
Abstract
Objective
The sensitivity of immune checkpoint inhibitors (ICIs) as monotherapy is low in non-small cell lung cancer (NSCLC) patients with epidermal growth factor receptor (EGFR) exon 20 insertion mutations (ex20ins). This study aims at investigating the effectiveness of the combination of ICI and chemotherapy (ICI-combined regimen) in a real-world population of NSCLC patients harboring near-loop insertions of EGFR exon 20.
Methods
We conducted a retrospective study of advanced NSCLC with EGFR ex20ins from April 2016 to March 2021 at Guangdong Provincial People's Hospital, Southern Medical University, China. A total of 126 cases of EGFR ex20ins were screened from 1610 patients with advanced NSCLC harboring EGFR mutations and 62 cases were further analyzed for different therapeutic efficacy.
Results
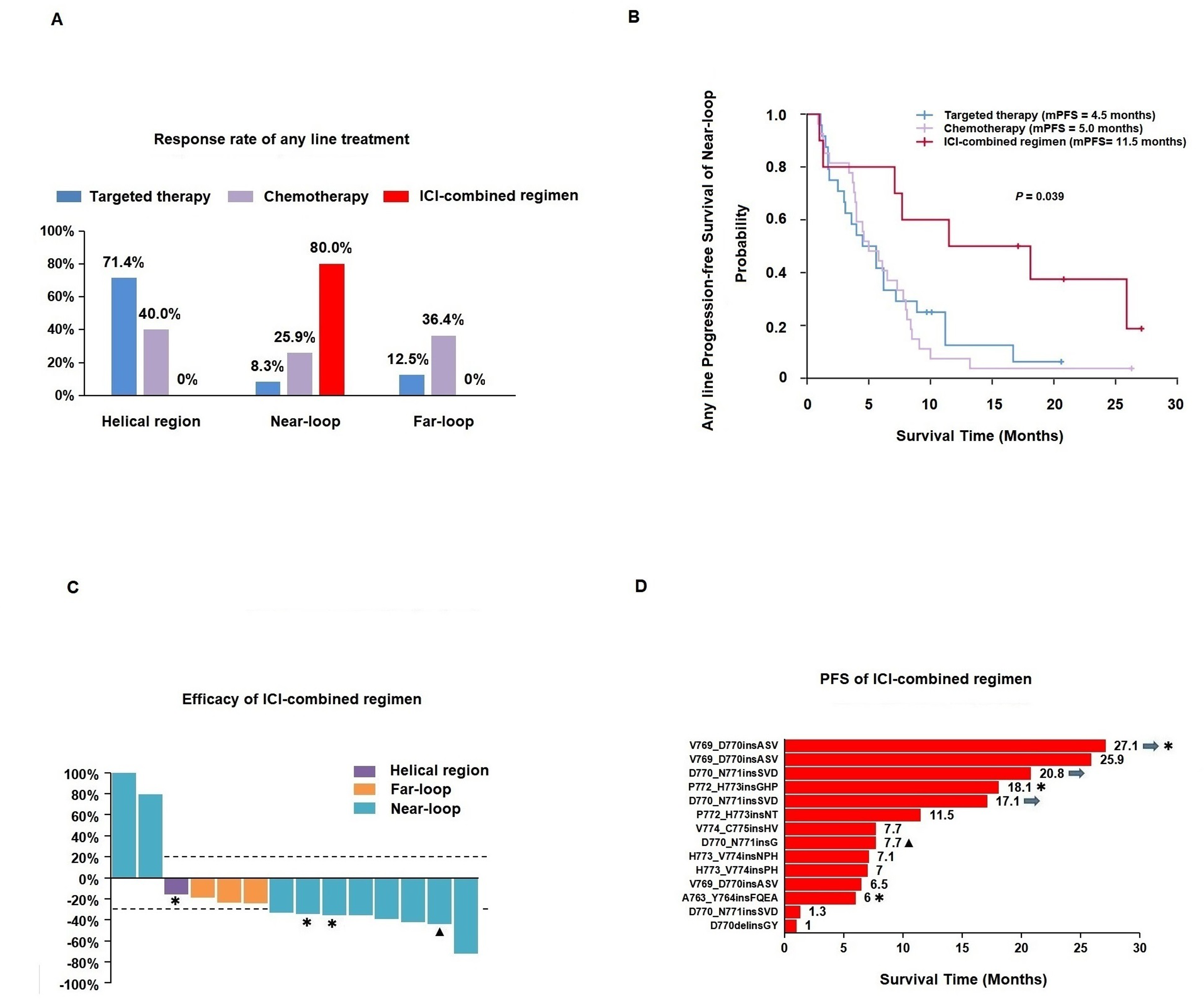
The first-line ICI-combined regimen showed marked efficacy for near-loop insertions of EGFR exon 20, with an ORR of 71.4% and a mPFS of 11.5 months, compared to ORRs of 12.5% for traditional targeted therapy (P = .003) and 18.8% for chemotherapy (P = .013). The first-line mPFS of traditional EGFR-TKIs and chemotherapy were only 5.6 and 5.8 months, respectively. Similar results were observed for any-line therapy of ICI-combined regimen, with an ORR of 80%. The median progression-free survival (PFS) of any-line therapy of ICI-combined regimen was 11.5 months, which were significantly longer than that of traditional targeted therapy (4.5 months, P = .026) and chemotherapy (5.0 months, P = .013).
Conclusions
ICI-combined regimen may be superior compared to targeted therapy and chemotherapy for advanced NSCLC with near-loop insertions of EGFR exon 20. Further exploration is warranted to confirm the efficacy of ICI-combined regimen.
Introduction
