
Abstract
Introduction
Obstructive sleep apnea (OSA) is linked to a complex network of comorbidities, including cardiovascular, metabolic, neurological, and oncological diseases. The comorbidome visually maps disease associations, highlighting the interconnected comorbidities of OSA, whose incidence and severity are strongly correlated.
Methods
A retrospective cohort study was conducted between 2005 and 2020 to identify the comorbidities most frequently associated with OSA through a comprehensive comorbidity map. The prevalence of each comorbidity was calculated as a percentage, and a detailed analysis was performed to examine the relationship between these comorbidities and the severity of OSA. This graphic represents all comorbidities with significant associations to OSA, where the size of each bubble is proportional to the prevalence of the disease within the cohort, and the proximity to the center reflects the strength of the association.
Results
A total of 3043 patients diagnosed with OSA were included, of whom 51.1% (1154/3043) had severe OSA, 29.2% (889/3043) had moderate OSA, and 19.7% (600/3043) had mild OSA. The average age was 57.6 years (SD ± 15.32), and 65.6% (1995/3043) were men. Among patients with mild OSA, hypertension was present in 48.0% (288/600), in moderate OSA in 53.0% (470/889), and in severe OSA in 58.5% (909/1554). Renal failure (OR: 9.39; 95% CI: 3.7–23.84), cardiovascular disease (OR: 7.73; 95% CI: 3.92–15.21), dementia (OR: 6.98; 95% CI: 2.85–17.11), hemiplegia/stroke sequelae (OR: 6.90; 95% CI: 2.02–23.51), smoking (OR: 5.54; 95% CI: 2.74–11.21), and diabetes (OR: 4.34; 95% CI: 2.02–9.35) were associated with mild OSA. Hemiplegia/stroke sequelae (OR: 10.11; 95% CI: 3.8–26.89), cardiovascular disease (OR: 9.77; 95% CI: 6.18–15.46), chronic pulmonary disease (OR: 7.48; 95% CI: 4.76–11.77), and dementia (OR: 6.80;95% CI: 3.37–13.71) were associated with moderate OSA. Dementia (OR: 10.59; 95% CI: 6.41–17.5), leukemia and lymphoma (OR: 7.49; 95% CI: 2–28.1), chronic pulmonary disease (OR: 7.24; 95% CI: 5.33–9.83), hemiplegia or stroke sequelae (OR: 6.33; 95% CI: 3.3–12.16), and renal failure (OR: 6.10; 95% CI: 3.97–9.36) were associated with severe OSA.
Conclusion
The most prevalent comorbidities were hypertension, smoking, and cardiovascular disease, with a higher incidence in patients with severe OSA. Additionally, a significant association was observed between certain comorbidities and mortality, particularly conditions such as renal failure and dementia. Malignant or neoplastic diseases were related to severe OSA.
Introduction
Obstructive sleep apnea (OSA) is characterized by repetitive episodes of complete or partial collapse of the upper airways during sleep.1–3 This condition affects approximately 2–4% of the adult population and has a high prevalence worldwide.2,3 It is estimated that 936 million adults aged 30 to 69 suffer from OSA, regardless of disease severity (95% CI: 903–970 million).2,3 Of these, approximately 425 million (95% CI: 399–450 million) suffer from moderate to severe OSA.2,3 OSA has been linked to the pathogenesis of various cardiovascular disease (CVD), metabolic, neurological, oncological, and other diseases.4–6 In addition, patients with OSA have a high burden of comorbidities, which can significantly impact their prognosis and survival, affect their response to treatment, and reduce their quality of life.7–9
The incidence of comorbidities and the severity of OSA are closely related, which may negatively affect patient survival.10,11 Diseases such as heart failure and metabolic syndrome may not only be consequences of OSA,8,9 but may also predispose to the development of this condition, suggesting a bidirectional relationship between OSA and certain comorbidities.9,12–14 In this context, mechanisms such as intermittent hypoxia, fluctuations in intrathoracic pressure, and recurrent microarousals play a crucial role.1,8,15 These phenomena trigger sympathetic excitation, systemic inflammation, and oxidative stress, contributing to disorders such as hypertension, atherosclerosis, and diabetes.8,10,16,17 At the same time, conditions like obesity and metabolic syndrome can predispose to OSA, creating a cycle in which each disorder exacerbates the other.1,16–18 This bidirectional link complicates the independent evaluation of their effects, highlighting the complexity of their therapeutic management.1,8
In Colombia, there is limited evidence on the relationship between OSA, the prevalence of comorbidities, and the characteristics of this population.2,3,9,19 The comorbidity map (comorbidome) is a valuable tool to understand the comorbidities associated with OSA, being essential for personalizing treatments and improving risk stratification.8–15,19 This can increase the available data and improve characterization in these patients, potentially fostering the development of comprehensive management protocols.8,9,19,20 Therefore, the main objective of this study is to determine the prevalence of comorbidities in patients diagnosed with OSA in Colombia and describe the most frequently associated diseases using the Comorbidome.
