
Abstract
Background:
Ischemia–reperfusion injury (IRI) poses a significant challenge for physicians, necessitating the management of cell damage and the preservation of organ functions. Various surgical procedures, such as vascular surgery on extremities, temporary cross-clamping of the abdominal aorta in aortic surgery, and the use of a tourniquet in extremity surgeries, may induce lower limb IRI. The susceptibility to IRI is heightened in individuals with diabetes. This study aimed to investigate the effects of fullerenol C60 and sevoflurane on mouse muscle tissue in a lower limb IRI model and to assess their potential in preventing complications arising from ischemia–reperfusion in mice with streptozocin-induced diabetes.
Methods:
A total of 36 adult Swiss albino mice were randomly divided into six groups, each consisting of six mice: control group (group C), diabetes group (group D), diabetes–ischemia/reperfusion group (group DIR), diabetes–ischemia/reperfusion–fullerenol C60 group (group DIR-FC60), diabetes–ischemia/reperfusion–sevoflurane group (group DIR-S), and diabetes–ischemia/reperfusion–sevoflurane–fullerenol C60 group (DIR-S-FC60). Streptozocin (55 mg/kg) was intraperitoneally administered to induce diabetes in the relevant groups, with mice displaying blood glucose levels of 250 mg/dL or higher at 72 h were considered diabetic. After 4 weeks, all groups underwent laparotomy under anesthesia. In DIR-FC60 and DIR-S-FC60 groups, fullerenol C60 (100 mg/kg) was intraperitoneally administrated 30 min before the ischemia period. Sevoflurane, delivered in 100% oxygen at a rate of 2.3% and 4 L/min, was administered during the ischemia period in DIR-S and DIR-S-FC60 groups. In the IR groups, a microvascular clamp was placed on the infrarenal abdominal aorta for 120 min during the ischemia period, followed by the removal of the clamp and a 120-min reperfusion period. At the end of the reperfusion, gastrocnemius muscle tissues were removed for histopathological and biochemical parameter examinations.
Results:
Histopathological examination revealed a significant reduction in the disorganization and degeneration of muscle cells in the DIR-S-FC60 group compared to the DIR group (p = 0.041). Inflammatory cell infiltration was notably lower in the DIR-S, DIR-FC60, and DIR-S-FC60 groups than in the DIR group (p = 0.031, p = 0.011, and p = 0.013, respectively). The total damage scores in the DIR-FC60 and DIR-S-FC60 groups were significantly lower than in the DIR group (p = 0.018 and p = 0.008, respectively). Furthermore, the levels of malondialdehyde (MDA) in the DIR-S, DIR-FC60, and DIR-S-FC60 groups were significantly lower than in the DIR group (p < 0.001, p < 0.001, and p < 0.001, respectively). Catalase (CAT) enzyme activity in the DIR-S, DIR-FC60, and DIR-S-FC60 groups was higher than in the DIR group (p = 0.001, p = 0.014, and p < 0.001, respectively). Superoxide dismutase (SOD) enzyme activity in the DIR-FC60 and DIR-S-FC60 groups was also higher than in the DIR group (p < 0.001 and p = 0.001, respectively).
Conclusion:
Our findings indicate that administering fullerenol C60 30 min prior to ischemia in diabetic mice, in combination with sevoflurane, led to a reduction in oxidative stress and the correction of IR-related damage in muscle tissue histopathology. We believe that the administration of fullerenol C60 before IR, coupled with sevoflurane administration during IR, exerts a protective effect in mice.
Introduction
Injury, certain medical conditions (e.g. embolism, thrombosis), and various surgical procedures (e.g. vascular surgery on extremities, temporary cross-clamping of the abdominal aorta in aortic surgery, and the use of a tourniquet in extremity surgery) can lead to lower limb ischemia–reperfusion injury (IRI). This situation poses a critical challenge for physicians, necessitating the management of cell damage and the preservation of organ functions.
