
Abstract
This feasibility study evaluated the psychological status of patients with differentiated thyroid cancer (DTC) before, during, and 40 days after administration of I-131 radionuclide therapy (RAI). We investigated the appropriateness of providing patient a comprehensive psychological assessment in an isolation ward. Thirty consecutive patients (Study Group; SG) who received RAI were enrolled. The tools used were the Hospital Anxiety and Depression Scale (HADS) at three different moments, and the Coping Responses Inventory (CRI) at baseline for each patient. A supportive approach was also implemented. Data were collected at the first specialist visit, at the day of admission, and at 40 days follow-up visit. A matched cohort of patients (Control Group; CG), who did not receive psycho-oncological counseling, was retrospectively studied only about their medical needs and requests. Staff exposure to radiation was also compared during SG and CG hospitalization, to assess a possible reduction of radiological risk for them. A significant difference between the basal, intermediate, and final psychological status was observed (p < 0.0001), which was found to be irrespective of the induced hypothyroidism. Patients showed a significant worsening of their status in terms of anxiety and depression after the consent, but it improved 40 days after treatment. Repeated measures analysis showed a similar trend in patients’ psychological status over this period. At hospital discharge, patients showed indirect signs of increased well-being. CG required more nursing and medical interventions. Staff exposure was significantly lower during hospitalization of SG as compared to CG. This study demonstrates that timed psychological evaluation and appropriate support may help to reduce anxiety and depression of patients receiving a diagnosis of cancer and undergoing RAI. Moreover, an improvement of workplace safety was recorded.
Introduction
Management of patients with differentiated thyroid cancer (DTC) undergoing radionuclide therapy represents a challenge due to both historical misconceptions and recent legal limits.1–4 Patients candidate for admission to nuclear medicine isolation rooms may need timely psychological assessment and support before, during, and after hospitalization. Nevertheless, the most appropriate moment for psychological assistance has not been widely confirmed by standard operative procedures and remains uncertain in such setting. At present, psychological support is not routinely provided to these patients and their emotional needs are underestimated. I-131 radionuclide therapy (RAI) preparation requires several preliminary operations in charge of a multidisciplinary staff, but it does not still consider psychological support as essential at this stage.
5
Patients must undergo hypothyroidism by
Materials and methods
Patients
This study enrolled 30 consecutive patients (12 men and 18 women; mean age, 51 ± 18 years) from April to June 2022 at IRCCS CROB, Referral Cancer Center of Basilicata, Italy. All patients underwent RAI and were admitted to an isolation ward of nuclear medicine for a standard duration of three days after radiation. All of them received a psycho-oncology assessment and support, before, during, and after hospitalization. Inclusion criteria were age above 18 years; pregnancy test negative; total or near-total thyroidectomy 2 to 6 months before RAI; histology with papillary or follicular histotype, surgical stage ≥ pT1; induced hypothyroidism; scheduled hospitalization in an isolation ward. Patients were treated with an empirical radioiodine activity ranged from 3700 MBq to 4440 MBq, according to tumor histological type and staging. Metastatic disease, previous serious medical conditions, prior or current psychiatric illness, and habitual use of psychotropic substances were considered exclusion criteria. Patients with matching clinicopathological features (number = 30, female to male ratio, type of tumor, eligibility for iodine therapy) hospitalized in isolation constituted the CG and were retrospectively studied only concerning their medical needs and requests. The CG served to assess the frequency and type of daily demands of patients hospitalized in isolation as compared to that of the study group, retrieving patients’ data from medical records. They were evaluated considering the number, type, and timing (day/night) of complaints during the hospitalization, irrespective of their nature (e.g. from referred headache to the compulsory need for coffee). They not received psycho-oncological counseling.
Our institutional review board approved this study (protocol # 20210009766 / CEUR 35/2020). All patients who underwent RAI together with psycho-oncology assessment signed an informed consent form in accordance with the Declaration of Helsinki. They had the decisional capacity to provide written informed consent themselves.
Radioiodine treatment
Patients of the study group were separated into two groups based on the hypothyroidism induction approach: fifteen patients discontinued Levothyroxine replacement therapy, 1 month before hospitalization; the other group (#15), underwent exogenous TSH stimulation with recombinant human TSH (rhTSH). All patients had to follow a diet without iodine 2 weeks before RAI. Patients were admitted after testing negative for SARS-CoV-2. On the first day, patients received oral administration of a tailored activity of I-131 and after 3 days in isolation were discharged to home with a general behavioral guide according to current radiation safety rules. Levothyroxine therapy was gradually resumed for patients who discontinued the treatment.
