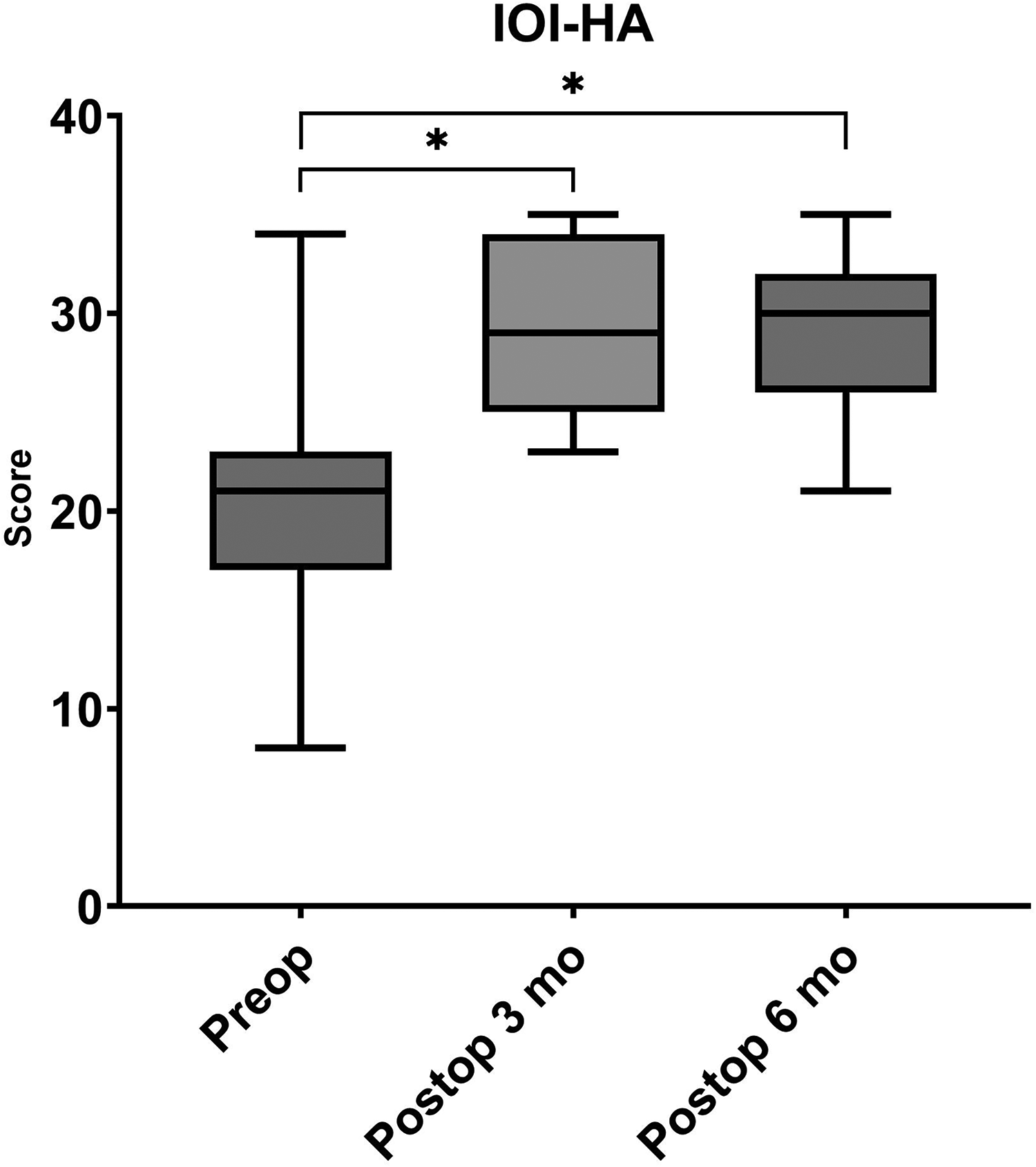
Scores from the Korean version of the International Outcome Inventory for Hearing Aids questionnaire (K-IOI-HA). The bar graph illustrates the mean scores of the preoperative (Preop) period with the hearing aid, as well as the scores at 3 months postoperative (Postop 3 mo) and 6 months postoperative (Postop 6 mo) when using the Osia 2. Statistical comparisons were conducted among these time points. The scores exhibited a statistically significant increase in both the 3-month and 6-month postoperative groups compared to the Preop group.