Contemporary knowledge acknowledges that restoring blood flow to ischemic tissue, referred to as reperfusion, can induce re-injury in the previously ischemic tissue, a phenomenon known as IRI. 1 The underlying mechanisms of IRI are intricate, with key factors including a metabolic shift toward anaerobic metabolism, an imbalance of Ca2+ homeostasis, mitochondrial dysfunction, increased oxidative stress, and an immune response. 2
Diabetes mellitus (DM), characterized by a metabolic disorder in blood sugar regulation, has emerged as a common chronic disease of our time. The World Health Organization (WHO) estimates that the global number of individuals with DM will reach approximately 360 million by the year 2025. 3 Research indicates that irregularities in endoplasmic reticulum homeostasis 4 and mitochondrial dysfunction 5 contribute to the development of DM. Consequently, the impact of IRI in individuals with DM is even greater.
Fullerenes, distinguished by their unique lattice structure of carbon nanomaterials, hold promise in various fields such as anticancer or antimicrobial therapy, cell protection, enzyme inhibition, controlled drug delivery, and contrast-based or radioactivity-based diagnostic imaging. 6 The carbon cage inherent in fullerenes, which contains a highly conjugated π-electron system, gives them the ability to accept electrons, enabling them to have antiradical activities and catalytic roles in biochemical reactions. 7 Fullerenols, being amphiphilic, exhibit water solubility due to hydroxyl groups, and fragments of the fullerene skeleton enhance their affinity for the lipid structures of cell membranes. 8 Studies have shown that fullerenes have protective effects against IR damage in the brain, kidney, and skeletal muscle due to their strong antioxidant capacity.6,8–11
Sevoflurane, an inhaled anesthetic widely used in surgeries, is favored for its low blood solubility, rapid induction and awakening, and ease of depth control during anesthesia maintenance. 12 It is noted that sevoflurane exhibits organ-protective properties by mitigating stress-induced damage, primarily through its anti-oxidative and anti-inflammatory effects. 13 The protective effect of sevoflurane extends to various organs, including the liver, lung, brain, and kidney, operating through multiple pathways.14–17
This study aimed to investigate the potential protective effects of fullerenol C60 and sevoflurane on muscle tissue in a lower limb IRI model in mice with streptozocin-induced diabetes.
Materials and methods
Animals and experimental protocol
This experimental study was conducted at the Gazi University Animal Experiments Laboratory in accordance with the ARRIVE guidelines between August 2022 and September 2022. Approval for the study was obtained from the Experimental Animals Ethics Committee of Gazi University (G.Ü.ET-22.064), and all procedures adhered to the accepted standards outlined in the Guide for the Care and Use of Laboratory Animals.
Thirty-six Swiss albino mice weighing between 20 and 25 g were used in the study. The mice were housed at a temperature of 20–21°C with 12-h cycles of daylight and darkness and had free access to food until 2 h before the anesthetic procedure. The animals were randomly divided into six groups, each containing six mice: control group (group C), diabetes group (group D), diabetes–ischemia/reperfusion group (group DIR), diabetes–ischemia/reperfusion–fullerenol C60 group (group DIR-FC60), diabetes–ischemia/reperfusion–sevoflurane group (group DIR-S), and diabetes–ischemia/reperfusion–fullerenol C60–sevoflurane group (group DIR-S-FC60).
Diabetes was induced by a single injection of streptozocin (Sigma Chemical, St Louis, MO, USA) at a dose of 55 mg/kg (i.p.) body weight. Blood glucose levels were measured 72 h after the injection. Mice were classified as diabetic if their fasting blood glucose (FBG) levels exceeded 250 mg/dL, and only animals with FBGs of >250 mg/dL were included in the diabetic groups (groups D, DIR, DIR-FC60, DIR-S, and DIR-S-FC60). The mice were kept alive for 4 weeks after streptozocin injection to allow the development of chronic diabetes before they were exposed to IR. Before the experiment, all mice were anesthetized with 50 mg/kg intramuscular ketamine (Ketalar®; 1 mL = 50 mg; Pfizer, Istanbul, Turkey) and 10 mg/kg xylazine hydrochloride (Alfazyne® 2%, Ege Vet, Turkey).
To prevent hypovolemia, an isotonic saline solution was administered hourly (3 mL/kg, i.p.). The abdomen was covered with a moist sterile pad during the reperfusion period. At the end of the experiments, gastrocnemius tissue samples were collected for biochemical and histopathological analyses. Following the end of the reperfusion period, all mice were anesthetized using ketamine (50 mg/kg) and sacrificed by collecting blood from their abdominal aortas. After the heartbeat and respiration ceased, the mice were monitored for a further 2 min to confirm death.
