
Abstract
Examination of the variability of stress biomarkers among people living with dementia and their family caregivers can provide evidence of stress reactions and corresponding self-regulation capacities, but no such research has been conducted to date. The aim of this study was to examine day-to-day variability patterns of salivary biomarkers in dyads of people living with dementia and their family caregivers and to investigate differences in variability patterns between music intervention and control groups. This study involved secondary analysis of data collected during a two-group, non-randomized open trial examining the effects of an 8-week music intervention on physiological stress markers. A total of 5791 salivary samples from 34 dyads were used to analyze the variability of morning and evening cortisol and of morning dehydroepiandrosterone sulfate (DHEA-S). The variability indices employed were the intra- and inter-individual standard deviation, coefficient of variation, and intra-class correlation coefficient. We found that family caregivers in the music intervention group had significantly greater coefficients of variation for all three biomarker endpoints than those in the control group. Our findings provide evidence that stress biomarkers in family caregivers with functional self-regulation capacities may be more likely to respond to music intervention. However, stress biomarkers in people living with dementia may not be responsive to music intervention, possibly due to their dysfunctional self-regulation capacities. Future stress biomarker studies involving dyads of people living with dementia and family caregivers should consider biomarker variability patterns in determining the effectiveness of behavioral interventions.
Introduction
Due to the progressive cognitive and functional decline characteristic of dementia, people living with dementia (PLWD) and their family caregivers (FCGs) experience long-term stress that leads to negative health outcomes such as inflammation and cardiovascular disease. 1 It is clearly important to assess stress in PLWD and their caregivers, but the validity of self-reporting among PLWD in particular is questionable due to their cognitive impairment. Consequently, physiological biomarkers have emerged as a promising option for stress assessment in PLWD as well as FCGs. 2
Cortisol and dehydroepiandrosterone sulfate (DHEA-S) are two frequently studied biomarkers used as measures of stress. Cortisol regulation is part of the circadian rhythm. Levels start to rise from 2:00 to 4:00 am, peak about 30 min after awakening, and then decline throughout the day to reach a nadir at midnight. 3 DHEA-S is released simultaneously with cortisol in response to stress and may play a significant role in mitigating the negative impact of stress. 4 The level of DHEA-S in the body peaks from ages 20 to 24 years and then declines with age. 4 A number of studies have demonstrated the relationship between cortisol and DHEA-S levels and stress.5,6 Saliva sample collection has been commonly used to measure psychological stress due to its non-invasiveness, ease of performance by participants, and ability to measure spontaneous cortisol concentrations in the living environment.7,8 Therefore, use of saliva to measure a stress-related biomarker as an indicator of perceived stress is an innovation that promises to facilitate stress assessment in PLWD and their FCGs. 9 Several other biomarkers of stress could have been utilized, but repeated assessments of the concentrations of stress-related steroids in saliva were considered likely to provide the best opportunity to study daily variations in stress levels in this particular kind of elderly population.
Despite the increasing interest in stress biomarkers, the variability of such biomarkers makes it challenging to interpret findings in dementia and stress research, often leading to inconsistent results. 10 Cortisol levels show variability throughout the day based on the circadian rhythm, and both cortisol and DHEA-S levels are influenced by aging, cognitive impairment, and chronic stress. 7 Thus, the variability of such biomarkers in older PLWD and FCGs having chronic stress may show patterns different from those of healthy individuals. The variability of the circadian rhythm within and between individuals is mainly attributable to the variability of cortisol levels, which is influenced by individual characteristics (e.g. reaction to stress), circumstances (e.g. a stressful environment), and dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis by cognitive impairment. 11 Therefore, examination of the variability of cortisol and DHEA-S levels can facilitate explanation of observed changes or lack of changes in levels of these stress-related hormones in PLWD-FCG dyads during interventions.