Non-small cell lung cancer (NSCLC) is one of the most common malignant tumors worldwide. 1 Epidermal growth factor receptor (EGFR) gene mutations account for approximately 30–50% of lung adenocarcinoma in East Asia. Among these mutations, exon 20 insertion mutations (ex20ins) represent a rare subtype, with an incidence rate of 4–12% in EGFR-mutated advanced NSCLC.2–4 Similar to classical mutations, such as exon 19 deletions and L858R point mutations, which are sensitive to tyrosine kinase inhibitors (TKIs), EGFR ex20ins are also prone to occur in Asian, female, non-smoking and adenocarcinoma populations. There are over 120 different forms of EGFR ex20ins, with only a few are located in the C-helix region (A763-M766). Conversely, more than 90% are found in the loop region, which is further divided into near-loop (A767 to P772) and far-loop (H773 to C775).5,6 The insertion site, sequence and length of EGFR ex20ins are highly diverse. 7 The most common two mutation subtypes are V769_D770insX and D770_N771insX, both located in the near-loop of EGFR exon 20.8–10
The first generation of tyrosine kinase inhibitors (TKIs) shows poor efficacy for EGFR ex20ins (except for A763_Y764insFQEA).11–14 Afatinib and osimertinib may be effective for certain types of ex20ins but evidence from large-scale studies is limited.15–17 One study indicated that the median progression-free survival (mPFS) for first-line therapy of traditional EGFR-TKIs in EGFR ex20ins patients was only 2.0–2.9 months. In contrast, the mPFS for first-line chemotherapy for EGFR ex20ins was 6.4 months, suggesting that chemotherapy may be superior to traditional EGFR-TKIs for this mutation. 18 Novel drugs such as pozitinib, CLN-081, mobocertinib, amivantamab and sunvozertinib have promising efficacy against EGFR ex20ins.19–23 Among these, mobocertinib and amivantamab were approved by the US Food and Drug Administration (FDA) for subsequent-line therapy in 2021. The CHRYSALIS study demonstrated that amivantamab achieved a notable overall response rate (ORR) of 40% and a mPFS of 8.3 months in patients with EGFR ex20ins who had progressed after first-line standard chemotherapy. Despite the promising results of these novel agents for certain EGFR ex20ins subtypes, their availability remains limited.