Biochemical analysis
The gastrocnemius muscle tissue was first washed with cold deionized water to eliminate blood contamination and then homogenized in a homogenizer.
To measure cell contents, tissues need preliminary preparation, often involving grinding the tissue in a ground-glass tissue blender using a rotor driven by a simple electric motor. The homogenizer is a tissue blender similar to a typical kitchen blender, which is used to emulsify and pulverize the tissue (Heidolph Instruments GMBH & CO KGDiax 900, Germany) at 1000 U for about 3 min. After centrifugation at 10,000 g for about 60 min, the upper clear layer was removed. Malondialdehyde (MDA) levels were determined using the method of Van Ye et al. 18 based on the reaction of MDA with thiobarbituric acid (TBA). The results are expressed in nmol/mg protein.
Part of the homogenate was extracted in an ethanol/chloroform mixture (5/3 v/v) to discard the lipid fraction, which caused interference in the activity measurements of superoxide dismutase (SOD), 19 catalase (CAT), 20 and glutathione S-transferase (GST) 21 activities. The results are expressed in U/mg protein.
Histopathological analysis
Muscle tissue samples from mice were fixed in 10% buffered formalin for 48 h. After fixation, the muscle samples taken for routine tissue follow-up were embedded in paraffin. Sections of 4-µm thickness were taken from paraffin blocks using a microtome (Leica RM2245, Germany) and stained with hematoxylin and eosin (H&E) to evaluate histopathological changes. Prepared tissue samples were viewed under a Leica DM 4000B (Germany) computer-aided light microscope, evaluated in the Leica LAS V4.9 program, and compared between groups. H&E-stained muscle tissue samples were examined at 20× and 40× magnifications, and muscle damage, disorganization, and degeneration of muscle cells, as well as changes in inflammatory cell infiltration in the tissue, were evaluated, and images were taken at 40× magnification. Each parameter was scored between 0 and 3 (0, normal; 1, mild; 2, moderate; 3, severe), and the level of IRI was semi-quantitatively obtained by summing the scores of these two parameters, and scores between 0 and 6 were determined.22,23
Statistical analysis
The Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA) 20.0 for Windows was used. Each categorical variable was analyzed using the Kolmogorov–Smirnov test. Biochemical and histopathological parameters were tested using the Kruskal–Wallis test, Bonferroni Correction test, and Mann–Whitney U test. A statistical value of less than 0.05 was considered significant. All values were expressed as mean ± standard deviation (Mean ± SD).
Result
When gastrocnemius tissue samples were compared in terms of MDA levels, there was a significant difference between the groups (p < 0.001). MDA levels were significantly higher in the D, DIR, DIRS, and DIRS-FC60 groups than in the C group (p = 0.010, p < 0.001, p < 0.001, and p = 0.014, respectively). In addition, the MDA level was significantly higher in the DIR group than in the D group (p < 0.001). MDA levels in the DIRS, DIR-FC60, and DIRS-FC60 groups were lower than in the DIR group (p < 0.001, p < 0.001, and p < 0.001, respectively) (Table 1).
Biochemical data of gastrocnemius muscle tissue [Mean ± SD].
