
Abstract
Objective
The aim of this study was to evaluate the efficacy of hybrid therapy and endovascular therapy in the treatment of complex femoropopliteal Trans-Atlantic Inter-Society Consensus II D(TASC D) lesions involving the common femoral artery bifurcation.
Methods
Patients with complex femoropopliteal TASC D lesions involving the bifurcation of the common femoral artery for atherosclerotic disease were retrospectively analyzed in our institution from July 2018 to July 2023. Patients were followed up at 1, 3, 6, and 12 months and then every year. Clinical data were collected, including perioperative and follow-up information. The patency rate and the rate of freedom from clinically driven target lesion revascularization (CD-TLR) were measured using the Kaplan–Meier method.
Results
A total of 29 patients with 31 limbs (mean age 73.5 ± 11.5 years; 20 men) were included, divided into the hybrid therapy group (20 limbs, Group 1) and endovascular treatment group (11 limbs, Group 2). The mean follow-up time was 22.5 ± 16.3 months (1–60 months), and the mean length of the lesion was 31.5 ± 11.6 cm. Between these two groups, there was no statistically significant difference on baseline data P>.05). Group 1 had more long-segment chronic total occlusive (CTO) lesions than Group 2(P<.05). Totally, the 1- and 2-year patency rates of TASC D lesions were 74.6% and 55.2%, respectively; and the rate of freedom from CD-TLR was 81.2% and 70.3%, respectively. There was no statistically significant difference between these two groups in terms of 1-year primary patency rate(88.7% vs 100%) and freedom from CD-TLR of the common femoral artery (CFA) bifurcation(93.8% vs 100%)(P>.05).
Conclusions
For common femoral artery bifurcation lesions, both hybrid endarterectomy and endovascular treatment demonstrate favorable clinical outcomes. While these findings support their use, definitive conclusions on comparative efficacy remain conditional on confirmation from large-scale, long-term studies.
Introduction
The incidence of peripheral arterial disease (PAD) is still quite high.1,2 Treatment remains difficult for Trans-Atlantic Inter-Society Consensus II D (TASC D) lesions, 3 particularly the long-segment lesions involving both the iliac and femoral arteries. Based on the data from earlier research, the 1-year patency rate is only roughly 70%. 4 For lesions involving the bifurcation of the common femoral artery (CFA), endarterectomy remains the gold standard. 5 The benefits of endovascular therapy include minimal trauma, a brief hospital stay, and a quick recovery. The straightforward endovascular treatment of CFA bifurcation remains controversial and has generated a lot of discussion among academics. 6
TASC D lesions represent a heterogeneous subset of peripheral artery disease, with femoral bifurcation involvement introducing unique anatomical challenges, such as diffuse calcification and multi-vessel involvement. Hybrid therapy, combining endarterectomy with endovascular revascularization, has emerged as a promising approach for such complex lesions, leveraging the benefits of open plaque removal and minimally invasive distal revascularization. 5 However, its specific role in femoral bifurcation lesions remains understudied. Some articles published in the past few years have highlighted the need to further investigate the viability of endovascular treatment for appropriate bifurcation of CFA lesions, based on the type of lesions involved.6–9 For both mechanical and anatomical reasons, the CFA lesion has been a red line for a long time in peripheral artery diseases. Furthermore, some research endeavored to surpass this red line. 6 It is challenging to obtain the optimal lumen plastic effect with simple balloon dilatation for chronic total occlusive (CTO) lesions in the bifurcation of CFA because of the burden of plaque and thrombus. Currently, there is a new option for treating the disease of CFA bifurcation thanks to a few debulking devices and the use of drug-coated balloons (DCB).10,11 While open repair remains undoubtedly the most standard operation for the treatment of femoral bifurcation lesions, an increasing number of cases and reports using endovascular treatments have been published, 12 as minimally invasive technology is reserved for the aging patients. The discussion on the function of endovascular repair has been rekindled by the encouraging outcomes. Nevertheless, there aren't any independent studies on the management of intricate TASC D lesions that involve bifurcation of CFA currently. Here, we reported 5-year experience of our institution in the treatment of patients with complex lesions involving bifurcation of CFA.
