
Abstract
Objective:
We sought to characterize the clinical prognostic factors in veterans with amyotrophic lateral sclerosis (ALS) followed in our ALS clinic.
Background:
ALS is a rare, progressive neurodegenerative condition associated with decreased survival compared to that in the normal population.
Method:
The electronic medical records of 105 veterans diagnosed with ALS who are followed in our ALS clinic between 2010 and 2021 were reviewed. Approval from the institutional review board was obtained from the study protocol. Demographic and clinical variables included age at symptom onset, age at initial evaluation, survival (from symptom onset to death), gender, site of onset (appendicular, bulbar, and respiratory), initial amyotrophic lateral sclerosis functional-related score-revised (ALSFRS-R), total functional independence measure (TFIM) scores, initial forced vital capacity (FVC), and interventions (Riluzole, gastrostomy, noninvasive ventilation [NIV], and tracheostomy). Normally distributed data was expressed as mean ± standard deviation. Fischer's exact analysis of the distribution differences of categorical data. The Kaplan–Meier plot analyzed the time-to-event.
Results:
The mean (SD) age at symptom onset was 62.0 (11.1) years, age at diagnosis was 65 (11) years, with 72% of the patients being over 60 years at diagnosis. The median survival time from symptom onset was 4.12 (3) years. Limb-onset ALS (appendicular) was the most frequent (52%) followed by bulbar-onset ALS (43%). The mean ALSFRS-R and TFIM scores were 31 (8) and 91 (25), respectively. Family history (familial), bulbar, and respiratory presentation at diagnosis were associated with shorter survival times.
Conclusion:
This study suggests that of the clinical prognostic factors veterans with familial ALS, bulbar, and respiratory onset at presentations had shorter survival. The presence of Agent Orange, PEG placement, and NIV did not affect survival.
Introduction
Amyotrophic lateral sclerosis (ALS) is a rare, progressive neurodegenerative disease with a fatal outcome in which 50% of the affected individuals are dead within the initial 2 to 5 years of the first symptom onset.1,2
Prior studies have suggested risk factors responsible for ALS in veterans include exposure to organophosphorus pesticides and chemical nerve agents, mercury-containing vaccines, alpha particles emitting heavy dust from exploding (depleted uranium) ammunition, and head trauma in veterans with ALS.3–5 Intense (strenuous) physical activity military personnel undergo has also been considered a risk factor for the death of motor neurons. 6 Weisskopf et al. in their prospective study showed those who served in the military (veterans) had a higher mortality rate than expected in comparison to those who did not serve in the military. This increase in mortality rate was evident across all military branches (though to a lesser extent for the US Marine Corps), independent of the number of years served in the military, and the self-reported exposures to the number of lifetime exposure to known occupational toxins. 7
The risk of ALS in veterans is 1.5 to 2 times the rate of the general population among young US military veterans in their 20s through 40s who were deployed to the Gulf War compared to non-deployed veterans.8,9 This increase in ALS incidence was noticed across all military branches, but significantly among the Army and Airforce branches of service. 8 This increase in ALS incidence was noticed over an 8-year study period (1991–1998). 9 Lastly, a recent review by the US Institute of Medicine Committee found “limited but suggestive evidence of an association between deployment to the Gulf War and an increased risk for ALS” with ALS developing later in their life among veterans deployed to the Gulf War than non-deployed veterans. 10 Thus, ALS is now considered by the US Department of Veterans Affairs (VA) as a service-connected disease, which makes veterans eligible for VA Health care and disability benefits.
In the absence of an underlying etiology responsible for ALS and poor prognosis for any individual patient with ALS, clinicians have been unable to provide well-reasoned prognosis to newly diagnosed patients and their families. It is unclear which clinical variables are important for predicting survival. Prior population-based studies have identified older age (>75 years), female sex, BMI <25 kg/m2, rapid disease progression (shorter time from symptom onset to diagnosis indicate an aggressive disease), and bulbar-onset were poor prognostic factors.11–14 Dysphagia, forced vital capacity (FVC) <50% of predicted, and high arterial carbon dioxide pressure (PaCO2 40 mmHg or higher) are significantly associated with poor prognosis.15,16 In a recent large European cohort study older age, bulbar-onset, C9orf72 mutation, FVC <50%, and presence of frontotemporal dementia were shown to be poor prognostic factors. 17 The main shortcomings of these outcome studies have been that in the population-based case-control studies diagnosis could be less certain with key clinical features missing compromising its validity, while in the placebo arm of pharmacological trials enrolling younger motivated ALS patients do not reflect the general ALS population and so prone to selection bias. Likewise, risk factors of prognostic importance are overlooked in both sets of studies.