Immune checkpoint inhibitors (ICIs) have demonstrated good efficacy as first-line therapy for advanced NSCLC patients.24–26 However, patients with EGFR or ALK mutations were excluded from the previous studies of pembrolizumab plus chemotherapy or nivolumab plus ipilimumab in advanced NSCLC. Currently, several studies have shown that the sensitivity to ICI monotherapy is low in advanced NSCLC patients with EGFR ex20ins.27,28 The combination of ICI and chemotherapy (ICI-combined regimen) may be effective for certain patients, as suggested by recent studies. One study reported a median time to treatment discontinuation (mTTD) of 7 months for ICI-combined regimen, which was significantly longer than that of ICI monotherapy. 28 Our previous report also indicated that combining chemotherapy with ICIs may be beneficial for these patients. 29 To date, it remains unclear whether ICI-combined regimen is efficacious for near-loop insertions, the largest subgroup of EGFR ex20ins.
In this study, we conducted a retrospective analysis to compare the efficacy of ICI-combined regimen with other treatment methods in order to identify the most effective treatment approach for advanced NSCLC patients with near-loop insertions of EGFR exon 20.
Materials and methods
Patient selection
We conducted a retrospective study of advanced NSCLC with EGFR ex20ins from April 2016 to March 2021 at Guangdong Provincial People's Hospital, Southern Medical University, China. The reporting of this study conforms to STROBE guidelines. 30 This study adhered to the principles of the Declaration of Helsinki and was approved by the Guangdong Provincial People's Hospital ethics committee. Patient information was collected from hospital records, with all data de-identified to ensure unbiased analysis.
Eligible patients were selected based on the following criteria: aged 18 or older, diagnosed with EGFR ex20ins, and presenting with stage IIIB, IIIC or IV NSCLC, with at least one measurable tumor site according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. 31 Patients were required to receive at least one systemic treatment and undergone at least one follow-up CT scan. Patients were excluded from this study if they declined anti-tumor treatment, harbored other driver gene mutations, participated in clinical trials, had primary organ failure, had incomplete clinical data, or were lost to follow-up were excluded from this study.
EGFR ex20ins mutations were identified using next-generation sequencing technology (NGS), the peptide nucleic acid-locked nucleic acid polymerase chain reaction clamp method (Sanger), or the scorpion amplification refractory mutation system (ARMS) method. These tests were conducted at accredited biotechnology companies or local hospitals on tumor tissues, peripheral blood, or pleural fluid samples. All specimens underwent rigorous quality control, and EGFR testing was performed following standard operating procedures.
Treatment schedule
The treatment regimens were grouped into three categories, regardless of the line of therapy: traditional EGFR-TKIs, chemotherapy, and ICI-combined regimen, with or without bevacizumab. Patients receiving ICIs combined with TKIs, TKIs combined with chemotherapy, ICI monotherapy, or investigational regimens as either first-line or subsequent therapies were excluded from this analysis. All the regimens were prescribed by physicians at our hospital based on the specific conditons of each patient. As was previously reported, each regimen could be analyzed once per patient in a given therapeutic setting, meaning the efficacy results of the above regimens could be evaluated in the same patient across multiple lines of treatment. 28 Treatments were continued until disease progression, unacceptable toxicities, or discontinuation due to personal reasons.
Data collection
Baseline treatment efficacy data for advanced NSCLC patients with EGFR ex20ins were carefully recorded. The therapeutic duration of targeted therapy, chemotherapy, and ICI-combined regimens were also documented in detail. This cohort included 11 patients with EGFR mutations in the C-helix region, 80 patients with far-loop insertions, and 20 patients with near-loop insertions. Gene mutations were analyzed using R software. A waterfall plot was used to display the mutation landscape of the top 30 genes, with mutation types including missense, indel, nonsense, splice, fusion, copy number variation (CNV), and MultiHit mutations.
Tumor response was evaluated according to RECIST criteria. The response rate was defined as the percentage of patients achieving partial response (PR) or complete response (CR). The disease control rate included stable disease (SD), partial response (PR), complete response (CR), or the absence of progressive disease (PD). Progression-free survival (PFS) was defined as the time from the initiation of one of the above three treatment regimens to either PD or death. For patients who were alive without progression at the time of the last follow-up or who were lost to follow-up, data were censored. The cutoff date for PFS data was June 30, 2022, ensuring all patients had been treated for at least 6 months.
