
Abstract
This study aimed to evaluate a set of guidelines for music use with people with dementia. A secondary aim was to identify challenges and barriers to implementation of music interventions by caregivers. Caregivers (n = 16) were interviewed after implementing a music listening programme based on the guidelines with 29 people with dementia in home-care and aged care facilities. Caregivers found the guidelines informative, easy to understand and use. Positive effects on mood, reduced agitation and reduced challenges to care were reported. Difficulties with technology and finding time to implement the music programme were identified. Results highlight the need for more research around appropriate technology and the streamlining of processes and procedures for aged care staff. Further iterations of the guidelines will need to address these issues and consider the differing needs of home-based carers and aged care providers separately.
Introduction
Agitation and depression are frequent comorbidities of dementia. Between 20% and 60% of people with dementia and Mild Cognitive Impairment (MCI) also have Major Depressive Disorder.1,2 In addition to these high rates of comorbidity there is evidence of a bi-directional relationship between depression and dementia, with depressive episodes in later life increasing the risk of developing dementia by up to three times. 3 Risks are similarly increased in people with MCI who are twice as likely to develop dementia if they also have MDD. 3 In addition the presence of depression seems to increase rates of cognitive and functional decline as well as hastening institutionalisation in people with dementia, 4 compounding the stress upon caregivers and health services. 5 Agitation similarly occurs in up to 80% of people with dementia, 6 imposing additional stress on patients and caregivers, increasing disability and diminishing quality of life. 7
The presence of multiple co-morbidities and high levels of polypharmacy makes pharmacological approaches to addressing depression and agitation problematic in people with dementia. Antidepressants, anxiolytics and antipsychotics often used to treat depression and agitation in dementia are associated with side effects including nausea and insomnia, 8 and even adverse clinical events such as increased confusion or death. 9 Thus many bodies of experts from across the world recommend that non-pharmacological treatments be used as a first line treatment for the psychological and behavioural symptoms of dementia.8,10–12 Despite these recommendations, pharmacological treatments are still widely used. In fact a recent Royal Commission into Aged Care Quality and Safety in Australia identified a significant need to reduce the use of chemical restraints for dealing with behavioural symptoms of dementia in aged care facilities in that country. 13 Thus there is a great need for long-term residential aged care facilities to have access to cost effective, non-pharmacological approaches to managing these symptoms.
Music provides one such approach. Systematic reviews have highlighted numerous studies demonstrating the positive effects that active music therapy such as singing and playing musical instruments can have on depression, agitation and cognitive functioning in people with dementia.14,15 However, the response to music in people with dementia is not always positive. Several studies have shown that some individuals with dementia may fail to respond, while others may even respond adversely.16–20 This is particularly of concern where programmes are being implemented without the guidance of a trained music therapist, such as in programmes run by aged care staff or volunteers who may not recognise the potential for adverse reactions such as overstimulation, emotional flooding or the triggering of distressing memories. 21 These concerns highlight the need for evidence-based guidelines for the use of music with people with dementia. Indeed it is often the lack of such standardised guidelines that inhibits caregivers and medical professionals from implementing non-pharmacological solutions to managing the symptoms of dementia. 22
Based on this need, our team developed a set of written guidelines entitled Music Playlists For People With Dementia: A Guide for Carers, Health Workers and Family (referred to hereafter as ‘the Guide’). 23 The Guide draws on research from both music psychology and music therapy and was developed using standard procedures for development of guidelines in healthcare contexts, which included a systematic review of the evidence, and close consultation with caregivers and aged care providers.24,25 The Guide outlines strategies for identifying individuals who may be vulnerable to negative responses, offers tactics for the creation of playlists designed to address key challenges to care, and provides suggestions about programme monitoring and integration of music into care plans for people with dementia.
The current study reports on the qualitative analysis of data obtained in a trial of the Guide with patient-caregiver dyads. The aim of the study was to evaluate how helpful the guidelines had been and to identify further challenges and barriers to implementation of music programmes by caregivers.
