
Abstract
In head and neck, adenoid cystic carcinoma (ACC) is a rare malignant tumor. ACC mainly generated from minor salivary glands, especially in the palate. We report an extremely rare case of ACC generating in the left palatine tonsil. A 50-year-old woman with foreign body sensation in the pharynx for 6-month was admitted to our hospital. Physical examination revealed a dark red mass in the soft palate near the upper pole of the left tonsil. Preoperative imaging examinations indicated a low-density mass in the left tonsillar area on the CT plain scan, which was a hyperintense mass at the anterior superior pole of the left tonsil on T2-weighted MRI. Complete surgical resection of the mass together with the left palatine tonsil was conducted under general anesthesia. The diagnosis of ACC was established based on histopathology and immunohistochemistry results. Then, postoperative radiotherapy of 60 Gy was administered. During regular medical follow-up for 12 months, no local recurrence was observed. Complete surgical resection, with or without postoperative radiotherapy is generally acknowledged as the standard of care for ACC. Despite the extremely low incidence in palatine tonsil, clinicians should consider the differential diagnosis of ACC.
Introduction
Adenoid cystic carcinoma (ACC) is extremely rare. It is characterized by indolent growth, perineural invasion, and distant metastasis, but regional lymph node metastases are uncommon.1,2 Risk factors for ACC include exposure to ionizing radiation, smoking, and low vitamin C intake. 2 It can occur at any age but is more common in people aged 40 to 60 years, 1 with a female predominance. 2 It is the most common malignancy of the minor salivary glands, especially in the palate. 3 Among the major salivary glands, ACC occurs most commonly in the submandibular gland, and less commonly in the sublingual and parotid glands. ACC can also arise from secretory glands at other sites, including the paranasal sinuses, nasopharynx, larynx, lacrimal glands, external auditory canal, tracheobronchial tree, skin, esophagus, breast, lungs, prostate, and uterine cervix. 2
ACC originating in the palatine tonsil is extremely rare, only three cases of palatine tonsil ACC had been reported till now. The first case of ACC in palatine tonsil was reported by Azarpira et al. in 2011. The patient, one 70-year-old man, admitted to the hospital due to a 3-month history of a mass in the right palatine tonsil. After fine-needle aspiration (FNA), the histologic examination established the diagnosis of ACC. 4 However, the information about the histologic pattern, medical imaging, treatment and follow-up of the case was not reported. 4 In the same year, Azizli et al. reported the second case of palatine tonsil ACC. 5 A 49-year-old woman presented with left otalgia was diagnosed with ACC generated from the left palatine tonsil parenchyma and right peritonsillar tissue. At the inferior poles of both palatine tonsils, two pale, solid, soft, painless lesions were found on examination, respectively. After bilateral tonsillectomy, postoperative adjuvant radiotherapy was arranged. 5 The latest case of palatine tonsil ACC is published by Tretiakow et al. in 2021. 6 A 26-year-old female patient suffered from stabbing pain on the left side of the throat and left-sided earache for about 4.5 months was diagnosed with cylindrical ACC of palatine tonsil. 6 Tonsillectomy together with adjuvant radiotherapy involving the primary focus and the cervical fields were administrated. During the following-up period, no evidence of recurrence and metastases was found. 6 However, the patient was followed up for only 3 months after therapy till their publication. 6 Another limitation is that the CT figures of the case were relatively fuzzy and no histopathology and immunohistochemistry figures was provided. 6 Here, we report the fourth case of primary ACC originating in the palatine tonsil.
Case report
A 50-year-old woman was admitted to our hospital with a 6-month history of a foreign body sensation in the oropharynx since January. No pharyngeal pain, cough, abundant expectoration, hemoptysis, shortness of breath, chest tightness, or dysphagia was reported. No enlarged cervical lymph node was observed in the neck. The patient did not have habits of smoking and drinking. No history of radiotherapy of the neck was reported. The remaining medical history of the patient was unremarkable. Physical examination revealed a hard, well-demarcated, dark red mass in the area near the upper pole of the left tonsil with intact mucosa (Figure 1(a)).