Statistical analysis
Statistical analyses were performed using R software (version 3.6.1) and SPSS software (version 26). Differences in PFS across the three treatment settings and associations between marker expression and PFS were analyzed using the Kaplan‒Meier method. The statistical significance of differences between survival curves was assessed using the log-rank test. All tests were two-sided, and P values < .05 were considered statistically significant.
Results
Subtypes of EGFR ex20ins in advanced NSCLC patients
We screened 1610 patients with advanced NSCLC harboring EGFR mutations and identified 126 cases with EGFR ex20ins (7.8%) at Guangdong Provincial People's Hospital between April 1, 2016, and March 31, 2021 (Figure 1

Study design and patient selection flow diagram.
Concomitant mutations of EGFR ex20ins in advanced NSCLC patients
We analyzed the distribution of concomitant mutated genes in patients with EGFR ex20ins. A waterfall plot analysis of the top30 mutations in 111 patients revealed that 59% of the patients had TP53 mutations (Supplemental Figure S2). Mutations in other EGFR sites or CNV alternations accounted for 35% of cases, with 20.4% of these involving CNV variants alongside EGFR mutations. Other frequently observed concomitant mutations included NQO1 (26%), XRCC1(22%), MTHFR (17%), DPYD (14%) and GSTP1 (12%) and UGT1A1 (11%), mainly in the form of missense mutations. TYMS 3R was predominantly altered by indels. CNV alternations were common in genes such as CDK4, CDKN2A, MYC, CCND1, and other genes. The rates of concomitant TP53 mutations were 45%, 59%, and 65% in patients with mutations in the helical region, near-loop, and far-loop regions, respectively. Other concomitant mutations also varied by the EGFR ex20ins regions. For example, GSTP1 mutations were observed only in near-loop insertions (14%) and C-helix regions (18%). Meanwhile, CDKN2A mutations were primarily found in the V769_D770insASV subtype (12.9%) and were absent in the D770_N771insSVD subtype.
Baseline clinicopathologic characteristics of EGFR ex20ins
A total of 75 patients with EGFR ex20ins were included for analysis of clinicopathological characteristics, among whom 62 qualified for the efficacy analysis of various treatment regimens. The clinical characteristics of these patients at baseline are listed in
Clinicopathologic characteristics of patients with EGFR ex20ins.

Abbreviations: EGFR, epidermal growth factor receptor; ex20ins, exon 20 insertion mutations; TMB, tumor mutation burden; ICI, immune checkpoint inhibitor.
Treatment and efficacy of different regimens for EGFR ex20ins
All NSCLC patients in this study received anti-tumor therapies. Among them, 24 (32%) cases received EGFR-targeted therapy, 28 (37.3%) cases received chemotherapy, and 10 (13.4%) cases received ICI-combined regimen as first-line therapy, with or without bevacizumab (Supplemental Table S1). Additionally, 9 (12%) patients participated in clinical trials, and 4 (5.3%) patients received other therapies at diagnosis. Across the entire treatment period, 40 patients with EGFR ex20ins received targeted therapy, 47 received chemotherapy, and 14 received ICIs combined regimen. Targeted therapies included second- and third-generation TKIs, such as afatinib (37.5%, N = 15) and osimertinib (47.5%, N = 19). First-generation TKIs, such as gefitinib and erlotinib, were rarely prescribed, both accounting for only 7.5%. Chemotherapy primarily involved platinum combined with pemetrexed (74.5%, N = 35) or paclitaxel (14.9%, N = 7), with or without bevacizumab. The ICI-combined regimen primarily included pembrolizumab (57.1%, N = 8) or camrelizumab (21.4%, N = 3) combined with standard chemotherapy, pemetrexed, or paclitaxel plus carboplatin. Other ICIs included durvalumab, atezolizumab, and toripalimab, each accounting for 7.1% of cases.
