
Abstract
Background
Most children with neurocritical illness are at risk of physical, neurocognitive, and psychosocial sequelae and need centralized early rehabilitation care.
Objective
To identify the effectiveness and safety of centralized early rehabilitation care for children with severe acquired brain injury.
Methods
This is a mixed methods study—an implementation study and single-center retrospective cohort study with historical control. All children with severe acquired brain injury hospitalized in a specialized rehabilitation center in a comprehensive tertiary pediatric hospital between September 2016 and August 2020 were included. Patients treated in the centralized early rehabilitation unit were compared to historical controls dispersed in the normal inpatient rehabilitation ward. The effectiveness outcomes were measured by the Pediatric Cerebral Performance Category (PCPC) scale and the incidence of newly onset comorbidities. The safety outcomes were indicated by the mortality rate and the incidence of unexpected referrals.
Results
One hundred seventy-five patients were included. The delta PCPC scores of the first 4 weeks of inpatient rehabilitation in the intervention group were significantly lower than the control group (Z = −2.395, p = 0.017). The PCPC scores at 1 year in the intervention group were significantly reduced as compared to the control group (Z = −3.337, p = 0.001). The incidence of newly onset pneumonia/bronchitis was also decreased in the intervention group (χ2 = 4.517, p = 0.034). No death of patients was recorded, and there was no significant difference in unexpected referral rate between the two groups (χ2 = 0.374, p = 0.541).
Conclusions
The centralized pediatrics early rehabilitation unit is effective and safe for children with severe acquired brain injury. Further multicenter prospective implementation studies on effectiveness, safety, and economic evaluation are needed.
Introduction
With the development of critical care medicine, there is an increase in the survival of children suffering from critical illnesses, especially severe acquired brain injury (sABI).1,2 Children with neurocritical illness are at a risk of physical, neurocognitive, and psychosocial sequelae, which can lead to lifelong impediments and reduction in the quality of life of patients and their families.3–5 Most of these medically stable children in the intensive care unit (ICU) or the neurointensive care unit (NICU) still require centralized early rehabilitation care provided by the professional multidisciplinary team in the inpatient rehabilitation settings.
Emerging literature has demonstrated that a continuous chain of centralized early rehabilitation can contribute to functional recovery, while being safe and cost-effective for adult survivors of critical illness.6–11 However, such vital care centers are rarely available in low-resource settings. 12 Notably, there is no existing literature on children in this field. Our previous national survey on early rehabilitation also revealed the shortage of rehabilitation resources for critically ill children in China and further suggested building a regional two-level integrated system comprising centralized early rehabilitation units and surrounding early rehabilitation networks to solve this problem. 13
In order to explore the appropriate rehabilitation strategies for critically ill children in China, a centralized pediatric early rehabilitation unit has been established in the rehabilitation department of Children's Hospital of Chongqing Medical University (CHCMU) since September 2018 by the leader of the Rehabilitation Group of Pediatrics Branch of Chinese Medical Association. 14 However, there is insufficient evidence on the advantages of such rehabilitation units for children with sABI as well as lack of scientific descriptions of these patients. Therefore, we designed this implementation study on children with sABI to identify the effectiveness and safety of the centralized early rehabilitation care implemented in this unit.
Methods
Study design, setting, and participants
This is a mixed methods study—an implementation study and single-center retrospective cohort study with historical control. The Standards for Reporting Implementation Studies (StaRI) checklist 15 and the STROBE Statement—checklists are presented as the Supplemental Digital Content eTable 1 and eTable 2. This study was conducted in CHCMU with approval from the Ethics Committee of CHCMU (2021-34). Written informed consent was obtained from the parents or legal guardians of each child at admission.