Images of the tumor. (a) The appearance of the tumor on laryngoscopy. (b) Plain computed tomography (CT) image showing a low-density, soft tissue mass in the tonsillar area of the left oropharynx. (c) Contrast-enhanced CT image showing a lack of enhancement and unclear boundary. (d) T1-weighted magnetic resonance imaging (MRI) showing an isointense mass. (e, f) T2-weighted MRI showing hyperintensity of the tumor. (g) Contrast-enhanced MRI showing uneven enhancement of the tumor. (h) Anterior view of the resected lesion. (i) Posterior view of the resected lesion.
Computed tomography (CT) revealed a low-density mass in the left tonsillar area on the plain scan with unclear boundaries and no enhancement (Figure 1(b) and (c)). T1-weighted magnetic resonance imaging (MRI) revealed an isointense soft tissue mass at the anterior superior pole of the left tonsil, measuring approximately 1.7 × 1.4 cm (Figure 1(d)), which was hyperintense on T2-weighted MRI (Figure 1(e) and (f)). The boundary was irregular, and the left palatine tonsil was compressed and squeezed backward and outward. It exhibited regional inhomogeneous moderate contrast enhancement, accompanied by hypointense lesions without enhancement (Figure 1(g)). Diffusion-weighted imaging showed no obvious diffusion restriction. Considering the liquefactive region in the mass, the radiologist suggested hemangioma or malignant tumor should be considered for differential diagnosis. CT and MRI revealed no enlarged cervical lymph nodes.
Considering the possibility of a malignant tumor, FNA biopsy was not performed to avoid possible metastasis. Radical resection of the mass and left palatine tonsil were carried out under general anesthesia. Following the dissection of the upper pole of the left palatine tonsil, the mass was revealed, located laterally to the upper pole of the left tonsil. The mass was meticulously dissected from the surrounding tissues, maintaining its integrity, and was subsequently excised along with the left palatine tonsil using low-temperature plasma radiofrequency (LPRF) coblation. The capsule of the mass was intact (Figure 1(h) and (i)). The tumor was diagnosed as ACC based on the histopathology and immunohistochemistry results. The histologic subtype was cribriform (Figure 2), which was the most common phenotype. 7
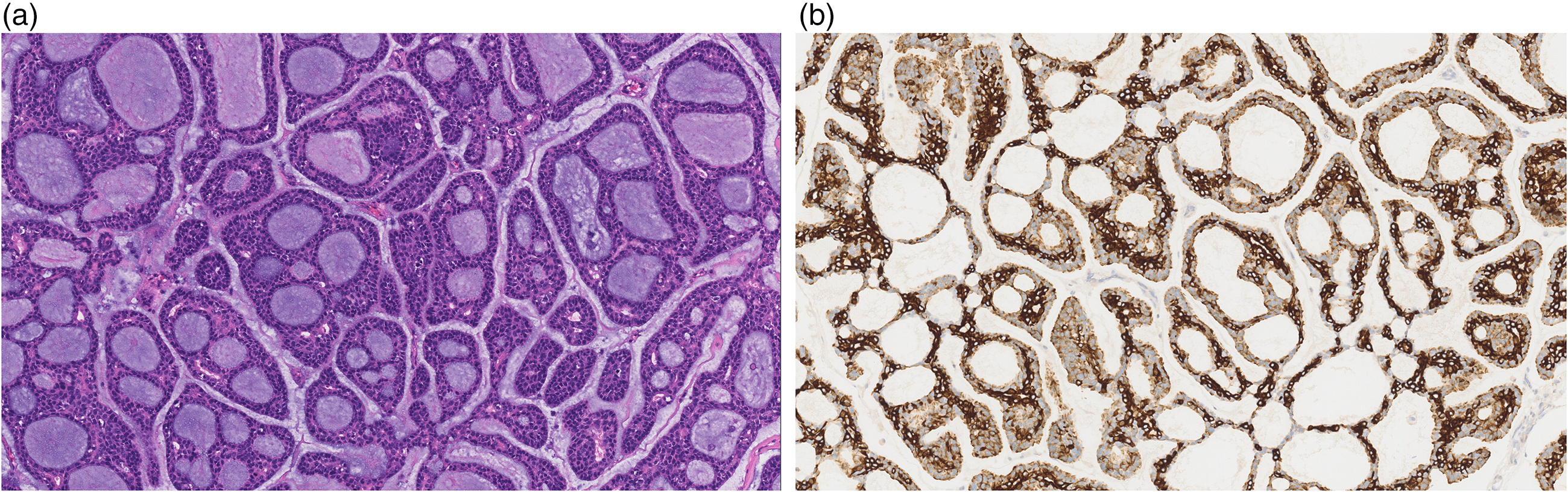
Histologic appearance of the excised tumor. (a) Hematoxylin–eosin stain and (b) positive stain for Ck-7.
