
Abstract
Objective
Acute lower limb ischemia (ALI) is closely linked to conditions like diabetes mellitus and peripheral arterial disease, as well as the presence of polyvascular disease (PVD). The present retrospective observational study aimed to evaluate the impact of PVD on perioperative outcomes in patients with ALI.
Methods
Among 161 consecutive patients, these were categorized into subgroups based on their PVD status: control (N = 81), PVD1 (single arterial bed involvement) (N = 62), and PVD2 (coronary and cerebrovascular) (N = 18). Descriptive statistics and univariate analysis were performed.
Results
The mean age was 71.17 ± 11.6. Higher prevalences of diabetes mellitus (n = 21, 33.9% in PVD1; n = 8, 44.4% in PVD2) and hypertension (n = 55, 88.7% in PVD1; n = 16, 88.9% in PVD2) were reported for the PVD groups, when comparing to controls, who registered 13 (16.0%) and 41 (50.6%) individuals, respectively. Anticoagulant therapy and acute myocardial infarction were more common in the PVD1 and PVD2 groups (p = 0.005 and p = 0.001). Non-cardiovascular mortality rates were significantly higher in the PVD groups, with 24.2% in PVD1 and 33.3% in PVD2 compared to 11.1% in the control group (p = 0.033).
Conclusions
The study concluded that PVD significantly impacts the status of ALI patients, emphasizing the need for tailored, multidisciplinary care.
Keywords
Introduction
Acute lower limb ischemia (ALI) has been inherently associated with the prevalence of conditions such as diabetes mellitus and peripheral arterial disease (PAD). Diabetes mellitus has been shown to be present in at least 49.1% of patients diagnosed with ALI. 1 Overall, ALI patients’ prognosis underlies a significant risk of combined death and amputation, with recent data reporting a 15–20% risk at 30 days, escalating to a 50–60% risk at the 1-year mark. 2
One of the most important prognostic factors is the presence of multivessel disease, which can be defined as the presence of significant atherosclerosis in peripheral and/or coronary arteries, this way becoming an excellent indicator for systemic vascular health and reflecting not only on the presence of widespread atherosclerosis as well as the compromise of the overall cardiovascular function.3,4
According to the current epidemiological data, the prevalence of higher rates of ALI is especially correlated with elderly populations and those affected by comorbidities such as multivessel disease. In a study conducted in Japan, regarding 531 patients diagnosed with ALI, its incidence significantly increased with the aging of patients, as only 19.2% of individuals being under 65 years of age, while 27.9% were aged over 80 years. 5 Additionally, another study, conducted in the context of EUCLID, the Examining Use of Ticagrelor in Peripheral Artery Disease, analyzed 13,885 individuals with PAD, reporting 232 (1.7%) to have been hospitalized in the context of ALI, stating this condition to be associated with limb morbidity. 6 Such conditions end up compromising not only the normal function of the circulatory system and the viability of these patient's limbs, as well as their day-to-day activities and overall quality of life. 7
The aim of this study is to assess the impact of multivessel disease on perioperative outcomes in patients with ALI, specifically analyzing its influence on perioperative mortality, complication rates, and immediate postoperative recovery.
Methods
Study design and participants
This is a retrospective observational study involving consecutive patients with ALI admitted to the Department of Vascular Surgery from a tertiary referral hospital in Warsaw, Poland between January 2014 and November 2018. The respective flow diagram of this study is contemplated in Figure 1.

Study’s population selection flow diagram.
A complete medical history, including information on prior treatment, was obtained from all participants and medical documentation. The diagnosis of ALI was based on established criteria: sudden onset of the symptoms in the prior 2 weeks, presence of rest pain, sensory and mobility alteration, and other symptoms of ALI. Computed tomography angiography was performed to aid in complex revascularization planning and to resolve diagnostic uncertainties, providing detailed imaging data of each patient's vascular impairment and its impact on the affected area of ischemia. After surgery, all patients underwent a duplex ultrasound, accompanied by either a cardiologist, neurologist, or a specialized internist to evaluate multivessel disease status, assess atherosclerosis, and determine the effectiveness of the procedure.