Assessment of psychological status
All patients enrolled received two standard questionnaires: HADS to evaluate anxiety and depression, CRI for coping mechanisms. Self-assessment scale results of HADS were expressed for both anxiety and depression. This is a 14-questions survey designed to assess depression and anxiety in the setting of a hospital ward. The depression items tend to focus on the anhedonic symptoms of depression. The anxiety and depressive subscales are also suitable to measure the severity of the emotional disorder. Each question is rated from 0 to 3 on a 4-point severity scale. The HADS produces two scales, one for anxiety (HADS-A) and one for depression (HADS-D), differentiating the two states. Scores greater than or equal to 11 on either scale indicate a definitive case. CRI was used at baseline encompassing two main conceptual domains: cognitive approach strategies and cognitive avoidance strategies. Both domains included four items for each strategy: logical reasoning, positive reevaluation, behavioral approach strategies, problem solving, cognitive avoidance, acceptance or resignation, behavioral avoidance strategies, and emotional outbursts. On a patient basis, the number of normal, borderline, or pathological approaches was reported for each domain. They were also guided in completing the questionnaires. Moreover, patients joined unscheduled psychological interview according to their psychological status. The semi-structured psychological interview is a widely used data collection technique in psychology characterized by a combination of predetermined questions tracing the psychic and intrapsychic functioning of the patient. This approach allows flexibility to the researcher, which can ask tailored questions based on the participant's responses, hence adapting the support. The combination of defined and open-ended questions makes it possible to balance data standardization with the ability to explore inner experiences. The semi-structured interview is a valuable tool for research purposes. Generally, the questions were aimed at investigating self-coherence, reality examination, interpersonal relationships, and defense and rigidity.
Daily needs and demands of patients were routinely registered during the hospital permanence. Particularly, the psychological assessment was carried out at three different moments: the days (2–7) before hospitalization (Time 0), during pre-hospitalization procedures (as per pandemic-related issues and medical preliminary assessment); at the time of admission, for administration of radioactive iodine (Time 1), and 1 month after discharge (Time 2). The visits were replicable, although performed with a different methodology in reason of radioprotection control. At first approach, patients underwent a direct assessment whereas phone interviews were performed afterward. Questionnaires at Time 1 were completed by patients but, the psychological support was warranted by a phone interview to avoid prolonged and close contact with radioactive patients. At the follow-up assessment (Time 2) patients went through phone interview and counseling, and the questionnaires were completed by the psycho-oncologist.
Workplace safety assessment
All nurses involved in the radiometabolic ward (eight on the roster) were monitored for the radiation dose during the trial. The mean dose rates were measured by thermoluminescent dosimeters (TLDs) used to record the radiation dose (gray/Gy) accumulated by the staff. TLDs do not yield immediate information about radiation exposure and were monthly checked retrospectively. The data of the same professionals were compared with those registered during hospitalization of the CG.
Statistical analysis
Continuous data were expressed as percentages, median, and mean ± SD as appropriate. Comparison between the mean values was performed with paired Student's t-test (two-tailed probability), when necessary. One-way analysis of variance (one-way ANOVA test) with Sheffè's method (post-hoc test in ANOVA) was used to test the difference between the means of subgroups of variables. To compare data under different conditions, we used the repeated measures analysis of variances (within-subjects effect). Our hypotheses were tested using Bonferroni-adjusted alpha levels. The Greenhouse–Geisser and Huynh–Feldt corrections16,17 attempt to estimate epsilon (sphericity). Sphericity refers to the similarity of variances of differences between measurements. With this method, an epsilon of 1 indicates that the condition of sphericity is exactly met. As epsilon decreases below one, the greater is the violation of sphericity. Moreover, the Friedman test was performed to assess the difference between several related measures. Correlation analysis (correlation coefficient r) was used to determine whether the values of variables were associated, when requested. A p value <0.05 was considered statistically significant.
Results
Overall patients’ characteristics are shown in Table 1. In the study group, the patients who underwent rhTSH stimulation presented higher TSH values at the zenith, as normally encountered in daily routine. The mean HADS over time and baseline CRI results for each domain are presented in Table 2, while overall HADS box-and-whisker plots are reported in Figure 1. Figure 2 shows scores obtained on an individual basis. Diagrams with HADS scores concerning patients who withdrew Levothyroxine and those who received rhTSH are shown in Figure 3. Differences between scores at each time point were statistically significant (p < 0.0001; Table 3). Data were reported for both anxiety and depression, with increasing values from Time 0 to Time 1, reaching minimum levels 1 month later. No statistically significant difference over time was observed between the group of patients who withdrew Levothyroxine and those who did not.