Methods
Interviews were conducted with caregivers in both aged care facilities and home-based care contexts, drawing on principles of grounded theory 26 in the approach to data collection and analysis, although theory development was not the aim of the analysis. As in grounded theory methodology, we took an inductive approach to exploring the research questions without prior hypotheses. 27
Participants and recruitment
Ethics approval was granted by the Human Research Committee at Western Sydney University. Participants were recruited from aged care facilities and support groups for caregivers in NSW, Australia. Organisations were randomly selected and contacted by email or phone and invited to participate in developing a personalised playlist programme for people with dementia in their care using our guidelines. When interest in participation was expressed a visit was made by a member of the research team to talk about the research and distribute information sheets and consent forms. Written consent was sought from both the person with dementia who would be listening to the music (or a legal guardian where appropriate) and the caregiver who would prepare the music and participate in the interviews. Inclusion criteria for the person with dementia was a score on the Standardised Mini Mental State Exam (SMMSE) 28 of less than 25 indicating the presence of some cognitive impairment. There were no exclusion criteria for caregivers.
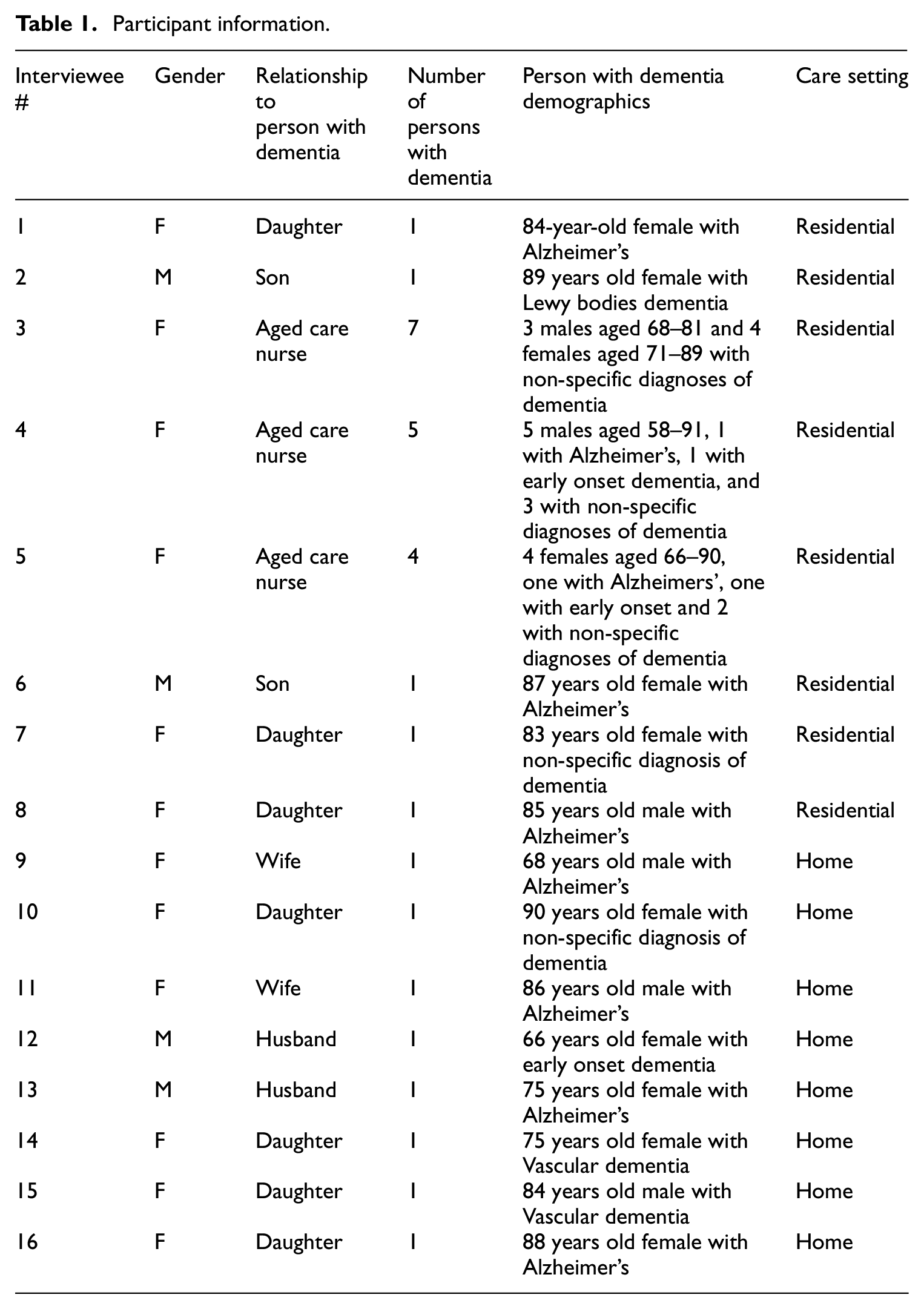
Participants in the music listening programme included 37 people with dementia and 18 caregivers. Four of these caregivers were staff from three different aged care facilities who participated along with more than one resident with dementia (range of 4–7 residents per staff member, n = 23), nine were family caregivers, and five were family members of individuals living in residential care. Two caregivers (one from an aged care facility, and one home-based carer) were unable to participate in the interviews, giving a total of 16 interviews with caregivers of 29 people with dementia (see Table 1).
Participant information.
Materials and Interview Procedures