Polyvascular disease (PVD) is considered the presence of atherosclerotic disease in two or more arterial beds. 8 The patients were divided into three different groups. The first group, serving as the control group, consisted of patients with no known atherosclerotic lesions. The second group included patients with ALI and a diagnosis of one condition among cerebrovascular disease (CVD) and coronary artery disease (CAD) (polyvascular disease 1, PVD1). The third group comprised of patients with ALI and both CVD and CAD (polyvascular disease 2, PVD2).
The present work follows the Strengthening the Reporting of Cohort Studies in Surgery Criteria (STROCCS) and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.9,10 The study protocol respects the Helsinki Declaration, as revised in 2024, and is under the European Union General Data Protection Regulation. All patients’ details have been de-identified. The study was approved by the Medical University of Warsaw Bioethics Committee (no. 111/2020). The university Ethics Committee waived the requirement of obtaining informed consent from the patients.
Surgical treatment
All patients underwent surgical treatment using open, endovascular, or hybrid methods, or underwent primary amputation. The treatment approach for ALI was determined based on the underlying cause (embolism or acute thrombosis) and the Rutherford classification of ischemia, guiding the use of direct thrombolysis, mechanical thrombectomy, or embolectomy. Revascularization was not performed in the case of Rutherford grade III, advanced limb ischemia/necrosis. In patients with major comorbidities who experienced significant improvement in their clinical condition following conservative treatment, surgical intervention was postponed to allow for elective preparation. Peripheral circulation played a critical role in determining the treatment approach. Due to the lack of peripheral blood flow in most patients, direct catheter thrombolysis (DCT) was implemented. Restoring peripheral blood flow was an introduction to other procedures, depending on the clinical status of said impaired lower limb in each specific patient. Treatment was discontinued if adequate circulation was achieved.
In most cases, limb open embolectomy or thrombectomy was performed under epidural or spinal anesthesia. For patients in whom these types of anesthesia were contraindicated, local anesthesia combined with sedation was used. Clots were removed using Fogarty catheter, both proximally and distally, until acceptable inflow and outflow were achieved. An additional endarterectomy was performed in massive atherosclerotic plaques were present at the site of the arterial incision. The arteriotomy was closed with either a primary suture or patch angioplasty in case of a small arterial diameter. Patients without adequate inflow or outflow were considered eligible for bypass surgery. Fasciotomy was performed in cases of suspected subfascial edema.
Endovascular treatment
DCT and mechanical thrombectomy were the first-choice endovascular methods for treating acute ischemia in all areas. 11 Access was obtained via the common femoral or left radial artery. During DCT infusion, Alteplase (Actilyse-Boehringer-Ingelheim®, Ingelheim am Rhein, Germany) was administered at 1 mg/hour, preceded by a 5 mg bolus. Unfractionated heparin (UFH) was simultaneously administered through the sheath at a rate of 500 IU/hour. Fibrinogen and activated partial thromboplastin time (APTT) levels were monitored four times daily. DCT was discontinued early if the fibrinogen level dropped below 150 mg/dL. 12 Control arteriography was performed before sheath removal.
For mechanical thrombectomy, the AngioJet® (Boston Scientific, Marlborough, MA, USA) and Rotarex® (Straub Medical, Wangs, Switzerland) systems were used, with catheter diameters selected based on the size of the artery. If the procedure was deemed insufficient, DCT or PTA/stenting was performed as needed. The Spider embolic protection system (Medtronic, Minneapolis, MN, USA) was employed in some lower limb arterial procedures.
Postoperatively, UFH was administered intravenously via infusion pump, targeting an APTT prolongation of 2.5–3 times the normal range.
Statistical analysis
The sample size for a survival test was calculated using online Sample Size Calculators for Designing Clinical Research (https://sample-size.net/sample-size-survival-analysis/), with a statistical power (β) of 80% and a significance level of 0.05. The sample was estimated (131) for a hazard ratio >2 between groups and a predicted survival at the end of follow-up of 80%, although higher event rate differences are described. 4 Although bigger event rate disparities are stated, the sample was calculated at 147, with a hazard ratio of 1.6 (1.3 to 1.9) across groups.4,13 A total estimated sample of 154 was collected with an expected loss-to-follow-up rate of 5%.