All consecutive series of children between 1 month and 18 years of age who had been initially treated in ICU/NICU in CHCMU or other hospitals due to sABI and were hospitalized in the rehabilitation department of CHCMU during the subacute phase from September 2016 to August 2020 were retrospectively included in this study. Patients with previous ABI, neurodevelopmental disorders, epilepsy, or genetic and metabolic abnormalities, and patients that willingly left ongoing treatment in the hospital without doctors’ advice were excluded.
sABI was defined as injuries to the central nervous system due to acute traumatic or nontraumatic (vascular, anoxic, neoplastic, or infectious) causes that produced a state of coma (Glasgow Coma Scale ≤ 8) lasting at least 24 h, resulting potentially in a wide range of impairments to the physical, cognitive, and/or psychological functioning.16,17
CHCMU is the largest comprehensive tertiary pediatric hospital with over 2000 beds and the National Clinical Research Center for Child Health and Disorders in southwest China. Critically ill children from the local and surrounding provinces would be admitted to or transferred to this hospital. The rehabilitation department is a specialized rehabilitation center providing comprehensive rehabilitation services that are beyond the scope of the local rehabilitation services.
Intervention
The centralized early rehabilitation unit was established in the rehabilitation department in September 2018. After its establishment, all the children with sABI would be admitted to this unit. In this study, all eligible patients treated only in the normal inpatient rehabilitation ward for 2 years prior to September 2018 were regarded as historical controls, whereas children with sABI admitted in this unit thereafter till August 2020 were included as part of the intervention group.
Different from the traditional rehabilitation ward, this centralized early rehabilitation unit had 18 beds with necessary monitoring and nursing equipment dedicated to critically ill children with serious dysfunctions and comorbidities. Comprehensive rehabilitation and general medical services were provided by a 24/7 independent multidisciplinary team consisting of pediatric rehabilitation medicine physicians, nurses, physical therapists, occupational therapists, and speech and language therapists specialized in treating children with sABI. On the other hand, patients in the historic control group were dispersed in the normal inpatient rehabilitation ward where physicians, nurses, and therapists simultaneously treated patients with different disorders such as children with cerebral palsy, neurodevelopmental disorders, or osteoarthropathy, etc.
Individual interventional programs were made for every patient due to the heterogeneous nature of the patient population as well as the variation in comorbidities and functional impairments associated with sABI. The rehabilitation approach was planned and implemented according to the principle of rehabilitation medicine. 18 The comorbidities were managed by pediatric rehabilitation physicians with necessary assistance from medical professionals from other specialties.
Outcomes
The primary effectiveness outcomes were measured as the patients’ short-term and long-term neurological outcomes measured by the Pediatric Cerebral Performance Category (PCPC) scale. The PCPC scale is a conventional, reliable, and valid tool for assessing the neurological outcome of pediatric intensive care. 19 To measure the improvement in the short-term neurological outcome, the delta PCPC scores were calculated as the difference of scores at the end and beginning of the first 4 weeks of inpatient rehabilitation. The long-term neurological outcome of patients was directly determined by PCPC scores at 1 year of course. The baseline PCPC score was considered 5 as all patients were in coma in the acute phase as mentioned in the inclusion criteria of this study. The long-term neurological outcome was only measured for successfully followed-up patients.
The secondary effectiveness outcome was determined by the incidence of the newly onset comorbidities during the first 4 weeks of inpatient rehabilitation. Patients with comorbidities requiring regular monitoring with/without treatment in the time-window were recorded. Comorbidities occurring in patients with sABI were classified into three types: “Newly onset” comorbidity—this refers to the onset of comorbidity during the first 4 weeks’ time-window. “Not newly onset” comorbidity—this indicates the beginning of the comorbidity in the patient before admission to the rehabilitation department and exists thereafter. “Unknown” comorbidity—this refers to the comorbidity where onset time was unknown as no diagnostic tests were conducted before admission to the rehabilitation department. Whether the comorbidities led to unexpected referral was also recorded.
The primary and secondary safety outcomes were revealed by the mortality rate of patients and the incidence of unexpected referral during the time-window of first 4 weeks of inpatient rehabilitation, respectively. All the referrals from the rehabilitation department to other departments were recorded and analyzed. “Unexpected referrals” are those caused by the deterioration of the patient's condition. Typical expected referrals resulted from selective operations like cranioplasty, internal fixation removal surgery, etc.
Data collection and statistical analysis
Patients’ electronic medical records were reviewed for sociodemographic information, medical history, present illness, examinations, diagnosis, and treatments. All the PCPC scores were obtained from the medical records of hospitalization and outpatient visit or phone-call follow-up retrospectively.