One promising dyadic intervention for stress is music therapy, which is easily accessible and cost-effective. 12 Our previous publication demonstrated pronounced intra-individual cortisol variability in a sample of PLWD-FCG dyads. 13 A more systematic examination of day-to-day biomarker variability was considered necessary to better understand the mechanisms of the music intervention's effects in the population. Differences in day-to-day variability of the two hormonal parameters considered in this study could have arisen between the two study populations (PLWD and FCG). In particular, we assumed that PLWD may have reduced endocrine responsiveness to the change in life situation caused by the intervention; this is why we investigated the variability of the biomarkers instead of their absolute values. It was also important to compare the variability in hormonal parameters in the PLWD and FCGs with and without the intervention. In particular, consideration of the variability in relation to the mean levels (coefficient of variation) of the hormonal parameters was imperative.
Our study aimed to (1) estimate day-to-day variability of salivary cortisol and DHEA-S levels in PLWD-FCG dyads and (2) investigate differences in their variability between music intervention and control groups.
Methods
Sample and setting
This study involved secondary analysis of the data collected during a two-group, non-randomized open trial examining the short-term effects of music on physiological markers of stress among PLWD and their FCGs. 14 The data used in the present study were collected in participants’ homes in Sweden between November 2018 and March 2020. All participants provided written informed consent before data collection. The PLWD had cognitive problems but they were fully able to understand the consent statements. The study was approved by the Karolinska Institutet Institutional Review Board in Stockholm, Sweden (Dnr: 2018/1596-31/2) (2019-06-28).
A total of 34 PLWD-FCG dyads were included in the study based on the following inclusion and exclusion criteria. Eligible PLWD (1) were 65 years of age or older, (2) had received a diagnosis of dementia from a physician, (3) had moderate to very severe cognitive decline as defined by a Global Deterioration Scale (GDS) score greater than 4, 15 (4) had a Brief Agitation Rating Scale score greater than 15, 16 (5) were living at home with an FCG, and (6) agreed to participate in the study (or a proxy agreed to their participation). Eligible FCGs (1) were at least 18 years of age, (2) were the FCG of a PLWD at home, and (3) consented to participate in the study. PLWD and FCGs were excluded if they had an active mental disorder (e.g. depression or anxiety disorder) or had previous experience with music therapy.
Measures
Demographic and clinical characteristics
Demographic characteristics for PLWD included age, gender, degree of activities of daily living (ADL), months since dementia diagnosis, and severity of cognitive impairment. The Katz Index of Independence in ADL (Katz ADL) was used to assess PLWD's basic physical function and was completed by their FCGs. The Katz ADL includes six items with dichotomous response options of 0 (dependent) and 1 (independent): the items address bathing, dressing, feeding, transferring, toileting, and continence. 17 A higher Katz ADL score indicates greater independence. The GDS was used to measure the severity of cognitive impairment of PLWD 15 and was completed by the study coordinator, who has 20 years of dementia evaluation experience. This instrument addresses seven stages of cognitive status ranging from 1 (no cognitive decline) to 7 (very severe cognitive decline).
Demographic characteristics for FCGs included age, gender, and perceived general health. A single item, “In general, would you say that your health is excellent, very good, good, fair, or poor?” was used to assess FCGs’ perceived overall physical health. FCGs rated their own physical health on a 5-point Likert scale ranging from 1 (excellent) to 5 (poor).
Salivary cortisol and DHEA-S
Among both PLWD and FCGs, each participant was asked to collect 120 saliva samples. The samples were collected three times a day (twice in the morning [immediately after awakening and 15 min after the first sample's collection] and once in the evening [before bedtime]). This sampling process was to be performed 5 days per week (from Sunday evening to Friday morning) for 8 consecutive weeks. Despite our intention that participants collect saliva only on weekdays, some participants collected a few samples on weekends (Saturdays and Sundays), and we elected to include these samples in the analysis. Participants were allowed to collect the samples based on their own diurnal cycle rather than at specific times. In this study, the first morning sample and the evening sample were generally used for the analysis. On three occasions in which the first morning sample was inadequate in quantity or unusable, the second morning sample was employed.