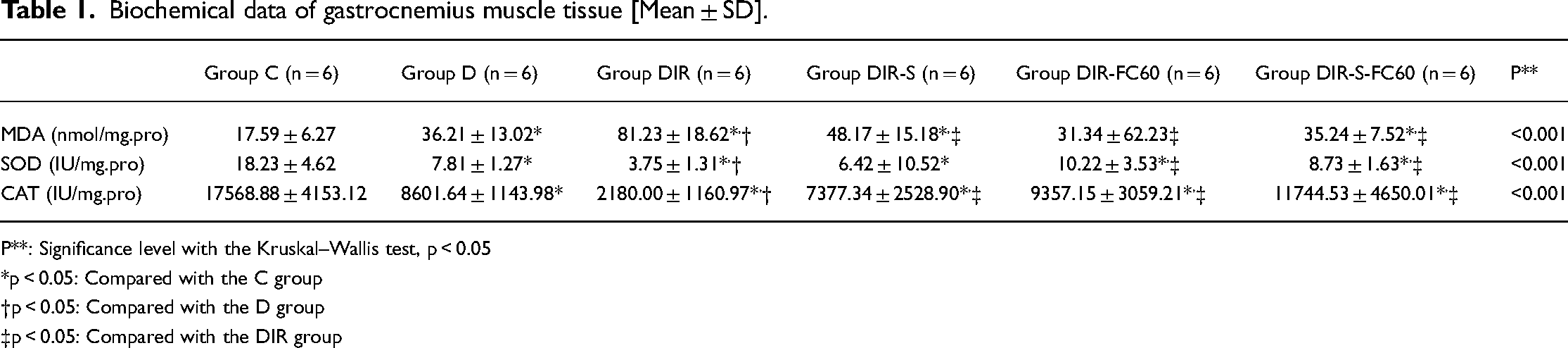
P**: Significance level with the Kruskal–Wallis test, p < 0.05
p < 0.05: Compared with the C group
p < 0.05: Compared with the D group
p < 0.05: Compared with the DIR group
The enzymatic activity of CAT and SOD in gastrocnemius tissue showed significant differences between the groups (p < 0.001 and p < 0.0001, respectively). CAT enzyme activity was significantly reduced in all groups compared with the C group (p < 0.001, p < 0.001, p < 0.001, p < 0.001, and p = 0.005, respectively). Furthermore, CAT enzyme activity was significantly lower in the DIR group than in the D group (p = 0.002). CAT enzyme activity was higher in the DIRS, DIR-FC60, and DIRS-FC60 groups than in the DIR group (p = 0.001, p = 0.014, and p < 0.001, respectively) (Table 1).
SOD enzyme activity was lower in all groups than in the C group (p < 0.001, p < 0.001, p < 0.001, p < 0.001, and p < 0.001, respectively). Moreover, SOD enzyme activity was significantly lower in the DIR group than in the D group (p = 0.007). SOD enzyme activity in the DIR-FC60 and DIR-S-FC60 groups was higher than in the DIR group (p < 0.001 and p = 0.001, respectively) (Table 1).
There was a significant difference in disorganization and degeneration of muscle cells when the groups were compared (p < 0.001). The disorganization and degeneration of muscle cells were significantly greater in all groups compared with the C group (p = 0.016, p < 0.001, p < 0.001, p < 0.001, and p < 0.001, respectively). In addition, the disorganization and degeneration of muscle cells in the DIR, DIR-S, and DIR-FC60 groups were significantly greater than in the D group (p < 0.001, p = 0.001, and p = 0.014, respectively). The disorganization and degeneration of muscle cells in the DIR-S-FC60 group were significantly less than in the DIR group (p = 0.041) (Table 2, Figure 1).

Gastrocnemius muscle tissue, HE ×40. In the cross sections of the control group specimens, muscle cells with polygonal shapes and peripherally located nuclei, normal fascicle structures formed by muscle cells and cell groups, transverse striations in longitudinal sections, and normal muscle cells with peripherally located nuclei were observed. When the samples from the diabetes group were examined, it was observed that the muscle cells mostly lost their polygonal shape, and the typical placement of the nuclei was lost in some of the cells. These degenerative changes were accompanied by interstitial edema, in which the intercellular space was widened, and marked inflammatory cell infiltration. In ischemia–reperfusion groups, it was observed that muscle damage became more prominent, cells increased in eosinophilia in places, cells increased in size with edema and loss of transverse striation, degeneration occurred in varying degrees from small cytoplasmic vesicles to large cytoplasmic vacuoles, and there was fragmentation in which cytoplasmic integrity was disrupted. When muscle damage and accompanying inflammatory cell infiltration were evaluated by scoring, it was observed that the damage caused by ischemia–reperfusion was milder in the treatment groups, especially in the DIR-FS group.
Histopathological data of gastrocnemius muscle tissue [Mean ± SD].

P**: Significance level with the Kruskal–Wallis test, p < 0.05
p < 0.05: Compared with the C group
p < 0.05: Compared with the D group
p < 0.05: Compared with the DIR group
When the groups were compared in terms of skeletal muscle inflammatory cell infiltration, there was a significant difference between the groups (p < 0.001). Skeletal muscle inflammatory cell infiltration in all groups was significantly greater than in the C group (p < 0.001 for all). In addition, skeletal muscle inflammatory cell infiltration was significantly greater in the DIR group than in the C group (p = 0.043). The inflammatory cell infiltration in the DIR-S, DIR-FC60, and DIR-S-FC60 groups was significantly less than in the DIR group (p = 0.031, p = 0.011, and p = 0.013, respectively) (Table 2, Figure 1).