For statistical analysis, SPSS (IBM Corp., released 2023. IBM SPSS Statistics for Windows, version 29.0, Armonk, NY, USA) was used.
Categorical data are expressed as numbers of patients and percentages. The chi-square test or Fisher's exact test were used to compare proportions. Numeric variables were presented as medians and quartiles and compared using mainly analysis of variance and Kruskal–Wallis H test when their distribution was not normal. In the context of survival analysis, the endpoint was defined as all-cause mortality.
Survival analysis was assessed using the Kaplan–Meyer estimator and lifetable method. Perioperative deaths were removed. Log-rank estimator was applied to compare time-dependent variables. Stratified analysis was conducted for PVD1 and PVD2 patients. Statistical tests were two-tailed, and p-values <0.05 were considered significant.
Results
This study has included a total of 161 participants, divided into three groups based on their vascular disease status: control (N = 81), PVD1 (N = 62), and PVD2 (N = 18). The median follow-up period was 47 months (95% confidence interval (CI): 42.9–51.1). The mean age of participants differed significantly between the groups: 68.78 years (±11.713) in the control group, 74.10 years (±11.206) in the PVD1 group, and 71.83 years (±10.629) in the PVD2 group (p = 0.03) (Table 1).
Populations’ characteristics and demographics.

AF: atrial fibrillation; CABG: coronary artery bypass grafting; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease; CKD: glomerular filtration rate <60 mL/min; PAD: peripheral artery disease; PCI: percutaneous coronary intervention; PVD: polyvascular disease; SD: standard deviation.
aCollinearity.
The prevalence of diabetes mellitus was significantly higher in the PVD1 (N = 21, 33.9%) and PVD2 (N = 8, 44.4%) groups compared to the control group (N = 13, 16.0%, p = 0.009). Similarly, hypertension was significantly more prevalent in the PVD1 (N = 55, 88.7%) and PVD2 (N = 16, 88.9%) groups compared to the control group (N = 41, 50.6%, p < 0.001).
The prevalence of atrial fibrillation (AF) was N = 19 (23.5%) in the control group, N = 22 (35.5%) in the PVD1 group, and N = 9 (50.0%) in the PVD2 group (p = 0.056). Regarding the presence of emboli, it was recorded in N = 29 (35.8%) of the control group, N = 30 (48.4%) of the PVD1 group, and N = 9 (50.05%) of the PVD2 group (p = 0.249), indicating that embolism did not have statistical significance in this study.
Anticoagulation status varied significantly: 12 (19.7%) of PVD1 and 7 (38.9%) of PVD2 patients were on anticoagulant therapy, compared to 7 (8.6%) in the control group (p = 0.05). Notably, within the PVD2 group, two patients (11.1%) with recorded embolism were not anticoagulated, and an additional two patients (11.1%) with AF had not yet initiated anticoagulant therapy.
The surgical interventions performed according to the PVD status (Table 2) indicate that the majority of participants in all groups underwent embolectomy or thrombectomy, with N = 57 (70.4%) in the control group, N = 48 (77.4%) in PVD1, and N = 12 (66.7%) in PVD2, showing no significant statistical differences (p = 0.536). Mechanical thrombectomy was performed in N = 8 (9.9%) of patients in the control group, N = 7 (11.3%) in PVD1, and N = 4 (22.2%) in PVD2, but this also did not reach statistical significance (p = 0.336). Primary amputation occurring in only two patients from the control group (2.5%, p = 0.368).
Surgical interventions according to polyvascular disease status.

DCT: direct catheter thrombolysis; PVD: polyvascular disease.
In the surgical management of ALI based on etiology, direct embolectomy/thrombectomy was the most common approach, performed in 50 (53.8%) of thrombotic cases and 67 (98.5%) of embolic cases. Primary amputation was extremely rare, occurring only in thrombotic cases (two patients, 2.2%) (Table 3).