The response rates and median PFS for first-line treatment of advanced NSCLC with EGFR ex20ins did not differ significantly among traditional EGFR-TKIs, chemotherapy, and ICI-combined regimen. The ORRs were 20.8% (95% CI: 3.3–38.4) for traditional EGFR-TKIs, 21.4% (95% CI: 5.2–37.6) for chemotherapy, and 50% (95% CI: 12.3–87.7) for ICI-combined regimen (P > .05). The first-line mPFS were 5.8 months (95% CI: 1.1–10.5), 7.3 months (95% CI: 5.3–9.3), and 7.1 months (95% CI: 6.0–8.2), respectively (

Efficacy results of first-line treatment for EGFR ex20ins.
Efficacy of treatment regimens for different regions of EGFR ex20ins
We further investigated the efficacy of first-line traditional EGFR-TKIs, chemotherapy and ICI-combined regimen in patients with EGFR ex20ins located in different structural regions. Traditional EGFR-TKIs demonstrated superior ORR for insertions in the helical region compared to the near-loop region (50% vs. 12.5%) (
Efficacy results of first-line treatment for near-loop region of EGFR ex20ins.

Note: The P value of response rates: Targeted therapy versus chemotherapy is .64. Targeted therapy versus ICI-combined regimen is .003. Chemotherapy versus ICI-combined regimen is .013. The P value of disease control rates: targeted therapy versus chemotherapy is .081. Targeted therapy versus ICI-combined regimen is .147. Chemotherapy versus ICI-combined regimen is .903. The P value of median PFS: Targeted therapy versus chemotherapy is .36. Targeted therapy versus ICI-combined regimen is .22. Chemotherapy versus ICI-combined regimen is .138.
Abbreviations: EGFR, epidermal growth factor receptor; ex20ins, exon 20 insertion mutations; ICI, immune checkpoint inhibitor; PR, partial response; SD, stable disease; PFS, progression-free survival.
For any-line treatment in patients with helical region insertions, traditional EGFR-TKIs achieved the highest ORR (71.4%, 95% CI: 26.3–100) (
Efficacy results of any-line treatment for EGFR ex20ins.
Efficacy results of any line treatment for near-loop region of EGFR ex20ins.

Note: The P value of response rates: Targeted therapy versus chemotherapy is .109. Targeted therapy versus ICI-combined regimen is <.001. Chemotherapy versus ICI-combined regimen is <.001. The P value of disease control rates: targeted therapy versus chemotherapy is .069. Targeted therapy versus ICI-combined regimen is .039. Chemotherapy versus ICI-combined regimen is .457. The P value of median PFS: Targeted therapy versus chemotherapy is .621. Targeted therapy versus ICI-combined regimen is .026. Chemotherapy versus ICI-combined regimen is .013. Abbreviations: EGFR, epidermal growth factor receptor; ex20ins, exon 20 insertion mutations; ICI, immune checkpoint inhibitor; PR, partial response; SD, stable disease; PFS, progression-free survival.
Efficacy for specific subtypes of EGFR ex20ins
Regarding specific mutation subtypes, traditional EGFR-TKIs achieved the highest ORR for the A763_Y764insX subtype (71.4%, 95% CI: 26.3–100) (Supplemental Figure S4A), while the mPFS was longest with the H773_V774insX subtype (8.3 months, 95% CI: 0–19.0) (Supplemental Figure S4B). The ORRs differed significantly between the D770_N771insX and H773_V774insX subtypes (P = .047). Chemotherapy demonstrated superior efficacy for the V769_D770insX subtype, achieving an ORR of 50% (95% CI: 12.3–87.7) (Supplemental Figure S4C), although the mPFS was shorter than that of other mutation sites (Supplemental Figure S4D). The ORR for the V769_D770insX subtype was significantly higher than that of the H773_V774insX subtype (P = .011).