Participants were directed to collect saliva using the SalivaBio Children's Swab and/or the passive drool method (both from Salimetrics, State College, PA; Salimetrics, 2021). No difference in salivary glucocorticoid concentrations has been observed between the SalivaBio Swab and passive drool. 18 First, participants were informed about the process of saliva collection in detail. Before saliva collection began, the study coordinator provided each participant with saliva tubes and a storage box. Participants were asked to immediately place the tubes in a designated bag and store them in their home refrigerator. Trained assistants picked up saliva samples from participants’ homes every morning and stored them in a refrigerated biological box. Samples were transported to the Biobank at the Karolinska Institutet and stored there until being shipped to a laboratory for analyses. During the 8 weeks of the study period, the study coordinator made a reminder call to participants every Saturday and also dealt with any issues pertaining to sample collection. The detailed protocol for saliva collection was described in the parent study. 14
Music intervention
The PLWD and their FCGs were assigned as dyads to a music-based intervention group or a control group. In the intervention group, PLWD and FCGs participated in an online, in-home music intervention whenever they wanted, together or alone, throughout the 8 weeks of the study period. The detailed intervention protocol was described in the parent study.19,20 In summary, prior to the intervention, the study coordinator provided an education session to the PLWD-FCG dyads in the intervention group, explaining how to access the music-based intervention. The online music program was developed by FoU Nordost, a research organization in Sweden, in collaboration with the Swedish Dementia Centre for PLWD and their caregivers. Participants were asked to listen to various songs familiar to the Swedish population, such as pop music, classical music, and traditional nursery rhymes, and create a personal playlist. We also provided participants with a compact disc (CD) player in case they did not have access to the internet. In the control group, the dyads did not receive the music intervention and simply engaged in routine activities at home. Of the 72 dyads initially approached about study participation, data for 34 dyads (24 in the intervention group and 10 in the control group) were included in the study's analyses. Compared to the intervention group, the control group showed much greater dyad dropout due to COVID-19.
Statistical analysis
All statistical analyses were performed using SAS® version 9.4 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were used to delineate demographic characteristics of PLWD and FCGs at baseline. Continuous variables were described in terms of number of observations, number of missing observations, mean, and standard deviation (SD). Dichotomous and categorical variables were described in terms of number of observations, number of missing observations, and percentage.
The three primary endpoints were morning and evening salivary cortisol and morning DHEA-S in saliva collected over 8 weeks. Due to skewed distributions of the salivary samples, all analyses for cortisol and DHEA-S values were transformed with natural logarithms, resulting in values of log morning cortisol, log evening cortisol, and log DHEA-S (in picograms per milliliter; pg/ml).
Statistical tests and confidence intervals (CI) were two-sided (where applicable), and p < .05 was used to determine a statistically significant result. No adjustments were made for multiple tests, and no imputations of missing values were made.
Day-to-day variability of salivary biomarkers
The day-to-day variability indices employed in the study were as follows: the intra (within)-individual SDs (wSD), coefficient of variation (CV), and intra-class correlation coefficient (ICC). Also, inter (between)-individual SDs (bSD) were calculated.
Intra-individual variability refers to differences within individuals across repeated observations, and inter-individual variability identifies differences between individuals. 21 The wSDs were pooled estimates based on each individual's SDs over all the individual's observations. 11 The wSDs, CVs, and ICCs were estimated from linear mixed-effects models with autoregressive errors of order one for all four combinations of PLWD/FCG and music intervention/control groups. Normality of residuals from the models was confirmed by visual inspection and the rule of thumb 22 which states that data are sufficiently normally distributed when skewness is −2 to 2 and kurtosis between −9 and 9. These criteria were fulfilled for all variables. The CV refers to the ratio of the SD to the mean value. In this study, CV was calculated using wSDs as a percentage of the total mean and was presented with 95% CIs. The ICC refers to the degree of intra-individual variability compared with inter-individual variability over time. The ICC was calculated as the ratio of between-individual variance to total observed variance (both estimated from the linear mixed-effects model) and was presented with 95% CIs. 23 ICC values exceeding 0.75 were considered to reflect good to excellent sample reliability, indicating relatively low intra-individual variability compared to inter-individual variability. On the other hand, ICC values below 0.4 were considered to indicate that a single sample would provide poor reliability for characterizing longer-term biomarker concentrations. 24
For PLWD and FCGs, the number of observations, means, bSDs, wSDs, CVs, and ICCs were calculated for all primary endpoints, and wSDs, CVs, and ICCs were compared between the music intervention and control groups. Comparisons were made using an asymptotic z-test and were presented with p-values. In sensitivity analysis, wSDs for residuals obtained from a linear regression of each primary endpoint on time in days were compared between the groups.