After obtaining informed consent caregivers were visited by a member of the research team and given a written copy of the Guide, a set of Phillips Lightweight Over-Ear Hi-Fi headphones (SHP1900), a SONY NWZ-B183F MP3 walkman, and a $AUD30 iTunes voucher for downloading music for each person with dementia participating in the trial which they were able to keep after the end of the 2-month study period. Each caregiver was given approximately -1 hour training in how to use the equipment and prepare playlists. Carers were given 2 weeks to prepare one or more music playlists based on the individual’s preferences as recommended in the Guide. The Guide also gave suggestions about the musical features that might be most appropriate for use in addressing key challenges of care identified by the caregiver. After 2 weeks the caregiver received a phone call from the research team in which any technological issues or questions were addressed, and were then asked to begin using the music playlists regularly over a 4–6 week period.
At the conclusion of the music listening period interviews were conducted in person at the home or office of the interviewee by the first and second authors, and recorded using Voice Recorder Lite Version 4.0.1 on an Apple iPad 2. Interviews were conducted in a quiet place either alone or in the presence of the person with dementia and took place over a 4 month period in 2019. An interview guide was used, however, interviews were allowed to proceed freely based on participant responses.
Analysis
Interviews were transcribed verbatim. A preliminary analysis was conducted using open coding as described by Strauss and Corbin. 29 A second wave of analysis involved identifying data categories and themes that connected the various concepts in the data. In total, 264 segments of data were allocated to the data categories. Axial coding as described by Charmaz 30 was then used to discern connections and relationships between data categories and sub-categories and themes were generated within the larger data categories. In a final wave of analysis themes were compared across people in home-based care and people in residential care to determine whether the challenges and benefits differed depending on the context in which the music programme was being implemented. The final analysis resulted in 2 broad data categories relating specifically to the aims of the study, and 9 themes, most of which were replicated across the two samples (residential and home-based care), although sub-themes were not always the same (Tables 2 and 3).
Data categories, themes and sub-themes for people with dementia in long-term residential care.

Data categories, themes and sub-themes for people with dementia in home-based care.