Methods
Study design and data collection
A retrospective analysis was conducted on patients with complex femoropopliteal TASC D lesions involving the CFA bifurcation who underwent hybrid therapy (combined endarterectomy-endovascular intervention) or endovascular therapy between July 2018 and July 2023. The study was conducted in accordance with the Helsinki Declaration of 1975 as revised in 2024 and was approved by the Ethics Committee (B2025-018) with the need for written informed consent waived. We declare that all patient information has been de-identified. The reporting of this study conforms to STROBE guidelines. 13
Vascular characteristics were systematically evaluated using computed tomography angiography (CTA) and intraprocedural angiography to verify lesion morphology. Lower limb vascular lesions were classified according to the 2007 TASC II criteria and Rutherford Classification. Bifurcation lesions were subclassified using the amended Medina classification, 14 which included four subtypes: 1-0-0 (isolated CFA involvement), 1-0-1 (CFA + profunda femoris artery), 1-1-1 (CFA + profunda + superficial femoral artery [SFA] origin), and 1-1-0 (CFA + SFA origin).
Exclusion criteria included acute limb ischemia, a life expectancy of less than 1 year, or contraindications to antiplatelet therapy. Treatment selection: for CFA lesions with CTO, femoral endarterectomy or hybrid procedures were prioritized; for stenotic lesions, endovascular or hybrid therapy was considered. Endovascular techniques were used in patients unfit for surgery due to high-risk factors (e.g., severe cardiopulmonary compromise, end-stage renal disease) or anatomical challenges (e.g., high bifurcation location).
Data collected encompassed baseline demographics, stenosis/occlusion types, bifurcation lesion subtypes, baseline calcification severity, lesion length, ankle-brachial index (ABI), and proximal/distal outflow characteristics of the CFA, providing a comprehensive framework for comparative analysis.
Procedure details
Prior to surgery, all patients received dual antiplatelet therapy (clopidogrel 75 mg and aspirin 100 mg once daily) along with statin therapy (Atorvastatin 20 mg once daily). Intravenous heparin (70 U/kg) was administered to every patient. While most patients receiving endovascular treatment were under local anesthesia, all patients undergoing hybrid surgery were under general anesthesia. For endovascular procedure, arterial access was exclusively achieved via a contralateral femoral cross-over approach, utilized in 100% of patients in this cohort (no upper extremity access was employed). Prior to intervention, all patients underwent preliminary digital subtraction angiography to delineate vascular anatomy and characterize target lesions. Treatment of femoral bifurcation lesions was individualized based on lesion morphology, incorporating percutaneous transluminal angioplasty (PTA), self-expanding or balloon-expandable stent implantation, atherectomy, or combined modalities, with particular attention to calcification burden, lesion length, and bifurcation involvement. For occlusive lesions, retrograde popliteal artery access was employed if initial antegrade intraluminal or subintimal passage attempts were unsuccessful, ensuring procedural flexibility for complex anatomies. Simultaneous treatment of the superficial femoral artery (SFA) and profunda femoris artery was systematically performed, with intraoperative angiographic evaluation to confirm adequate outflow in both branches. Patency of the profunda femoris artery was meticulously monitored throughout the procedure, and no cases of post-procedural profunda occlusion were documented in this series. For hybrid surgery, the inguinal area was cleaned and sterilely draped in preparation. Usually, a longitudinal inguinal incision was used to expose the ipsilateral CFA bifurcation. Femoral artery exposure was performed first to facilitate open surgical preparation of the CFA. Following successful CFA reconstruction (e.g., endarterectomy), proximal/distal endovascular therapy was initiated, with arterial access established via the surgically exposed CFA using a 6-F sheath in an antegrade manner to address adjacent lesions. For all patients, either upward or downward endovascular revascularization came first, following an open arterial endarterectomy with or without a patch. The common femoral artery is used to place the artery sheath either above the anastomosis or by directly puncturing the patch. The elastic retraction of the vessel following balloon dilation of more than 50% and/or the occurrence of dissection were the signs of self-expanding stenting. For eccentric plaques or severely calcified lesions at the common femoral artery bifurcation, directional atherectomy with the Turbohawk/Silverhawk device (Medtronic) was used for plaque debulking. Thrombotic lesions were managed with the Straub Rotarex thrombectomy system (BD Medical) to remove the thrombus. After adequate vascular preparation, DCBs were preferentially used to inhibit neointimal hyperplasia.