Methods
A retrospective cohort study was conducted on patients treated at the Clínica Universidad de La Sabana, located in Chía, Colombia, between 2005 and 2020. The primary objective of this study was to describe the comorbidities most frequently associated with OSA and represent them in a comorbidity map (comorbidome) reflecting their prevalence according to the severity of OSA. The study was conducted in accordance with the principles of the current Helsinki Declaration of 1975, as revised in 2024, as well as local, regional, and international regulations pertaining to clinical research, including Colombian Law on Biomedical Research. Ethical approval was obtained from the Medical Ethics Committee of the Clínica Universidad de La Sabana (approval number: 20211203). All personal data of patients has been deleted. This was a retrospective study, and informed consent was not required. The reporting of this study conforms to STROBE guidelines Supplementary Table 1. 21
General characteristics.
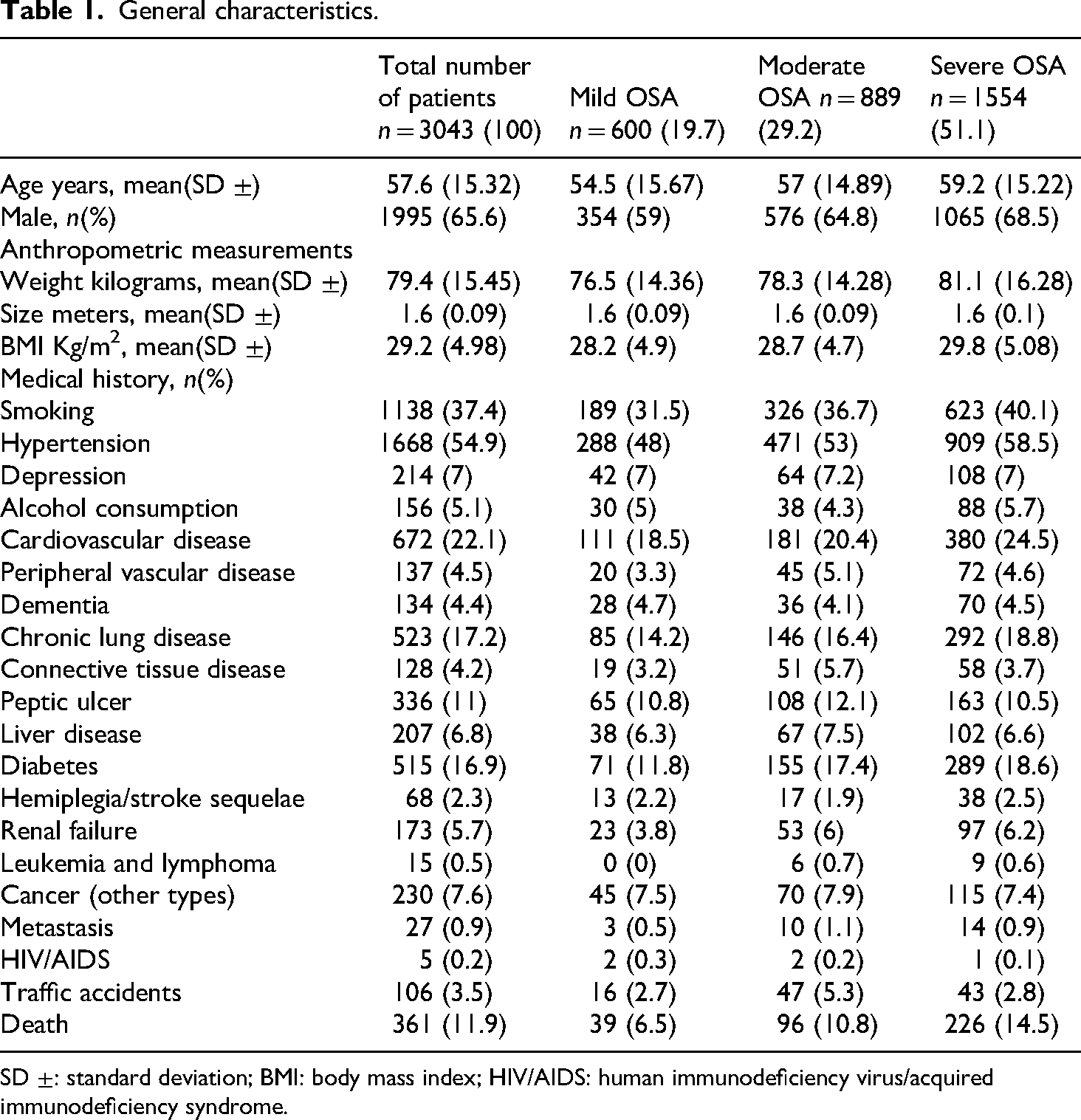
SD ±: standard deviation; BMI: body mass index; HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome.
Eligibility criteria
Patients aged 18 years and older with a diagnosis of OSA, defined by an apnea-hypopnea index (AHI) greater than 5, confirmed through polysomnography (PSG) according to the criteria of the American Academy of Sleep Medicine,22,23 were included. Patients with insufficient information or no AHI data were excluded. This was a retrospective study in which patients were included consecutively.
Variables and data collection