Surgical approach according to etiopathogenesis.
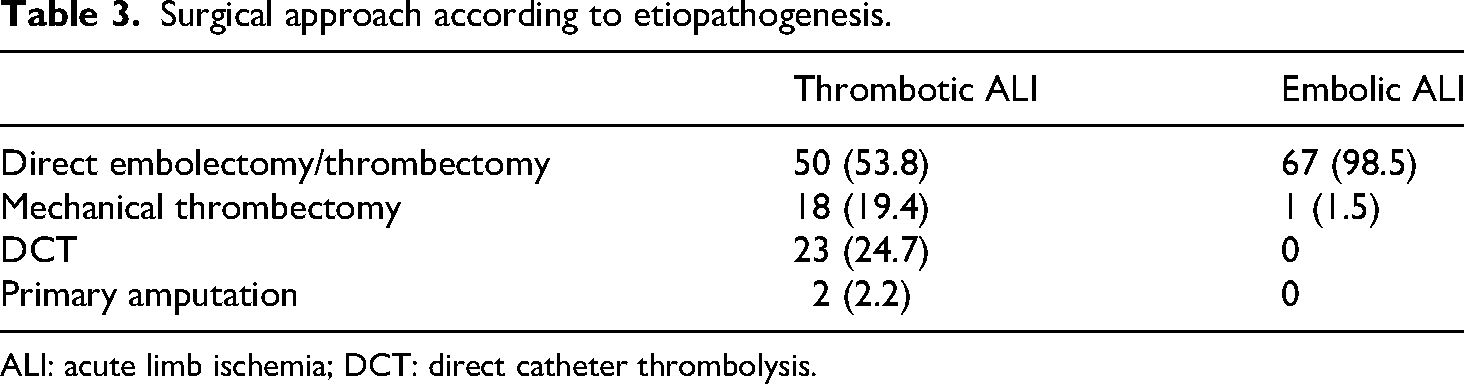
ALI: acute limb ischemia; DCT: direct catheter thrombolysis.
The overall in-hospital mortality rates for each group were N = 16 (19.8%) in the control group, N = 5 (8.1%) in PVD1, and N = 0 in PVD2 (p = 0.026). Secondary amputations occurred in N = 17 (21%) of patients in the control group, N = 18 (29%) in the PVD1 group, and only N = 2 (11.1%) of PVD2 group (p = 0.235) (Table 4).
Patient’s outcomes according to polyvascular disease status.

PVD: polyvascular disease.
Cardiovascular and all-cause mortality rates showed no statistically significant differences among the groups (log-rank p = 0.100 and p = 0.785, respectively), with survival rates remaining relatively high in all groups. However, significant differences were observed in non-cardiovascular mortality (log-rank p = 0.033). By 36 months, survival declined to 87.4% in the control group, 76% in PVD1, and 72.2% in PVD2 (Figure 2). The hazard ratio was 1.840 (95% CI: 1.141–2.967, p = 0.012).

Survival curves of multivessel disease models for long-term results: (a) survival curves for cardiovascular mortality; (b) survival curves for non-cardiovascular mortality; and (c) survival curves for all-cause mortality.
Discussion
The study revealed significant demographic and clinical heterogeneity among the groups. Patients in the PVD1 and PVD2 groups were older and had a higher prevalence of diabetes mellitus and hypertension compared to the control group. Notably, anticoagulant therapy was significantly more frequent in the PVD2 group. Cardiovascular mortality was lower in the PVD1 and PVD2 groups, whereas non-cardiovascular deaths were significantly more common in these groups compared to the control group. AMI and ischemic strokes were significantly more prevalent in the PVD groups, underscoring the severity of their conditions.