Data were represented as means with standard deviations, medians and interquartile ranges, or proportions according to the characteristics of the data. The chi-square test or the Fisher's exact test (when a cell has an expected value of 5 or less) was used to determine statistical difference between nominal data. The t test or the Mann-Whitney U test was used to determine the statistical difference between quantitative data of normal distribution or non-normal distribution, respectively. The level of statistical significance was established at p < 0.05. All statistical analyses were performed with IBM SPSS Statistics, version 21.
Results
Clinical characteristics
One hundred seventy-five patients (80 patients in the intervention group and 95 patients in the historical control group) were included. The characteristics of these patients are described in Table 1. Characteristics including age at onset, sex, etiology, record of hospitalization in ICU, history of mechanical ventilator use (>24 h), last department before rehabilitation, presence of prolonged disorders of consciousness (pDoC), conditions at admission to the rehabilitation department were compared between the two groups, all of which shared no statistic difference between the two groups, indicating that the source of patients was relatively stable over the 4 years. And 163 patients (75 patients in the intervention group and 88 patients in the historical control group) were successfully followed up for 1 year (Figure 1 shows the flowchart) and analyzed for the long-term neurological outcome. The demographic summary details of these successfully followed-up patients have been mentioned in eTable 3 in the Supplemental Digital Content. Similarly, the characteristics of the 163 patients in the two groups also shared no statical differences.

Flowchart.
Characteristics of patients.
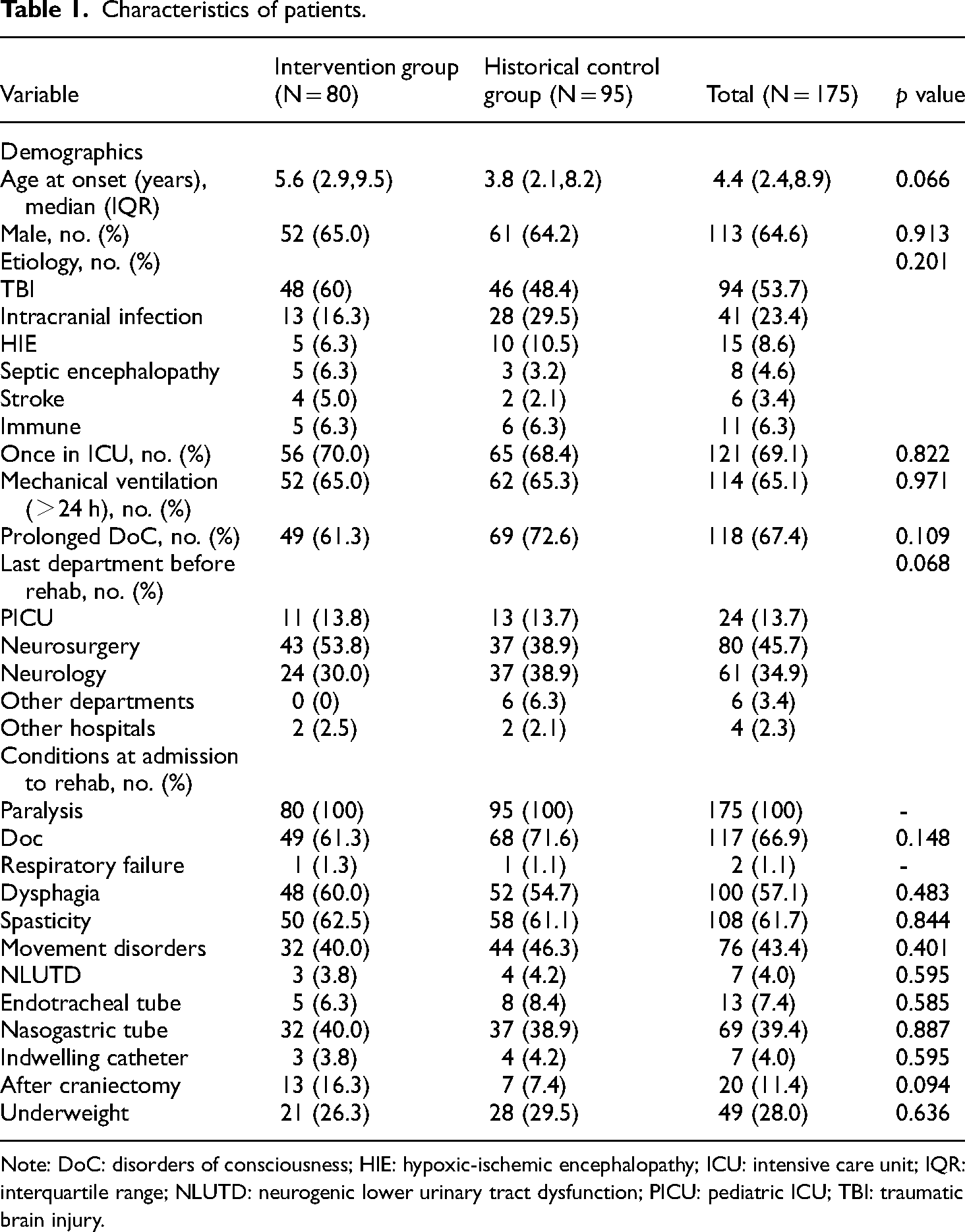
Note: DoC: disorders of consciousness; HIE: hypoxic-ischemic encephalopathy; ICU: intensive care unit; IQR: interquartile range; NLUTD: neurogenic lower urinary tract dysfunction; PICU: pediatric ICU; TBI: traumatic brain injury.
