
Abstract
Introduction
Evaluating the mechanical–anatomical alignment and angles of the knee joint is crucial for athletes. We aimed to analyse the relationship between lower extremity bone alignment and the importance of the Q angle (QA) in male athletes.
Methods
We included 38 male professional football athletes without any alignment or varus-valgus deformity who actively played football in various football clubs in Istanbul. This study was conducted using quantitative research methods within the scope of a cohort study design and employed a correlational survey method. A health specialist at the orthopaedic outpatient clinic of the Haseki Training and Research Hospital, Istanbul, evaluated the participants’ lower extremity bone alignment using standing anteroposterior radiographs and assessed the QA using the goniometric measurement method. The anatomical lateral distal femoral angle (aLDFA), medial proximal tibial angle (MPTA) and QA data were analysed to assess lower extremity straightness.
Results
Significant relationships between the right and left leg aLDFA, MPTA and QA values of the participants’ lower extremity mechanical axis values and between the aLDFA and right leg QA values (r = 0.380, p = 0.019) were found. These relationships were attributed to the difference between proximal and distal alignments of the lower extremities. The correlation between QA and certain mechanical alignment parameters was due to unilateral and bilateral symmetrical arrangements of the lower extremities.
Conclusions
The parameters of lower extremity mechanical–anatomical alignment are considered preliminary indicators of relationships among sports injuries, structural factors and predisposition to such injuries. Individual differences in the angular values of mechanical–anatomical alignment and the application of different methods for determining these angles have revealed some uncertainties. We determined the mechanical axis data of football athletes who predominantly used their lower extremities using the most reliable methods and examined the relationship among the right and left leg aLDFA, MPTA and QA values. We believe that our findings provide insights and guidance for experts in the field.
Introduction
Differences in some anatomical and mechanical values of athletes may cause variability in their daily life activities and athletic performance. Although sports performance is characterised by many parameters, the alignment of the lower extremities and the role of the knee joint are of paramount importance in sports involving the dynamic use of the lower extremities. Therefore, evaluating the mechanical–anatomical alignment and angles of the knee joint is crucial.
Lower extremity alignment is a framework term used to describe the relationship between the joints and bone structures of the lower extremities in three different planes. Alignment in the coronal, sagittal and axial planes is examined in different ways. For example, the alignment status is reported as varus or valgus in the coronal plane and recurvatum in the sagittal plane, whereas the amount of version or torsion is determined based on the anatomical structures assessed in the axial plane. 1 Based on its style of play, football is a type of sport that involves the predominant use of the lower extremities. Lower extremity alignment can be evaluated using various methods. Among these methods, Q angle (QA) measurement is used to evaluate the biomechanical status of the patellofemoral joint and lower extremity alignment. The QA refers to the angle between a line drawn from the anterior superior iliac spine (ASIS) to the centre of the patella and another line drawn from the centre of the patella to the centre of the tibial tubercle. Q angle measurement is used to define the relationship between sports injuries and structural factors and is considered a preliminary indicator of predisposition to sports injuries. 2
The anatomical lateral distal femoral angle (aLDFA) and medial proximal tibial angle (MPTA) values are other measures for determining bone alignment (Figure 1). 3 Anatomical lateral distal femoral angle is defined as the angle between the horizontal plane of the knee joint and the mechanical axis of the femur; it is approximately 87°. For this alignment, angles >90°, 85–90° and <85° are considered varus, neutral and valgus alignments, respectively. 4 Besides, the QA is defined as the angle between the anatomical axis of the femur and the distal femoral joint axis. 5 The MPTA comprises the anatomical axis of the tibia and the line tangent to the tibial plateau in the frontal plane that crosses it, with a normal limit range of 85–90°. 6 Specifically, the MPTA is defined as the angle between the line drawn from the tibial articular surface and the line drawn between the mechanical axis of the tibia; it is approximately 87°. 7 For this alignment, the reported references are >90°, 85° and 90° and <85° as varus, neutral and valgus alignments, respectively. 4 Anatomical MPTA and mechanical MPTA are similar because their axes are considered the same.