Box-and-whisker plots of HADS scores concerning anxiety (A) and depression (B), before (1), during (2), and after (3) hospitalization.

Dot and line HADS diagram on individual basis concerning anxiety (A) and depression (B) before, during and after hospitalization.

Diagrams of HADS scores for anxiety (A, C) and depression (B, D) in patients who withdrew Levothyroxine (LW) and those who received recombinant thyrotropin (rhTSH), before (b), during (d) and after (a) hospitalization.
Overall individual data of DTC patients.

DTC, differentiated thyroid cancer; *, hurtle, tall cell, columnar, sclerosing; TNM, tumor, node, metastasis stage; TSH, thyroid-stimulating hormone; rhTSH, recombinant human thyrotropin; HTg, human serum thyroglobulin.
Mean values of Hospital Anxiety and Depression Scales at different time points and Coping Responses Inventory at baseline.

HDSA, Hospital Anxiety and Depression Scale; b, before hospitalization; d, during hospitalization; a, after hospitalization; CRI, Coping Responses Inventory.
Pairwise comparisons of HADS values before, during and after hospitalization for both anxiety and depression.
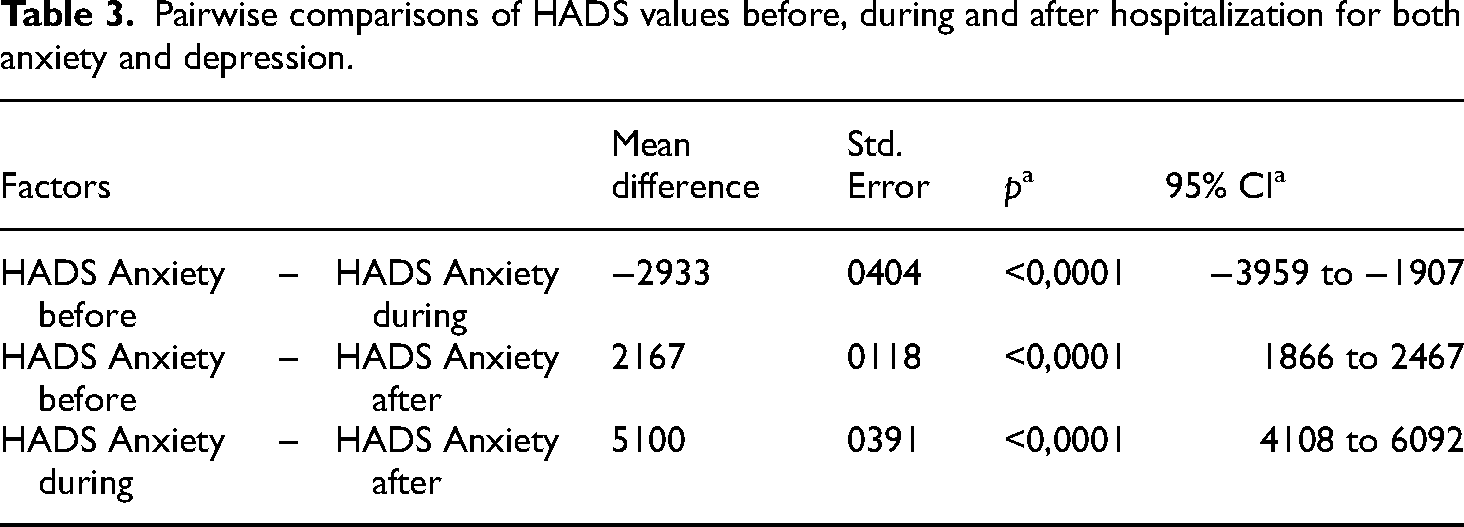

Bonferroni corrected; HDSA, Hospital Anxiety and Depression Scale.
Concerning the approach coping mechanism 35.8% of responses were normal, 37.5% borderline, and 26.7% pathological, whereas 41.7% of avoidance coping mechanisms were normal, 41.7% borderline, and 16.6% pathological. At last, approximately 61% (58–64%) of items showed a non-adaptive type of response to stress. At correlation analysis no significant relationship was found between patients’ age and both HADS and CRI scores throughout the time (r range: 0.003–0.5; all p: ns).