The causes of death have mainly been respiratory failure in 80% 18 and malnutrition (defined as BMI <20 kg/m2) in 20% of cases. Malnutrition was present in 16.4% of cases and associated with a 7.7-fold increase in risk of death in a prospective 7-month study of 55 ALS patients. 19 Though PEG helps by avoiding starvation, dehydration, and improving QoL, the effect of enteral nutrition via PEG on survival has presented with conflicting results. 20 In ALS patients PEG placement was shown to result in a longer survival time of 23 (15–35.5) months compared to the NoPEG group of 11 (4.75–18.5) months (p = 0.01). 21 Respiratory functions after PEG placement is the main predictor of the duration of survival.22–24
Involvement of inspiratory and expiratory respiratory muscles including the diaphragmatic dysfunction from phrenic N degeneration affects breathing and REM sleep. Early (before hypoventilation occurs) noninvasive ventilation (NIV) use has been shown to improve QoL and survival by approximately 13 months,25–28 compared to late NIV initiation.14,29 The main drawback with NIV use is compliance, as its efficacy is affected by NIV mask leaks, the presence of excess salivation gives a feeling of drowning in one's saliva, the inability to cough, and having an oral intake.
Most of the studies on ALS have been conducted in the general population and few in the veteran patient population, who make up 7% (22 million) of the US population. This study was conducted to investigate the clinical prognostic factors for survival among military veterans with ALS, who were periodically seen in our ALS clinic from 2010 to 2021. The prospectively gathered information will help us investigate underlying etiological factor(s), plan future clinical care decisions and preventive interventions to improve ALS care, and design future clinical trials.
Methods
Subjects
This is a single-center, observational study retrospectively analyzing prospectively collected electronic data of all veterans diagnosed with definite/probable ALS by the El Escorial criteria 30 and supported by neurophysiology testing. This study protocol is identical to our recently published study of the mortality prediction model in veterans with ALS. 31 In brief veterans were periodically followed every 4 months in our ALS clinic at the Oklahoma City VA Medical Center (OKC VAMC) from 1/1/2010 to 12/31/2021 were enrolled. The OKC VAMC as an ALS Regional Center of Excellence provides ALS-specialty care as a continuum in the disorder's acute, chronic, and long-term phases following the Veterans Health Administration policies. The ALS clinic has a structured set-up in which the veterans with ALS meet in a room simultaneously with multidisciplinary team members comprising a neurologist, respiratory physician, physician assistant, occupational, speech and respiratory therapist, dietician, prosthetist, social worker, and clinic coordinator.32–34
The inclusion criteria for this study were complete electronic records of veterans regularly followed in our ALS clinic including the use of gastrostomy and NIV. The exclusion criteria were incomplete electronic records, including a lack of documentation of the use of gastrostomy and NIV.
The demographic and clinical variables collected were the age of symptom onset, age at initial evaluation, survival (from symptom onset to death), gender, site of onset (limb/appendicular, bulbar, and respiratory), body mass index (BMI), initial amyotrophic lateral sclerosis functional-related score-revised (ALSFRS-R), 35 total functional independence measure (TFIM) scores,36–38 initial FVC. 39 Presence of co-morbidities such as hypertension, hyperlipidemia, diabetes mellitus, current smoking habit, presence of ALS-related complications such as depression, and interventions (Riluzole, gastrostomy, NIV, tracheostomy) shown to prolong survival were recorded. 40 PEG placement was advised both on initial evaluation and subsequent follow-up visits (at various stages of the disease) in detail when the patient complained of significant dysphagia (such as choking on solid food, thin liquids, and on swallowing medication) which was confirmed by bedside swallow test and modified barium swallow. PEG placement was also advised if there was significant weight loss, 5% to 10% of their premorbid weight. Veterans were advised to undertake early endoscopic PEG placement when they had adequate lung capacity (FVC > 50%) to reduce the complexity of placement. During this session, the risk of PEG placement was discussed such as procedure-related transient laryngeal spasm, gastric hemorrhage, and failure to place the PEG due to distorted local anatomy. Veterans and family members were informed how proper PEG care was essential to prevent tube blockage, tube displacement, and infection at the tube site. Administration risks such as formula intolerance (diarrhea, constipation), bloating from abdominal distension, and aspiration pneumonia could result if the formulation was administered without proper precautions such as gravity feed or via a feeding pump and the head not being raised at 45 degrees. Likewise, NIV usage was recommended on initial evaluation and subsequent follow-up visits (at various stages of the disease) when FVC was 80% or lower (as we considered FVC higher than 80% to be normal lung function). Our program utilizes the FVC and PaCO2 to measure respiratory function as they are easy to administer, low-cost, reproducible, and widely accessible to all health facilities. Veterans who were reluctant to agree to either procedure and wanted time to discuss these interventions with their family and friends were followed up by a phone call 1 to 2 weeks later as to their decision.