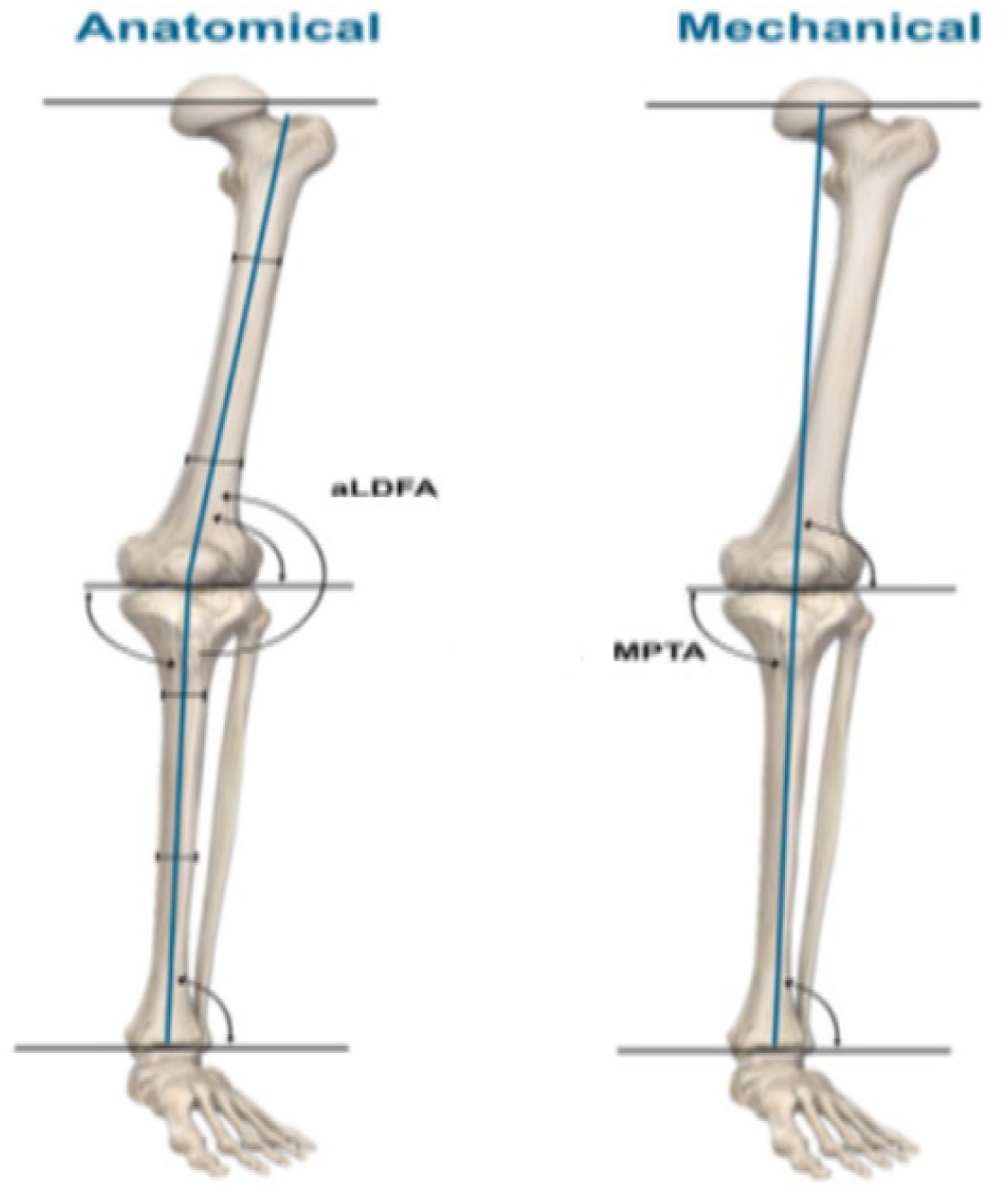
Physiological axes of the lower limb 1 (permission was obtained from the author).