The top 10 comorbidities during the first 4 weeks of inpatient rehabilitation are listed in Table 2.
The top 10 comorbidities during the first 4 weeks of inpatient rehabilitation.

Note: Values are presented in number and percentage in brackets.
a Statistically significant at the level of p < 0.05.
b This diagnose is only considered for children ≥ 3 years of age (59 in each of the two groups) as dual energy X-ray absorptiometry whole body measurements are feasible and can provide reproducible measures of BMD and areal BMD for children ≥ 3 years of age.
Outcomes of the effectiveness and safety
The comparison of effectiveness and safety outcomes between the intervention group and the historical control group is shown in Table 3.
Comparison of effectiveness and safety outcomes between the intervention group and the historical control group.

Note: a The number of patients who were successfully followed up, which was regarded as the total number of patents when calculating the PCPC score at 1 year.
b Statistically significant at the level of p < 0.05.
IQR: interquartile range; PCPC: Pediatric Cerebral Performance Category.
For the comparison of effectiveness outcomes, delta PCPC scores of the first 4 weeks of inpatient rehabilitation for patients treated in the centralized early rehabilitation unit were significantly lower than those for patients in the historical control group (−1 (−1, 0) vs. 0 (−1, 0), Z = −2.395, p = 0.017). Furthermore, the PCPC scores at 1 year of the course for patients treated in the centralized early rehabilitation unit were significantly lower than those for patients in the historical control group (2.0 (1.0, 4.0) vs. 3.0 (2.0, 4.75), Z = −3.337, p = 0.001). In addition, the incidence of newly onset pneumonia/bronchitis during the first 4 weeks of inpatient rehabilitation in the intervention group was also lower than that in historical controls (15.0% vs. 28.4%, χ2 = 4.517, p = 0.034).
With respect to the comparison of safety outcomes, no death was recorded during the 4-year observation period. There were seven cases of unexpected referral in the intervention group during the first 4 weeks of inpatient rehabilitation, including three patients with hydrocephalus requiring surgery, two with respiratory failure, one with subdural fluid requiring surgery, and one with newly onset anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis. The six cases of unexpected referral in the historical control group included two patients with respiratory failure, two with uncontrolled seizures, one with subdural fluid requiring surgery and one with unexplained acute deterioration in the level of consciousness. There was no significant difference in unexpected referral rate between the intervention group and the historical controls (8.8% vs. 7.4%, χ2 = 0.374, p = 0.541).
Discussion
This study was conducted to enhance our knowledge about actual rehabilitation practices in a centralized pediatric early rehabilitation unit for children with sABI in China and to demonstrate the effectiveness and safety of the pattern of centralized early rehabilitation care. The results obtained from this study indicate the highly effective nature of this rehabilitation department from the aspect of improving short- and long-term functional recovery as measured by the PCPC scale and decreasing the incidence of newly onset pneumonia/bronchitis during the first 4 weeks’ stay in the rehabilitation department. Moreover, the safety of this unit can be confirmed as there was no report of additional unexpected referral or risk of death during patients’ first 4 weeks’ stay in the rehabilitation department.