When comparing mortality outcomes in this study, it is notable that as the PVD status worsened, non-cardiovascular death rates increased. The differences in mortality rates, when stratified by PVD status, suggest that the presence of PVD increases the likelihood of patients being on anticoagulant therapy or undergoing percutaneous interventions, which may lower their cardiovascular death risk. 14
The present study did not specifically assess the causes of non-cardiovascular mortality. Therefore, the main contributors to this outcome were not specifically assessed in the present cohort. However, Mok et al. and Konig et al. respectively highlighted the association between PAD and a higher prevalence of infectious diseases, as well as the correlation between chronic kidney disease and PVD. These findings support the idea that patients with PVD face increased risks of systemic hazards like infections, renal failure, and metabolic imbalances, leading to higher non-cardiovascular death rates compared to the control group.15,16
This study also suggests that PVD is associated with higher rates of both ischemic stroke and AMI. These findings reflect the increased risk of thromboembolic events and heightened vulnerability to cardiovascular complications in patients with progressively advanced polyvascular impairment. This is consistent with the findings of Baumann et al. and Saito et al., who reported that PVD was a complicating factor in 40 to 70% of AMI cases in their studies.17,18
PVD has also been established as a solid predictor of mortality, particularly non-cardiovascular death. Specifically, individuals with PVD are more prone to suffering from a range of cardiovascular conditions, such as ischemic events, due to compromised vascular reserve, microcirculatory deficiencies, and overall issue and organ perfusion. This data is corroborated by Aday and Matsushita, whose study reported not only a higher risk of AMI, stroke, and sudden cardiac death, but also emphasized the role of microvascular disease and chronic limb ischemia in the pathophysiology of both PAD and PVD. 19 Patients with PVD are also more likely to be affected by conditions such as systemic atherosclerosis, which, when combined with the previously mentioned risk factors, contributes to the development of chronic hypoxia and compromised vascular function. This, in turn, leads to increased rates of postoperative mortality among individuals with PVD. 20 In this regard, Subherwal et al. noted that presence of PVD is directly associated with systemic atherosclerosis, which, for example, increases the risk for ischemic events and overall greater vascular burden, findings that align with those of our study.
Additionally, patients with PVD reported high prevalences of heart failure, although this data did not reach statistical significance (p = 0.058). This is likely associated with CAD, which is the primary risk factor for developing heart failure in these individuals. In fact, this finding has been observed in other studies, such as those by Velagaleti and Vasan, who reported that CAD could account for up to 73% of patients suffering from heart failure. 21 Since CAD has strong collinearity with PVD, this may explain why heart failure was not statistically significant in this study, despite its high prevalence among PVD patients. 22 Chunawala et al. found that the presence of PVD in individuals with both reduced and preserved ejection fraction heart failure significantly increased mortality rates in these patients, with rates of 26% (CI: 1.07–1.50) and 29% (CI: 1.03–1.62) for each subgroup, respectively. This reflects the higher likelihood of individuals with PVD likely having pre-existing conditions, such as heart failure. 23
Finally, when analyzing the results for the presence of AF, this parameter was found to be borderline statistically significant (p = 0.056). This could be because, although AF is associated with significant cardiovascular impairment in those with PVD, 24 it is less impactful than other risk factors, such as systemic atherosclerosis, hypertension, or diabetes mellitus, when specifically considering its association with PVD. AF may also contribute to the observed mortality, as it has been identified as a significant risk factor in patients with PAD, further complicating their clinical outcomes and increasing the likelihood of adverse events, 25 thereby diminishing the role of PVD in predicting long-term all-cause mortality. Our results align with previous studies demonstrating that advanced cardiovascular impairment, particularly the presence of CAD, is associated with worse perioperative outcomes and increased vulnerability to adverse events in patients with ALI, highlighting the systemic impact of multivessel atherosclerosis. 26
Most non-cardiovascular deaths in the cohort were attributed to cancer, predominantly lung and breast cancer, which likely explains the higher mortality observed in the PVD1 and PVD2 groups. Several studies support the observation that non-cardiovascular deaths, particularly from lung and breast cancers, contribute significantly to higher mortality rates in patients with vascular disease. 27 For instance, research indicates that lung cancer patients often present with multiple comorbidities, such as chronic obstructive pulmonary disease, diabetes, and congestive heart failure, which adversely affect survival outcomes. 27 Additionally, some patients were reported to have pneumonia as the cause of death; however, it is plausible that underlying comorbidities contributed significantly to their mortality, highlighting the multifactorial nature of their clinical decline. Importantly, our study adds to the existing literature by demonstrating that non-cardiovascular mortality is significantly higher in patients with multivessel disease, underscoring the need for tailored, multidisciplinary care in this population—a perspective that has not been extensively addressed in earlier studies. 28
One of the limitations of the study is the small size of the study group. Although patients with varying degrees of vascular impairment, there was still an uneven distribution of patients across the three subgroups (control, PVD1, and PVD2). The limited number of in-hospital mortality events (n = 20) restricted our ability to perform a reliable multivariable analysis on short-term outcomes. Moreover, all patients were treated and followed in a single high-volume tertiary care center, which could affect the external validity of the results. Other limitations include the lack of data on anticoagulant/antiplatelet therapies upon discharge, factors that could influence postoperative and long-term outcomes. Furthermore, the fact that the outcomes reported were measured within a 30-day timeline restricts the ability to generalize findings to a longer-term analysis.
