
Abstract
Purpose
Growing evidence reported that vitamin D and uric acid metabolism played roles in the occurrence of benign paroxysmal positional vertigo, an otoconia-related vestibular disorder. We aimed to investigate the serum 25-hydroxy vitamin D (25(OH)D) and uric acid in patients with benign paroxysmal positional vertigo and to determine the risk factor for benign paroxysmal positional vertigo.
Methods
This case-control study comprised 182 patients with benign paroxysmal positional vertigo and 182 age- and gender-matched controls. All subjects’ age, body mass index, systolic blood pressure, diastolic blood pressure, 25-hydroxyvitamin D (25(OH)D), uric acid and serum calcium measurements were analyzed.
Results
We found a female preponderance of benign paroxysmal positional vertigo patients, with a median of 60 (52–66) years old. The results showed low vitamin D status both in benign paroxysmal positional vertigo and controls, with no significant difference of 25(OH)D levels between benign paroxysmal positional vertigo patients and controls (P > 0.05). Compared with the control group, patients with benign paroxysmal positional vertigo had a higher prevalence of vitamin D deficiency and a lower prevalence of vitamin D sufficiency (P < 0.05). Uric acid was significantly lower in the benign paroxysmal positional vertigo groups (P < 0.05). Logistic regression analysis revealed that age and uric acid were considered higher risk predictors for benign paroxysmal positional vertigo.
Conclusion
Our study observed low vitamin D status in patients with benign paroxysmal positional vertigo, with no significant differences of the 25(OH)D level in patients with benign paroxysmal positional vertigo and controls. Elderly, vitamin D deficiency and low uric acid levels may be risk factors for benign paroxysmal positional vertigo occurrence.
Introduction
Benign paroxysmal positional vertigo (BPPV) is a common peripheral vestibular disorder characterized by the symptoms evoked by bead movements, short-duration episodes, and spontaneous remission. BPPV is an important health problem worldwide and can occur at any age, with a higher incidence in the elderly. The one-year incidence of BPPV increased with age, from 0.5% in those aged 18–39 years to 3.4% in those aged over 60 years. By age 80, the cumulative incidence of BPPV approaches almost 10%. BPPV is preponderance in females above 50 years old, almost consistent with the perimenopause age range of women. The lifetime prevalence of BPPV is twice as high in females as in males.
The most acceptable explanation of pathology is that BPPV is caused by the dislocation of otoconia from the utricle and saccule into the semicircular canals or adhering to the cupula. Otoconia is composed of calcium carbonate crystals and glycoprotein, and the otoconia metabolism and remodeling is a dynamic process. Otolith shedding is associated with calcium homeostasis in the inner ear. In recent years, several studies suggested that vitamin D deficiency affects calcium metabolism, which may influence otoconia homeostasis and increase the risk of BPPV onset and recurrence.1–4 Uric acid (UA) can play a protective antioxidant role, inhibit the inflammatory cascade, reduce the permeability of the blood–brain barrier, and protect the central nervous system. 5 There is emerging evidence that UA acts as an antioxidant against oxidative stress associated with aging, disease, 6 and calcium homeostasis, 7 which may play a role in the pathology of BPPV. 7 Some studies have investigated the association between UA and BPPV and reached different conclusions.5,6
In this study, we aimed to assess the possible risk factors for BPPV and may provide helpful information concerning the demographic risk factors of BPPV.
Material and methods
Subjects
This study was a case-control retrospective study review of 2 years and 10 months of data, which consisted of 182 inpatients diagnosed with BPPV in the Otolaryngology Department and 182 age- and sex-matched controls for routine health checkup recruited from the Physical Examination Center, who had lived in the urban area of Beijing without dizziness or imbalance during the preceding years between May 2019 and February 2022 in Beijing Chao-Yang Hospital. BPPV patients’ age ranged from 25 to 86 years, while controls ranged from 27 to 85 years. Subjects were enrolled for the study paired by gender.
Inclusion and exclusion criteria
All BPPV patients had a typical history of transient episodes of positional vertigo and were diagnosed by Dix-Hallpike test8,9 and supine roll test. 10 Only patients with new-onset idiopathic BPPV were included in this study. For BPPV patients, a detailed medical history was obtained and a neurological examination was performed.
