
Abstract
Objective:
In this study, we aimed to elucidate the potential association between H. pylori infection and the prevalence of hypertension in the Inner Mongolia population, while also exploring the impact of sex and age on the relationship between helicobacter pylori and hypertension.
Method:
We collected physical examination data from a cohort of 10,517 patients at the Second Affiliated Hospital of Baotou Medical College between January and December 2020. The patients were categorized into three groups based on their blood pressure and H. pylori infection status. Our findings revealed a significant correlation between H. pylori infection and blood pressure levels in the patients.
Result:
The infection rate of H. pylori was higher in patients with hypertension compared to those without hypertension. Additionally, sex and age exerted an influence on the association between helicobacter pylori and hypertension. Among the hypertensive patients, males displayed a greater likelihood of H. pylori infection and more severe infections than females. Furthermore, within the hypertensive patients infected with H. pylori, the degree of infection was lower in young adults compared to middle-aged adults and the elderly.
Conclusion:
Hypertension is associated with Helicobacter pylori infection.
Introduction
Hypertension, a prevalent cardiovascular disease with a high fatality rate, still lacks a detailed understanding of its pathophysiological mechanism. In recent years, the influence of inflammation on hypertension has gained significant attention. 1 Inflammatory responses not only contribute to the development of hypertension but also increase the risk of other cardiovascular diseases, such as stroke and heart failure. 1 Currently, the prevalence of hypertension in China has reached 23%. 2 Therefore, it is necessary to study the detailed mechanisms underlying hypertension. The prevalence of H. pylori in the Chinese population was higher than that in the Asian population (55.8% vs. 44.7%) probably due to the fecal-oral route of transmission and the common dietary pattern in China3–6. Recent studies have shown that inflammation is associated with hypertension, which is reminiscent of whether hypertension is associated with H. pylori infection, and whether there are differences in the prevalence of H. pylori infection in different populations. Numerous researchers have discovered a close association between inflammatory responses caused by intestinal dysbiosis and H. pylori infection and hypertension. Dysbiosis of intestinal flora leads to the production of short-chain fatty acids and corticosterone, which promote the development of hypertension.7–9 This avenue may provide insights into the mechanisms of hypertension. H. pylori may be associated with sodium retention, vascular endothelial damage, insulin resistance, disorders of lipid metabolism, and altered intestinal flora, all of which potentially contribute to elevated blood pressure and the severity of hypertension.10–14 A cross-sectional study by Wang et al. found a positive correlation between the prevalence of H. pylori infection and hypertension. 15 Xiong et al. further revealed that H. pylori infection not only affects the incidence of hypertension but also leads to a higher infection rate in hypertensive individuals compared to those with normal blood pressure. 16 Consequently, we investigated the association between hypertension and H. pylori by collecting various indicators from a physically examined population in Baotou City, Inner Mongolia, China. Through this study, the relationship between hypertension and H. pylori infection rate was verified, and the differences in different sex and age groups were analyzed, to provide a basis for further research on the correlation and influencing mechanism between hypertension and H. pylori. Future studies can refer to this study to exclude relevant influencing factors.
Subjects and methods
Our study was retrospective and in accordance with the 1975 Declaration of Helsinki (revised in 2013). Its reporting conforms to STROBE guidelines. 17
Study design and grouping criteria
We collected data from 10,517 patients who underwent physical examinations at the Second Affiliated Hospital of Baotou Medical College from January to December 2020. All participants were informed of the study's purpose and provided informed consent. 16 (In terms of sample size, we did not calculate the sample size by formula, but all the people who met the sample during this period were included in the study). Inclusion criteria: 14C breath test, blood pressure measurement, age, and past medical history were recorded. People who took antibiotics and proton pump inhibitors in the past two weeks, and those with serious liver and kidney diseases, serious blood diseases, malignant tumors, and autoimmune diseases were excluded. All patients underwent 14C breath tests and blood pressure measurements. Based on their blood pressure status, participants were divided into hypertensive and normotensive groups. Within the hypertensive group, individuals were further categorized into those with and without H. pylori infection. Sex-based divisions were made for both hypertensive and normotensive populations, and age-based divisions included young, middle-aged, and elderly groups. (We defined the age group between 20 and 40 years as young, 41–65 years as middle-aged, and over 66 years as elderly).