Outcome and follow-up evaluation
Patency rate, freedom from clinically driven target lesion revascularization rate (CD-TLR), and complications were among the study's endpoints. The state of continuous stent patency following revascularization was referred to as primary patency. Following the documentation of recurrent clinical symptoms, the CD-TLR referred to procedures carried out for >50% diameter stenosis within 5 mm of the target lesion identified by duplex ultrasound or CTA. Any amputation above the ankle was considered a major amputation.
Routine follow-up included Doppler ultrasound at 1, 3, 6, and 12 months. CTA was performed when ultrasound images were suboptimal or when clinical suspicion of restenosis existed (Rutherford class progression, ABI decrease ≥0.15). After 30 days of the index procedure, adverse events and complications were noted.
Statistical analysis
The standard deviation ± mean was used to present continuous data. Numbers were provided for categorical data. When conducting statistical analysis on data that follows a normal distribution, use the paired t-test. If the data were not in line with the normal distribution, the Wilcoxon–Whitney U test was run. The Kaplan–Meier life table method was used to conduct patient and CD-TLR analyses. With the log-rank test, the variations in patency rates were ascertained. Regarding categorical variables, the X2 test was employed to assess the variations between the patient groups. It was assumed that P<.05 had statistical significance. Version 22 of IBM SPSS software, from IBM Corporation in Somers, New York, USA, was used for statistical analysis and graph charting.
Results
Twenty-nine patients total with 31 limbs (mean age 73.5 ± 11.5 years; 20 men) were included and divided into two groups: hybrid therapy (Group 1, 20 limbs) and endovascular treatment (Group 2, 11 limbs). The follow-up period averaged 22.05 ± 16.03 months. Technical success in both groups was 100% in the primary procedural. Baseline data identified that between these two groups, there were no statistically significant differences in established risk factors for vascular disease, such as smoking, type II diabetes, hypertension, and hyperlipidemia. (Table 1). In terms of Rutherford classification distribution, group 1 had a larger percentage of chronic limb-threatening ischemia (CLTI) patients than group 2, and this difference was statistically significant (P < .05). Regarding the type of lesions, there were more CTO lesions in group 1 compared with group 2 (P < .05). There was no significant difference in ABI between these two groups before and after surgery (P > .05). Between the two groups, there was no statistically significant difference in run-off, calcification and Medina classification (P > .05) (Table 2). Most patients in both groups received simultaneous treatment for combined run-in and run-off tract obstruction (Table 3).
Baseline data of the patients.
