
Abstract
Objectives
To present a case report of sinonasal glomangiopericytoma (GPC) in a female patient in her thirties and to highlight the importance of collecting pathology specimens even in routine sinus surgery cases.
Methods
A case report detailing the diagnosis of GPC in a female in her thirties, including her initial presentation, treatment, and follow-up, along with a brief review of the literature.
Results
Pathology of the collected specimen revealed sinonasal GPC along with chronic rhinosinusitis. Immunohistochemistry was positive for SMA, beta-catenin, and cyclin D1; and negative for STAT6, ERG, pankeratin, SOX10, and S100.
Conclusion
This diagnosis expands the knowledge around the demographic profile of GPC patients. GPC should be included in the differential diagnosis of sinonasal masses, even in younger patients. The case highlights the importance of collecting the entire pathology specimen in all cases, even of ones that seem routine and benign.
Introduction
Sinonasal glomangiopericytoma (GPC) is an extremely rare type of neoplasm which is defined as a sinonasal mesenchymal neoplasm demonstrating a perivascular myoid phenotype. 1 Notably, even though rarely, GPC has also been related to oncogenic osteomalacia.2,3 GPC tumors have low malignant potential and are reported to represent less than 0.5% of sinonasal neoplasms.4–9 The definition of the disease has a complex history since the first report in 1942 describing this as hemangiopericytoma. 10 While initially thought to be within the spectrum of vascular tumors ranging from capillary hemangioma to glomus tumors, GPC has been classified as a distinct entity by the World Health Organization since 2005.1,6,7,11,12 Based on early reports in the literature, cases were described as typically in older patients in their sixtieth and seventieth decades of life and commonly presented with nasal obstruction and/or epistaxis.4,5,11 The standard treatment course is complete surgical excision, with the risk of recurrence described as low (16–17%).13,14 Our report here of a case in a 37-year-old female with no significant history of epistaxis, expands the available information on such rare sinonasal neoplasms and highlights the importance of collecting the entire pathology specimen in all cases, even of ones that seem routine and benign.
Case
Patient presentation and treatment
A 37-year-old adult female patient presented with a five-year history of intermittent bilateral nasal obstruction and facial pain and pressure. She denied a history of anosmia and epistaxis. She had a past medical history significant for type II diabetes mellitus and hypertension. She had no prior nasal surgeries or history of nasal trauma. The patient had a deviated septum on clinical exam. Flexible nasopharyngolaryngoscopy demonstrated deviated septum, diffuse edema, and a large nasal polyp in the left nasal cavity extending from the medial surface of the middle turbinate and obstructing the left middle meatus. CT findings showed evidence of polypoid appearance of mucosa partially obstructing the left nasal airway, mild scattered areas of mucosal thickening and secretions, and no obstruction of drainage pathways (see Figure 1). The imaging findings were reviewed in the clinic with the patient. Her symptoms were refractory to maximal medical therapy of steroid sprays and sinus rinses. She therefore elected to proceed with surgery which included left endoscopic maxillary antrostomy, anterior and partial posterior ethmoidectomy with imaging guidance, septoplasty, and bilateral inferior turbinate reduction and lateralization.

CT findings showed evidence of polypoid appearance of mucosa partially obstructing the left nasal airway, mild scattered areas of mucosal thickening and secretions, and no obstruction of drainage pathways.
During her surgery, the middle turbinate was partially resected given its polypoid changes. The large solitary left-sided polyp was removed using a microdebrider. All specimen including the collection from the microdebrider was sent for pathologic examination. A Lukens Trap with a tailored sock collector was used for specimen collection to ensure all tissue that was microdebrided and suctioned was collected in the Lukens Trap and was sent for pathologic analysis. There was no evidence of features suggestive of malignancy and the remainder of the procedure was carried out without complication.
Diagnosis
Left nasal and sinus contents were collected and sent for pathology. The final pathology diagnoses were sinonasal GPC and chronic rhinosinusitis. Immunohistochemical (IHC) staining was performed and was shown to be positive for SMA, beta-catenin (nuclear), and cyclin D1, and yet negative for STAT6, ERG, pankeratin (AE1/AE3 + CAM5.2 + MNF116), SOX10, and S100, consistent with GPC (see Figure 2). Histologic features suggestive of aggressive behavior, such as profound nuclear pleomorphism, increased mitotic activity, or tumor necrosis, were not identified.