Evaluation of hypertension
Blood pressure measurements were conducted using a reliable electronic sphygmomanometer (automatic sphygmomanometer HPP-9020). Prior to measurement, participants were required to refrain from smoking, drinking tea or coffee, empty their bladder for at least 30 min, and then sit in a quiet environment for at least 5 min to ensure complete relaxation. The average value of three measurements was recorded as the test result. 18 Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg.
Assessment of Helicobacter pylori inion
The presence of H. pylori infection was determined by a 14C breath test in the examined population. Participants were tested on an empty stomach or two hours after eating, and they orally consumed one urea [14C] capsule. After 15 min, the H. pylori tester HUBT-20A was used to measure the breath test results, expressed as 20-min DPM (disintegrations per minute). Results equal to or greater than 100 were considered positive for H. pylori infection.
Covariate measurement
During blood pressure measurements, the patient's age, sex, and past medical history were recorded. Designated professional physicians recorded and uploaded the data, simultaneously making corresponding diagnoses. The laboratory department of the hospital employed an automatic blood cell analyzer BC-6800PLUS to measure blood routine examination parameters (white blood cells, red blood cells, neutrophils, etc.). The Sysmex UF-50 urine sediment analyzer was used to detect urea, uric acid (UA), and creatinine (CREA). Automatic biochemical immunoassay CoBAS 8000 was employed to measure fasting plasma glucose (FPG), triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total bilirubin (TBil), direct bilirubin (DBil), alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyltransferase (GGT), globulin (GLb), and albumin/globulin ratio (A/G).
Informed consent was obtained from all participants, who signed the relevant informed consent form. Ethical approval was granted for the study (approved by the Ethics Committee of the Second Affiliated Hospital of Baotou Medical College, LW-014).
Data analysis
All data were analyzed using SPSS version 26.0. Measurement data with a normal distribution were expressed as means ± standard deviation (x ± s), and a t-test was employed for between-group comparisons. For example, urea, creatinine, and other indicators with specific numerical expression. Numerical data were presented as percentages such as sex, urinary protein, Helicobacter pylori infection status, and hypertension grade. The chi-square test was used for these indicators. For multi-group comparison, P values were derived from one-way ANOVA (continuous variables) or Chi-square test (categorical variables). All tests were two-sided, and p values < 0.05. Graphs were prepared in Graphpad Prism (version 7).
Results
Comparison of various clinical indicators between hypertensive and non-hypertensive populations in Inner Mongolia
A total of 10,517 physical examination subjects were included in this study, with 3335 diagnosed with hypertension, accounting for 33.3% of the examined population (Figure 1). The number of patients infected with H. pylori was 2,815, representing 28.1% of the total population. After excluding patients who did not complete all examinations, the remaining sample consisted of 9363 cases. Among them, 3015 had hypertension and 2599 were infected with H. pylori. The screened population was divided into hypertensive and normotensive groups, with 2044 patients in the hypertensive group after excluding those with white coat hypertension. Using SPSS, we randomly selected 2044 normotensive patients (without any other diseases) as the control group. The differences in clinical indices between the two groups were analyzed using SPSS. The population was divided into hypertensive and normotensive groups, and the differences in examined population indicators were analyzed. Significant differences were observed between the hypertensive and normotensive populations in terms of age, sex, urea, uric acid (UA), creatinine (CREA), urine protein, fasting blood glucose (FPG), triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), total bilirubin (TBil), direct bilirubin (DBil), indirect bilirubin (IBil), alanine aminotransferase (ALT), γ-glutamyltransferase (GGT), globulin (GLB), white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), platelets (PLT), lymphocytes, neutrophils, monocytes, and the infection rate of H. pylori (see Table 1). The infection rate of H. pylori in the hypertensive group was higher than that in the normal blood pressure group (29.16% vs. 25.44%, p < 0.05).

The detailed protocol of category volunteers.
Characteristics between the hypertensive group and non-hypertensive group.

Note: Crea: Creatinine; FPG: fasting blood-glucose; TG: triglyceride; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; TBil: total bilirubin; Dbil: direct bilirubin; IBil: indirect bilirubin; GGT: γ-glutamyltransferase; ALT: alanine aminotransferase; TP: total protein; ALB: albumin; GLB: globulin; A/G: ratio of albumin to globulin; WBC: white blood cell; RBC: red blood cell; Hb: hemoglobin; PLT: platelet; EOS: eosinophilic granulocyte; B: basophilic granulo there is helico differencesori Legethereise some difference bedifferencesrtensive people and the normotensive people in the prevmeane of H. pylori infection, m, mean age, sex composition, n and other clinical indicators.