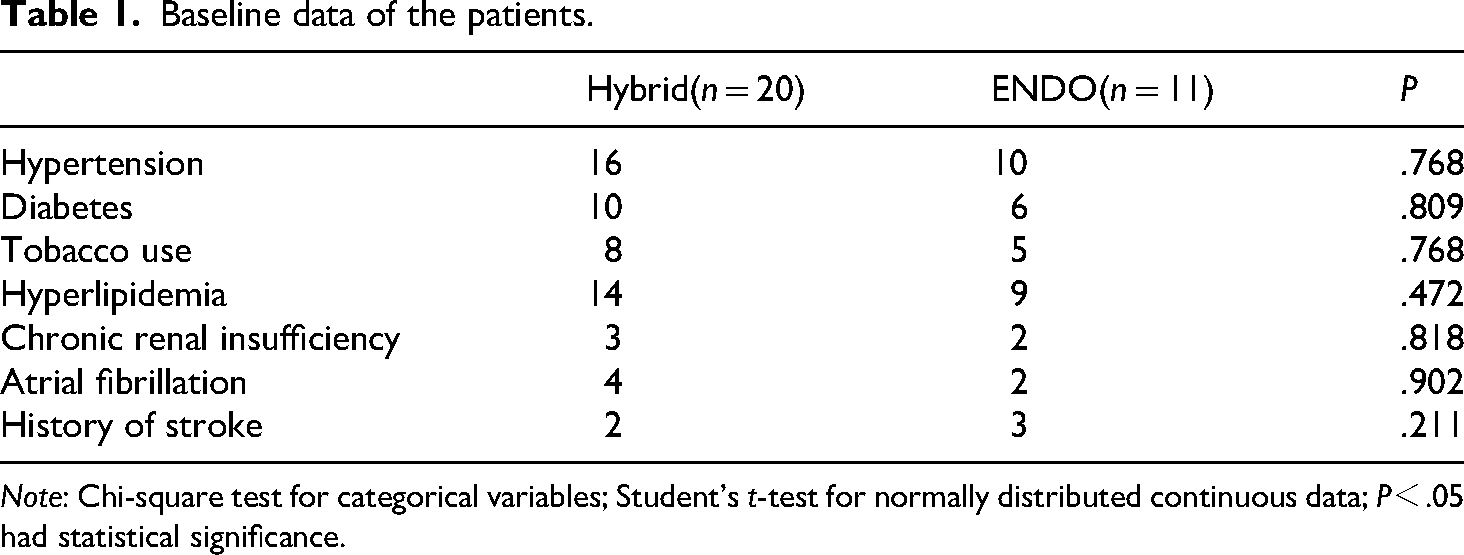
Note: Chi-square test for categorical variables; Student’s t-test for normally distributed continuous data; P<.05 had statistical significance.
Characteristics of the patients.
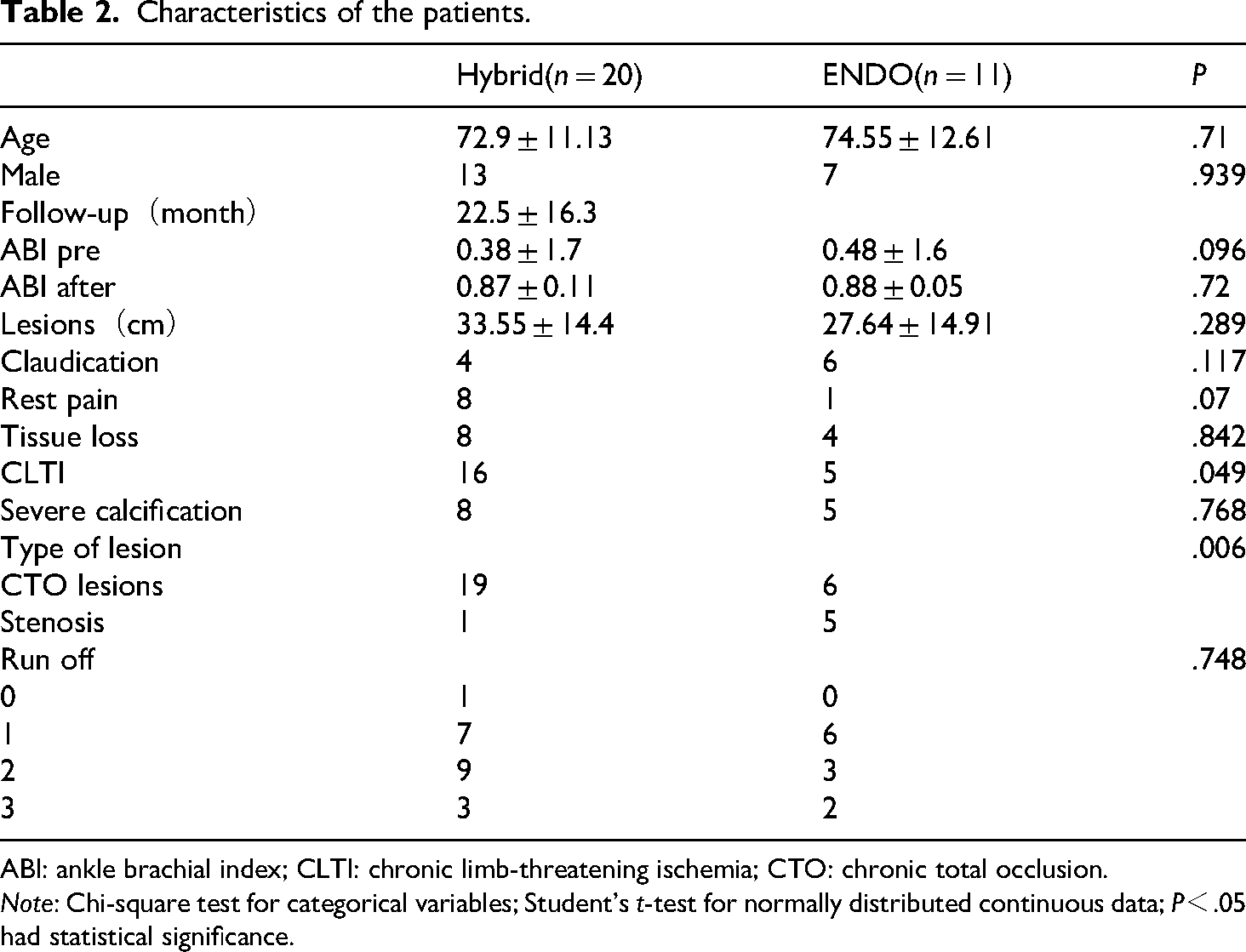
ABI: ankle brachial index; CLTI: chronic limb-threatening ischemia; CTO: chronic total occlusion.
Note: Chi-square test for categorical variables; Student’s t-test for normally distributed continuous data; P<.05 had statistical significance.
Comparison of the clinical outcomes and followed-up data.

CFA: common femoral artery; DCB: drug-coated balloon.
Note: Chi-square test for categorical variables; Student’s t-test for normally distributed continuous data; P<.05 had statistical significance.
According to Kaplan–Meier estimates, the 1-year and 2-year primary patency rates in the overall sample were 74.6% and 55.2%, respectively. The 1-year and 2-year patency rates of group 2 were slightly higher than those of group 1, but there was no statistically significant difference (P > .05) (72.4% and 49.8% vs 78.8% and 65.6%, group 1 vs group 2, Figure 1). In regard to the CD-TLR freedom rate, the 1-year and 2-year rates in the overall sample were, respectively. There was also no statistically significant difference between these two groups (81.2% and 70.3% vs 77.1% and 67.4%, group 1 vs group 2, P > .05) (Figure 2). The 1-year primary patency rate (Figure 3) and CD-TLR freedom rate of the CFA bifurcation were 88.7% vs 100% and 93.8% vs 100% in these two groups, respectively (P > .05, Figure 4).

Primary patency of each group and overall.

Freedom from CD-TLR of each group and overall.

Primary patency of CFA bifurcation of each group.

Freedom from CD-TLR of CFA bifurcation of each group.
Preoperative Rutherford grades demonstrated a significant improvement postoperatively (P < .001). The mean preoperative grade was 4.23 ± 1.06, which decreased to 2.19 ± 1.56 at 6-month follow-up. Preoperative mean Rutherford grade was 4.20 ± 0.95, improving to 2.30 ± 1.56 postoperatively (P < .001) in group 1, and 4.27 ± 1.27, decreasing to 2.00 ± 1.61 postoperatively (P < .001) in group 2 (Figure 5).

Comparison of Rutherford classification: overall preoperative vs postoperative outcomes (left panel) and group-based pre- and postoperative comparisons (right panel).