Findings
Evaluation of the Guide
Guide content
Both participants from aged care facilities and home-based caregivers agreed that the Guide was straightforward and easy to follow. However, several participants felt that the information could have been presented with less detail. The summary boxes contained in the Guide were seen as useful, although it was suggested that more information could have been presented that way. As Participant # 8 stated ‘The contents are good. I guess some of the text, more of it could be in summary boxes, so that maybe you could do it in a box at the top and then for further reading’. As noted by the same participant, people vary in their need for detail: ‘There would be people here that would be detail oriented and they would want to read every word’. In fact another user indicated that she would have liked more detail, particularly about previous research and other available music programmes for people with dementia (Participant 14).
Specific segments of information in the Guide were perceived as particularly useful. Participants in both groups especially appreciated the music suggestions found in the appendix of the Guide. As one participant stated, ‘I thought that was quite helpful because it reminded me of other tunes that mum liked’ (Participant 1). Caregivers also appreciated being alerted to the potential for negative responses and the influence of mental health issues. One participant said, ‘I highlighted things particularly about depression and anxiety’ (Participant 8). Another stated that that information ‘meant a lot to me’ (Participant 2). Others found it useful to have pointed out the need to monitor responses and modify playlists based on these responses. As one aged care nurse stated, ‘If you walk away you wouldn’t know what use it was. I think it’s important to stay with them’ (Participant 3). Another stated, ‘I didn’t know until I played the full – I think it’s about an hour and a half of music – what would get more conversation or a change of mood’ (Participant 8).
Information about strategies for music selection found in the Guide received a varying response from participants. Participants appreciated information about things such as the ‘reminiscence bump’– the idea that personally relevant music from the critical period of late adolescence and early adulthood will be more effective in triggering memories or emotional responses. 31 Some also found suggestions about choosing specific music to achieve particular mood effects useful. One home-based carer stated, ‘I enjoyed reading about the different tempos and things of the music. I thought that was really interesting and obvious really, but I just hadn’t thought about it’ (Participant 14).
However, other participants felt that selecting music according to tempo or other musical features was unnecessary. For example, one participant said, ‘I’ve only got a case study of one, but I think it [the Guide] may overestimate what can be done with varying the different aspects of music, such as its tempo and whatnot’ (Participant 2). The same participant added, ‘[The effects] might be there to some extent, but they’re not going to be the main thing’. Another participant described finding that information ‘a bit too much’ (Participant 9). She described her reaction to reading this in the Guide, saying: ‘Oh my goodness, now I’ve got to look at the music sheets and look at F and M and all this?’ At the end of the day all he needs is something that he loves to listen to. That would have been so much simpler (Participant 9).
Participants in home-based care seemed to particularly find this type of information less useful, arguing that their intimate knowledge of the listening tastes of the person with dementia made some of the information contained in the Guide irrelevant. For example, one daughter said, ‘A lot of these things I didn’t need. I guess I was lucky because I didn’t have to start from scratch or wonder what on earth my mother liked to listen to. I knew’. (Participant 10). Similarly another participant stated about his wife: There are pages on the rhythm and I think, ‘Oh I don’t need any of that, I know the music she likes’. Sometimes it’s fast and sometimes it’s slow. A lot of that is written for a person that is not an intimate carer (Participant 13).
Listener response
Caregivers noted many positive benefits for listeners from the music programme both in home care and in residential care. Substantial improvements in mood were noted on many occasions. One aged care nurse stated, ‘I was really, really surprised. Pleasantly surprised I must say. I was really surprised to see the difference it made’ (Participant 3). This participant described a particular instance of witnessing this, saying: Just one lady, she has dementia and she loves music but her reaction was amazing. I never expected it. She was crying with happiness. She just could not believe that all her favourites were just all coming out one after another. She was listening and tears were running down her face. She was singing at the top of her voice and she got up and did a little dance to all of her favourites (Participant 3).