Results
Baseline characteristics of PLWD and FCGs
Baseline characteristics of PLWD and FCGs and of the intervention and control groups are summarized in Table 1. For PLWD, the mean age was 79 years in both the intervention and control groups, and males (at more than 60%) were dominant in both groups. ADL scores were the same in both PLWD groups at 2.4, indicating moderate to severe functional impairment. In both groups, PLWD showed a mean of 20 months since dementia diagnosis, and their GDS scores indicated moderate to moderately severe cognitive decline. For FCGs, the mean ages were 73 and 77 years in the intervention and control groups, respectively. Females (at more than 60%) were dominant in both groups. Among the FCGs, 83% of the intervention group and 50% of the control group perceived their general health as good to very good.
Baseline characteristics of PLWD/FCGs in intervention and control groups.

PLWD: people living with dementia; FCG: family caregiver; M ± SD: mean ± standard deviation; ADL: activities of daily living; GDS: Global Deterioration Scale.
aOne PLWD in the intervention group was excluded due to item incompleteness.
Day-to-day variability of salivary biomarkers
For the salivary biomarkers, the total number of observations and the values of means, bSDs, wSDs, and ICCs with 95% CIs in the PLWD/FCG intervention and control groups are summarized in Table 2. Among the 34 dyads, a total of 5791 saliva samples were employed for data analysis. Among the total samples, 1988 were analyzed for morning cortisol (PLWD = 981 and FCGs = 1007), 1984 for evening cortisol (PLWD = 989 and FCGs = 995), and 1819 for morning DHEA-S (PLWD = 896 and FCGs = 923).
Variability measures for PLWD/FCGs in intervention and control groups.
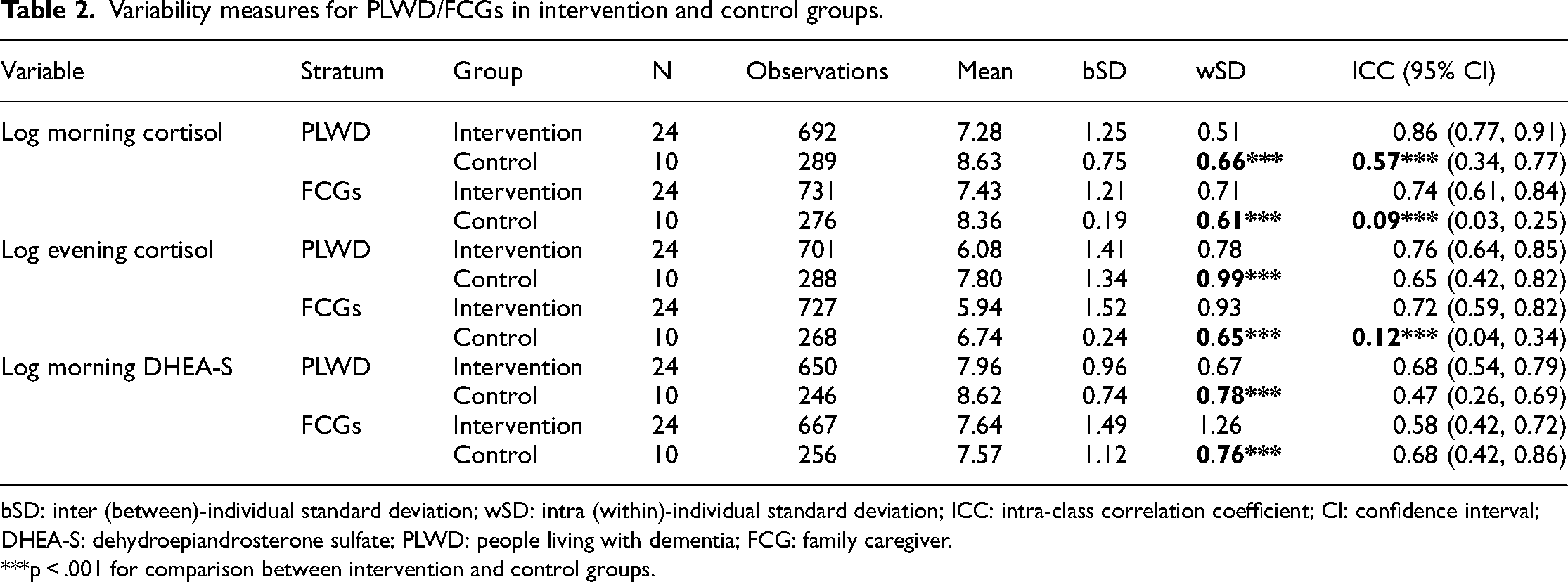
bSD: inter (between)-individual standard deviation; wSD: intra (within)-individual standard deviation; ICC: intra-class correlation coefficient; CI: confidence interval; DHEA-S: dehydroepiandrosterone sulfate; PLWD: people living with dementia; FCG: family caregiver.