A decrease in the normal MPTA value suggests the presence of bone damage medial to the tibia, indicating that the proximal articular surface of the tibia is slightly varus. This feature stabilises the valgus arising from the distal articular surface of the femur, allowing the knee joint to remain parallel to the ground during gait. 8
Complete visibility of the hip and ankle joints is necessary to fully determine lower extremity alignment. Currently, with the development of technology, computer software programs are being applied to perform the measurements. 9 Such digital measurements can be advantageous, especially when accuracy in millimetres is critical. Based on advancements in technology, efforts to measure the lower extremity axis with near-complete consistency by using not only radiography but also three-dimensional computed tomography reconstructions are ongoing. Nonetheless, further studies on these methods are required. 10 Multiple methods are used to determine QA, but most researchers use goniometers. Additionally, photographic techniques, radiography and computer imaging systems are utilised. Further research on these methods is required. 11
Changes in the QA may lead to injuries due to the abnormal force exerted by the quadriceps femoris on the knee joint, suggesting that the QA should be considered a risk factor for injury. 12 These changes in the QA lead to anterior pelvic tilt, increased femoral anteversion, increased valgus in the knee owing to deviation in the lower extremity mechanical–anatomical alignment and increased tibial rotation. Consequently, a change in the ankle position can be observed. 13 This situation may negatively affect sports performance, especially in football, in which the lower extremities are predominantly used. One of these lines represents the quadriceps femoris muscle, and the other represents the patellar tendon. The QA can help understand the patellofemoral joint biomechanics. The QA change is approximately 8° during flexion and 10–13° for men and 15–17° for women during extension. 14 As the QA falls below 13°, knee injuries such as patellar instability, chondromalacia patellae and patella alta may occur, increasing the risk of injury and negatively affecting performance in sports that require the predominant use of the knee. A QA >18° is associated with chondromalacia patellae, subluxated patella, patellofemoral pain syndrome, genu valgum, increased femoral anteversion, tibial tubercle lateralisation and increased lateral tibial torsion. 15
Previous studies have used various QA measurement methods. However, at present, there are no internationally accepted methods for measuring this angle. When the QA is measured while standing, it increases by an average of 1.4° in men and 2.4° in women compared to the QA value measured in the supine position. Increased femoral anteversion in the standing position can cause internal rotation of the femur. This internal rotation can lead to medial turning of the femur, resulting in the patellar tendon attaching more laterally to the tibia, which can mechanically increase the QA. Another reason for this difference is that the standing position is more affected by the foot, ankle and hip joints than the supine position. Q angle measurements are generally preferred with the knee in extension because, in flexion, the patella shifts position, leading to a reduction in QA. 11
The present study aimed to analyse the relationship between the bone alignment of the lower extremities and the importance of QA in male athletes.
Methods
This cohort study was conducted using quantitative research methods and a correlational survey method. In addition, the study was conducted as an “exploratory correlation research” by applying the relational screening method. All parameters were collected by a specialist physician at the Orthopaedics and Traumatology Clinic of the Haseki Training and Research Hospital, Istanbul. Data were collected from all participants on 13 May 2024 and date study ended on 19 May 2024 This study was reported following the relevant guidelines set forth by the EQUATOR Network for observational studies 16 and was conducted in accordance with the 1975 Declaration of Helsinki and its 2013 revision and was approved by the Iğdır University Scientific Research and Publication Ethics Committee, Approval number: 2024/15. Date of approval: 13 May 2024.
All participants provided written informed consent prior to study participation. All participant data were kept confidential to ensure confidentiality and privacy. The study was limited to 38 professional male athletes aged 18–27 years without varus and valgus deformity in themselves and their families.
Lower extremity bone alignment assessment
Measurements such as the mechanical axis of the lower extremity and the mechanical axis deviation (MAD) are used to detect lower extremity deformities. The mechanical axis of the lower extremity is represented by a vectorial line connecting the midpoint of the femoral head to the midpoint of the tibia-talus joint surface. Body weight was transmitted along the axis to the ground. The distance between the midpoint of the mechanical axis and the genu joint represents the MAD. To perform these measurements, we used orthoradiography (leg length radiography), allowing clear differentiation of the femoral head, knee joint and ankle joint. 17
In our study, the participants’ lower extremity bone alignment was evaluated using the aLDFA and MPTA methods with the Marca X2-C model device (Usx-ray, Bolu, Turkey) and weighted anteroposterior radiographs. Radiographs of the lower extremities were obtained with the participant's knee positioned in full extension, feet bare and body weight equally distributed across both extremities. Once the tibial tubercle was correctly placed in the beam, the intra- and interobserver reliabilities of aLDFA and MPTA were consistent. The angular calculations were performed by an experienced specialist using the obtained radiographs.