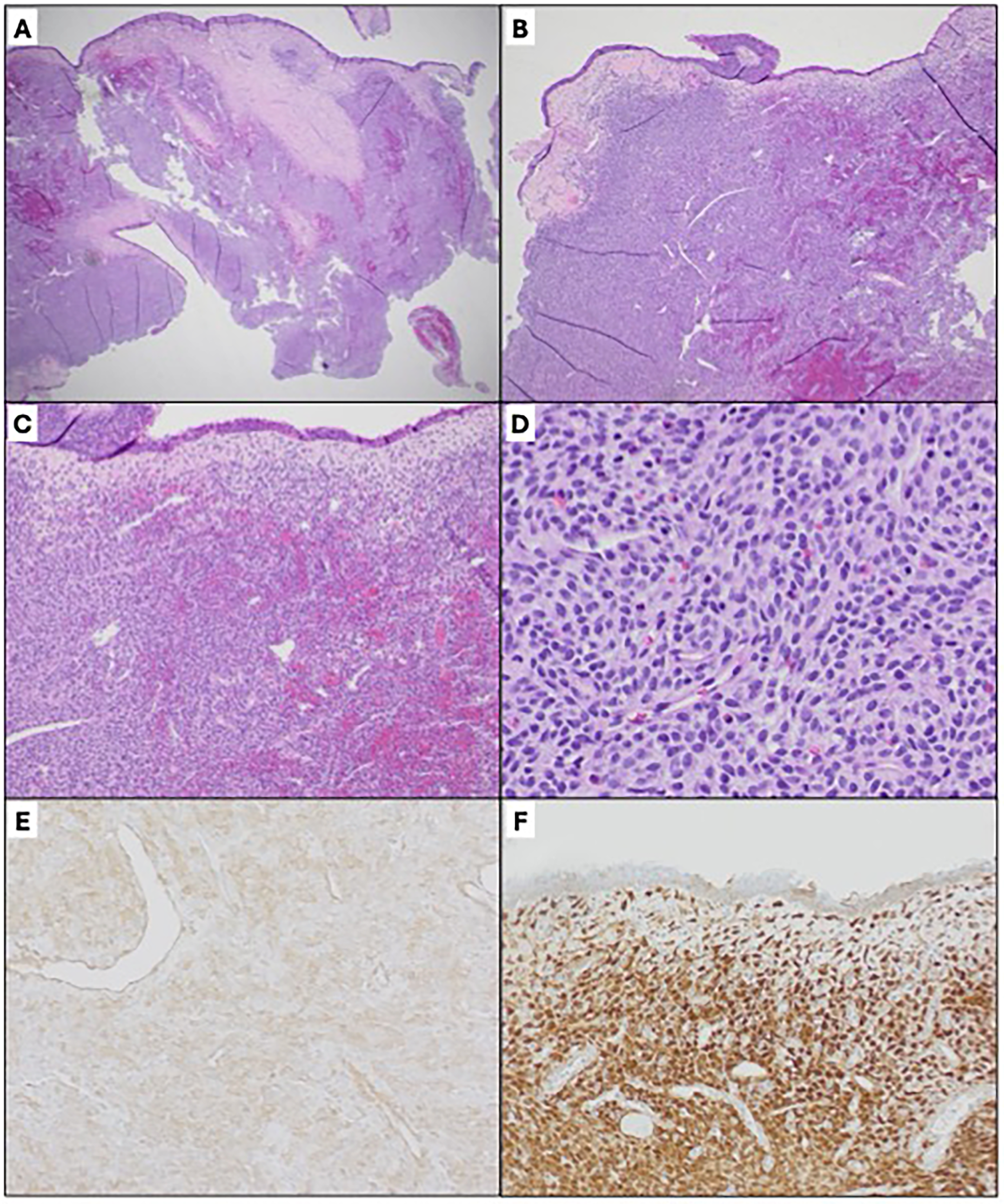
Histologic sections demonstrate a polypoid lesion with intact surface epithelium and subepithelial diffuse proliferation of tumor cells (2A). Within the tumor are frequent branching vessels (2B) with perivascular hyalinization (2C). The tumor exhibits a syncytial arrangement of bland spindle cells, intermixed eosinophils, and mast cells are noted in the background (2D). Features suggestive of aggressive behavior, such as profound nuclear pleomorphism, increased mitotic activity, or tumor necrosis, are not identified. Immunohistochemical staining shows the tumor is positive for SMA (2E), beta catenin (nuclear staining, 2F), and cyclin D1 while negative for STAT6, ERG, pankeratin (AE1/AE3 + CAM5.2 + MNF116), SOX10, and S100, immunoprofile consistent with glomangiopericytoma.