As for complications, in group 1, three patients had major amputations; three patients had cerebrovascular accidents during the perioperative phase; one patient experienced stent rupture at the CFA bifurcation during the follow-up period. Subsequently, a secondary intervention was carried out to remove the ruptured stent and reconstruct the artery. Despite these efforts, this patient ultimately underwent major amputation during the follow-up. In Group 2, two patients experienced perioperative hematomas at the puncture site, and one patient underwent a major amputation. There was no statistically significant difference between these two groups (Table 3) (P > .05).
Discussion
This study retrospectively analyzed the therapeutic effects of hybrid therapy and endovascular therapy on complex TASC-D lesions involving the common femoral bifurcation. The overall patency rate was still relatively low, with a 1-year patency rate of approximately 70% and a 2-year patency rate of approximately 50%. The patency rate of the hybrid surgery group was lower than that of the endovascular therapy group, but there was no significant statistical difference. Regarding the patency rate of the target vessels of the CFA, the endovascular therapy group had a higher patency rate, but there was no statistically significant difference between the two groups. Complications did not differ significantly between groups (P > .05), though the hybrid group had more perioperative strokes (3 vs 0), a finding warranting clinical attention despite statistical insignificance, possibly related to longer anesthesia times in open-hybrid cases.
This study was the first to report complex TASC D lesions with bifurcation of CFA. Previous meta-analyses have reported that the overall 1-year and 2-year primary patency rate for TASC D-grade lesions was 49%–74% and 41%–82%, respectively, with the rate of freedom from CD-TLR 76%–95% and FCD-TLR 47%–76%. 15 The interval value of patency rate varies widely, indicating that the overall patency rate is still not ideal for complex lower extremity arterial lesions. The overall 1-year and 2-year patency rates in this study were 74.6% and 55.2%, respectively. The overall rate of CD-TLR for 1-year and 2-years were 81.2% and 70.3%, respectively, similar to the research reports. However, the lesions in this study were more complex, as all lesions involved the common femoral bifurcation. Half of the samples had both run-in lesions, and almost all cases had poor run-off lesions to treat.
Endarterectomy has always been the gold standard for the treatment of common femoral artery lesions. Its advantage was to directly maximize the reduction of plaque load in the vessel lumen.16,17 The technical success rate reported in literature reaches 95%–100%. 10 According to the report,8,10,18,19 the 1-year and 5-year patency rates are approximately 90% and 80%, respectively. However, many PAD patients are elderly and cannot tolerate long-term surgery under general anesthesia, which is related to a higher incidence of perioperative complications in open surgical specimens.8,20 Although there was no statistically significant difference in the incidence of complications between these two groups in this study, the incidence of central cerebrovascular accidents was higher in the hybrid surgery group. For such patients, endovascular treatment may be a better option to reduce the risk associated with general anesthesia. At least so far, endarterectomy has been shown to be superior to endovascular treatment, although this may be due to insufficient long-term data on endovascular treatment. 21 With the development of innovative endovascular instruments in recent years, many studies have explored and confirmed the feasibility of endovascular therapy for the treatment of CFA bifurcation lesions, but currently, there is no clear diagnostic and treatment standard.
Which type of lesions are more suitable for endovascular treatment? In the CONFESS study, when evaluating the anatomical factors and plaque burden of the common femoral artery, 90% of the lesions can still be treated endovascularly.6,22 The technical success rate of this study was 100%, and the endovascular treatment group had a higher patency rate of the CFA bifurcation. This could be related to the inclusion of more stenotic lesions in the endovascular treatment group, while almost all members of the hybrid surgery group had occlusive lesions in the CFA bifurcation. Although the sample size of the endovascular treatment group included in this study was relatively small, including cases of simple balloon dilatation (or in combination with DCB), the use of debulking devices and stents, the patency rate of the target vessels of the common femoral artery in total patients in this group was 100%, and the high patency rate deserved recognition. In this study, three cases were treated with debulking devices (including the use of Turbohawk and Rotarex), all of which achieved good clinical results and were worthy of recognition for their efficacy. A retrospective study compared the use of debulking devices and balloon dilation alone in 164 CFA patients, with the former demonstrating a higher 4-year primary patency rate (87.1% vs 66.7%). 23 However, there were still few reports on the use of debulking devices to treat CFA bifurcation lesions, and more evidence is needed to support this hypothesis.