Anatomical lateral distal femoral angle determination
To determine the aLDFA, two regions on the femoral shaft were selected (Figure 2). Two lines perpendicular to the femoral shaft were drawn from these regions, and their midpoints were identified. A line connecting these two midpoints was drawn. In addition, a line connecting the most inferior subchondral points of the medial and lateral femoral condyles, known as the distal femoral orientation line, was drawn. The lateral angle between the two lines was calculated as the aLDFA. 3

Radiograph used in aLDFA determination. Radiograph used in MPTA determination. aLDFA: anatomical lateral distal femoral angle; MPTA: medial proximal tibial angle.
Medial proximal tibial angle determination
To determine the MPTA, the midpoint of the tibial plateau joint surface was connected to the midpoint of the distal tibial joint surface to draw the tibial mechanical axis (Figure 2). Thereafter, a line connecting the subchondral points of the tibial plateaus was drawn to create a proximal tibial orientation line. The medial angle between the tibial mechanical axis and proximal tibial orientation line was calculated as the MPTA, and its angular value was determined.7,18,19
Q angle measurement
The participants’ QA was measured using a 360° 21-cm plastic goniometer (SH5201, Saehan, Korea) and a tape measure (Figure 3). During the QA measurement, the participants were placed in a supine position with the knees extended, and the ideal position was ensured to keep the leg muscles relaxed. The participants lay on an examination table with the patella facing upward (anteriorly). The examiner marked the centre of the tibial tubercle using a pen. Draper et al. showed that a long-arm goniometer was more accurate than a short-arm goniometer. 20 Therefore, we used a 21-cm (8-in.) goniometer to better visualise the ASIS point. The long arm of the goniometer was placed on the ASIS, and the participant was asked to hold it in place, thereby freeing the hands of the measuring specialist and allowing them to perform their movements more freely. The examiner held the goniometer and patella together and ensured that they were in the correct positions after centring the pivot of the goniometer at the centre of the patella. After the pivot point was centred on the distal femur at the trochlear insertion, the QA was measured precisely with the short arm of the goniometer. 21 This angle is typically 8–14° for men and 11–20° for women. An increase >20° in the QA indicated lateral displacement of the patella.

QA measurement. QA: Q angle.
Statistical analysis
Statistical analysis was performed using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA). The relationship between all parameters was evaluated using Pearson's correlation coefficient, with statistical significance set at a p-value <0.05. The mean values of all participants’ parameters were evaluated using descriptive statistical analysis. Power analysis for the one-tailed paired correlation analysis indicated that the minimum sample size required to achieve a statistical power of at least 80% with a medium effect size (d = 0.5) was 23. The analysis was conducted at an alpha level of 0.05.
Results
The mean age of the study population (n = 38) was 22.39 ± 1.966 years, and the mean height and weight of the participants were 178.16 ± 6.092 cm and 77.18 ± 8.798 kg, respectively. The mean values of the right and left leg QA are presented in Table 1. In addition, Table 1 shows the mean values of the right leg aLDFA, left leg aLDFA, right leg MPTA and left leg MPTA.
Mean angular values of mechanical axis alignment.