***p < .001 for comparison between intervention and control groups.
Figure 1 displays intra-individual CVs (%) with 95% CIs for the three primary endpoints for both the PLWD/FCG and the intervention/control groups. The results of the sensitivity analysis in which wSDs for residuals were obtained from a linear regression of each primary endpoint on time in days were compared between the intervention and control groups, and the results were similar to those for wSDs (data not shown).

Intra-individual coefficients of variation of stress biomarkers for PLWD/FCGs in the intervention/control groups. CI: confidence interval; DHEA-S: dehydroepiandrosterone sulfate; PLWD: people living with dementia; FCG: family caregiver; MI: music intervention. *** p < .001 for comparison between intervention and control groups.
Comparison of variability indices between intervention and control groups in PLWD
The PLWD in the control group had significantly greater wSDs in log morning and evening cortisol and log morning DHEA-S than those in the music intervention group. Specifically, the values in the control group were 0.66, 0.99, and 0.78 for log morning cortisol, log evening cortisol, and log morning DHEA-S, respectively, all of which were significantly higher than the 0.51, 0.78, and 0.67 values in the intervention group (all p < .001). ICC values ranged from 0.47 to 0.86 for log morning and log evening cortisol and log morning DHEA-S, indicating relatively good sample stability. The PLWD in the control group had CVs of 7.6%, 12.7%, and 9.1% in long morning and evening cortisol and log morning DHEA-S, respectively, and those in the music intervention group had CVs of 7%, 13%, and 8.3%. However, these CV differences were not statistically significant.
Comparison of variability indices between intervention and control groups in FCGs
In contrast with the findings for PLWD, FCGs in the intervention group had significantly greater wSDs in log morning and evening cortisol and log morning DHEA-S than those in the control group. Specifically, FCGs in the intervention group showed values of 0.71, 0.93, and 1.26 for log morning and evening cortisol and log morning DHEA-S, respectively, all of which were significantly higher than the 0.61, 0.65, and 0.76 values in the control group (all p < .001). ICC values ranged from 0.58 to 0.74 for the three primary endpoints, indicating relatively good sample stability except for two ICC values for log morning and evening cortisol (0.09 and 0.12, respectively) in the control group. FCGs in the music intervention group had significantly greater CVs, showing 9.7%, 15.9%, and 16.7% in log morning and evening cortisol and log morning DHEA-S, respectively, than those in the control group (7.4%, 9.7%, and 10.1%) (all p < .001).
Discussion
This study examined the day-to-day variability of stress-related salivary biomarkers, cortisol and DHEA-S, in PLWD and FCGs and compared differences in their variability between music intervention and control groups. Many studies have identified the variability of cortisol levels in various populations, including healthy adults, 25 prepubertal children, 26 people in early adolescence, 27 people with suspected endometrial cancer, 28 postmenopausal women, 29 breast cancer survivors, 30 and caregivers of hematopoietic stem cell transplant patients. 31 Although physiological stress biomarkers can provide many benefits for measurements of treatment effects in PLWD and their FCGs, they are seldom used in these populations. 2
In a previous publication, 19 based on the same study we reported that during the music intervention period, the FCGs in the experimental group had a significantly lower mean morning cortisol level compared to the control group. However, there was no parallel significant mean difference among PLWD in the intervention versus control group. No intervention effect was observed for evening cortisol or DHEA-S. These observations prompted us to conduct the present analysis, which is focused on variability rather than mean cortisol levels. In an effort to understand whether the lack of significant intervention effects on means could be a result of differences in ability to respond, we focused on variability patterns in this study.