In the APHAB questionnaire, with the hearing aid in use, the preoperative average score for the ease of communication (EC) questions among Osia 2 patients was 70.7 ± 28.2. When using the Osia 2, the average score at 3 months post-surgery was 14.7 ± 15.4, and at 6 months post-surgery, it was 16.2 ± 15.0. When comparing across the three time points, a statistically significant difference was observed (F = 12.7, p < .001). During post hoc analysis, significant differences were found between the preoperative score and the score at 3 months, as well as between the preoperative score and the score at 6 months (p = .007, p = .016). However, there was no statistically significant difference between the 3-month postoperative group and the 6-month postoperative group (p = 1.000).
With the hearing aid in use, the preoperative average score for the reverberation (RV) questions was 61.8 ± 27.0. When using the Osia 2, the average score at 3 months post-surgery was 21.3 ± 19.5, and at 6 months post-surgery, it was 26.5 ± 17.6. When comparing across the three time points, a statistically significant difference was observed (F = 12.6, p < .001). During post hoc analysis, significant differences were found between the preoperative score and the score at 3 months, as well as between the preoperative score and the score at 6 months (p = .002, p = .022). However, there was no statistically significant difference between the 3-month postoperative group and the 6-month postoperative group (p = 1.000).
With the hearing aid in use, the preoperative average score for the background noise (BN) questions was 73.2 ± 28.5. When using the Osia 2, the average scores at 3 months and 6 months post-surgery were 22.0 ± 16.3 and 27.7 ± 13.4, respectively. When comparing across the three time points, a statistically significant difference was observed (F = 16.8, p < .001). During post hoc analysis, significant differences were found between the preoperative score and the score at 3 months, as well as between the preoperative score and the score at 6 months (p < .001, p = .022). However, there was no statistically significant difference between the 3-month postoperative group and the 6-month postoperative group (p = .539).
For the aversiveness (AV) questions, the preoperative average was 28.3 ± 31.8, and the scores 3 months and 6 months after surgery were 42.4 ± 32.9 and 44.7 ± 27.0, respectively. There was no statistically significant difference in the average AV scores of the three time points (F = 2.84, p = .283) (Figure 3).

Scores from the four categories of the Korean translation of the Abbreviated Profile of Hearing Aid Benefit questionnaire (APHAB). The bar graph illustrates the mean scores across the preoperative (Preop) period with the hearing aid, and at 3 months postoperative (Postop 3 mo) and 6 months postoperative (Postop 6 mo) when using the Osia 2. Statistical comparisons were made across four categories: ease of communication subscale (EC), reverberation subscale (RV), background noise subscale (BN), and aversiveness subscale (AV). The scores in the EC, RV, and BN categories were statistically significantly lower in both the 3-month and 6-month postoperative groups compared to the Preop group. However, this difference was not statistically significant in the AV category.
Audiological tests
In the Osia 2 group, the mean AC thresholds (average of 0.5, 1, 2, and 4 kHz) of the patients before implantation were 67.4 ± 17.2 dB, and the mean thresholds in SF audiometry at 1, 3, and 6 months post-surgery were 34.2 ± 15.6 dB, 34.8 ± 15.6 dB, and 34.3 ± 15.3 dB, respectively, while the mean best ear BC thresholds of the patients before Osia 2 implantation were 32.4 ± 13.1 dB (Supplementary Table 1).
When comparing the preoperative-unaided PTA AC threshold with the aided SF audiometry results at 6 months postoperatively in the implanted ear of the Osia 2 implant group, statistically significant improvements were observed in all tested frequencies (Figure 4(a))

Comparison of the preoperative air conduction thresholds and postoperative sound field audiometry results. (A) For the Osia 2 implant group, the 6-month postoperative thresholds were significantly different from the preoperative thresholds at the following frequencies: 0.25 kHz (p < .001), 0.5 kHz (p < .001), 1 kHz (p < .001), 2 kHz (p < .001), 4 kHz (p < .001), and 8 kHz (p = .037). (B) In the Baha Attract group, the 6-month postoperative thresholds showed significant differences compared to the preoperative thresholds at 0.25 kHz (p < .001), 0.5 kHz (p < .001), 1 kHz (p < .001), 2 kHz (p < .001), and 4 kHz (p = .020).