Follow up
The pathological findings were discussed with the patient in the clinic after the surgery and she was scheduled for six-month follow-up in the clinic to assess for recurrence.
Discussion
Importance of collecting pathology specimen
Collection and IHC analysis of pathologic specimens are essential for the diagnosis of GPC. Common patient symptoms such as unilateral nasal obstruction and/or epistaxis, and tissue mass features evident on imaging by CT, MRI, or endoscopy do not necessarily lead a provider to consider GPC on the differential due to its rarity. We commonly use a Lukens Trap and a tailored sock collector for sinonasal cases for specimen collection. This case serves as a great reminder to always collect specimens even for routine cases to ensure an important pathologic diagnosis is not missed. Further, this case serves as a helpful reminder to consider neoplastic diagnoses when one encounters a solitary nasal polyp without additional polypoid changes. IHC testing results were consistent with the literature as definitive for GPC, with positive results for SMA, beta-catenin (nuclear), cyclin D1, and negative results for STAT6, ERG, pankeratin (AE1/AE3 + CAM5.2 + MNF116), SOX10, and S100. GPC diagnostic reliance on SMA positivity or CD34 negativity (not tested here) can be misleading as some cases have been shown to be SMA negative, 5 or CD34 positive.15,16 These findings indicate that a panel of IHC tests is needed, as no single marker has been found to be sufficient for definitive GPC diagnosis.4,5,15–17
Patient demographics and medical history
The literature describes GPC cases as being mainly in patients in their sixtieth and seventieth decades of life, with a slight female to male bias,5,11 however the rarity of GPC and a limited number of case descriptions makes it difficult to generalize regarding patient demographics. Indeed, two recent GPC case series comprising of 16 cases found a male-to-female ratio of 1:1,15,17 and another series of 6 cases, a male-to-female ratio of 5:1. 4 Recent GPC reports are consistent with most patients being in their 50s–70s, although the age range can be from 21 to 81 years old.18,19 Collectively, these findings together with our report here of a 37-year-old female patient suggest that GPC should be considered in all patients regardless of sex or age.
The etiology of GPC remains obscure, although increased vascularity associated with hypertension, pregnancy, previous trauma, or corticosteroid use has been mentioned in the literature.4,5,9,11 Interestingly, for the six GPC cases recently described by Schauwecker et al., five of the patients had hypertension and/or type 2 diabetes mellitus which can be associated with increased vascularity. 4 Our patient also reported a past medical history of hypertension and type 2 diabetes mellitus, in alignment with these previous case findings of comorbidities associated with increased vascularity. However, further research is needed to elucidate the etiology of GPC.
Conclusion
Although there are few detailed reports of GPC and these tumors remain rare, they should be included in the differential diagnosis of sinonasal masses. The initial presentation (unilateral nasal obstruction and/or epistaxis) and evidence of a mass on imaging by CT, MRI, or endoscopy of GPC patients can lead to a lack of differentiation from other more common sinonasal diagnoses, such as nasal polyps. Our case highlights the importance of the following: it is imperative to always collect pathology specimens regardless of the preoperative level of concern and neoplasms such as GPC can occur in young patients without risk factors and a compelling history. Further research is needed to clarify the exact pathogenesis of GPC as well as its natural history to better improve the management of this rare disease entity.
Footnotes
Acknowledgements
We thank the patient and staff involved in this case.
Author contributions
AN, BB, and SG all contributed to data gathering involved in drafting the manuscript; AN drafted the initial manuscript; and BB and SG provided input and review of the manuscript. All three authors approve of the final manuscript.
Consent
The authors obtained written informed consent from the patient for the publication of the case information and any images.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethics approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Ariadne A. Nichol is a third-year medical student at University of California, San Diego School of Medicine.
Benjamin J. Bernard, MD, is a PGY-3 in the Department of Otolaryngology at the University of California, San Diego School of Medicine.
Sapideh Gilani, MD, is a board-certified otolaryngologist who specializes in treating disorders of the nose and sinuses, as well as facial plastic and reconstructive surgery. She is also an associate professor in the Department of Otolaryngology at the University of California, San Diego School of Medicine.