Moreover, from the analysis of medical records, the matched CG of patients not subjected to psycho-oncology support required more nursing and medical interventions. On a patient basis, overall needs during hospitalization were 4 in the SG and 23 in the CG (p < 0.0001). Two patients referred transient headache in SG and 12 in CG (p < 0.05). One patient required intervention for stomach spasms in SG and 10 in the CG (p < 0.01). All complaints registered in medical records were likely linked to anxiety and stress because of their rapid reversibility. One patient in each groups experienced a transient swollen tender neck (radioiodine-related).
The monthly mean absorbed dose rates for the 8 staff unit exposed to radioactive patients were 0.7 ± 0.2 mSv versus 1.2 ± 0.5mSv, the latter referring to consolidated historical data recorded during CG hospitalization (p < 0.001).
Discussion
There are several issues arising during management of patients undergoing radionuclide therapy and that have to be hospitalized in an isolated, controlled ward.
18
The psychological status of subjects represents a critical concern. In fact, they are generally hypothyroid, they are conscious of having had cancer, become aware of being isolated and receiving radioactive drugs. It is also important to consider the public misconception surrounding this therapy due to recent accidents and environmental radioactive events.
19
As stated above, most patients belonging to this setting exhibit a mishmash of distress conditions. It is well known that patients referred to a nuclear medicine ward for therapy have several anxiety-predisposition factors (e.g. hypothyroidism, cancer-related apprehension, isolation admission distress).
20
Our study was designed to establish whether a sequential psycho-oncological approach before, during, and after admission of patients undergoing RAI can be implemented and if this setting could benefit from a sustained comprehensive timely support. A better radioactive patient management was also expected. The results showed that the patient's distress (anxiety and depression) was mitigated during pre-hospitalization days, it worsened at the time of radioactive drug administration and significantly decreased 1 month later. This finding, although not completely new
14
was obtained for the first time in all patients’ categories undergoing RAI, those presenting endogen hypothyroidism, and patients subjected to preparation with rhTSH administration. There were no differences between the two groups. It can be doubted that the pre-hospitalization days are near to admission and consequently the psychological status of patients is sensibly similar. However, during the preparation procedures, apart from psychological support, patients were enrolled into a familiar environment with the support of staff; the nuclear medicine doctor is committed to explaining to them the benefits, adverse reactions, and complications of the treatment. In patients with DTC ablation success or diagnostic uptake requires high TSH stimulation to reach target levels. Unfortunately, this condition is accompanied by symptoms such as fatigue, weight gain, constipation, cold intolerance, coarse skin and hair, hair loss, decreased memory, muscle aches, weakness, and depression. It encompasses a psychological status that should be recognized and that is usually worsened in a context of general misapprehension. Patients undergoing RAI are conscious of their cancer, even after surgery, and they are worried about radiometabolic therapy and isolation. This distressed scenario needs the development of the best attainable supportive care system involving professionals such as nurses, nuclear medicine doctors, technical staff, and psycho-oncologists. Nevertheless, Banihashem et al.
14
found that in a cohort of patients with previous DTC undergoing
In our study patients were evaluated for their distress but they also received unplanned psychological support. Anxiety and depression were significant at the first visit, reaching the highest level at the day of treatment. These data support the hypothesis that a timely and real help could be provided on the day of radionuclide administration, or that maximum care engagement is required at that moment. It is reasonable that the first psychological approach (the days before hospitalization) was partially inefficient or insufficient considering the worsening of patients’ moods. However, after the drug administration, we detected initial signals of improvement, thereafter, confirmed at the 1-month evaluation. Patients who attended the first two psychological visits were less demanding for the following 2 days after admission compared to those of CG. It can be speculated that once received the radioactive therapy they can become relaxed, though the beneficial effect of psychological support cannot be excluded. Our patients were helped with both interview at admission and targeted psychological intervention. In fact, the interview was used as a way to support them through this experience of awareness of illness as well as to compensate for their distress, according to other authors.22–25 Like others, we detected significant psychological stress that justified the support interventions.26–28 In the context of the abovementioned misapprehension, anxiety, and depression, patients frequently will ask for staff support. Unfortunately, this occurrence can increase the exposure to radiation of the professional staff. In addition, within the environment of the radiometabolic ward, it is mandatory to respect the dose limits that various groups may receive, including staff and the public. Iodine-131 results in the largest dose to medical staff, caregivers, and relatives.