This study meets the STROBE guidelines and the information required is reported accordingly (see the Supplementary Checklist). This study was approved by the Oklahoma University Institutional Review Board (IRB# 10358) after determining that the study was exempt from veterans’ informed consent because of the retrospective review of electronic medical records, veterans were still being followed clinically, and most of the veterans had died.
Statistical analysis
Summary statistics were reported according to data type, including mean, standard deviation (SD), median, maximum, minimum, count, and proportion. Differences in the distribution of categorical variables were analyzed using Fisher's exact test. Survival was defined as the time from the onset of symptoms to death. Time-to-event analysis was analyzed using the Kaplan–Meier plot, and comparisons among variables used the log-rank test. The Cox proportional hazards model performed the multivariate analysis. The proportional hazard (PH) assumption was examined using the R function cox.zph based on weighted residuals. 41 Hazard ratio (HR) with 95% confidence intervals (CI) measured the effect sizes. Statistical significance was defined as a p-value < 0.05 using two-tailed analysis. Statistical analyses were performed using the R 4.0 version (Vienna, Austria).
Results
The clinical characteristics of our study sample of 105 veterans with ALS based on their initial clinic visits over 11 years are described in Table 1. The mean age at symptom onset, diagnosis, and death (± SD, years) were 62.0 (11), 65 (11), and 67 (11), respectively. There were 101 (96%) men and 95 (91%) were non-Hispanic white. Army was the service branch at the time of separation and comprised a greater than expected proportion of individuals in our study (55%). Sporadic ALS was observed in 81 patients (77%). The ALS-onset types, appendicular/bulbar/ respiratory were 55 (52.4%), 45 (42.9%), and 5 (4.8%), respectively. The mean (SD) admission ALSFRS-R and TFIM scores in this study were 31 (8) and 91 (25). Gastrostomy and NIV were used in 28 (27%) and 36 (34%) patients, respectively following initial evaluation. Greater gastrostomy use was found with bulbar-onset than limb/appendicular or respiratory-onset (bulbar vs. limb vs. respiratory onset = 56% vs. 8% vs. 40%, Fisher's Exact p-value < 0.0001) disease. NIV use was 53% vs. 32% vs. 60% in bulbar vs. limb vs. respiratory onset of the disease and did not reach significance among the three groups irrespective of their respiratory status (Fisher's exact p-value = 0.113).
Demographics of the study sample based on their first clinic visit.

ALS: amyotrophic lateral sclerosis; ALSFRS-R: amyotrophic lateral sclerosis functional rating scale-revised; BMI: body mass index; FVC: forced vital capacity; NIV: noninvasive ventilation; TFIM: total functional independence measure.