When the groups were compared in terms of skeletal muscle total damage scores, there was a significant difference between the groups (p < 0.001). Skeletal muscle total damage scores in all groups were significantly higher than in the C group (p < 0.001 for all). The skeletal muscle total damage score was also significantly higher in the DIR group than in the C group (p = 0.003). The total damage scores in the DIR-FC60 and DIR-S-FC60 groups were significantly lower than in the DIR group (p = 0.018 and p = 0.008, respectively) (Table 2, Figure 1).
In the cross sections of the control group samples, normal muscle cells with polygonal shapes and peripherally located nuclei, muscle cells, and normal fascicle structures formed by cell groups, transverse striations in longitudinal sections, and peripherally located nuclei were observed (Figure 1, Group C). When the samples from the diabetes group were examined, it was seen that the muscle cells mostly lost their polygonal shape, and the typical placement of the nuclei was lost in some cells. These degenerative changes were accompanied by interstitial edema, in which the intercellular space was widened, and there was marked inflammatory cell infiltration (Figure 1, Group D). In the IR groups, notable muscle damage was observed. There was an increase in eosinophilia in certain areas, accompanied by an enlargement of cell size, edema, and loss of transverse striation. In addition, varying degrees of degeneration were evident, ranging from small cytoplasmic vesicles to large cytoplasmic vacuoles, and there was fragmentation in which cytoplasmic integrity was disrupted (Figure 1, all DIR groups). When muscle damage and accompanying inflammatory cell infiltration were evaluated by scoring, it was seen that the damage caused by IR was milder in the treatment groups, especially in the DIR-S-FC60 group (Figure 1, DIR-S, DIR-FC60, and DIR-S-FC60 groups).
Discussion
In this study, we examined the effects of fullerenol C60 and sevoflurane application on histopathological and oxidative damage to gastrocnemius muscle tissue in lower extremity IRI. The study results showed that fullerenol C60 and sevoflurane application improved IR-induced damage in muscle tissue histopathology by reducing oxidative stress.
Diabetes mellitus (DM) is a common chronic disease. One of the most important reasons for the development of peripheral artery disease (PAD) is the presence of diabetes, and PAD is more severe in these patients. 24 Diabetes increases the risk of PAD fourfold, which occurs at an earlier stage and progresses more rapidly than in people without diabetes.25,26
The endoplasmic reticulum (ER) is responsible for intracellular protein folding, post-transcriptional modification, lipid synthesis, and Ca2+ storage. 27 This organelle also regulates numerous other molecular pathways and has a role in reduction–oxidation regulation, autophagy, and cell death. 28 Disturbance of ER internal balance causes the increase of unfolded or misfolded proteins in the cell, causing the cell to undergo apoptosis. It has been stated that ER homeostasis disorder plays a role in the pathophysiology of DM by causing β-cell dysfunction in type 1 and type 2 diabetes. 4
Also, hyperglycemia present in DM causes excessive superoxide production by the mitochondrial electron transport chain through the activation of pathways such as increased polyol pathway flux, increased advanced glycation end product (AGE) formation, activation of protein kinase C (PKC) isoforms, and increased hexosamine pathway flux. For these reasons, mitochondrial dysfunction, which is already present in DM due to hyperglycemia, causes more reactive oxygen species (ROS) production in IR, basal oxidative stress, and depletion of antioxidant defense systems, leading to further damage in DM. 5 Along with these factors, the susceptibility to IRI increases in diabetes.
IRI, the imbalance between oxidant–antioxidant processes, accompanied by excessive production of ROS, 29 can be expressed as a pathophysiological stress that develops with local and systemic inflammation caused by the inability to ensure and restore blood flow to the organ. 30 The increase in ROS and inflammatory cells in the ischemic tissue affects blood flow in the ischemic tissue, causing even more inflammation. 31 It is important to apply anti-oxidative stress and anti-inflammatory strategies to reduce the damage in IRI. This is especially important in diabetes.