The exclusion criteria were as follows: Subjects with a history of head trauma, vestibular neuritis, Menière's disease, sudden hearing loss, labyrinthitis, autoimmune diseases, gout, malignant tumors, neurological diseases, chronic renal and hepatic impairment, parathyroid or thyroid dysfunction, use of any calcium or vitamin D supplementation or allopurinol that could affect vitamin D, calcium, and UA levels were excluded. 11
Data collection
All subjects’ age, body mass index (BMI), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were collected. Blood samples were collected in the fasting condition in the morning after an overnight and analyzed shortly after blood collection. 25-hydroxyvitamin D (25(OH)D), and UA were measured using electrochemiluminescence immunoassay (ECLIA) with Roche Elecsys 2010 analyzer (Roche Diagnostics GmbH, Mannheim, Germany) and automatic biochemical analyzer (ADVIA 2400, Siemens, Germany). Serum 25(OH)D levels are used to classify the vitamin D status as follows: vitamin D sufficiency (≥30 ng/mL), vitamin D insufficiency (21–29 ng/mL) and vitamin D deficiency (≤20 ng/mL). 12
Ethical approval
This study obtained ethics approval from the Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University (No. 2020-KE-226). Verbal informed consent was obtained from all individual subjects included in the study for their anonymized information to be published in this article.
Statistical analysis
Statistical analyses were performed by SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY). One sample Kolmogorov-Smirnov test was used for the normality test. Descriptive statistics were shown as median (interquartile range) for continuous variables, and categorical variables were expressed as numbers and percentages. The independent-sample t-test was used for normally distributed data, while the Mann-Whitney U test was used for non-normally distributed data to analyze whether there were statistical differences between the groups. Chi-square (χ2) test were used to compare the differences in the frequency distribution between groups. Multivariable binary logistic regression analysis was conducted to investigate the associated risk factors for BPPV. Results were expressed as adjusted odd ratios (OR) with the corresponding 95% confidence interval (CI). Pearson's correlation and Spearman's rank correlation coefficient test were used to examine whether there was a statistically significant correlation between UA and other variables. All P values were two-sided. Statistical significance was defined as P < 0.05.
Results
The clinical data of the study are summarized in Table 1. The present case-control study included 182 patients of BPPV and 182 age- and gender-matched controls. There was a female preponderance with a percentage of 78.6%, and 21.4% were males in patients with BPPV. The age of patients with BPPV range from 25 to 86 years old, with a median of 60 (52–66) years old. The age of controls ranges from 27 to 85 years old, with a median of 57 (50–68) years old. There was no statistically significant difference between the BPPV and control groups with respect to the median age or gender distribution (Table 1).
Clinical characteristics of patients with BPPV and controls.

SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index; UA: uric acid, 25(OH)D: 25-hydroxyvitamin D; IQR: interquartile range. Data are presented as the median (IQR) for continuous variables or as n (%) for categorical variables. * P < 0.05.
The results showed low vitamin D status both in BPPV and controls, with no significant difference of 25(OH)D levels between BPPV patients [17.06 (12.30–24.71) ng/mL] and controls [19.21 (13.41–26.33) ng/mL, P > 0.05]. Compared with the control group, patients with BPPV had a higher prevalence of vitamin D deficiency and a lower prevalence of vitamin D sufficiency (P < 0.05).
UA was observed significantly lower in the BPPV groups [310 (263–366) μmol/L] when compared with control subjects [328 (277–381) μmol/L, P = 0.011]. In contrast, no significant difference was found in SBP, DBP, BMI, and serum calcium between BPPV and control groups (P > 0.05).