Differences in the prevalence of H. pylori infection between men and women in a hypertensive population
The hypertension group was divided by sex, including 721 females and 1323 males. We selected 721 females as one group and randomly selected 721 males from the 1323 male population. After analysis with SPSS, no statistical difference was found between the two groups, except for hypertension level and A/G. Among the female hypertensive patients, 188 were infected with H. pylori, while among the male hypertensive patients, 224 were infected. The prevalence of H. pylori infection was higher in male hypertensive patients than in female hypertensive patients (31.07% vs. 26.07%, p = 0.036) (Figure 2).

Differences in the prevalence of Helicobacter pylori infection in male versus female hypertensive patients.
Differences in clinical indicators between men and women in a population with hypertension co-infected with H. pylori
Among them, 596 patients had hypertension and H. pylori infection. They were divided into groups based on sex, with 188 females and 188 males (randomly selected from a total of 408 cases using SPSS). Statistical analysis showed significant differences in diastolic blood pressure (DBP), urea, creatinine (Crea), uric acid, urine protein, fasting blood glucose (FPG), total cholesterol (TC), HDL-C, total bilirubin (TBil), direct bilirubin (DBil), indirect bilirubin (IBil), γ-glutamyltransferase (GGT), albumin (ALB), globulin (GLB), A/G ratio, white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), platelets (PLT), neutrophils, monocytes, eosinophils, and the infection degree of H. pylori(The degree of H. pylori infection was divided into according to the 14C breath test. 1:0-60 2:61-120 3: > 120) between the two groups (Table 2, Figure 3).
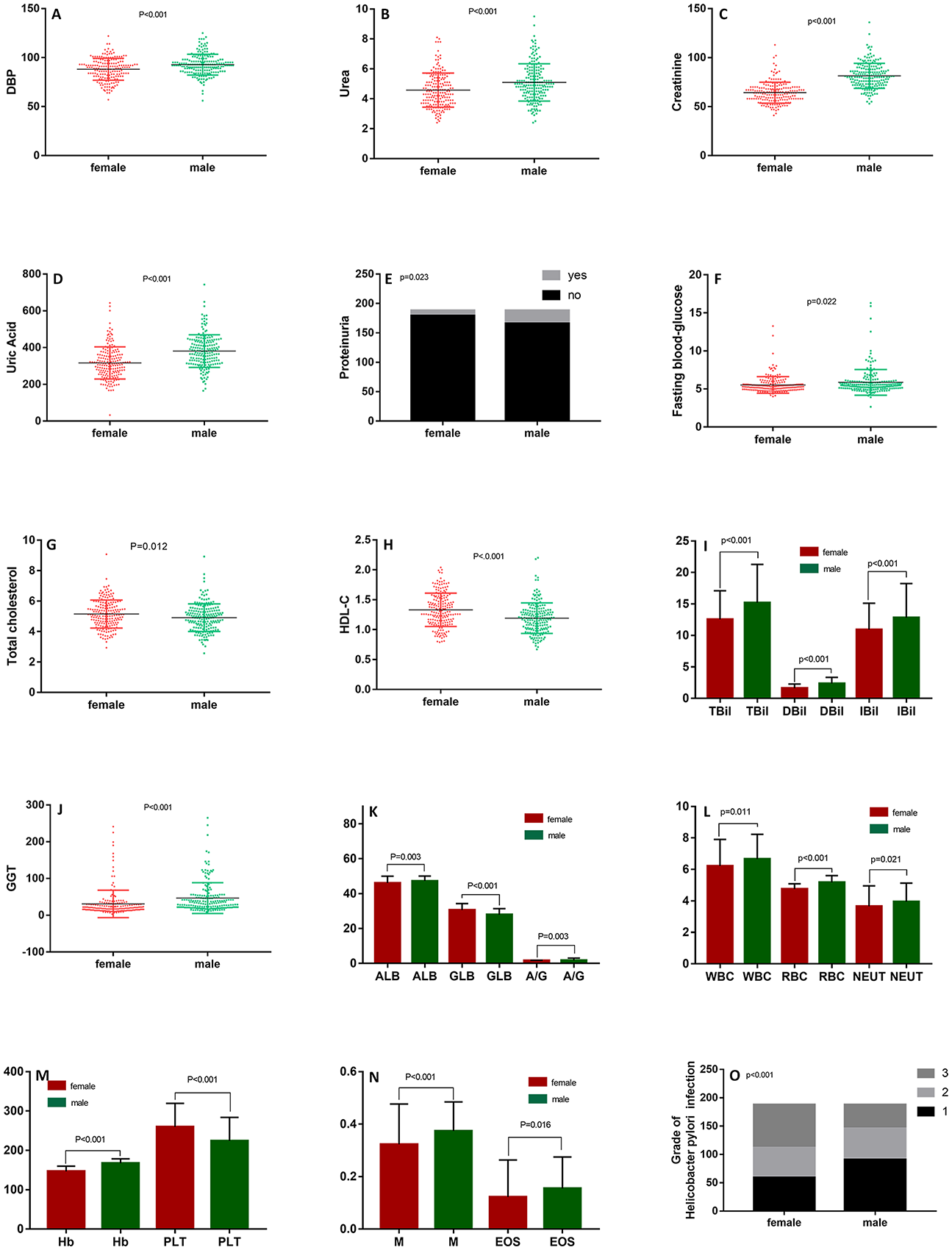
Characteristics between men and women in hypertensive combined with H. pylori populations.