Discussion
EGFR ex20ins demonstrate primary resistance to first- and second-generation TKIs, with an ORR less than 10%. 32 In this study, we reconfirmed the efficacy of different therapies for EGFR ex20ins. The overall efficacy of traditional EGFR-TKIs observed in this study was higher than in previous studies, mainly due to extensive utilization of osimertinib in our hospital and the potential influence of factors such as the absence of central review or varied CT-scan schedules. However, traditional EGFR-TKIs still failed to show significant efficacy for near-loop and far-loop insertions for any-line treatment. Although mobocertinib and amivantamab have shown favorable efficacy for advanced NSCLC that has progressed on platinum-based chemotherapy, the ORR remained below 43%, with mPFS not exceeding 8.3 months for both agents. Recently data from the PAPILLON study suggested that amivantamab plus chemotherapy may be effective as a first-line treatment for advanced NSCLC with EGFR ex20ins. 33 However, the monotherapy of mobocertinib failed to demonstrate efficacy in the EXCLAIM-2 trial recently, leading to the withdrawal of its approval. The MOON trial showed that there was no significant difference in PFS between patients receiving mobocertinib treatment with near-loop and far-loop insertions. 34 These findings highlight that not all patients benefit from these therapies due to the heterogeneity in EGFR ex20ins.
Recent studies have shown that NSCLC harboring EGFR ex20ins treated with chemotherapy or ICIs as first-line therapy exhibited a similar prognosis as wild-type NSCLC.35,36 In this study, we found that chemotherapy as initial treatment yielded an ORR of 21.4% across all mutation regions of EGFR ex20ins, consistent with previous findings.37,38 Nevertheless, the first-line ICI-combined regimen demonstrated a much higher response rate for near-loop insertions than chemotherapy. Our study also showed that the ICI-combined regimen is effective in second-line or later settings. We further explored factors associated with the efficacy of treatment for EGFR ex20ins. Our study revealed no correlation between PD-L1 expression, TMB levels, or concomitant mutations and treatment response, except for TP53 co-mutations. These co-mutations, occurring in 59% of EGFR ex20ins patients, were associated with shorter survival when treated with targeted therapy.39,40
To date, ICI monotherapy or ICI-combined regimen is not recommended as first-line treatment for advanced NSCLC patients with EGFR ex20ins. Chemotherapy remains the preferred first-line therapy for these patients in most countries. In our study, we observed that the ORR and median mPFS of ICI-combined regimen for advanced NSCLC with EGFR ex20ins in the first-line setting were comparable to those of traditional EGFR-TKIs and chemotherapy. However, ICI-combined regimen was not effective for all patients with EGFR ex20ins. For example, it showed minimal efficacy for helical or far-loop insertions, confirming the heterogeneity in treatment response among different EGFR ex20ins subtypes. The tumor immune microenvironment is closely related to the efficacy of immunotherapy for EGFR ex20ins, as was indicated in our previous study. 41 The specific structural characteristic of EGFR ex20ins may also contribute to this variability, warranting further investigation.
Previous studies have suggested that ICIs and chemotherapy may work synergistically to kill cancer cells, as chemotherapy may enhance immune response by increasing PD-L1 expression and altering the tumor immune microenvironment.42–44 In this study, different subtypes of EGFR ex20ins demonstrated varying sensitivities to ICI-combined regimen. Near-loop insertions, in particular, were more sensitive to this combined therapy, showing significantly higher ORRs and longer mPFS in any-line settings. For first-line treatment, ICI-combined regimen also demonstrated a significantly higher ORR for near-loop insertions. However, compared to chemotherapy and traditional EGFR-TKIs, the improvement in mPFS for first-line ICI-combined regimen did not reach statistical significance, mainly due to the small sample size in the ICI-combined regimen group. Large studies may further confirm the PFS benefit of ICI-combined regimen.
This study underscores the efficacy differences among ICI-combined regimen, chemotherapy and traditional EGFR-TKIs for advanced NSCLC with near-loop insertions of EGFR exon 20. In the future, large clinical studies will be necessary to confirm the efficacy of ICI-combined regimen for this specific subset of patients. However, this study has several limitations. Firstly, this was a single-center investigation, with a relatively small sample size of EGFR ex20ins cases, which may limit the statistical power of some comparisons. Secondly, confounding factors, such as variations in treatment lines and drug types within each treatment category, may have influenced the results. In addition, selection bias may occur in our study. Among patients included for analysis of clinicopathological characteristics, some were not included for efficacy comparison because they received other first-line treatments or participated in clinical trials. Finally, our study did not include patients treated with novel agents such as mobocertinib and amivantamab, as these drugs were not routinely available during the study period.