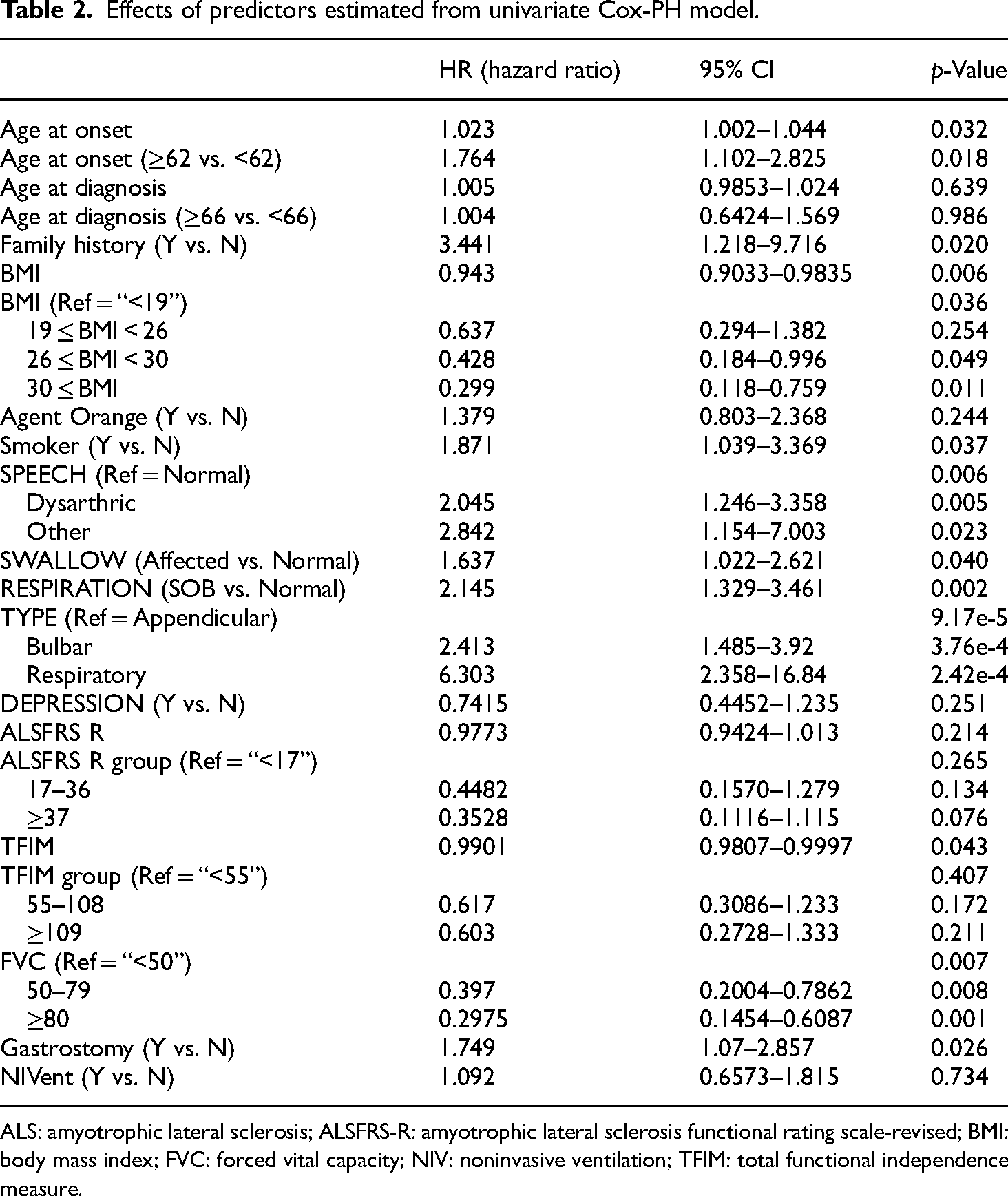
The univariate cox-PH model (Table 2) showed that familial ALS, current smokers, respiratory and bulbar-onset ALS-type with dysarthria, dysphagia, and shortness of breath, FVC less than 50%, and PEG placement was associated with decreased survival. However, obesity, FVC greater than 50%, and a higher TFIM score (90 and above) were associated with increased survival. Exposure to chemicals (solely Agent Orange) though increased the risk of dying but did not reach statistical significance. The multivariate Cox-PH model (Table 3) showed that familial ALS, respiratory and bulbar-onset ALS-type, and TFIM score were the main variables influencing survival. The multivariate Cox-PH model findings persisted even after adjusting for age at diagnosis (Table 4). The median survival from symptom onset was 4.12 (3) years. Shorter survivals were associated with the bulbar and respiratory-onset and familial ALS at initial diagnosis. The Kaplan–Meier survival plot shows the survival curves for the three types of ALS onset (Figure 1).

Kaplan–Meier survival plot.
Effects of predictors estimated from univariate Cox-PH model.
ALS: amyotrophic lateral sclerosis; ALSFRS-R: amyotrophic lateral sclerosis functional rating scale-revised; BMI: body mass index; FVC: forced vital capacity; NIV: noninvasive ventilation; TFIM: total functional independence measure.