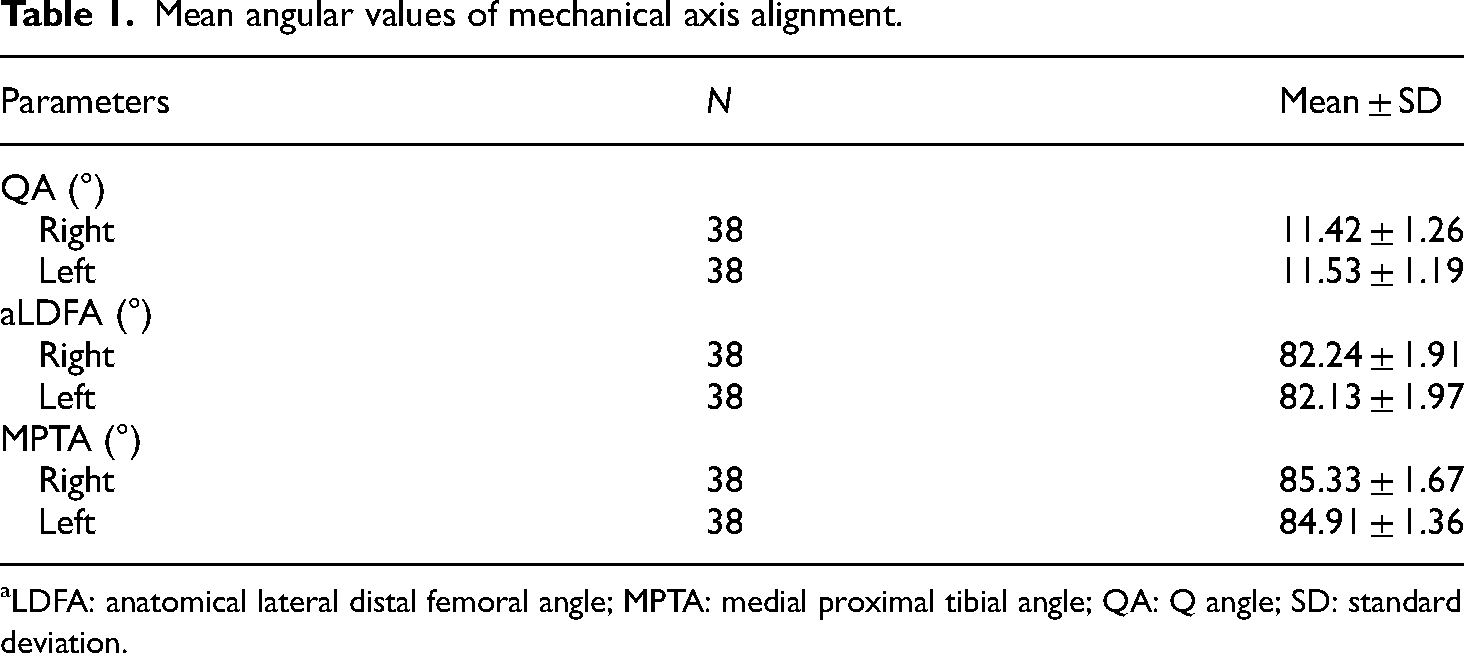
aLDFA: anatomical lateral distal femoral angle; MPTA: medial proximal tibial angle; QA: Q angle; SD: standard deviation.
Table 2 shows a statistically significant relationship between the QA values of the participants’ right and left legs (r = 0.782, p < 0.001). Similarly, there was a statistically significant relationship between the MPTA values of the participants’ right and left legs (r = 0.630, p < 0.001). Additionally, a statistically significant relationship was found between the aLDFA values of the right and left legs (r = 0.653, p < 0.001). Furthermore, a statistically significant relationship was observed between the aLDFA value of the left leg and the QA value of the right leg (r = 0.380, p = 0.019).
Relationships among mechanical axis values of the lower extremity and QA.

aLDFA: anatomical lateral distal femoral angle; MPTA: medial proximal tibial angle; QA: Q angle; SD: standard deviation.
Correlation is significant at the 0.01 level (two-tailed).
Correlation is significant at the 0.05 level (two-tailed).
Discussion
In this study, we analysed the relationship between lower extremity bone alignment and the QA in male athletes. The results showed significant relationships between the right and left leg aLDFA, MPTA and QA values of the participants’ lower extremity mechanical axis values and between the aLDFA and right leg QA values (r = 0.380, p = 0.019). In our study, the mean value of the right and left leg QA was 11.42 ± 1.26° and 11.53 ± 1.19°, respectively. Paulos et al. reported that all individuals with lower extremity alignment disorders had a QA ≥15°, whereas those with good or excellent results had a QA ≤10°. 22 Therefore, we can argue that the QA values of athletes who participated in our study were close to the ideal reference ranges.