Conclusions
NSCLC with EGFR ex20ins demonstrates varying responses to ICI-combined regimens, chemotherapy and traditional EGFR-TKIs. ICI-combined regimen may be superior in advanced NSCLC with near-loop insertions of EGFR exon 20. Further large-scale studies are needed to confirm the efficacy of ICI-combined regimens for these patients.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251325406 - Supplemental material for The combination of immune checkpoint inhibitor and chemotherapy may be efficacious for advanced non-small cell lung cancer with near-loop insertions of EGFR exon 20: A retrospective analysis
Supplemental material, sj-docx-1-sci-10.1177_00368504251325406 for The combination of immune checkpoint inhibitor and chemotherapy may be efficacious for advanced non-small cell lung cancer with near-loop insertions of EGFR exon 20: A retrospective analysis by Ke-Jun Liu, Hong-Rui Li, Quan-Quan Tan, Tao Jiang, Kai-Cheng Peng, Hua-Jun Chen, Qing Zhou, Xu-Chao Zhang, Zheng Zheng, Shi-Yuan Chen, Xue Zheng, Hong-Bo Zheng, Bei-Bei Mao, Long-Long Gong, Xian-Wen Chen, Wendy Wu, Yi-Long Wu, Jun Jia and Jin-Ji Yang in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504251325406 - Supplemental material for The combination of immune checkpoint inhibitor and chemotherapy may be efficacious for advanced non-small cell lung cancer with near-loop insertions of EGFR exon 20: A retrospective analysis
Supplemental material, sj-docx-2-sci-10.1177_00368504251325406 for The combination of immune checkpoint inhibitor and chemotherapy may be efficacious for advanced non-small cell lung cancer with near-loop insertions of EGFR exon 20: A retrospective analysis by Ke-Jun Liu, Hong-Rui Li, Quan-Quan Tan, Tao Jiang, Kai-Cheng Peng, Hua-Jun Chen, Qing Zhou, Xu-Chao Zhang, Zheng Zheng, Shi-Yuan Chen, Xue Zheng, Hong-Bo Zheng, Bei-Bei Mao, Long-Long Gong, Xian-Wen Chen, Wendy Wu, Yi-Long Wu, Jun Jia and Jin-Ji Yang in Science Progress
Footnotes
Abbreviation
Acknowledgments
We would like to thank doctors, nurses, patients, and their family members engaged in this study for their kindness to support our work. We also thank colleagues for their kind technical help, psychological support, theoretical guidance, and writing assistance during the present study.
Authors’ contributions
Jin-Ji Yang, Jun Jia and Yi-Long Wu designed the investigation and contributed to writing the paper. Hua-Jun Chen, Qing Zhou, Xu-Chao Zhang, Zheng Zheng and Xue Zheng designed the investigation and supervised the study. Kai-Cheng Peng, Hong-Bo Zheng, Bei-Bei Mao and Long-Long Gong performed the investigation. Shi-Yuan chen, Xian-Wen Chen and Wendy Wu provided essential assistance and analyzed data. Jin-Ji Yang, Ke-Jun Liu, Hong-Rui Li, Tao Jiang and Quan-Quan Tan designed and performed the research, analyzed data and wrote the paper. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the work presented in the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval
The present study was approved by the Ethics Committee of Guangdong Provincial People's Hospital (Guangzhou, China), Ethical approval number: 2019-217H-2.
Funding
This study was supported by funding from the National Natural Science Foundation of China (grant number 81972164), the Provincial Natural Science Foundation of Guangdong Province, China (grant number 2019A1515010931), and the High-Level Hospital Construction Project (grant number DFJH201809). This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
National Natural Science Foundation of China, (grant number 81972164).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.