Variables such as age, sex, anthropometric measurements, and medical history of conditions like hypertension, diabetes, congestive heart failure, atrial fibrillation (AF), cerebrovascular events, acute myocardial infarction, chronic kidney disease, chronic obstructive pulmonary disease, and cancer (leukemia, lymphoma, metastatic disease), among others, were collected. For PSG variables, the first AHI reported in the medical record was used for diagnosis. Data collection was performed using a database directly obtained from electronic medical records and diagnostic test results. Precise eligibility criteria were established to minimize selection bias. To reduce transcription bias, at least two team members reviewed the information. Additionally, all variables were clearly defined, and the researchers responsible for data collection were trained.
Confounders and assumptions underlying comorbidity visualization
To account for potential confounders, we performed a stratified analysis by OSA severity and adjusted for key demographic and clinical variables, including age, sex, and body mass index (BMI), which are known to influence the presence of comorbidities. Additionally, the construction of the comorbidome assumed that the prevalence and strength of association of each comorbidity with OSA severity reflect underlying pathophysiological and epidemiological relationships. The inverse odds ratio (1/OR) was used as a measure of association to ensure that stronger relationships were visually represented by greater proximity to the center of the comorbidome. This approach allows for a clearer depiction of disease clustering patterns within the cohort.
Statistical analysis
The collected data were transcribed into the Research Electronic Data Capture (REDCap) software. 24 Quantitative variables were summarized using measures of central tendency and dispersion. For normal distributions, means and standard deviations (SD ±) were calculated, and for non-normal distributions, medians and interquartile ranges were used. The normality of distributions was assessed using the Shapiro–Wilk test.