Effects of predictors estimated from multivariate Cox-PH model.

TFIM: total functional
Effects of predictors estimated from multivariate Cox-PH model with age at diagnosis adjusted.
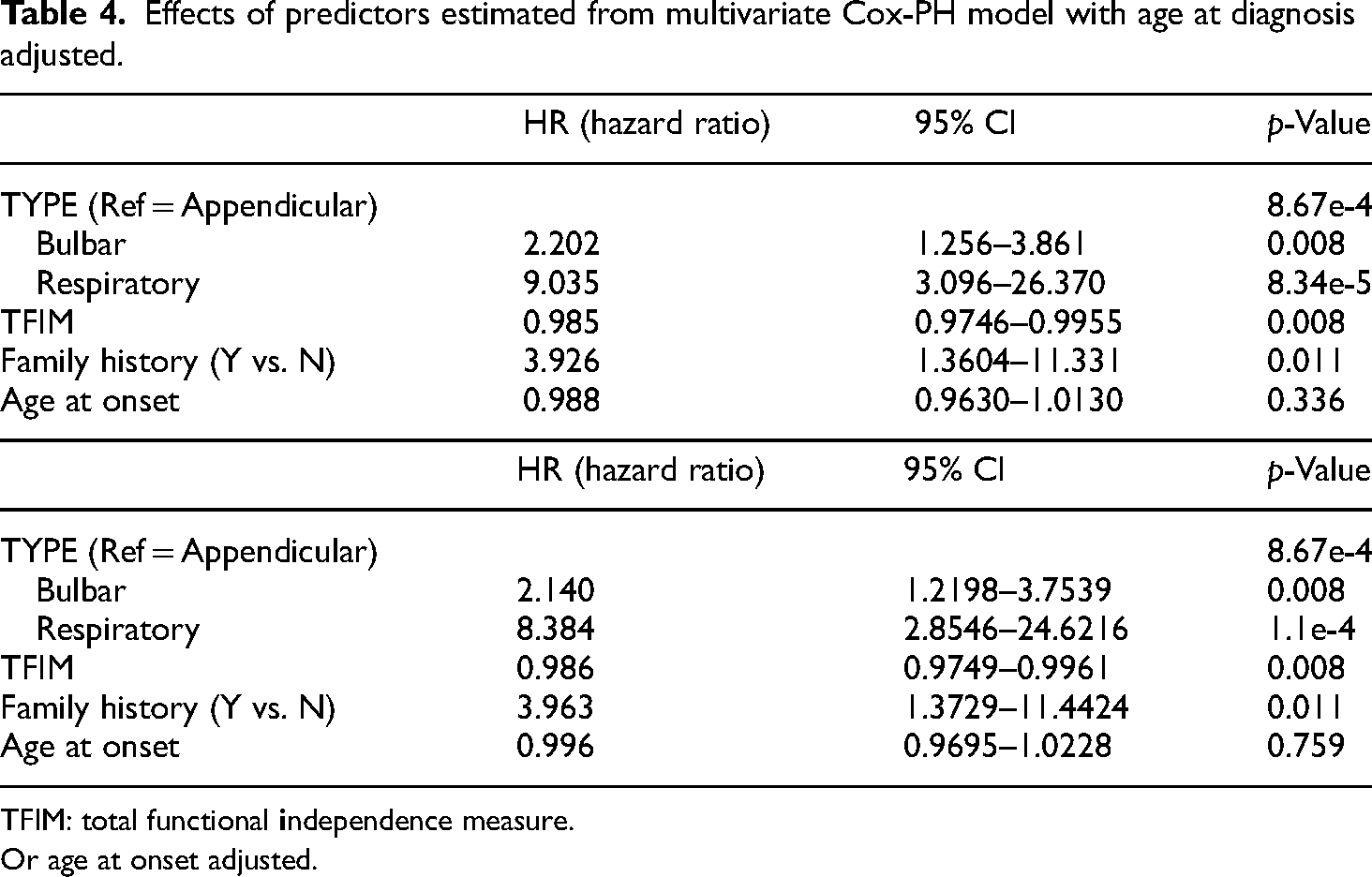
TFIM: total functional
Or age at onset adjusted.