Malondialdehyde (MDA), an intermediate product of lipid peroxidation, is an important marker indicating the level of oxidative stress in tissues. 32 It is stated that catalase (CAT) is a type of conjugate with a potent radical scavenging function that can protect tissues from oxidative damage. 33 Superoxide dismutase (SOD), similar to CAT, plays a crucial role as an important antioxidant. 34
In this study, we investigated whether fullerenol C60 and sevoflurane ameliorated IR-induced damage through histopathological examination of the gastrocnemius muscle in a lower limb IRI model in streptozocin-induced diabetic mice. In our study, we evaluated antioxidant protection with CAT and SOD and oxidative stress with MDA. Because the blood sample showed overall damage, we used biochemical markers of muscle tissue to demonstrate tissue damage.
In our study, MDA levels in the DIR-S, DIR-FC60, and DIR-S-FC60 groups were lower than in the DIR group. CAT enzyme activities in the DIR-S, DIR-FC60, and DIR-S-FC60 groups were higher than in the DIR group. SOD enzyme activities in the DIR-FC60 and DIR-S-FC60 groups were higher than in the DIR group. SOD enzyme activity in the DIR-S group was higher than in the DIR group, but the difference was not significant. Upon reviewing the histopathological results of our study, it was observed that the disorganization and degeneration of muscle cells in the DIR-S-FC60 group were less than in the DIR group. In addition, in the DIR-S and DIR-FC60 groups, these aspects were lower than in the DIR group, but the difference was not significant. The inflammatory cell infiltration in the DIR-S, DIR-FC60, and DIR-S-FC60 groups was less than in the DIR group, and the total damage scores in the DIR-FC60 and DIR-S-FC60 groups were lower than in the DIR group. In the DIR-S group, the total damage score was lower than in the DIR group, but the difference was not significant. According to our results, regarding the total histopathological damage score, we found the best result in the group in which both fullerenol C60 and sevoflurane (group DIR-S-FC60) were applied, followed by the DIR-FC 60 and DIR-S groups.
Sevoflurane is a volatile anesthetic that is frequently used in the clinic due to its advantages, such as having a low blood-gas partition coefficient, providing sufficient depth of anesthesia in a short time, short awakening time, less airway irritation, and being able to be used in inhalation anesthesia. 35 The protective effects of sevoflurane at different pathways in IRI have been demonstrated in various studies.
Wu et al. 36 stated that pyroptosis contributes to inflammatory activation, involving the production of caspase-1 and gasdermin-D (GSDMD), and along with the release of various pro-inflammatory cytokines. According to their studies, sevoflurane reduced the effects of IRI on heart tissue by inhibiting the purinergic receptor-7 (P2X7)-NLR family pyrin domain-containing 3 (NLRP3) signaling pathway. This inhibition resulted in reduced expression of interleukin (IL)-1β, IL-18, and GSDMD, thereby regulating pyroptosis and diminishing inflammation. It has been stated that heart function is thus preserved. Another study revealed that sevoflurane alleviated hepatic IRI in mice by reducing oxidative stress and inflammatory response via the miR 218 5p/GAB2/PI3 K/AKT pathway. 37 Zhao et al. 38 stated that postconditioning with sevoflurane reduced cerebral IR-induced neurological deficits in rats by suppressing neuroinflammatory responses through inhibition of the TLR4/MyD88/TRAF6 signaling pathway.
Fullerenols are water-soluble polyhydroxylated derivatives of fullerenes with hard nanosized carbon particle skeletons. The lack of electrons in their structures makes them effective catalysts in biochemical reactions. Hydroxyl groups, which determine the affinity of cell membranes to hydrophobic enzymatic fragments and lipid structures, provide fullerenols with aqueous solubility. 39 Various studies have shown that fullerenol C60 acts as an effective radical scavenger, effectively eliminating ROS in ischemic conditions and reducing the effects of oxidative damage.9,40,41
There are few studies in the literature showing the effect of fullerenol C60 on diabetes and lower limb IRI. Kartal et al. 10 intraperitoneally administered fullerenol C60 (100 µg/kg), 30 min before the ischemia period, in a lower extremity ischemia–reperfusion model in streptozocin-induced diabetic rats, and the results of their study showed that fullerenol C60 reduced IR-induced skeletal muscle damage in diabetic rats. Nozdrenko et al. 42 obtained positive results in the biomechanical and biochemical markers examined when they intramuscularly administered water-soluble C60 fullerene at doses of 0.5, 1, and 2 mg/kg 1 h before creating a muscle ischemia model in rats. They stated that soluble C60 fullerenes can be used for protective purposes to reduce the negative consequences of ischemic damage in skeletal muscles. In the study of Zavodovskyi et al., 43 following a 3-h ischemia period in the skeletal muscle of rat limbs, C60 fullerene was intramuscularly administered at 1, 2, and 3 mg/kg immediately after 1 h of reperfusion. It was observed that there were positive results in both skeletal muscle contractions and biochemical parameters.