In the Baha Attract group, the mean AC thresholds (average of 0.5, 1, 2, and 4 kHz) before implantation were 76.7 ± 16.8 dB. Six months post-surgery, the mean thresholds in SF audiometry were 41.8 ± 18.6 dB, while the mean best ear BC thresholds of the patients before Baha Attract implantation were 27.7 ± 22.1 dB (Supplementary Table 1). When comparing the preoperative-unaided AC threshold with the aided SF audiometry results at 6 months postoperatively in the implanted ear of the Baha Attract group, statistically significant improvements were observed in hearing across all frequencies except at 8 kHz (Figure 4(b)).
The MCL in the implanted ear of the Osia 2 implant group was recorded as 66.9 ± 6.5 dB during preoperative SF audiometry. This decreased to 60.0 ± 3.5 dB at 1 month postoperatively, further to 58.5 ± 5.8 dB at 3 months postoperatively, and remained stable at 58.0 ± 3.5 dB at 6 months postoperatively. A statistically significant difference was observed between the preoperative MCL and the MCL measured at 1, 3, and 6 months postoperatively (F = 12.2, p = .007). Moreover, significant differences were identified when comparing the MCL values preoperatively to those at 1 month (p = .023), 3 months (p = .017), and 6 months (p = .005) postoperatively, as evidenced by post hoc analysis (Figure 5(a)).

The assessment of most comfortable loudness levels (MCLs) and word-recognition scores (WRSs) in the Osia 2 implant groups. (A) In the Osia 2 implant group, a statistically significant disparity was observed between the preoperative (Preop) MCL and the MCLs recorded at 1 month (Postop 1 mo), 3 months (Postop 3 mo), and 6 months (Postop 6 mo) postoperatively. (B) There were no statistically significant differences observed when comparing the WRSs across the specified time intervals.
In the Osia 2 implant group, the WRS in the implanted ear was measured as 87.0 ± 22.6% during preoperative SF audiometry. This score slightly improved to 92.4 ± 15.7% at 1 month postoperatively, further increased to 94.0 ± 13.6% at 3 months postoperatively, and reached 94.4 ± 10.2% at 6 months postoperatively. However, there was no statistically significant difference observed between the preoperative WRS and the scores at 1, 3, and 6 months after surgery (F = 2.31, p = .510) (Figure 5(b)).
The effective gains in hearing abilities six months post-surgery were compared between the Osia 2 implant group and the Baha Attract implant group across various test frequencies (Figure 6(a)). The Osia 2 group exhibited effective gains of −12.0 ± 16.0 dB at 0.25 kHz, 0.5 ± 14.2 dB at 0.5 kHz, 0.5 ± 8.6 dB at 1 kHz, 9.0 ± 7.4 dB at 2 kHz, and −12.0 ± 15.7 dB at 4 kHz, with an average effective gain (at 0.5, 1, 2, and 4 kHz) of −0.5 ± 13.6 dB HL. In contrast, the Baha Attract group showed effective gains of −18.5 ± 18.1 dB at 0.25 kHz, −12.3 ± 22.6 dB at 0.5 kHz, −6.2 ± 15.7 dB at 1 kHz, −10.8 ± 11.0 dB at 2 kHz, and −27.3 ± 16.9 dB at 4 kHz, with an average effective gain (at 0.5, 1, 2, and 4 kHz) of −14.1 ± 18.2 dB HL. Overall, the Osia 2 group demonstrated superior effective gains. Statistically, the effective gain of the Osia 2 group was significantly higher than that of the Baha Attract group at 2 kHz (p < .001) and 4 kHz (p = .038). However, there were no significant differences observed at the frequencies of 0.25 kHz (p = .383), 0.5 kHz (p = .133), and 1 kHz (p = .242).