Other positive mood effects the music listening had on participants were described as ‘giving her that bit of pleasure’ (Participant 13), feeling ‘happy every time she had the music on’ (Participant 12), making them ‘feel important’ and ‘more relaxed’ (Participant 3), boosting the participant’s ‘energy level’ and putting ‘a spring in his step’ (Participant 9). Some noted behavioural indicators of enjoyment such as ‘clapping his hands in enjoyment’ (Participant 9), ‘tapping her foot or tapping her hand’ (Participant 10), ‘whistling and then humming a bit’ (Participant 12). One participant said of his mother, ‘She would come to life if she was flat. She would settle down if she was restless’ (Participant 2).
Caregivers also reported some positive effects of music listening on symptoms. The husband of one participant with dementia who was hospitalised while participating in the study spoke about how staff at the hospital used the music for the agitation his wife often experienced towards the end of the day: ‘they are using the headphones at the end of the day to calm her down’ (Participant 13). Another reported, speaking of his mother’s agitation, ‘the music brought short periods of repose and otherwise seemed to arrest the typical and expected escalation of this sort of presentation after a sleepy day’ (Participant 2).
Some caregivers reported that the music increased opportunity for conversation and reminiscing and overall provided mental stimulation. For example, one participant said of her husband: He would bring up old memories. He remembered, ‘We used to do this and we had parties’. It’s not only about the ears. It’s about thinking about what that song means or something. You can then start talking about things that relate to that. (Participant 9).
Another participant noticed that the music seemed to reduce hallucinations and involuntary movements in his mother, calming her to the point where she would be more likely to eat well if the music had been used just before a meal. He stated about one listening session: ‘She ate a good-sized lunch very well. No hesitations or refusals. Finished all in twenty minutes, exceptionally quickly for her’ (Participant 3).
Despite these effects, responses to the music were not always positive. Some caregivers reported participants whose response was minimal: ‘I didn’t get much response from X (Name has been removed for privacy reasons). Sometimes a smile’. (Participant 5). Some participants didn’t want to listen to the music at all. As one daughter stated: On several occasions mum didn’t want to listen to the music. Some of the time when I wanted to play her the music she didn’t want to. Other times she enjoyed the music for a short period and then would want to stop (Participant 1).
Participant 1 put this down to her mother’s low mood, stating: ‘Mum’s quite withdrawn and she doesn’t like to get involved in activities’, and ‘It’s hard to do things to improve mum’s quality of life because she’s so resistant to doing anything’ (Participant 1).
While such reports were not frequent, some participants noted that negative responses could also occur. For example, Participant 2 stated, ‘Whilst music is good, I’ve found that on the whole silence is better. You have to be careful with music, because if you get it wrong it can be worse than not having it’. He gave an example of this, describing one occasion on which his mother was crying and becoming upset by the music. Participants noted a number of factors that seemed to be able to contribute to negative responses, including mood, general wellbeing and comfort level at the time, and the volume or familiarity of the music. Other caregivers also reported occasions where the music brought up distressing emotions, or even caused anxiety when the listener couldn’t remember the words of songs they used to know.
Effect on caregiver
Caregivers also reported ways in which they had benefited from the music programme. For example, one carer reported that she was able to get things done such as preparing dinner while her husband was occupied with listening to the music (Participant 11). Another said, ‘That’s my zen time when he’s listening. As a carer it gives me some time to just sit down and look at my emails’ (Participant 9). By making symptoms more manageable, the music programme also reduced caregiver stress. As Participant 2 stated about himself: ‘It certainly was enjoyable for her carer who does not enjoy the evening periods of restlessness approaching true agitation. This was very regular before the programme commenced and is now becoming irregular’.
Because of its potential to help ward off difficult emotional reactions, caregivers described using the music to manage situations that would usually cause distress including mealtimes, going out, bedtime, and hospitalisations. One participant described a situation in which her mother was hospitalised stating, We had to use [the music] as a different sort of tool while she was in the hospital that really surprised us and the staff that were looking after her. The security that it gave her and the difference it made to her daily routine being in a busy medical ward, i thought that was really valuable. It meant that it was a transportable tool. It had an immediate effect on her of distracting her because she was having a lot of blood taken and people prodding and poking and all that sort of thing (Participant 14).