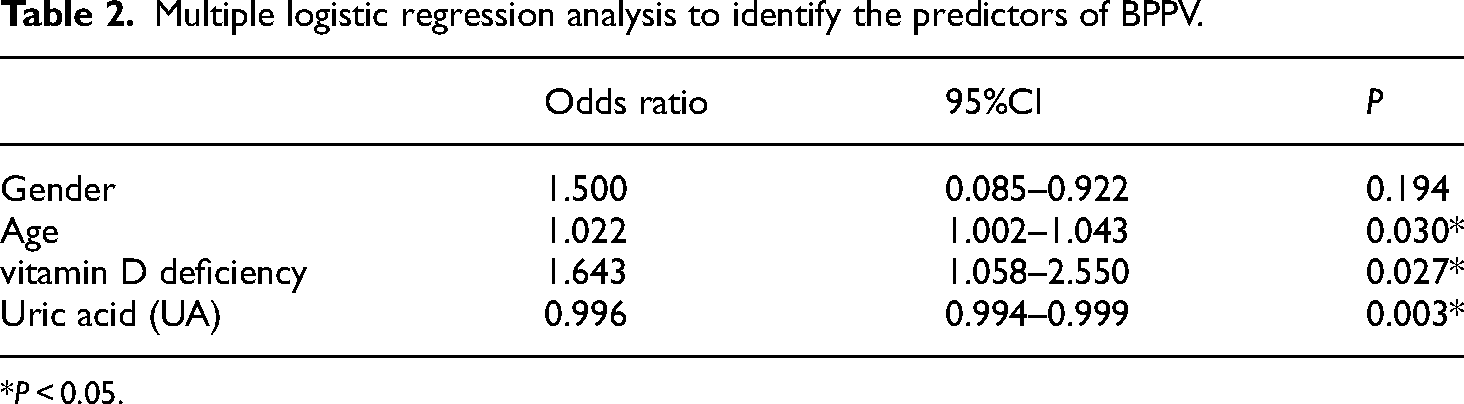
According to logistic regression analysis, age (OR 1.022, 95% CI 1.002–1.043, P = 0.030), UA (OR 0.996, 95% CI 0.994–0.999, P = 0.003) and vitamin D deficiency (OR 1.643, 95% CI 1.058–2.550, P = 0.027) were considered risk predictors for BPPV (Table 2).
Multiple logistic regression analysis to identify the predictors of BPPV.
*P < 0.05.
Discussion
BPPV is a frequent vestibular disorder, contributing to about 20%–30% of vestibular vertigo,13,14 with more onset in elderly people. Our results showed that the median age of BPPV patients was 60 years old with female preponderance, which is in accordance with previous studies. 13 The underlying mechanism might be the changes in otoconial morphology according to aging. Studies about the morphology of human vital otoconia in patients of higher age showed age-related otoconia degeneration may potentially lead to imbalance and play an important role in elucidating the degeneration etiology of BPPV. 15 Degenerated otoconia not only mediates inadequate or inappropriate sensory input to the utricle and saccule but also loose and prone to dislocation into the ampulla/canals. 16 The pathogenesis may be an age-related decrease of endolymphatic calcium supply, which may be limited from the beginning due to the lack of dark cells in the saccule. 17 In addition, weakened or broken junctional filaments and otoconial fragments were observed in aged rats, which may contribute to BPPV. 18
BPPV has been found more frequently in females over 50 years old, almost consistent with the period of perimenopause and estrogen fluctuation. Estrogen is a key regulator of calcium/bone metabolism and can affect the synthesis/absorption of otoconia. 19 A study conducted by Yang et al. 16 showed that estrogen deficiency led to abnormal otoconia and insufficient expression of otoconial proteins, which further resulted in imbalance behaviors and otoconia maintenance and anchoring. Additionally, estrogen deficiency may be involved in the occurrence of BPPV by regulating the expression of ion channels and affecting endolymphatic Ca2+ homeostasis. 20 Estrogen replacement therapy can reduce the incidence of BPPV in menopausal women. 21 The mechanism may be that adequate and stable blood estrogen levels can protect against intestinal Ca2+ absorption and loss of bone mineral density. 22 Furthermore, estrogen replacement therapy also reversed the decline of otoconin-90 levels, a major protein that maintains normal otolith morphology and growth.23,24
Vitamin D is known to influence calcium metabolism, which is critical for otoconia. Vitamin D deficiency is a public health consequence and a not well-recognized epidemic problem in the world. In a cross-sectional study examining the vitamin D status of urban Beijing residents, the results showed an extremely high prevalence of vitamin D deficiency and the vitamin D level in females was 11.8 ng/mL, lower than that of our study. 25 Some studies have shown associations between serum vitamin D levels and BPPV and speculated low levels of vitamin D were linked with a high prevalence and relapse of BPPV.4,26 However, some other studies have come up with conflicting results. Goldschagg et al. 27 investigated 25(OH)D concentrations between patients with BPPV, other vestibular disorders, and other neurological non-vestibular disorders. The results showed no evidence of a specific deficiency of 25(OH)D concentration in patients with BPPV or recurrent BPPV. Our results also failed to establish a direct correlation between vitamin D and BPPV. However, based on our data, low vitamin D status existed in BPPV patients and vitamin D deficiency was a risk predictor for BPPV. According to earlier studies, vitamin D supplementation is beneficial in preventing BPPV,4,28 and treatment is needed only in BPPV patients with reduced vitamin D levels, not all patients. 27