A comparative analysis of effective and functional gains in patients’ hearing abilities six months post-surgery between the Osia 2 implant group and the Baha Attract implant group across various test frequencies. (A) The effective gains in the Osia 2 group were superior to those in the Baha Attract group across all frequencies. Specifically, statistically significant improvements were observed at 2 kHz (p < .001) and 4 kHz (p = .038). (B) In terms of functional gains, both groups exhibited improvements in hearing. However, no significant differences were observed between the two groups at any of the tested frequencies: 0.25 kHz (p = .616), 0.5 kHz (p = .273), 1 kHz (p = .321), 2 kHz (p = 1.000), 4 kHz (p = .403), and 8 kHz (p = .421).
The functional gains in hearing abilities six months post-surgery were compared between the Osia 2 implant group and the Baha Attract implant group across different test frequencies (Figure 6(b)). The Osia 2 group demonstrated functional gains of 35.5 ± 19.6 dB at 0.25 kHz, 36.5 ± 15.5 dB at 0.5 kHz, 44.5 ± 13.8 dB at 1 kHz, 31.5 ± 13.8 dB at 2 kHz, 20.0 ± 16.3 dB at 4 kHz, and 17.8 ± 24.6 dB at 8 kHz, with an average functional gain (at 0.5, 1, 2, and 4 kHz) of 33.1 ± 16.7 dB HL. In comparison, the Baha Attract group showed functional gains of 39.2 ± 15.5 dB at 0.25 kHz, 43.8 ± 15.6 dB at 0.5 kHz, 50.8 ± 15.3 dB at 1 kHz, 31.5 ± 18.0 dB at 2 kHz, 13.5 ± 19.5 dB at 4 kHz, and 10.0 ± 21.0 dB at 8 kHz, with an average functional gain (at 0.5, 1, 2, and 4 kHz) of 34.9 ± 21.7 dB HL. No significant differences were observed between the two groups at any of the tested frequencies: 0.25 kHz (p = .616), 0.5 kHz (p = .273), 1 kHz (p = .321), 2 kHz (p = 1.000), 4 kHz (p = .403), and 8 kHz (p = .421).
Discussion
This study aimed to evaluate the satisfaction, effectiveness, and safety of the active transcutaneous BCD Osia 2 System in patients with MHL/CHL. Subjective satisfaction post-surgery was assessed using the K-IOI-HA and APHAB questionnaires. The results indicated a significant improvement in subjective satisfaction as evidenced by the K-IOI-HA scores and the EC, RV, and BN categories of the APHAB. Additionally, patients experienced noticeable auditory benefits. The effective gains in patients were statistically significantly higher at 2 kHz and 4 kHz compared to the Baha Attract, demonstrating objective auditory benefits. In a 2017 study by Hougaard et al., 20 following Baha Attract implantation, 7 out of 23 patients experienced a non-beneficial outcome, with 3 being non-users and 4 being non-benefiting users. In contrast, in our study among all patients who received BCD, only one patient with the Baha Attract implant was classified as a non-user. Most patients effectively utilized BCDs and benefited from it. Specifically, the group of patients who used the Osia 2 demonstrated better compliance compared to those using the Baha Attract.
In our study, a comparison of preoperative AC and postoperative 6-month SF audiometry results revealed that Osia 2 implants exhibited objective auditory benefits at frequencies of 0.25 kHz, 0.5 kHz, 1 kHz, 2 kHz, and 4 kHz. Similarly, the Baha Attract demonstrated significant postoperative threshold improvements at the same frequencies, indicating comparable objective auditory benefits. While the Osia 2 implants displayed enhanced MCLs following surgery, no significant difference was observed in WRSs.
A market release analysis of the Cochlear™ Osia® 2 System by Goldstein et al. 7 in 2020 reported favorable outcomes in both WRS and PB max. In 2021, Marszal et al. 13 compared the mean values of 0.5 kHz, 1 kHz, 2 kHz, and 4 kHz in pure-tone audiometry (PTA4) before and after Osia 1 implant surgery, revealing a significant benefit. Furthermore, the Osia 1 was found to have a notable advantage over the Baha® 5 Power Processor on the Softband, particularly evident at 6 kHz. Speech audiometry results also indicated significant auditory benefits in both quiet and noisy environments. 13 In our study, the Osia 2 System demonstrated superior effective gains at high frequencies compared to the Baha Attract system, aligning with previous research findings.