Intraoperatively, QA measurement can help prevent the tibial tubercle from moving excessively medially beyond a 0° QA, which can lead to serious injuries such as iatrogenic medial patellar subluxation complications. 23 Q angle measurement is the only method for assessing tibial tubercle lateralisation, without expensive and possibly unnecessary imaging procedures. Therefore, a simple, practical and standardised QA measurement protocol is necessary to prepare an appropriate treatment protocol. 22 In the present study, a statistically significant relationship was found between the right and left leg QA values of the participants. This result is due to the bilateral symmetry of the lower extremities. Changes or decreases in neuromuscular control with an abnormal increase in QA may cause the knee joint to deviate out of the plane of motion and overload the joint while performing sports movements.24–26 Atbaşı et al. reported that with an increase in QA, injuries such as medial synovial plica, osteochondral fractures, patellar retinacular ligament injuries, loose bodies and tendinitis, as well as other anterior knee pain injuries, may occur. 27
In our study, the mean aLDFA value of the participants’ right and left leg was 82.24 ± 1.91° and 82.13 ± 1.97°, respectively. The distal femur joint orientation line formed an average angle of 81° (minimum of 79°–maximum of 83°) laterally with the anatomical axis. An increase of more than 5° in the angle indicates valgus deformity. 4 In this regards, the mean aLDFA in the athletes participating in our study was within the ideal reference range. Additionally, a statistically significant relationship was found between the left leg aLDFA and right leg QA values of the participants. The change in the aLDFA may have affected the other mechanical alignments because the participants might have contracted or relaxed their left quadriceps muscle groups during the measurement. Metgud et al. reported that angular changes in the knee joint structure may cause disturbances in the biomechanical alignment of lower extremities. 28 This situation can be partially explained by the quadriceps femoris muscle pulling the patella laterally with an increase in QA and by shifting the centre of the patella more laterally, leading to an increase in QA. The mechanical axis can physiologically pass through the centre of the knee joint or approximately 15 mm medially or laterally. Increased medial deviation of the mechanical axis beyond these limits indicates a varus deformity, whereas increased lateral deviation indicates a valgus deformity. In varus deformities, there is an increase in loading on the medial side of the joint; in contrast, an increase in loading on the lateral side of the joint is observed in valgus deformities. 29
The mean value of the right and left leg MPTA was 85.33 ± 1.67° and 84.91 ± 1.36°, respectively. The proximal tibial joint orientation line angulates 87° (minimum of 85°–maximum of 90°) medially with the mechanical axis of the tibia. 30 An increase of more than 5° in the angle indicates varus deformity. 13 Therefore, the angle in the athletes participating in our study was within the ideal reference range. A statistically significant relationship was observed between the mean MPTA values of the right and left legs, which may be attributed to the lower extremity mechanical–anatomical alignment, indicating symmetry. No correlation was found between the MPTA and QA values of the participants, possibly because a low QA does not necessarily indicate that the patella always shifts medially. Herrlin et al. reported that as the aLDFA and QA increased, the Tegner–Lysholm and Oxford Knee scores decreased, whereas as the MPTA increased, the Tegner–Lysholm score increased. This report indicates that the functional scores deteriorate along with the deterioration of the mechanical axis alignment towards varus. Therefore, with the deterioration of the angles, individuals may find difficulties in performing daily activities and athletes cannot fully reach their functional capacity. 31
Lower extremity alignment in the coronal plane is important in terms of load distribution on the joints. Misalignment can lead to asymmetric loading and, consequently, injuries that negatively affect sports performance. Therefore, it is crucial to measure lower extremity alignment accurately and reproducibly and to interpret the findings according to different variables; this will ensure improvements in sports performance and the protection of athletes’ health. 9
In a 2010 study, Barton et al. pointed out the importance of dynamically evaluating the biomechanics of lower extremity alignment for determining pathology. They suggested that foot pronation, excessive heel strike during running and abnormal mechanical alignment (such as hallux valgus) are associated with injuries in this area. 32