Postoperative adjuvant radiation therapy, totaling 60 Gy, was administered to the patient, targeting the left upper neck, the operative bed, the left oropharynx, and extending to the left maxillary nerve up to the cavernous sinus apex. The patient underwent regular clinical evaluations, which included enhanced MRI scans of the head and neck and thin-slice CT plain scans of the lungs every 3 months, as well as neck and abdominal ultrasounds every 6 months over a 12-month period, with no evidence of recurrence observed. The reporting of this study conforms to CARE guidelines.8,9
Discussion
Most tonsillar malignancies are squamous cell carcinoma, including lymphoepithelioma, with malignant lymphoma composing the majority of the rest.10,11 Tonsillar metastases may occur from primary lesions in the lung, stomach, skin, kidney, and breast. 10 In head and neck, the favorable prognostic factors of ACC were proved to be early stages and major salivary gland subsite. 12 ACC accounts for 2% to 4% of malignant head and neck tumors, and 5% to 10% of salivary gland tumors. 3 ACC generating from tonsil were rarely read.5,6,13,14
Radiological imaging using either CT or MRI is useful for preoperative diagnosis. In the cases reported by Azizli et al. 5 and Tretiakow et al., 6 CT and MRI were conducted before surgery. Their results suggested the tumor showed mixed density and was contrast enhanced on T1W1 MRI. Besides, no evidence of infiltration or regional invasion and lymphadenopathy was detected. The radiological findings in those two cases and our case were consistent with the literature. ACC typically appears as an irregular soft-tissue density mass on CT, with mild-to-moderate contrast enhancement. 15 T1W1 on MRI of ACC located at head and neck generally presents isointense or hypointense signals, and T2W1 generally presents hyperintense or slightly hyperintense signals. After contrast medium administration, uneven enhancement could be observed in most cases. 15 However, no CT or MRI results were displayed in the case reported by Azarpira et al. 4 In ACC of the head and neck, 18F-fluorodeoxyglucose positron emission tomography-computed tomography (18F-FDG PET/CT) can improve the detection of local tumor and metastatic spread.5,16
A meta-analysis found that painless swelling is the most common clinical presentation of intraoral ACC, 3 as in this case. However, otalgia was reported as initial symptom in both cases reported by Azizli et al. 5 and Tretiakow et al., 6 suggesting the clinical importance of foreign body sensation in the pharynx and otalgia as early clinic symptoms of palatine tonsil ACC. On the other hand, among the four instances of ACC of the palatine tonsil, three were female and one was male, aligning with the established female predominance in ACC incidence. 2 Although two cases occurred within the most prevalent age range of 40 to 60 years, one case involved a younger individual aged 26, and another involved an older individual aged 70. Given that ACC can manifest at any age, 1 it is crucial to consider the potential for ACC in patients outside the typical age range.
The asymmetry of palatine tonsils was the consistent character across all reported cases,4–6 including our case. Different from our case here, the abnormally large tonsil exhibited an ulcerative tender in the case reported by Azarpira et al.. 4 The other two cases represent themselves as solid masses without ulceration, as in our case.5,6 Generally, tonsil tumors exhibit exophytic, infiltrative, or ulcerative growth patterns, with ulcerative growth patterns being most common which indicating poor prognosis. 10 However, the histologic subtype, treatment and the outcome of the patient were not recorded. 4 Thus, the prognoses of palatine tonsil ACCs with or without ulceration could not be compared. Besides, considering the extreme small sample size, if ulcerative growth pattern indicates poor prognosis in palatine tonsil ACC needed further studies.