UA is a metabolite of purine and acts as a strong endogenous protective antioxidant in neurodegenerative diseases. Oxidative stress, related to calcium metabolism, has been identified as a potential mechanism to inhibit osteoblastogenesis and bone formation, affecting bone health and mass. 29 Our results showed that UA was significantly lower in the BPPV group compared to the control group, which is consistent with the results of some earlier studies.5,30 Tsai et al. 7 found there were elevated oxidative stress markers in BPPV patients, which remained higher in BPPV post-treatment patients. Sahin et al. 31 reported a significant reduction in native thiol/disulfide (SH/SS) levels in BPPV patients, which is a novel indicator of oxidative stress and suggests that oxidative stress plays a role in the occurrence and development of BPPV. Nabipour et al. 6 have reported higher serum UA levels were associated with higher bone mineral density (BMD) at all skeletal sites and a lower prevalence of osteoporosis. Xie et al. 5 found lower serum UA levels in the BPPV group, suggesting an association between weaker antioxidant capacity and a higher incidence of BPPV. Otoconia mainly consists of calcium carbonate, which is similar to that of bone. Therefore, we speculated that oxidative stress attenuated endolymphatic calcium homeostasis and influenced otolith function, which could explain the lower UA level in patients with BPPV compared to controls.
However, there are some conflicting results. Yang et al. 32 reviewed 12 studies and found that the heterogeneity of the UA levels was high. Studies from different areas of the world have produced different results. In a large cross-sectional study, researchers investigated the UA status in China and reported the median UA level in females living in eastern China (including Beijing) was 262.8 μmol/L, 33 which was lower than that in our study. UA levels vary significantly within humans as the result of factors that increase generation (such as high purine or protein diets, alcohol consumption, conditions with high cell turnover, or enzymatic defects in purine metabolism) or decrease excretion (such as diuretics, especially thiazides). 34 Besides, different ethnicities, geography, socioeconomic characteristics, and lifestyles may contribute to the discrepancy. Therefore, there is no consensus on whether UA is a protective or risk factor for BPPV and further research should examine genetic and environmental factors that may mediate an association between serum UA level and BPPV.
There were some limitations of the study. First, the study lacked an analysis of BMD and estrogen levels, which could be associated with BPPV. Second, we do not have a prior estimate of the sample size, the study only included inpatients and controls from the Physical Examination Center, so there may be selection bias by omitting outpatients and the small sample size. Generalization to other populations may be limited. Third, with regard to vitamin D and UA levels, factors such as outdoor activity, UVB exposure, diet, ethnicity and geographical location also need to be taken into account in further studies. We will make up for these limitations in subsequent studies with larger sample sizes.
Conclusion
In summary, we found a female preponderance of BPPV patients, and mainly affects elderly patients. The present study showed that low vitamin D status was found in both BPPV patients and controls, and no association was established between vitamin D and BPPV. Age and vitamin D deficiency may be risk factors for BPPV. UA was significantly lower in the BPPV groups, which may be a risk factor for BPPV occurrence and related to low antioxidative status.
Footnotes
Acknowledgments
The authors thank all the participants of the study.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Yuan-Yuan Ren, Jin-Lan Li, and Fei Xia. The first draft of the manuscript was written by Yuan-Yuan Ren and all authors commented on previous version of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approval was granted by the Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University (2020-KE-226). The date of approval for the study was April 8, 2020. This study was performed in accordance with the ethical principles of the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.
Author biographies
Yuan-Yuan Ren holds a MD in Otolaryngology Head & Neck Surgery. Her area of research is peripheral vertigo focusing on benign paroxysmal positional vertigo and Meniere's disease.
Yan-Jun Wang holds a MD in Otolaryngology Head & Neck Surgery. Her area of research is benign paroxysmal positional vertigo.
Jin-Lan Li is a nurse in Otolaryngology Head & Neck Surgery. Her area of research is otology and audiology focusing on vestibular vertigo.
Mo Liu holds a MD in Otolaryngology Head & Neck Surgery. Her area of research is otology focusing on vestibular vertigo.
Fei Xia holds a MD in Otolaryngology Head & Neck Surgery. Her area of research is peripheral vertigo focusing on benign paroxysmal positional vertigo and Meniere's disease.