Qualitative variables were described using absolute and relative frequencies. Additionally, the prevalence of each comorbidity was calculated as a percentage, and an analysis of the comorbidities in relation to the severity of OSA (mild AHI 5–15 apneas per hour, moderate AHI 15–30 apneas per hour, severe AHI >30 apneas per hour) was performed.
To visualize the comorbidities associated with OSA, a comorbidome was created. This graphic represents all comorbidities with significant associations to OSA, where the size of each bubble is proportional to the prevalence of the disease within the cohort, and the proximity to the center reflects the strength of the association. This strength was quantified numerically as the inverse of the odds ratio (1/OR). Statistical analysis was carried out in Microsoft Excel, while data preparation and graphical visualizations were performed using Python 3.12.
Comorbidome interpretation
The comorbidome visually represents the relationships between OSA and its associated comorbidities. In this graphical model, each comorbidity is depicted as a bubble, with its size proportional to the prevalence within the study cohort. The proximity of a bubble to the center reflects the strength of its association with OSA, quantified using the inverse odds ratio (1/OR). Comorbidities closer to the center have a stronger association with OSA severity, while those positioned further away have weaker associations.
Results
General characteristics
A total of 3043 patients diagnosed with OSA were included, of which 51.1% (1154/3043) had severe apnea, 29.2% (889/3043) had moderate apnea, and 19.7% (600/3043) had mild apnea (Figure 1). The average age was 57.6 years (SD ± 15.32). 65.6% (1995/3043) were male. The average BMI was 29.8 kg/m² (SD ± 5.08) in severe OSA, 28.7 kg/m² (4.7) in moderate OSA, and 28.2 kg/m² (4.9) in mild OSA. In this study, 54.9% (1668/3043) had a history of systemic hypertension, 37.4% (1138/3043) were smokers, 22.1% (672/3043) had CVD, 17.2% (523/3043) had chronic pulmonary disease, and 16.9% (515/3043) had diabetes. The overall mortality rate was 11.9% (361/3043). Table 1 shows the general characteristics of the study participants.