In our study, confirmed cases of exposure to Agent Orange (dioxin) were present in 20% of cases and 5% of cases received multiple vaccinations. None of the veterans were exposed to pesticides. Their presence was not significantly associated with the type of ALS (Fisher's exact test p-value 0.099), cognition (MMSE, Wilcoxon rank sum test p-value 0.379) nor depression (Chi-squared test p-value 0.970). Likewise, there was no significant association with survival (Log-rank test p-value 0.236) or mortality (Fisher's exact test p-value 0.134).
Discussion
The main finding of this retrospective, observational study on the 11-year longitudinal data collected on veterans with ALS was as follows: (i) most were diagnosed in their 60 s, (ii) familial, (iii) bulbar, and (iv) respiratory-onset ALS had shorter survival. (iii) The median survival interval from symptom onset was 4 years, which is the same as that previously reported.12,42,43 However, longer survival was observed among the limb-onset (appendicular) disease at initial evaluation at 5.3 ± 5.2 years.
In the univariate analysis, the presence of gastrostomy was a poor prognostic factor but lost significance in the multivariate analysis. This could be because patients receiving gastrostomy were more likely to have the bulbar and respiratory-onset type of ALS, which have an elevated risk of death than appendicular ALS patients. Several observational studies have provided conflicting results about the effect of gastrostomy on survival in patients with ALS. This is due partly to the different definitions of control in prior studies, such as those who did not have a gastrostomy in all stages of the disease, and those in need of a gastrostomy, but declined the procedure.44,45
Gastrostomy in carefully selected patients as per recommendation in the current practice guidelines from the American Academy of Neurology is still beneficial. 40 In our study only 27.6% of veterans underwent PEG placement despite discussing the benefit of PEG usage on their initial evaluation. The main reason for this low uptake was that some veterans preferred to continue taking their nutrition by mouth as long as possible, some refused it outright as personal preference, and in some PEG, placement was considered a risk due to their poor respiratory state (FVC <50%) with the fear they would end up on continuous invasive ventilation based on the clinical judgment of the respiratory and gastrointestinal clinical providers on the ALS team. However, the percentage of PEG placement in our study mirrors the 23.5% PEG placement documented by Chio et al. in their study of 221 patients with ALS. 46
A survival benefit of greater than 12 months has been shown in previous literature reviews on NIV26,47; however, this was not the case in our cohort in univariate analysis. Only 34.3% of veterans underwent NIV usage despite discussing the benefit of NIV use on their initial evaluation irrespective of their respiratory status. The main reason for this poor compliance was that either they could not tolerate the various masks provided or was an inconvenience as they were unable to put on and take off the masks due to lack of arm-hand function or felt they were drowning in their saliva/drooling. Chio et al. in their study of 221 patients with ALS had 10.4% on NIV compared to the 34% NIV usage in our study. 46
Finally, McKay et al. 5 in their systemic review of 19 articles found that exposure to pesticides including Agent Orange, chemicals such as exhaust and burning agents, and contact with heavy metals, could increase the risk of ALS among military personnel. The veterans who had confirmed exposure to Agent Orange, it did not affect their survival and mortality in our study which could be due to the small number of confirmed documented cases of exposure.
The limitations of the present study are as follows. First, the small sample size of 105 patients, may bias the results as it reduces the power to detect an association. Second, we had a small cohort of confirmed cases of exposure to Agent Orange (dioxin) in 20% of cases and 5% of cases received multiple vaccinations. Analysis of their exposure did not affect variables shown to be associated with shorter survival.
Finally, though this study represents real-world data, the patients included were veterans who happen to be men and non-Hispanic white (96%); and all veterans with ALS receive highly quality subsidized medical care through the Veteran Health System; which may not be available to the general Oklahoma population, thus making the conclusions less generalizable to the general ALS patient population.
The strength of this study is the completeness of data collected by the standardized ALS registry over 11 years with no loss on periodic follow-up reflecting real-world clinical experience. Second, this study applies to the veteran population served, and the demographics of our study population mirror the recent publication by Reimer et al., where they analyzed the electronic health records of 19,662 veterans with ALS. They found the disease to be predominantly in men (99%), and white (72%), with a median age of disease onset of 68 years with the army being the branch of service with a greater than expected proportion of individuals on discharge from the service. 48 The information obtained is useful in planning future interventions to improve clinical care such as the provision of home delivery of essential medical equipment needed and home-based health aide support such as aid-and-attendance, the number of hours for caregiver support, and home-based primary care through all stages of ALS disease to help reduce caregiver burden. It also forms the basis for enrolling veterans in investigational drugs and assistive devices such as the trial of negative-pressure external ventilation being undertaken in veterans unable to tolerate NIV to determine their efficacy.