Characteristics between males and females in hypertensive combined with H. pylori populations.

Note: Crea: Creatinine; FPG: fasting blood-glucose; TG: triglyceride; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; TBil: total bilirubin; Dbil: direct bilirubin; IBil: indirect bilirubin; GGT: γ-glutamyltransferase; ALT: alanine aminotransferase; TP: total protein; ALB: albumin; GLB: globulin; A/G: ratio of albumin to globulin; WBC: white blood cell; RBC: red blood cell; Hb: hemoglobin; PLT: platelet; EOS: eosinophilic granulocyte; B: basophilic granulocyte Hp: helicobacter pylori.
Effect of age on the relationship between H. pylori and hypertension
Variation in H. pylori infection rates among young, middle-aged, and elderly patients with hypertension
The hypertensive group was divided into three age groups: young, middle-aged, and elderly. The young group consisted of 372 patients, the middle-aged group had 1330 patients, and the elderly group included 342 patients. We randomly selected 342 patients from each group as the final study subjects. Statistical analysis using SPSS showed that among these study subjects, 100 young patients, 98 middle-aged patients, and 109 elderly patients were infected with H. pylori, accounting for 29.24%, 28.65%, and 31.87% of the population in each group, respectively. However, there was no statistical difference in the H. pylori infection rate (Figure 4).

Prevalence of H. pylori infection in young, middle-aged, and elderly people. Legend: In the hypertensive population, the highest rate of H. pylori infection was 37.87% in those aged 65–99 years, followed by 29.24% in those aged 20–40 years and the lowest rate of 28.65% in those aged 41–65 years, but this difference was not statistically significant.
Clinical indicators in young, middle-aged, and elderly individuals with co-infection of H. pylori in the hypertensive population
According to the aforementioned age grouping method, the patients were divided into three categories: young, middle-aged, and old. Among them, there were 110 young patients, 377 middle-aged patients, and 109 elderly patients. After excluding other diseases, we randomly selected 109 patients from each age group the young group, middle-aged group, and elderly group. After statistical analysis, significant differences were observed among the three groups in terms of systolic blood pressure (SBP), DBP, urea, uric acid, triglycerides (TG), alanine aminotransferase (ALT), γ-glutamyltransferase (GGT), albumin (ALB), globulin (GLB), A/G ratio, WBC, RBC, Hb, PLT, lymphocytes, neutrophils, monocytes, basophilic granulocytes, and the degree of H. pylori infection (Table 3). The expression levels of urea, ALT, ALB, RBC, Hb, and PLT differed significantly between the young and middle-aged groups, middle-aged and elderly groups, and young and middle-aged groups (p < 0.05). Differences in SBP, DBP, GGT, GLB, and A/G ratio were mainly observed between the young and elderly groups and between the middle-aged and elderly groups (p < 0.05). Uric acid, TG, WBC, lymphocytes, neutrophils, basophilic granulocytes, and monocytes showed significant differences between the young and middle-aged groups and between the young and elderly groups (p < 0.05). The difference in monocyte levels was only observed between the young and middle-aged groups (p = 0.009). Regarding H. pylori test results, the infection level was lower in the young population compared to the middle-aged population (196.39 ± 91.34 vs. 239.49 ± 125.16, p < 0.01), and also lower in the young group compared to the elderly group (196.39 ± 91.34 vs. 273.84 ± 157.93, p < 0.001).