We considered the literature in our study when deciding on the doses and the method of administration. 10 In this experimental study, we preferred to intraperitoneally apply fullerenol C60 because it is easy to apply and provides rapid absorption.44,45
To establish the lower extremity IRI model, we chose to apply an atraumatic microvascular clamp to the infrarenal abdominal aorta. This approach, utilized in previous studies, was chosen for its ease of application.10,45,46
The study has some limitations. A sample size/power analysis could not be performed due to the restriction imposed by the animal research committee on the number of animals allowed. Consequently, the number of mice in each group was determined based on the committee's authorization. The administration of ketamine and xylazine for mouse anesthesia raises the possibility that the effects of these drugs on oxidative damage could not be entirely ruled out. Similarly, the use of sevoflurane with 100% oxygen in the study may have influenced the increase in reactive oxygen products in the sevoflurane groups. This potential impact could not be excluded in our study. Another limitation is the absence of hemodynamic monitoring during the experiment.
Conclusion
Our study indicates that the administration of fullerenol C60 at a dose of 100 mg/kg, given intraperitoneally 30 min before the ischemia period in mice, in conjunction with sevoflurane application, effectively ameliorated muscle damage induced by IRI through the reduction of oxidative stress. Sevoflurane demonstrated its capacity to mitigate oxidative damage in muscle tissue during IRI, and this protective effect was enhanced in combination with fullerenol C60, leading to improved histopathological outcomes. These findings highlight the tissue-protective effects of sevoflurane anesthesia and fullerenol C60 administration in the context of IRI in diabetic mice, providing valuable insights for future research on IRI in diabetes.
Footnotes
Acknowledgments
Not applicable.
Authors’ contributions
MA, NŞ and AK designed the study and analyzed and interpreted data. YP, ABB and ÇÖ performed the experiments. AK and MA analyzed and interpreted data. MA, AHA and ZK confirm the authenticity of all the raw data. YP, AK, MA and NŞ provided scientific and technical assistance and critically revised the article for important intellectual content. ÇÖ and AİE collected samples. ZY and MK performed cellular and molecular experiments. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Yücel Polat is a Cardiovascular Surgeon. His research area is ischemia reperfusion, nanoparticles, CABG.
Necmiye Şengel is an Anesthesiology and Reanimation specialist. Her research area is ischemia reperfusion, nanoparticles, anesthesia applications.
Ayşegül Küçük is Professor of Physiology. Her research area is ischemia reperfusion, nanoparticles, Alzheimer's, neurophysiology, behavior.
Çağrı Özdemir is an Anesthesiology and Reanimation specialist. His research area is ischemia reperfusion, nanoparticles, anesthesia applications.
Zeynep Yiğman is a specialist in Histology and Embryology. She is working as assistant professor in the Department of Histology and Embryology in Gazi University Faculty of Medicine. Her research area: histology, histopathology, mesenchymal stem cells, ischemia-reperfusion injury, neuroscience.
Abdullah Burak Balcı is a Cardiovascular Surgeon. His research area is ischemia reperfusion, nanoparticles, CABG.
Aydan İremnur Ergörün is an Anesthesiology and Reanimation specialist. Her research area is ischemia reperfusion, nanoparticles, anesthesia applications.
Mustafa Kavutçu is a professor of Medical Biochemistry. His research areas are free radicals and antioxidants, oxidative stress, toxicology, purification and kinetic properties of enzymes (protein), flavonoids and other basic and clinical research related to medical biochemistry.
Mustafa Arslan is Professor of Anesthesiology and Reanimation. His research area is ischemia reperfusion, nanoparticles, Alzheimer's and anesthesia applications.