29
Providing patients at hospitalization with psycho-oncological support would improve management also in terms of workplace safety, avoiding and reducing unnecessary exposure. Patients who received the psycho-oncologist aid required less, and often banal, staff support. The feasibility of this approach justified the need and the timing of the psycho-oncological support provided to our patients. It seemed that psychological support on the day of admission is not an important benefit, for this reason the procedure might be started on the subsequent day. This model could be easily implemented in daily practice. Even though hypothyroidism seems to be a dominant factor in this contest, our study demonstrated that patients with
It appears that isolated patients could be managed easily in terms of both professionals’ safety and patients’ control. There is evidence for implementing a comprehensive approach to patients, including psycho-oncology assessment. From an organizational point of view, our data sustain the hypothesis of improving multidisciplinary patient management hospitalized in isolation rooms because of their radioactivity. 33 Repeated measures analysis confirmed the mutability of psychological status over time, hopefully finding the optimal moment to implement supportive care.
Clinical implications
This study demonstrates that timely and appropriate psychological evaluation and tailored support on specific needs may be valuable for patients undergoing radionuclide therapy with I-131 for thyroid cancer.
Study limitations
The results of our work should be interpreted in the view of certain limitations. First, this study included patients that strictly fulfilled inclusion criteria but was a monocentric study with a relatively small cohort. Moreover, the wide age range of patients was found not correlated with the psychological reaction, and the impact of all other intrinsic variables, if any, has not been figured out.
Conclusion
This study shows that the implementation of a psycho-oncological evaluation and support of patients hospitalized for radionuclide therapy in an isolation ward is feasible within the logistic limits. It could be useful to spend more time on patients’ needs to reassure them, this will also reflect on workplace management optimization.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504241253715 - Supplemental material for Assessment of psychological status by a comprehensive approach in thyroid cancer patients undergoing radionuclide therapy: A feasibility study
Supplemental material, sj-pdf-1-sci-10.1177_00368504241253715 for Assessment of psychological status by a comprehensive approach in thyroid cancer patients undergoing radionuclide therapy: A feasibility study by Alessia Giordano, Ilaria Bochicchio, Rosj Gallicchio, Giovanni Deiana, Rebecca Storto, Anna Nardelli, Michele Di Cosola, Alessandro Lettini and Giovanni Storto in Science Progress
Footnotes
Acknowledgments
The authors wish to thank Mrs. Piccolella A. and Mr Volpicelli F. for their valuable contribution to perform the study.
Authors’ contributions
All authors made a significant contribution to this work. A.G., I.B., and G.S. contributed to the design and implementation of the research, to analysis of results, and writing the manuscript. I.B. and G.D. developed the theoretical framework, performed the interviews, and provided psychological support to patients. R.G., R.S., and A.N. aided to data interpretation and drafted the manuscript. M. DC. and A.L. interpreted results and supervised the findings of this work.
Data availability
All data reported in the manuscript are stored in digital form by the corresponding author and are available upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institutional review board approved the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the this research received funding from the MoH 2024 current research program.
Patient consent statement
All patients undergoing RAI and psychological assessment study signed an informed consent in accordance with the Declaration of Helsinki. All the patients had the decisional capacity to provide written informed consent themselves.
Supplemental material
Supplemental material for this article is available online.
Author biographies
Alessia Giordano is a nuclear medicine physician involved in metabolic radiotherapy and patients care.
Ilaria Bochicchio is a psychologist who is particularly committed to psycho-oncology, she has a longtime experience in the field.
Rosj Gallicchio is a nuclear medicine physician involved in metabolic radiotherapy and in PET/CT related diagnostics.
Giovanni Deiana is a psychologist who is particularly committed to psycho-oncology, he has a longtime experience in the field.
Rebecca Storto is a medicine and surgery student. She is involved in research and in data and paper revision.
Anna Nardelli is an experienced radiopharmacist who takes care of radiopharmaceuticals and quality controls.
Michele Di Cosola is a head and neck surgeon involved in post-radiotherapy issues and undue effects and takes care of head and neck tumors.
Alessandro Lettini is the chief of psycho-oncology service and coordinates a group of psycho-oncologist with a multidisciplinary approach.
Giovanni Storto is the director of Nuclear Medicine Dept. at IRCCS CROB referral cancer center of Basilicata, Italy. He is the director of the Services Department as well which includes Diagnostic Imaging, Laboratory, Pathology, and Radiation Oncology Depts. He was Chief resident at CHUV Lausanne University Hospital and He worked at IAEA Wien in the nuclear medicine section. He has held roles in several universities as professor.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.