Description of the characteristics of people of different ages with hypertension combined with H. pylori.
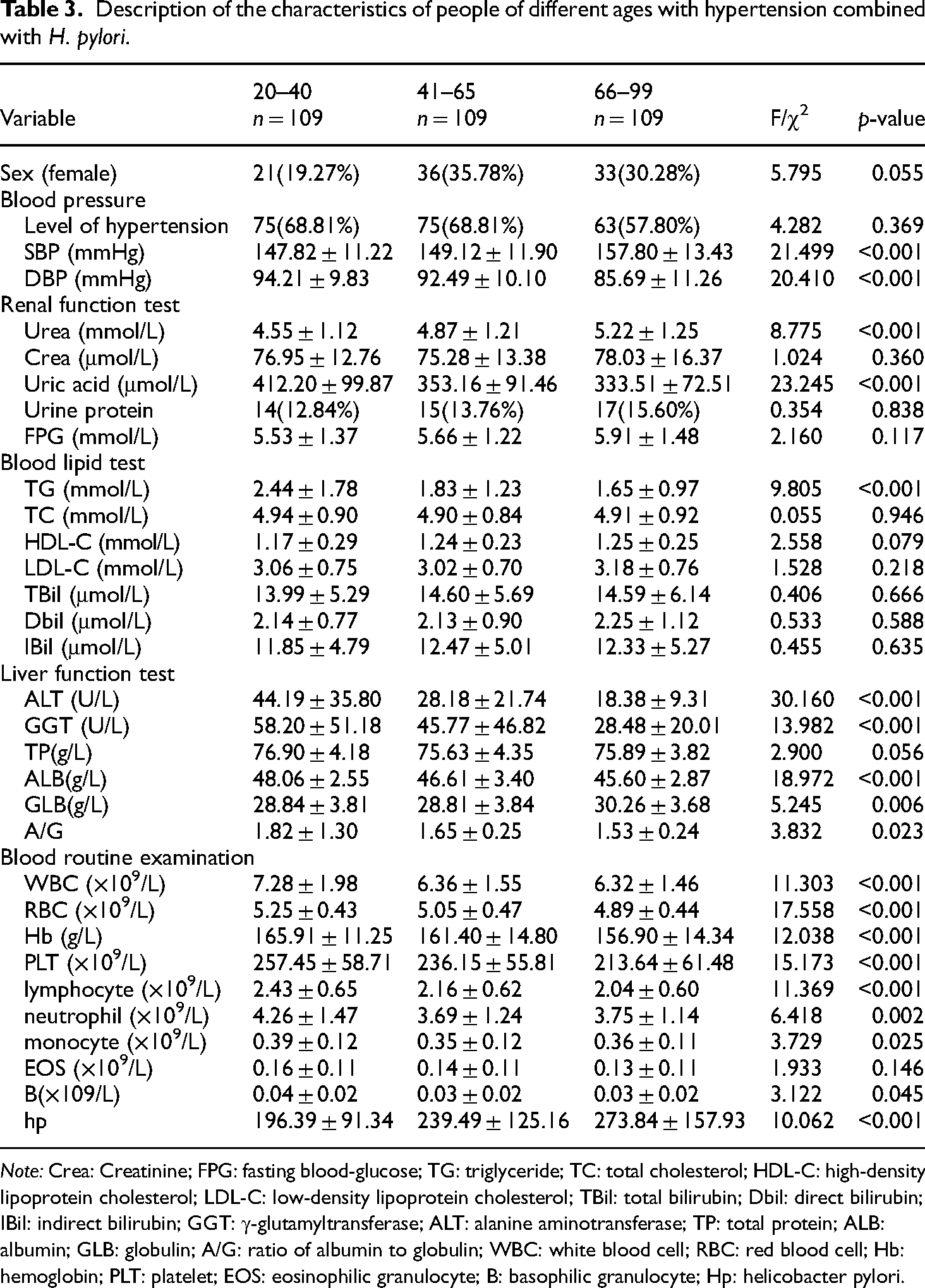
Note: Crea: Creatinine; FPG: fasting blood-glucose; TG: triglyceride; TC: total cholesterol; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; TBil: total bilirubin; Dbil: direct bilirubin; IBil: indirect bilirubin; GGT: γ-glutamyltransferase; ALT: alanine aminotransferase; TP: total protein; ALB: albumin; GLB: globulin; A/G: ratio of albumin to globulin; WBC: white blood cell; RBC: red blood cell; Hb: hemoglobin; PLT: platelet; EOS: eosinophilic granulocyte; B: basophilic granulocyte; Hp: helicobacter pylori.