The placement of a stent for the CFA bifurcation has long been regarded as a red line, as the unique anatomical environment of the inguinal region increases the risk of stent distortion and rupture, and stent placement limits the access options for future endovascular treatment and damage to the deep femoral artery.24–26 In previous reports of stent placement in the common femoral artery, the overall 1-year primary patency rate of the femoral target vessel was 67%–100%, the 1-year FCD-TLR was 54%–100%, and there was the highest stent rupture rate of up to 9%.9,26 Based on the data from our center, there were four cases of stent placement in the common femoral artery, all of which used self-expanding stents. Among them, 1 case had stent rupture, but it occurred in the hybrid treatment group (subsequent incision repair was performed to remove the broken stent), and there was no stent rupture in the endovascular treatment group. There were also articles reporting the performance of the Supera stent in CFA, with a 0-fracture rate and a 1-year 100% patency rate. 9 The stent was not used in this study, and further evidence-based reports were expected in the future. Based on the current body of research, caution should still be exercised when placing common femoral artery stents, but increasing reports suggest that the benefits of endovascular treatment of common femoral artery lesions have gradually been demonstrated.
Due to the retrospective nature of this study, there were many limitations: firstly, the study’s small sample size and single-center design limit statistical power, increasing the risk of Type II error (failure to detect true differences). While no significant differences were observed, this should not be interpreted as therapeutic equivalence. A longer, standardized follow-up period would provide more robust data on long-term patency and clinical outcomes, remaining a critical area for future research. Secondly, the hybrid group exhibited a higher proportion of long-segment CTO lesions, a known predictor of poorer patency. This baseline imbalance introduces confounding, as CTO complexity may influence outcomes independently of treatment modality. While statistical balance was achieved for most risk factors, the CTO burden highlights the need for caution when interpreting between-group comparisons. Finally, the follow-up period was not long enough, and further follow-up is required for the medium- to long-term patency rate with endovascular treatment.
Conclusion
In patients with complex TASC-D lesions involving the femoral bifurcation site, both hybrid surgery and endovascular treatment could achieve good clinical outcomes. However, the overall patency rate of TASC-D lesions was relatively poor, and the reintervention rate was high, which still remains a challenge. The results of this study suggest that endovascular treatment of common femoral artery lesions has good prospects and could be used as an alternative treatment, but further evidence-based hospital evidence is needed to support this standpoint.
Footnotes
Author note
Yue Lin (YL); Tianyue Pan (TP); Shichai Hong (SH); Weifeng Lu (WL); WeiGuo Fu (WF); LiXin Wang (LW); Xiang Hong (XH); Gang Chen (GC); Yulong Huang (YH); Yihui Chen (YC); Xinsheng Xie (XX).
Acknowledgements
We thank the Department of Vascular Surgery at Zhongshan Hospital for providing technical support and clinical data. Additionally, we utilized Doubao, an AI-powered software, to enhance the language quality of this manuscript.
Author contributions
Conception and design: YL, TP, SH, WL, WF, LW, XH, GC, YH, XX. Analysis and interpretation: YL, TP, SH, WL, WF, LW, XH, GC, YH, XX. Data collection: YL, TP, SH, WL, WF, LW, XH, GC, YH, XX. Writing the article: YL, TP. Critical revision of the article: YL, TP, SH, WL, WF, LW, XH, GC, YH, XX. Final approval of the article: YL, TP, SH, WL, WF, LW, XH, GC, YH, XX. Statistical analysis: YL. Obtained funding: YL, WL. Overall responsibility: WL, WF, YL, TP.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fujian Provincial Natural Science Foundation Project (grant numbers 2022J011422, 2024J011441).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.