Based on this, it is possible to mention the effects of lower extremity alignment problems of football athletes on injury factors and sports performance. Doral et al. emphasised the complex mechanical–anatomical structure of the knee region in the lower extremities, with references at the end of the study. They mentioned that alignment problems in this area result in severe pain on the back surface of the patella, especially during squatting, sudden stopping, sudden acceleration and deceleration, Moreover, repeated microtraumas caused by sudden squatting and jumping movements in sports, such as football and rugby, may have a higher risk of occurrence. 33 In the current study, we selected football athletes as the study population and focused on lower extremity alignments because the sport involves very complex skills and highly difficult movements that increase the injury risk factor; the importance of the related parameters was emphasised in this regard. Espregueira-Mendes et al. emphasised that because football is played with feet and has a high load on the lower extremity, most injuries occur in the lower extremity and knee joint. 34 In addition, Işın stated that knee alignment disorders such as genu varum and genu recurvatum are among the factors affecting knee injury. 35 Rerucha et al. and de Rezende et al. highlighted that genu varum is an angular deformity of the varus of the knee joint.36,37 Melekoğlu and Işın reported that genu varum is the most common knee alignment disorder among football athletes. 38 Arliani et al. found that the incidence of genu varum increases in former professional football athletes. 39 Asadi et al. emphasised that comprehensive football techniques such as running, passing, changing direction, tackling and kicking (shooting) may lead to the development of genu varum in young athletes. 40 Işın et al. stated that knowing the relationship between lower extremity alignment problems and other variables in football athletes aged >18 years is important for identifying and monitoring football athletes who are particularly at high risk and taking preventive measures, consistent with the results of our study. 41 Besides the aLDFA and MPTA values used in our study, the anatomical tibiofemoral angle, anatomical lateral distal tibial angle, mechanical lateral distal femoral angle, mechanical MPTA and mechanical lateral distal tibial angle values of lower extremity mechanical alignment can also be evaluated.
In future studies, the importance and relational status of these parameters should be evaluated. The present study emphasised the importance of lower extremity mechanical alignment angles and showed that misalignment might lead to certain injuries. Therefore, ensuring normal alignment can minimise health risk factors, and evaluating this alignment in more detail during health screenings of male athletes is crucial. Furthermore, our study suggests that these angles can vary according to individual differences. In this study, lower extremity alignment values were determined by applying clinical tests to male athletes without any surgical history. In line with the purpose of the study, we discussed the treatment of angular deformities in mechanical alignment. Lower extremity alignment problems, such as varus and valgus above a certain degree, are considered entirely pathological and require surgical intervention. This study aimed to determine the importance of certain parameters related to this alignment, their relationships, measurement methods and ideal reference ranges. Thus, rather than obtaining new data, we aimed to clarify some uncertainties in the measurement methods using existing reference values. For such complications, the final decision for male athletes should be made by a specialist.
Conclusions
In our study, anatomical and mechanical axis values were determined in football athletes and then compared with the results of similar studies. In this context, ideal reference ranges for lower extremity skeletal alignment and QA are provided. The relationship between the obtained parameters was examined, and the correlation between the structural factors in this region was investigated. The research results will contribute to the measurement, diagnosis, treatment and preparation of relevant application protocols, particularly for specialists in health and sports.
Footnotes
Acknowledgements
Author contributions
Conceptualization: Ömür GÜLFIRAT, Mehmet EKİNCİ; Methodology: Ömür GÜLFIRAT, Mehmet EKİNCİ; Formal analysis: Ünsal TAZEGÜL; Investigation: Ömür GÜLFIRAT; Resources: Ömür GÜLFIRAT; Writing – original draft preparation: Ömür GÜLFIRAT; Writing – reviewing and editing: Aliasker KUMAK. All authors have read and agreed to the final version of the manuscript.
Consent to participate
Prior to study participation, all participants filled out an informed consent form.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was conducted in accordance with the 1975 Declaration of Helsinki and its 2013 revision and was approved by the Iğdır University Scientific Research and Publication Ethics Committee, Approval Number: 2024/15.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.