Discussion
Through this cross-sectional study, we have discovered a significant association between H. pylori infection and hypertension. Patients with H. pylori infection exhibited higher systolic blood pressure (SBP), diastolic blood pressure (DBP), and a higher prevalence of hypertension compared to those without H. pylori infection. Furthermore, we observed differences in the prevalence and severity of H. pylori infection between males and females, with males showing higher rates and more severe infections. Age also played a role, with higher H. pylori infection rates in the elderly and middle-aged patients compared to young patients.
The overall incidence of H. pylori infection in our study was 28.1%, which is lower than in other studies. For instance, a cross-sectional study in Wuhan, China, reported an H. pylori infection rate of 32.6% among healthy people. 14 The prevalence of H. pylori infection is influenced by regional factors and is strongly associated with family size, education level, lifestyle habits, and income level. 19 Our analysis revealed a higher prevalence of H. pylori infection in the hypertensive population compared to the normotensive population (29.16% vs. 25.44%). This finding aligns with the results of a previous study. 20 However, early studies on H. pylori and metabolic syndrome did not find a significant association with blood pressure. 21 It is worth noting that these studies used serological indicators to determine H. pylori infection, which may have lower sensitivity and specificity compared to the urea breath test (UBT), currently recognized as the gold standard for H. pylori detection. 22 . Significant differences were observed in age and sex between the hypertensive and normal blood pressure groups. Data from the National Health and Nutrition Examination Survey also indicate sex and age differences in hypertension control. 23
We also identified differences in the prevalence of H. pylori infection between males and females. The infection rate and severity of H. pylori were higher in males than in females. This finding is consistent with the studies conducted by Sun and Chen, which also reported a sex-related association with H. pylori infection.24,25 Males and females exhibit variations in intragastric acidity and plasma gastrin concentration profiles, which may influence H. pylori infection. 26 Xiong and other researchers found a correlation between H. pylori infection and elevated blood pressure. 16 Upon H. pylori infection, the body produces proteins involved in cytotoxic immune responses, leading to the generation of H. pylori antibodies. These antibodies cross-react with antigens on blood vessel walls, triggering the release of inflammatory factors that stimulate vascular walls. This immune response affects microvascular systolic and diastolic functions, with the release of IL-8 activating norepinephrine. Disturbed immune responses to H. pylori infection result in vasoconstriction and endothelial dysfunction, impacting blood pressure regulation.27,28 The expression of IL-8 varies between sex, often exhibiting a protective effect in women but a risk factor in men. 29 This may explain the higher H. pylori infection rate and severity observed in males. Further analysis of clinical indicators in hypertensive patients with H. pylori infection revealed that females had higher levels of high-density lipoprotein cholesterol (HDL-C) compared to males. This may be attributed to the influence of H. pylori on lipid profiles, which may vary by sex. 30
Among hypertensive patients with H. pylori infection, age played a significant role in the severity of infection. The degree of H. pylori infection was lowest in young individuals (<40 years old) compared to middle-aged and elderly individuals. Wenjun and other scholars found that people over 40 years of age in China are more likely to develop homocysteinemia, 31 a condition in which H. pylori infection may play a role. H. pylori infection may decrease the absorption of folic acid and vitamin B12, leading to increased levels of homocysteine (Hcy). Elevated Hcy levels damage the vascular endothelium and stimulate collagen fiber synthesis, smooth muscle cell proliferation, and elastic fiber degradation in the vascular wall, resulting in vascular remodeling. Additionally, Hcy inhibits nitric oxide secretion by endothelial cells, leading to platelet aggregation and vasoconstriction. Endothelial damage also increases the levels of cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2), promoting prostaglandin production, platelet aggregation, and the development of ischemic heart disease.16,28,32. However, the rate of H. pylori infection in hypertensive individuals did not show a significant association with age. Some studies have reported that H. pylori infection rates increase with age up to a certain point (around 36 years old), after which the prevalence does not vary significantly with age. 19