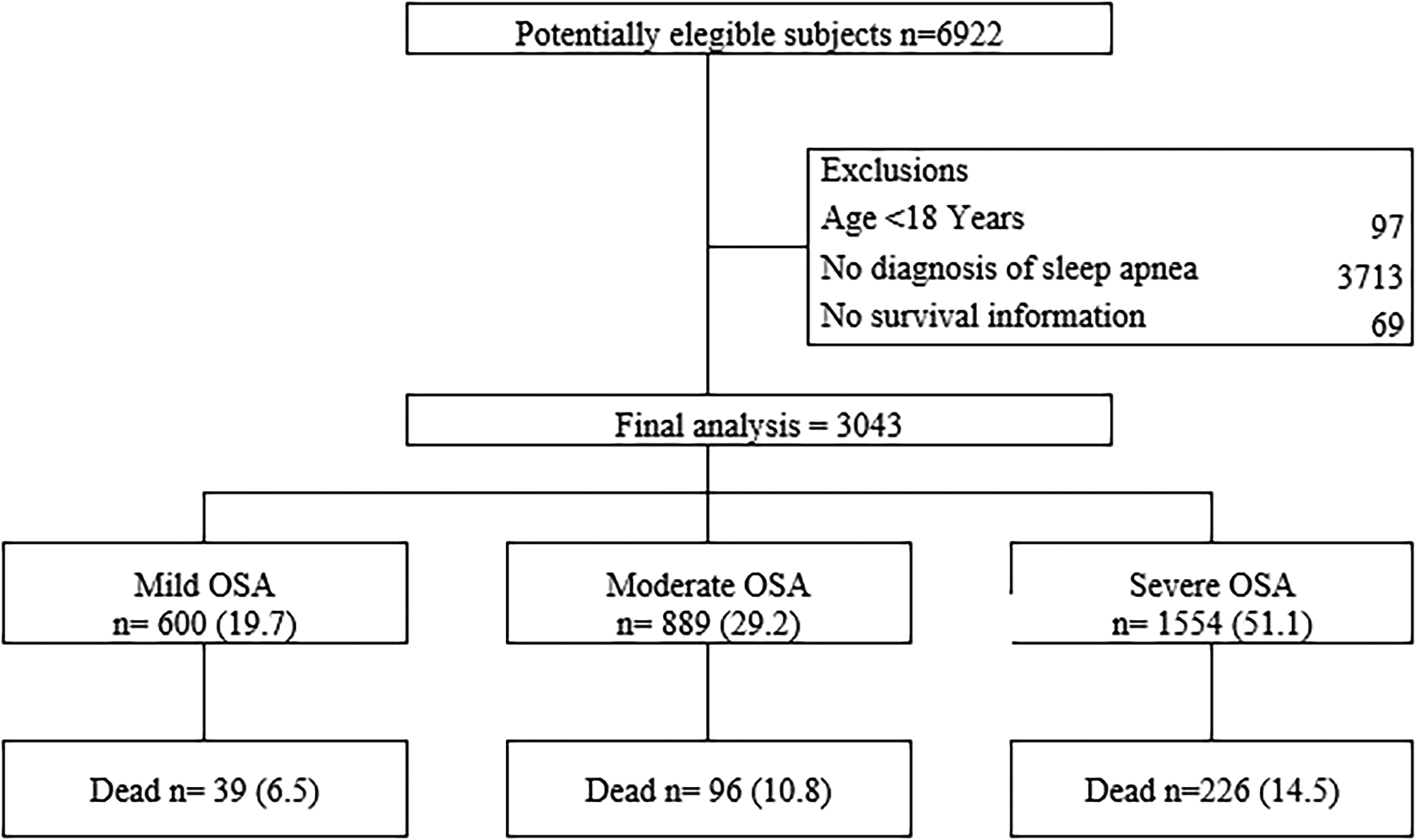
Flowchart of patient enrollment. OSA: obstructive sleep apnea.
Prevalence of comorbidities by OSA severity
In patients with mild OSA, the most prevalent comorbidities were hypertension, present in 48.0% (288/600), and smoking, with a prevalence of 31.5% (189/600). In those with moderate OSA, these prevalences were 53.0% (470/889) and 36.7% (326/889), respectively. In patients with severe OSA, the most frequent comorbidities were hypertension, with a prevalence of 58.5% (909/1554), smoking, with a prevalence of 40.1% (623/1554), and CVD, present in 24.5% (380/1554).
Other comorbidities, such as chronic pulmonary disease, had a prevalence of 17.2% (523/3043) in the study patients. In patients with mild, moderate, and severe OSA, these prevalences were 14.2% (85/600), 16.4% (146/889), and 18.8% (292/1554), respectively. Diabetes had a prevalence of 16.9% (515/3043) in the study patients, with values of 11.8% (71/600) in mild OSA, 17.4% (155/889) in moderate OSA, and 18.6% (289/1554) in severe OSA. The prevalences of comorbidities in the study patients are described in Supplemental Table 2.
Association of comorbidities with severity of OSA.

OSA: obstructive sleep apnea; PVD: peripheral vascular disease; CTD: connective tissue disease; *: stroke sequelae; HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome.
Association between comorbidities and mortality
In patients with mild OSA, the comorbidities with the greatest significant association with mortality were renal failure (OR: 9.39; 95% CI: 3.7–23.84), CVD (OR: 7.73; 95% CI: 3.92–15.21), dementia (OR: 6.98; 95% CI: 2.85–17.11), hemiplegia/stroke sequelae (OR: 6.90; 95% CI: 2.02–23.51), smoking (OR: 5.54; 95% CI: 2.74–11.21), and diabetes (OR: 4.34; 95% CI: 2.02–9.35).