Our study found that PLWD in the control group had greater within-individual SDs (wSD) of the salivary biomarkers than those in the music intervention group. In contrast with the findings for PLWD, FCGs in the music intervention group showed greater wSDs of the biomarkers than those in the control group. However, when similar comparisons were made of CVs, while accounting for differences in general means, no significant differences were found between PLWD in the two groups, but FCGs in the music intervention group had significantly greater CVs at all three primary endpoints than those in the control group. Although the FCGs could be assumed to represent a group with a normal endocrinological response pattern, an explanation for no significant intervention-control group differences related to the music intervention being observed in PLWD is that they had lowered endocrine responsivity to the music intervention due to their hampered ability to respond to cortisol and DHEA-S patterns.
In a normal stress reaction, the hypothalamus releases corticotrophin-releasing hormone (CRH) that signals the pituitary gland to secrete adrenocorticotropic hormone (ACTH) into the blood. This results in secretion of cortisol from the adrenal glands. 32 The response to stress can take the form of physiological arousal (e.g. increased heart rate, blood pressure, and cardiac output) or psychological states (e.g. worry, anxiety, restlessness, or nervousness).33,34 Increased glucocorticoid levels eventually suppress CRH secretion, a negative feedback loop that plays an important role in shutting off HPA axis activation. 35 The hippocampus is a crucial area for learning and memory and plays an important role in suppressing stress-related activation of the HPA axis. 35 Previous review papers have demonstrated the relationship between heart rate variability, a general indicator of healthy physiological self-regulation capacity, and cognitive function.36–38 Compared to healthy control, PLWD were found to have significantly lower resting heart rate variability. 37 Also, lower heart rate variability has been associated with cognitive impairment that results in poor functioning of self-regulatory systems. 38 These findings indicate that a dysfunctional brain may be one of the factors associated with flattened variability. In line with such reasoning, it would have been interesting to measure heart rate variability; however, it would not have been practically feasible to do such data collection from our study participants every day for 2 months. One of the strengths of our study design is that it was possible to analyze day-to-day variability of cortisol and DHEA-S.
Based on our findings, other factors may be associated with the day-to-day variability observed in PLWD and their FCGs. The study participants had a high mean age, and the prevalence of age-related disorders was high. Many kinds of medication were taken among the participants, all of whom took Alzheimer's disease medication, and some of whom took beta-blocking agents, anti-depressants, and thyroid hormone replacement medication. The side-effects of and interactions between those medications per se may have caused reduced hormonal responsivity. It has to be taken into account that this is “normality” for this participant group.
Additionally, chronic stress may produce different biomarker variability patterns than acute stress. Chronic stress causes dysregulation of the HPA axis, which in turn affects self-regulation capacity for stress response. 2 However, most of the changes in morning and evening cortisol levels over time in individual intervention group participants were not compatible with the flattened cortisol curves (low morning and high evening cortisol) that characterize chronic stress. 13 Thus, among our participants, it is likely that moments of acute stress were accompanied by peaks of cortisol excretion in individuals with a retained capacity to regulate cortisol levels.
In a systematic review of cortisol levels of informal caregivers of PLWD, the most consistent finding was that dementia caregiving was generally associated with elevated cortisol levels, indicating greater HPA axis activity. 39 However, no previous studies have simultaneously examined the variability of cortisol and DHEA-S in the dementia caregiver population. We found that FCGs in the music intervention group had significantly greater intra-individual variability in cortisol and DHEA-S measured by CV than those in the control group.