Another benefit to caregivers was that it helped them to create a good atmosphere: It’s like having a permanent presence in the house. It [the music] has it’s own personality and it does fill the atmosphere like a cushion. And it’s a cushion of sounds and it’s beautiful sound. I think it’s emotionally sustaining because after all these weeks, it’s still giving me pleasure (Participant 10).
It also helped the caregiver to relax in stressful circumstances. As described by Participant 8: You’re walking in there knowing that there might have been a fall or there might be some eczema or she might be in the same clothes as the day before. I found it useful for collecting myself and sitting just privately in the other chair to just be present and then have it in the ear piece (Participant 8).
For others the music provided an opportunity to share, ‘It’s extra nice when there’s something that we’re enjoying together and it did do a bit of that when she was in the right mood’ (Participant 1). For others the experience of selecting music and finding ways to use it was an enjoyable way to draw other family members into the caregiving experience. One participant stated, ‘It was great to involve him. My husband sat down and chose a lot of the music. I was the one who instigated playing the music but he was the one who actually did the playlists’ (Participant 14).
Barriers and challenges to implementation of music programmes
Technology issues
Whereas caregivers associated with long-term residential facilities identified a number of challenges, technology issues appeared to be the primary challenge faced by home-based carers in implementing the programme. Some found the MP3 players and headphones challenging to use or unsuitable for their needs. For example, despite the provision of written instructions and face-to-face assistance from the research team, some had to get help from family or friends to download the music or ended up just using CDs or other devices to play the music. As one home-based carer stated: ‘Of course actually setting up the music – I was not very good at it’ (Participant 9). Similarly, a participant whose mother is in residential care said: ‘We did have some difficulty working out how to get the music onto the MP3 player’ (Participant 7).
Some found the screen of the MP3 player too small to be able to see and easily use. Others found that the headphones were either not tolerated by the person with dementia, or were not ideal because they did not allow the caregiver to listen to the music along with the individual with dementia. As one participant stated: ‘I was apprehensive about the headphones so I bought myself a little speaker. I quite often like to sit with her, so that was good because then I could hear too’ (Participant 13). Other participants agreed that monitoring responses would have been easier if the caregiver had been able to listen to the music with the person with dementia. One said, ‘At ten or fifteen minutes mum smiled, opened her eyes and said, “isn’t that lovely”. I did not know exactly what that piece of music was and I didn’t want to take the headphones off her’ (Participant 2). One aged care nurse said, ‘Some people found the headphones a bit awkward to manage, and the little device, the little black thing, they weren’t able to manage that themselves due to arthritis in the hands, poor eyesight, stuff like that’ (Participant 3).
One participant also reported that her mother developed a great deal of anxiety about losing her equipment in the residential care facility, which interfered with her ability to enjoy the programme. She stated: There was a woman at the nursing home who was taking things, which is what happens sometimes, I guess. My mother got very paranoid about leaving it there. It did go missing and we found it a day or two later, but that stressed her. So I kept it with me and just played it when we were together. I think the staff would have done it but she was just too anxious about it (Participant 7).
Both home-based caregivers and those associated with residential care facilities noted that it would have been helpful to have more information about technology included in the Guide. As one aged care nurse stated, ‘I probably would have liked more exactly on how to put the music on and make a playlist properly and that kind of stuff’ (Participant 4).
Music selection
Home-based caregivers did not report any challenges to selecting music, possibly because of having access to the music the individual was used to listening to already, and having day-to-day experience with their response to music. However, for some individuals in residential care contexts some challenges were identified. One caregiver stated that finding the correct version of a song was difficult. He stated, It’s sometimes hard to get the version you want. And as the Guide makes clear, it can be the particular singer that had an effect rather than the particular song. I had to pass up a piece of music which I knew was a favourite because I couldn’t get the correct version. We put in the substitute version which I took out because it wasn’t doing it (Participant 2).