In patients with moderate OSA, the comorbidities with the greatest significant association were hemiplegia/stroke sequelae (OR: 10.11; 95% CI: 3.8–26.89), CVD (OR: 9.77; 95% CI: 6.18–15.46), chronic pulmonary disease (OR: 7.48; 95% CI: 4.76–11.77), and dementia (OR: 6.80; 95% CI: 3.37–13.71).
In severe OSA, the comorbidities with the greatest significant association were dementia (OR: 10.59; 95% CI: 6.41–17.5), leukemia and lymphoma (OR: 7.49; 95% CI: 2–28.1), chronic pulmonary disease (OR: 7.24; 95% CI: 5.33–9.83), hemiplegia/stroke sequelae (OR: 6.33; 95% CI: 3.3–12.16), and renal failure (OR: 6.10; 95% CI: 3.97–9.36). The odds ratios of comorbidities in the study patients are described in Table 2.
The prevalence and strength of the association of comorbidities in patients with OSA were visualized through graphical comorbidity maps (comorbidomes) for study participants (Figure 2) and each severity level (Figures 3–5).

Comorbidome of obstructive sleep apnea (OSA).

Comorbidome of mild obstructive sleep apnea (OSA).

Comorbidome of moderate obstructive sleep apnea (OSA).

Comorbidome of severe obstructive sleep apnea (OSA).
Discussion
This study described and analyzed the comorbidity map of OSA in Colombia, graphically illustrating the relationship between comorbidities and their prevalence at different OSA severity levels. The results showed that, in general, the most prevalent comorbidities were hypertension, smoking, and CVD, with a higher incidence in patients with severe OSA. Additionally, a significant association was observed between some comorbidities and mortality, highlighting conditions such as renal failure and dementia, which showed a strong correlation with the risk of death in patients with OSA at different severity levels. Tumor diseases were associated with severe OSA. These findings highlight the importance of considering demographic factors and comorbidities in the evaluation of risk and clinical management of OSA patients.
CVDs, such as coronary artery disease, heart failure, and AF, reduce the survival of patients with OSA,4,7,10,11 data supported by studies conducted in the Colombian population. 9 Although OSA is an independent risk factor for developing comorbidities, primarily of a cardiovascular nature, there is also a bidirectional relationship between these diseases and OSA. 8 In this study, it was observed that, hypertension, smoking, and CVD were the most prevalent comorbidities, with a higher incidence in those with severe OSA. These findings highlight the relevance of assessing cardiovascular risk in OSA patients, where adequate management and treatment of cardiovascular conditions may be essential to improving survival and quality of life for these patients.4,7,9–11
The increase in BMI contributes to the severity of apnea through several pathophysiological mechanisms, such as the reduction of pharyngeal space and the decrease in the muscular strength of the upper airway.17,18,25,26 Obesity also increases the risk of morbidity, especially in cardio-metabolic diseases, being 4.5 times greater in mild obesity and 14.5 times greater in severe obesity.25,26 Therefore, BMI should be considered a modifiable factor in OSA patients to improve disease progression and associated comorbidities.17,18,25
The prevalence and mortality of OSA increase proportionally with age,26–29 identifying age as an independent risk factor for mortality (HR: 1.05; 95% CI: 1.02–1.07; p < 0.001). 9 Likewise, the prevalence and mortality of moderate to severe OSA also increase with age.9,26–29 Our findings suggest that although advanced age is a key factor for mortality, its impact on OSA also seems to be influenced by coexisting comorbidities. This suggests that age could exacerbate OSA and comorbidities, increasing the risk and severity of each in elderly patients.8,26–29
The prevalence of OSA is two to three times higher in men than in women. 10 In our study, the highest percentage of patients also corresponded to men, reinforcing this trend. The accumulation of visceral fat and central obesity are highlighted as the main pathophysiological mechanisms explaining the higher prevalence of OSA in men.1,3,7,11,19 However, a higher burden of cardiovascular and chronic respiratory diseases could have a more significant impact on men than women, contributing to a greater burden of comorbidities associated with the development of OSA in this group.8,9,11,19,25,26–29
In severe OSA, there is a higher prevalence of tumor diseases compared to what is found in mild and moderate OSA.30–34 This relationship has been associated with tumors such as lung carcinomas, head and neck cancers, brain tumors, colon cancer, among others.30–35 Part of the pathophysiology that may explain this relationship includes prolonged periods of hypoxemia and chronic inflammatory states, which are potential factors for the development of these tumors.30–35