Conclusions
Veterans with ALS in this single-center study who had familial ALS, bulbar, and respiratory presentation at onset, had shorter survival. The presence of Agent Orange exposure, PEG placement, and NIV usage did not affect survival as there was underutilization of both interventions. Information based on this study (a) confirms the presence of familial ALS which is present in 10% of cases to be associated with shorter survival, (b) we continue to advise our veterans earlier in the course of their disease the benefit of having a PEG placement and NIV usage, and (c) developing a personalized treatment plan for that veteran. Finally, we are now looking at the underlying etiological factors of ALS to implement preventive strategies.
Supplemental Material
sj-doc-2-sci-10.1177_00368504241262902 - Supplemental material for Veterans with familial ALS and bulbar and respiratory presentations at onset had shorter survival
Supplemental material, sj-doc-2-sci-10.1177_00368504241262902 for Veterans with familial ALS and bulbar and respiratory presentations at onset had shorter survival by Meheroz H Rabadi, Kimberly A Russell and Chao Xu in Science Progress
Supplemental Material
sj-doc-3-sci-10.1177_00368504241262902 - Supplemental material for Veterans with familial ALS and bulbar and respiratory presentations at onset had shorter survival
Supplemental material, sj-doc-3-sci-10.1177_00368504241262902 for Veterans with familial ALS and bulbar and respiratory presentations at onset had shorter survival by Meheroz H Rabadi, Kimberly A Russell and Chao Xu in Science Progress
Footnotes
Abbreviations
Author contributions
Dr Meheroz H. Rabadi did study concept and design, data acquision, critical revision of the manuscript for intellectual content, and study supervision. Ms. Kimberly did just data acquisition.
Dr Chao Xu did analysis and interpretation and critical revision of the manuscript for intellectual content.
Data access statement
The data that support this study's findings are available upon request from the corresponding author [MHR]. This data is not publicly available owing to Veterans Health Authority restrictions, for example, as it contains patient-sensitive information that could compromise the privacy of the patient participants. If a request is made, approval needs to be obtained from the VA R&D and the Oklahoma University IRB.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical information
This study was approved by the Oklahoma University Institutional Review Board (IRB# 10358) after determining that the study was exempt from veteran's informed consent because of the retrospective review of electronic medical records, veterans were still being followed clinically, and most of the veterans had died.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Author biographies
Meheroz H Rabadi received his MD from Dow Medical College, Karachi University, Pakistan in 1982. He did post-graduate training in the United Kingdom and is a Member of the Royal College of Physicians, Ireland (MRCPI) in 1991. He is Board-Certified in Psychiatry and Neurology (ABPN) and Fellowship-trained and certified in Neurorehabilitation from Burke Rehab Hospital, Cornell University, NY. He is a Fellow of the American Academy of Neurology (FAAN) and the American Neurological Association (FANA). He is currently working in the Department of Neurology Oklahoma City VA Health Care System and is a Clinical Professor of Neurology at the University of Oklahoma. His research interests include Multiple Sclerosis, Spinal Cord Injury, ALS, and “Functional Motor Recovery Post-stroke” Measures, Interventions (nutritional, pharmacological, and devices), and predictors.
Kimberly A Russell completed her undergraduate studies (1990-1993) at Southwestern Oklahoma State University. She received her Bachelor of Science as a Physician Associate (1995) from the University of Oklahoma. She is currently working in the Department of Neurology Oklahoma City VA Health Care System. Her research interests include Multiple Sclerosis and ALS in Veterans.
Chao Xu received his BS, in Management Information Systems, from Jiangsu University of Science and Technology, in 2008, his MS in Systems Engineering, from the University of Shanghai for Science and Technology, in 2011, and his PhD degree in Biostatistics (2018) from the School of Public Health, Tulane University. He is currently working at the Department of Biostatistics and Epidemiology, Hudson College of Public Health, The University of Oklahoma Health Sciences. His research interests include biostatistics, bioinformatics, and genetic epidemiology.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.