For some participants with low levels of cognitive decline, preparing playlists that gave them enough variety was another challenge. One participant in an aged care facility who had been very excited about having access to music at the beginning of the study became bored with the playlists after a while. As his caregiver stated: ‘Toward the end, because it was the same playlist – he wanted some different stuff. I said, “do you want to listen to it today?” He said, “no, same stuff”’ (Participant 4). Another issue identified was that the volume of the recordings can be quite variable. Sources such as iTunes don’t have a set volume for downloads, and the volume has to be set manually for each track downloaded in order to avoid some tracks being too soft or too loud, which in some cases caused discomfort to the listener.
Staff time
The time required for staff to prepare playlists, organise equipment, and monitor responses was a significant challenge in the aged care facilities involved in the study. For some, it was filling out forms associated with monitoring the playlists that were time consuming. For others, the need to stay with participants while they were listening took significant amounts of time that were difficult to find. As one aged care nurse stated, I found it a little bit time-consuming. Maybe more time-consuming than I expected because you had to leave it with the resident for a half an hour. Sometimes I had to stay with them because if the headphones moved they didn’t know how to fix them. There was no point in continuing (Participant 3).
Another nurse similarly said, ‘It’s just about having the time. Even though this is only a twenty-bed facility, their needs are really huge. It’s absolutely hectic up here no matter what time of the day it is’ (Participant 5). Participant 1 similarly felt that the staff at her mother’s facility faced too many time pressures to think about playing music. She stated: I was not here all the time to make sure it got done regularly and the staff here had probably more important or bigger priorities and so it got forgotten about as well. I don’t think that we probably utilised it as much as we could have (Participant 1).
This participant suggested that if it had been a part of the daily scheduling, staff members might have utilised the music more frequently with her mother.
Staff commitment
In addition to time, staff commitment to the programme was also identified as a challenge. Participant 5 had some particularly insightful suggestions in relation to this. She discussed how other staff in the facility tend to view music as purely entertainment rather than as part of symptom management. She said, ‘I don’t think they’re thinking of it as a way to manage behaviours or anything like that. I think a lot of the time listening to music just wasn’t on their radar’. She suggested that educating more of the other staff would have added to the success of the programme, saying: I would have loved it if you came up and we had a toolbox talk and all the staff were there. Then they would have learned about it because I think relaying that to them and getting them to implement it – but I think if you were there and they saw that it worked, I think it would have had more impact in a way. If you were to do it and say ‘I’m not just going to talk to two people, I’m going to talk to the whole team’, everyone would have been more involved I think (Participant 5).
Participant 1 also felt that the use of music needs to become part of the care routine of those residents who are benefiting. Citing the case of one resident who had participated, she said: Everyone knows that X loves music so they just put the headphones on automatically. Because it was easy to do and it was something that was part of their routine. They know the drill that if someone’s upset there are catalysts that you have to look for. After those are met one of those scenarios could be to just try music to see if it will calm them down. I need to write a little print out and put it in the medication book (Participant 5).
Discussion
This study aimed to evaluate the usefulness of a printed guide to music use for caregivers of people with dementia, and to identify challenges and barriers to implementation of music programmes. Participants reported that they found the Guide easy to understand and use, and appreciated the information provided therein including music recommendations as well as the need to be aware of the potential for negative responses and to monitor responses for that reason. Nevertheless, participants made some useful suggestions for improvement, including suggesting that information could be presented more simply with options for further reading for people interested in more detail. Previous research has demonstrated that health materials can benefit from the use of plain language and a limited number of key points in order to enable readers to process the materials with ease. 32
The need to balance simplicity with informativeness and credibility in materials intended for an audience that includes both family members of people with dementia and health practitioners was a challenge in the development of these guidelines. In fact, in general, best practice guidelines are usually developed for the use of health professionals, while simpler materials might be developed for improving health literacy in members of the public. However, previous studies into the appeal of health-related interventions have demonstrated that some users don’t want to read materials that are too simplistic. 33 As the current study has demonstrated, both health professionals and others differ in their need for, interest in, and time to absorb various levels of detail. Nevertheless, this study suggests that future iterations of the Guide might benefit from having separate versions for family members and health practitioners. This was further reiterated by the fact that home-based carers faced fewer and different challenges to implementing the programme, and found some of the information included irrelevant given their intimate knowledge of the persons with dementia they were caring for.