Music has been found to be effective for stress reduction by reducing physiological arousal and negative emotions and increasing positive feelings. 40 Our previous study findings provide evidence that music may be a promising intervention for reduction of stress-related biomarkers in FCGs, 19 as they are responsive to music, but may not be effective for regulating hormonal stress in PLWD. The possibility that disabled cognitive function is associated with hampered physiological response to changes in external conditions must be accounted for when interpreting the physiological consequences of psychosocial interventions in persons with cognitive dysfunction. Future studies should examine relationships between self-regulation capacities and effects of psychosocial intervention in PLWD; such research would contribute to identification of an important factor to be considered in hormonal analyses of the effects of interventions for PLWD.
Strengths and limitations
Examination of dyadic cortisol levels can provide insights into the potential health consequences of interpersonal stress. One strength of our study is that it shows an approach that nurses and other healthcare personnel can use to work toward mitigating problems arising between PLWD and their caregivers; this approach could also apply to other kinds of patient-caregiver dyads. In this study, we observed that during the 2 months of the music intervention, the evening cortisol levels within the dyads showed a significant converging tendency. 13 When the evening cortisol level in a PLWD decreased, it tended to decrease in the caregiver as well and vice versa. As this finding shows that stress levels of the two individuals in a dyad are intimately connected, recording of biological stress levels in both the patient and caregiver may support interpretation of trends.
In addition, our findings have novelty in that they will facilitate future research on stress-related biomarkers and on PLWD and/or their caregivers. To our knowledge, this study is the first to examine the day-to-day variability of two stress biomarkers, cortisol and DHEA-S, as indicators of self-regulation capacities in PLWD and FCGs using a substantial number of salivary samples. This study is also the first to compare variability patterns of these biomarkers between music intervention and control groups. Our findings are in line with current evidence that hampered self-regulation capacities for stress biomarkers may be associated with cognitive impairment in PLWD. Use of saliva sampling with sufficiently reliable, precise, and repeatable results can contribute to development of timely interventions for PLWD and their FCGs to reduce their stress levels and mitigate other mental and physical conditions. Our examination of the variability of cortisol and DHEA-S levels based on continuous collection of up to 40 individual samples offers a better understanding of the underlying mechanisms of stress in PLWD and FCGs, which will in turn improve interpretation of biomarker results in stress and dementia research.
We also acknowledge several study limitations that should be considered in interpreting the results. First, we had a relatively small sample size and non-randomized study design. No formal sample size calculation based on a specified power was performed, so we cannot rule out the possibility that non-significant differences are effects of low power. In addition, there may have been a temporal difference between the intervention and control groups, as data from the intervention group were not collected during the same year as from the control group. According to a previous population study of differences in morning cortisol levels between seasons, 41 the impact of the difference in data collection years is likely to have been minimal because the data for both groups were collected from January through April, before seasonal changes occurred. Lastly, chronic stress may produce different biomarker variability patterns than acute stress. Future studies should identify types of stress present in PLWD and FCGs and examine their impact on variability patterns of stress biomarkers.
Conclusions
This study examined day-to-day variability patterns of stress-related salivary biomarkers, cortisol and DHEA-S, in PLWD-FCG dyads and compared their variabilities between music intervention and control groups. We found that FCGs in the music intervention group had significantly greater CVs in the biomarkers than those in the control group. Future researchers should consider the variability patterns of stress biomarkers in PLWD and FCGs when designing and testing interventions for these populations. In a forthcoming paper, we will facilitate design of future PLWD-FCG dyad studies by presenting the number of sample days needed to establish salivary cortisol and DHEA-S differences between intervention and control groups with a given number of dyads.
Footnotes
Acknowledgements
The authors would like to thank the study participants. The authors also gratefully acknowledge support from the Yale School of Nursing and the Department of Neurobiology, Care Sciences, & Society Division of Occupational Therapy, Karolinska Institutet.
Author contributions
Author's note
Azita Emami currently affiliated with Yale School of Nursing, Yale University, CT, USA.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from * Karolinska Institutet (2018/1596-31/2)*.
Funding
This work was supported by AMF Insurance Company (Dr Emami), Section of Elderly Research, in Sweden.
AMF Insurance Company in Sweden, Section of Elderly Research,
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.