Our findings have significant clinical implications, particularly for risk assessment and early intervention in OSA patients. The strong associations observed between severe OSA and CVDs, renal failure, and malignant or neoplastic diseases highlight the need for comprehensive screening and multidisciplinary management strategies.10,11,25,26,30–34 Identifying high-risk patients based on their comorbidity profiles could facilitate targeted interventions, potentially improving outcomes and reducing mortality.9,26–29 Furthermore, our study underscores the importance of addressing modifiable risk factors such as obesity and smoking, which were highly prevalent among OSA patients. Integrating these findings into clinical practice may contribute to the development of more personalized therapeutic approaches, emphasizing both OSA treatment and the management of its associated comorbidities.11,29,34
Limitations
As a retrospective study conducted in a single institution, the findings may not be fully representative of the population of Colombia, limiting the ability to generalize. However, the sample size obtained is considered sufficient to support the findings presented. The reliance on electronic medical records and clinical databases could have introduced biases related to the quality or availability of information. Although measures were taken to mitigate selection bias, the patients included in the study were those with a confirmed diagnosis of OSA and comorbidities, which may have excluded those with milder or underdiagnosed cases.
The observational design of the study does not allow for describing causality between OSA and comorbidities. While significant associations were identified, the directionality of these relationships remains uncertain. 24 This prevents establishing direct relationships between comorbidities and the progression of OSA or its long-term impact on mortality. 24 Furthermore, the data collection through medical records may have lacked the necessary depth in certain aspects, such as information on previous treatments or control of comorbidities, which could influence the interpretation of the associations. Prospective studies are recommended to investigate etiological relationships between OSA and comorbidities, especially cardiovascular and neoplastic diseases, including a detailed evaluation of treatment adherence.
Conclusion
The most prevalent comorbidities were hypertension, smoking, and CVD, with a higher incidence in patients with severe OSA. Additionally, a significant association was observed between some comorbidities and mortality, highlighting conditions such as renal failure and dementia. Tumor diseases were associated with severe OSA. These findings emphasize the importance of considering demographic factors and comorbidities in the evaluation of risk and clinical management of OSA patients.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251335196 - Supplemental material for Mapping the comorbidome: A novel analysis of the associations between obstructive sleep apnea and its comorbidities in Colombia
Supplemental material, sj-docx-1-sci-10.1177_00368504251335196 for Mapping the comorbidome: A novel analysis of the associations between obstructive sleep apnea and its comorbidities in Colombia by Johan Rincón-Hernández, Eduardo Tuta-Quintero, Kamil Faizal-Gómez, Alirio R Bastidas, Carlos Granados-Burgos, Andrés F Cruz González, Luis P Lesport Castro, Sergio G Torres Riveros, Diego A Rodríguez Barajas, Pablo S Montoya, Laura G Guerrero Carvajal, Valeria M Quimbaya, María A Velásquez Castañeda and Estefanía G Couto Luvie in Science Progress
Footnotes
Acknowledgments
The authors are most thankful for the Universidad de La Sabana.
ORCID iDs
Ethical considerations
The study was conducted in accordance with the principles of the current Helsinki Declaration of 1975, as revised in 2024, as well as local, regional, and international regulations pertaining to clinical research, including Colombian Law on Biomedical Research. Ethical approval was obtained from the Medical Ethics Committee of the Clínica Universidad de La Sabana (approval number: 20211203).
Informed consent
This is a retrospective database analysis study and the consent to participate is waived by the institutional review board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Universidad de la Sabana Grant (MEDESP-4–2025).
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.