Overall, participants with dementia responded well to music programmes implemented on the basis of the guidelines. Listening to music not only had a positive effect on mood, but also reduced agitation and made challenging times of day such as mealtimes or evenings less stressful for caregivers. For several, music also proved to be a tool for managing other difficult situations such as hospitalisations.
Some participants did not feel that the information in the Guide relating to musical features such as tempo was necessary. Indeed, there is support for the idea that merely listening to one’s favourite music can have a distracting and mood-improving effect without further regard for musical features. For example, it is well known that the pleasure and reward systems of the brain are activated when listening to music that one likes. 34 One study using functional magnetic resonance imaging (fMRI) found that brain activation in emotion-related and reward centres of the brain is particularly high when listening to familiar rather than unfamiliar music. 35 Studies of people with dementia have also shown that music programmes that rely merely on the selection of favourite music can often be effective in reducing agitation.36,37
However, there is evidence that the reward systems in the brain are not so easily activated in people with depression when listening to music. 38 Thus several studies have reported that protocols based purely on favourite music or age appropriate selections are not always successful, particularly in people with depression.18–20 Furthermore, studies with people with dementia have demonstrated the potential for both the mental health history of the individual 16 and musical features 17 to have an impact on mood outcomes of music programmes. This reiterates the need for people with a history of mental health conditions to be treated with more care than other participants. Trained music therapists can play an important role in determining the best approach for each individual with dementia. Nevertheless, where there is limited access to a music therapist, caregivers and health practitioners can follow best-practice guidelines to help them understand how to approach music selection.
Some of the most important information that has emerged from this study relates to the challenges to implementing music programmes with people with dementia. A key challenge for both home-based caregivers and people in long-term residential care was the need to find appropriate technology. Indeed this is something that has been seldom studied in the literature. One case study compared the use of headphones to speakers in a single participant and found that both conditions were equally successful. 39 Other studies have demonstrated that, despite popular perceptions that older adults are not comfortable using technology, touch-screen devices and other interactive devices can be used successfully for people with dementia. 40 However, no published research to date has systematically addressed the issue of technology in music programmes for people with dementia. Again, it is likely that there is no ‘one-size-fits all’ approach. Devices that enable the caregiver to listen to, or at least view what the person with dementia is listening to are likely to be needed for effective monitoring of music sessions. Nevertheless, further research in this area would enable future guidelines to make evidence-based recommendations on this subject.
Other challenges identified in this study relate to the importance of streamlining procedures and processes and ensuring that as many staff as possible are educated about the effective use of music. Care staff in long-term residential facilities often face immense pressures to adapt to changing governmental and market demands in the industry, while coping with a lack of financial resources and understaffing. For music programmes to be integrated successfully into care plans in residential care environments staff need to be convinced of its benefits and have a full understanding of how it can be used to reduce caregiver burden and reliance on medication to manage some of the challenges of dementia. While the use of best-practice recommendations such as the Guide evaluated in this study can go some way towards addressing this, there is a further need for education and training programmes for care staff, and the development of procedures at an organisational level that will see such programmes become a part of care routines.
Future research could benefit from exploring the research questions using a broader sample of staff from differing roles in residential aged care. Nevertheless this research has highlighted some important issues and the need for further systematic study in a number of areas that will be crucial to the success of future music interventions for people with dementia. It is our hope that continued work in this field will help caregivers to understand more about the potential for music to be used effectively to improve quality of life in people with dementia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an NHMRC-ARC Dementia Research Development Fellowship to the first author.