Generally, ACC is classified into three distinct architectural patterns: cribriform, tubular, and solid. Among them, the subtype of cribriform was the most common histology, while the subtype of tubular indicated better prognosis and solid signifying worse. 7 In this case reported by Azizli et al., 5 the histologic pattern consisted of mixed predominant cribriform and concomitant tubular structures. The subtype of the ACC in the case reported by Tretiakow et al. 6 was tubular (cylindrical). Although the prognosis of ACC subtype in their case was best, Tretiakow et al. suggested that the post-therapeutic follow-up should last the whole life of the patient.
Complete surgical resection, with or without postoperative radiotherapy, is generally acknowledged as the preferred treatment for ACC in head and neck.3,17 Based on the recommendation of the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) for Head and Neck Cancers, Chen et al. investigated the roles of postoperative radiotherapy in the ACC of head and neck. 18 Through employing high-energy radiation to induce DNA damage in tumor cells through direct ionization or indirect ionization mediated by photons or charged particles, radiotherapy is a critical modality for enhancing local tumor control. 18 The results validated that postoperative radiotherapy could improve local recurrence-free survival in patients with head and neck ACC. 18 Similarly, the incidence of both locoregional and distant relapses was observed to be lower in patients who received a combination of surgery and postoperative radiotherapy. 12 Regarding the chemotherapy treatment of ACC, particularly in the head and neck region, its efficacy remains a subject of debate.12,19 In a review conducted by Papaspyrou et al., 20 the authors concluded that the reported response rates to combination chemotherapy were low, and the duration of response was generally short-lived. No standard chemotherapy regimen could be recommended based on the available knowledge.12,20 Thus, complete surgical resection and followed postoperative radiotherapy was administered in our case.
Occult cervical metastasis is an essential prognostic factor for tonsil tumors, with a rate of approximately 27% in tonsil carcinoma. 10 Early diagnosis and timely treatment of cervical metastases can prevent distant metastases. 10 However, ACC is characterized by a low rate of regional lymph node metastasis and delayed distant metastasis, with an incidence of occult nodal invasion from the primary location of less than 20%. 21 Although the incidence of occult neck metastasis of ACC from the oral cavity and oropharynx is higher than that from other sublocations in the head and neck, this incidence does not reach the standard generally applied to justify elective neck dissection (END). 21 Compared with squamous cell carcinoma of the head and neck, the poor prognosis of ACC is mainly due to its propensity for distant metastasis rather than local or neck recurrence. 21 Thus, considering that postoperative radiotherapy can include the primary site and first echelon lymph nodes simultaneously, END is not recommended in patients with a clinically negative lymph nodes (cN0) neck suffered from ACC of oral cavity and oropharynx, if postoperative radiotherapy was administered. However, if postoperative radiotherapy is not arranged in high risk oral and oropharyngeal ACCs with lymphovascular invasion or high-grade transformation, END should be considered even a cN0 neck was presented. 21 In our patient, no signs of cervical metastasis were found during the preoperative examination. Therefore, due to that postoperative radiotherapy was administrated, prophylactic END was not performed.
Conclusion
This case of ACC presented as a foreign body sensation in the pharynx, and could easily have been misdiagnosed as a polyp. Contrast-enhanced CT and MRI were useful for making the correct diagnosis. Considering the long natural history of ACC, patients should be followed up for longer than 10 years.
Footnotes
Acknowledgments
The authors would like to thank Dr Hui Chen (Fudan University) for critical reading and English language editing of the manuscript.
Authors’ contributions
YG wrote the manuscript and prepared the figures. QH collected the clinic data and clinically contributed to this study. HD conceived and designed the case report, contributed to the clinical diagnosis and treatment, revised the manuscript. All the authors approved of the final manuscript.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from Institutional Ethics Committee of the Eye & ENT Hospital of Fudan University (2024-YS-216) in 2024.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Leading Talents of Minhang Distract (202207) and Shanghai Sailing Program (21YF1405600; 23YF1404700).
Patient consent for publication
Written Informed Consent was obtained from the subject for the publication of the case report.