An important limitation of this study is the relatively small number of patients in the PVD2 subgroup, which may reduce the statistical power and reliability of the findings specific to this population. However, the decision to maintain separate PVD1 and PVD2 groups was based on clinically relevant distinctions: PVD1 includes patients with involvement of a single arterial bed, whereas PVD2 represents individuals with two affected vascular territories (e.g. cerebrovascular, coronary, or peripheral), reflecting a more advanced atherosclerotic burden and potentially distinct prognostic implications. Although the results concerning the PVD2 group should be interpreted with caution, preserving this stratification allows for a more refined analysis of the progressive impact of PVD. Further studies with larger sample sizes are needed to validate and expand these findings.
Finally, the lack of detailed information on the postoperative period, including data on ischemic events during the follow-up and other factors such as patient adherence to therapy and rehabilitation progress, underscore the need for follow-up studies with broader data collection. This study should aim to evaluate the long-term survivability and the progression of morbidity and mortality rates within this population. Patients who were directly referred to end-of-life and palliative care were most likely those with higher PVD scores, which may have introduced selection bias. Additionally, conducting sensitivity analyses was not feasible in this study.
Further studies focusing more on long-term complications and therapeutic measures are needed to strengthen the findings of this study. Such research should aim to evaluate more effective therapeutic interventions, develop faster and more efficient screening techniques, and ultimately provide a better long-term prognosis for patients with PVD, exposed to acute limb ischemia.
Additionally, implementing a multidisciplinary care model could enhance the assessment of each patient’s overall vascular impairment and associated comorbidities, such as hypertension and diabetes mellitus. 29 This approach could not only improve the vascular viability of the affected limbs but also advance screening and treatment strategies for hazardous outcomes reported in this study, including AMI and ischemic stroke.
Conclusion
The presence of PVD may be associated with worse outcomes in patients diagnosed with ALI, also reflecting on higher rates of both cardiovascular and non-cardiovascular death. The results suggest that measures such as an optimized prescription of anticoagulant drugs and the use of revascularization techniques could improve the systemic cardiovascular function in these patients. However, as indicated by the high non-cardiovascular death rates observed, a multidisciplinary approach would be the most effective way to enhance postoperative quality of life and event-free survival of these patients. Further studies are necessary to validate PVD as an independent risk factor in this patient population, and prospective cohort studies are warranted to better characterize its prognostic impact.
Footnotes
Author contributions
Simão Almeida-Oliveira: conceptualization; methodology; writing—original draft; equally contributed as first author. João Rocha-Neves: supervision; writing—review and editing; project administration; equally contributed as first author. Leonardo Araujo-Andrade: visualization; formal analysis; writing—review and editing. Mariana Fragao Marques: literature review; validation; writing—review and editing. Tomasz Goryń: data collection; investigation; writing—review and editing. Izabela Taranta: data collection; resources; methodology. Włodzimierz Hendiger: data collection; validation; investigation. Hugo Ribeiro: statistical analysis; conceptualization; writing—review and editing. Piotr Myrcha: data collection; supervision (local); writing—review and editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by National Funds through FCT - Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mariana Fragao Marques is an employee of Novo Nordisk.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.