While our study had a large sample size and comprehensive statistical analysis, establishing a clear causal relationship between H. pylori and hypertension requires further experiments. Our study did not include the height, weight, and lifestyle habits of the study population, which have been shown in previous studies to be associated with H. pylori infection. For instance, studies have found that individuals with H. pylori infection tend to have higher body mass index (BMI) compared to those without H. pylori infection.33–35 In this study, we found that there were significant differences in age, sex, Renal function test, FPG, Blood lipid test, Liver function test, and Blood routine examination between hypertensive and non-hypertensive people. We did not examine the possible reasons for these differences or whether these factors also affect the rate of H. pylori infection, which is a limitation of our study. In addition, our study had limitations in the diagnostic criteria for hypertension and H. pylori infection. Diagnostic criteria for hypertension are recommended that 2–3 visits be made to confirm hypertension in patients. Since this study was a retrospective study and the study population was a physical examination population, the study subjects could not be required to visit the doctor 2–3 times. Although 14C breath tests are currently used as the clinical standard for Helicobacter pylori infection, according to the studies of other scholars, compared with the gold standard examinations such as histology, 14C breath tests have a certain degree of false negative, and some patients may be infected with Helicobacter pylori but this test is negative.36,37 These errors will inevitably affect our study, which is the weakness of this study. The correlation between H. pylori infection and alcohol consumption and smoking in daily life remains debated among scholars. Some studies suggest that moderate alcohol consumption may reduce H. pylori infection,38,39 while others conclude that alcohol can damage the gastric mucosa or enhance H. pylori adherence, promoting infection. The relationship between alcohol consumption, smoking, and H. pylori infection may also vary by sex, with both alcohol consumption and smoking being risk factors for males but not females.40,41. Further research and analysis are needed to clarify the correlation between H. pylori infection and alcohol consumption and smoking, which were not addressed in our study. In conclusion, this study provides a foundation for conducting further research on the association and mechanism of influence between hypertension and H. pylori. The current study may be used as a reference for future studies to exclude relevant influencing factors.
Conclusion
This study confirms the association between H. pylori infection and hypertension. Among individuals with established hypertension, males are more likely to be infected with H. pylori and exhibit more severe infections. Additionally, H. pylori infection is less prevalent in younger individuals. Therefore, male middle-aged and elderly patients with hypertension and H. pylori infection should receive increased attention and timely treatment.
Summary: This study adds to the existing knowledge by establishing a significant association between H. pylori infection and hypertension. It highlights the sex and age differences in H. pylori infection rates and severity among hypertensive individuals. The study also emphasizes the need for further research to explore the causal relationship between H. pylori and hypertension, as well as the impact of lifestyle factors on H. pylori infection.
Supplemental Material
sj-docx-1-sci-10.1177_00368504251320300 - Supplemental material for Helicobacter pylori and hypertension-a cross-sectional study based on a healthy population
Supplemental material, sj-docx-1-sci-10.1177_00368504251320300 for Helicobacter pylori and hypertension-a cross-sectional study based on a healthy population by Ping Yang, Wei Shi, Hai Liu, Chi Wang, Xianbin Wang, Zengshuai Wang, Guanrong Huang and Guanhua Huang in Science Progress
Footnotes
Acknowledgement
The authors would like to express thanks to the patients and their families for their long-term cooperation. We also thank all the authors for their work on this study. Our manuscript has a preprint and DOI of the preprint is 10.21203/rs.3.rs-2634360/v1.
Author contribution
This study was proposed by Guanhua Huang who was responsible for the overall coordination, with Ping Yang in charge of paper writing, We Shi in charge of statistical guidance, Chi Wang in charge of research scheme design, Hai Liu in charge of data collation, Xianbin Wang and Zengshuai Wang in charge of data collection, and Guanrong Huang in charge of results analysis.
Consent
We hereby declare by signing below that this manuscript is original, has not been published before, and is not currently under consideration for publication elsewhere. We confirm that the manuscript has been read and approved by all named authors, and that there are no others who meet the criteria for authorship but are not listed. We further confirm that the order of authorship as listed in the manuscript has been approved by all of us.
Data availability statement
Data is available on request from the authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations and consent
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Baotou Medical College, No. LW-014, on January 4, 2020.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Research Project of Higher Education Institutions in the Inner Mongolia Autonomous Region (grant number (NJZY22069)).
Patient consent
Consent for this study has been obtained from all participants. Our study subjects are adults who take part in the health examination, and all of them have signed the relevant informed consent form.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.