By contrast, a review of 11 studies examining hearing outcomes after the implantation of the active bone conduction device, Bonebridge, in patients with MHL/CHL demonstrated a functional gain ranging from 24 to 37 dB. 21 In our study, a functional gain of 33.1 ± 16.7 dB HL was observed, indicating a similar level of improvement. Also, Canzi et al. 22 reported a mean pure-tone effective gain of −12.25 dB HL following Bonebridge implantation, and this result is comparable to our findings, where the mean effective gain after Osia 2 implantation was −14.1 ± 18.2 dB HL.
In a separate study by Goycoolea et al. 6 in 2020, speech recognition in both quiet and noisy settings was statistically significantly higher in patients utilizing the Osia 1 System compared to those using the Baha Attract on a Softband. However, it is noteworthy that in both the studies of Marszal et al. 13 and M. Goycoolea et al., 6 the Baha Attract was not surgically implanted but was instead utilized on a Softband. Therefore, further follow-up studies are imperative for a comprehensive understanding.
In a study conducted by Rauch et al. 10 in 2022, the upgrade from the Osia 1 to the Osia 2 sound processor (SP) did not demonstrate objective auditory benefits over the Osia 1. However, the Osia 2 SP offered enhanced technical functionalities. When considering surgical auditory rehabilitation, factors such as ease of use and appearance hold significant importance for patients.
The Osia 2 sound processor stands out due to its lightweight design compared to older devices. It weighs merely 9.4 g, in contrast to 10.3 g for the Baha 4 and 15.6 g for the Baha 5 Power. Unlike percutaneous BCDs, the Osia System utilizes a magnetic connection to the internal device, eliminating the need for lifelong care of the implant and offering improved esthetics. While passive BCDs like the Baha Attract necessitate a robust magnetic connection for effective vibration transfer, the sound processor in the Osia System does not vibrate. Consequently, it typically does not require a strong magnetic connection for sound transfer. This feature enhances patient comfort during prolonged use of the Osia System. 7
In our study, while there was no significant difference in functional gain between the Osia 2 and Baha Attract implants among patients with MHL/CHL, the effective gain of the Osia 2 System was notably higher at 2 kHz and 4 kHz. In the context of patients with MHL/CHL, effective gain is regarded as a superior parameter to functional gain when evaluating objective auditory gain. This preference stems from the understanding that the auditory benefit of BCDs correlates with the BC threshold hearing level of the better ear.23,24
A 2023 study by Kim et al. 9 examined 17 patients with Osia 2 System implants, comprising 9 MHL/CHL patients and 8 SSD patients. Among the CHL/MHL patients using the Osia 2 System, the effective gain was significantly higher at 2 kHz compared to those utilizing the Baha Attract or Bonebridge (MED-EL, Innsbruck, Austria) systems. In SSD patients, those equipped with the Osia 2 System exhibited a notably higher functional gain at 4 kHz than those with the Baha Attract or Bonebridge systems. 9 The reason for the different results in this study is believed to be due to the inclusion of the active BCD system, the Bonebridge, in the control group. This may have partially offset the skin attenuation effect of the Baha Attract system's sound processor.
Within our study, among MHL/CHL patients, the effective gain was consistently higher in the Osia 2 implant group across all frequencies. Moreover, the gains at 2 kHz and 4 kHz were statistically significantly superior. The heightened gain in high frequencies, observed in several prior studies, may be attributed to factors such as the absence of skin attenuation or damping typically found in passive BCDs, optimal positioning of the osseointegration point, or the use of a piezoelectric transducer.6,25 Furthermore, the common feedback issues associated with traditional Baha devices have been markedly reduced with the Osia System, potentially contributing to its relative advantages. 7
According to prior research, active transcutaneous BCDs present complications that are comparable to those of passive transcutaneous BCDs but exhibit fewer and less severe issues than percutaneous BCDs. 26 Previous studies have indicated a minimal risk of complications among patients.7,17 Active transcutaneous BCDs represent a relatively novel technology compared to passive transcutaneous BCDs Consequently, a comprehensive understanding of their potential complications and device malfunctions is still evolving.
In our study, six months post-implantation, 10% of patients (1 out of 10) in the Osia 2 group reported issues with poor magnetization, while an equal percentage reported symptoms of abnormal noise. No other discomforts were reported by this group. When assessing postoperative complications, there was no statistically significant difference observed between the two implant devices.
However, upon comparing the Osia 2 implant group with the Baha Attract implant group, the percentages were as follows: 10.0% vs. 23.1% for “Poor magnetization,” 0.0% vs. 7.7% for “Pain & Infection,” and 10.0% vs. 23.1% for “Abnormal noise.” With an increase in the study's sample size, there is a potential for these differences to reach statistical significance.
Furthermore, compliance was notably higher in the Osia 2 implant group. This variance in compliance could potentially be attributed to the passive nature of the Baha Attract device. Given that the sound generator in the Baha Attract is situated outside the skin, it may be more susceptible to disturbances from the surrounding hair rubbing against it and wind noise. Additionally, the Baha Attract's heavier weight compared to the Osia 2 may contribute to magnet detachment, necessitating a tighter skin attachment, which can result in discomfort.
This study possesses several limitations that warrant consideration. First, due to the limited number of patients in the Osia 2 and Baha Attract implant groups, non-parametric tests were employed in cases where data did not exhibit normal distribution. Such an approach may not robustly capture all potential effects. Second, given that the device was recently introduced in South Korea, the outpatient follow-up period post-surgery was confined to six months. A longer-term observational study spanning several years is essential to comprehensively evaluate the efficacy of hearing implants. Third, the statistical analysis compared the Osia 2 implant group, which collected data prospectively, to the Baha Attract implant group, which gathered data retrospectively. This could introduce several biases into the results.
Despite these limitations, this study holds significance in demonstrating that the effective gain at the frequencies critical for human conversation (2 kHz and 4 kHz) was superior with the Osia 2 implant compared to the established Baha Attract implant for MHL/CHL patients. Additionally, the issue of patient discomfort leading to non-use of hearing aids is prevalent. In this context, it is noteworthy that compliance was statistically significantly higher with the Osia 2, an active transcutaneous BCD, than with the Baha Attract, an existing passive transcutaneous BCD.
Conclusion
The findings of this study suggest that the Osia 2 System offers enhanced patient satisfaction and superior audiological outcomes for individuals with CHL/MHL compared to the Baha Attract device. Specifically, the Osia 2 System demonstrated greater audiological gain (effective gain) and exhibited higher compliance, particularly at the critical frequencies of 2 kHz and 4 kHz. Consequently, the Osia 2 System may be regarded as a favorable option for patients presenting with MHL/CHL.
Supplemental Material
sj-docx-2-sci-10.1177_00368504241280252 - Supplemental material for The impact of the Cochlear™ Osia® 2 System on patients with mixed or conductive hearing loss: A comparison with Cochlear™ Baha® Attract System outcomes
Supplemental material, sj-docx-2-sci-10.1177_00368504241280252 for The impact of the Cochlear™ Osia® 2 System on patients with mixed or conductive hearing loss: A comparison with Cochlear™ Baha® Attract System outcomes by Kyeong-Suk Park, Hong-Chan Kim, Sungsu Lee and Hyong-Ho Cho in Science Progress
Supplemental Material
sj-docx-4-sci-10.1177_00368504241280252 - Supplemental material for The impact of the Cochlear™ Osia® 2 System on patients with mixed or conductive hearing loss: A comparison with Cochlear™ Baha® Attract System outcomes
Supplemental material, sj-docx-4-sci-10.1177_00368504241280252 for The impact of the Cochlear™ Osia® 2 System on patients with mixed or conductive hearing loss: A comparison with Cochlear™ Baha® Attract System outcomes by Kyeong-Suk Park, Hong-Chan Kim, Sungsu Lee and Hyong-Ho Cho in Science Progress
Footnotes
Author contributions
KSP gathered the data, performed statistics, and then wrote the initial draft of the paper. HCK also performed data acquisition, manuscript writing, and editing. SL helped data curation and revised the data analysis and manuscript. HHC conceived the study design and goals, oversaw data collection, completed preparing the manuscript, and managed the team working.
Data availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. The shared data of this study can be obtained by emailing the corresponding authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (HR20C0021) and Chonnam National University Hospital Biomedical Research Institute grant (No. BCRI24083).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.