Specialized neurorehabilitation is highly recommended by Lancet Neurology Commission authors for sTBI patients in acute and postacute phase, as it can facilitate recovery and restoration of functional independence in the long term. 12 Hence, concept of specialized early rehabilitation care was put into practice by the establishment of a centralized pediatric early rehabilitation unit for neurocritically ill children. This preliminary study demonstrated that patients admitted in this unit showed significant improvements in short and long-term neurological functional recovery on the PCPC scale. Though there are no similar studies on children mentioned in the literature, reports on adult patients with sTBI show comparable findings. A population-based study in Denmark showed significantly better scores on the Glasgow Outcome Scale scores at discharge in patients admitted in a centralized unit as compared to patients that received subacute rehabilitation in different wards. 9 Andelic et al. 8 also reported that better functional outcomes assessed with the Glasgow Outcome Scale Extended and the Disability Rating Scale 1-year postinjury could be observed in patients who received early onset and a continuous chain of rehabilitation.
Our research data also shows that the risk of newly onset pneumonia or bronchitis during the first 4 weeks of hospitalization in the rehabilitation department decreased after the establishment of this unit. The absence of respiratory tract infection could directly reduce the suffering of patients and the burden of care; furthermore, we suspect that it gave a more stable physical state for rehabilitation therapy, which might be a potential reason for the better functional outcome. As reported by Ganesh et al., in inpatient rehabilitation facilities, patients with higher number of medical complications are associated with lower functional levels 1-year postinjury. 20 Hence, we presume that the specialized care provided by our unit could aid in improving the stability of the physical state for rehabilitation therapy, indicating a potential reason for better functional outcomes.
As for the benefits of centralized early rehabilitation care on the respiratory system and overall health for critically ill patients, direct evidence has been reported in a study conducted by Wang et al. describing the benefits of centralized early rehabilitation care on the respiratory system and overall health for critically ill adult patients. For adult patients with severe stroke associated pneumonia, the respiratory “critical care-sub-critical care-rehabilitation integrated management model” could significantly improve the treatment effect by measuring clinical pulmonary infection score (CPIS), oxygenation index and the acute physiology and chronic health evaluation II (APACHE II) score at discharge, shorten average hospitalization days and improve patient/family satisfaction. 21
In addition, there is also research evidence that the monitoring and rehabilitation interventions of dysphagia can also prevent pneumonia in sABI patients. Dysphagia is a common and critical consequence of sABI, which can lead to the tracheobronchial aspiration that may cause pneumonia.22,23 Langmore emphasized neurologists should detect and treat dysphagia early to prevent pneumonia in neurological ICU patients. 24 The efficacy of dysphagia rehabilitation in preventing pneumonia in acute stroke patients has been confirmed by Hamada et al. 25 In our study, dysphagia was a common dysfunction for sABI children, affecting more than half (57.1%) of our patients at admission to the rehabilitation department. The professional multidisciplinary team in our centralized rehabilitation care unit provided patients with more frequent evaluation and management, such as suctioning of the oropharyngeal secretions, positioning the patient to facilitate swallowing and coughing, and so on, which might indicate the reason for lower risk of newly onset pneumonia or bronchitis.
The safety of the rehabilitation approach is usually assessed by the occurrence of adverse events, including abnormal physiological responses reflected by changes in heart rate, blood pressure, transcutaneous oxygen saturation of the blood, and respiratory rate, and inadvertent removal of invasive devices during training.6,7,26 However, as a retrospective study, the data in our study were collected from medical records. These adverse events observed by therapists were not compulsively informed to and recorded by doctors. Therefore, these parameters were not utilized in our study to reflect the safety of the unit. Instead, only the parameters of risk of death and unexpected referral were analyzed as these are considered strong negative events for rehabilitation facilities. From our research data, no additional risk of death or unexpected referral occurred during patients’ first 4 weeks of stay in the rehabilitation department.
The unexpected referrals in our study almost resulted from severe comorbidities, including respiratory failure, hydrocephalus, subdural fluid, and uncontrolled seizures. Clinically, the management of various comorbidities is a crucial part of work for rehabilitation physicians and sometimes it is given higher priority than the management of dysfunctions, because some comorbidities (such as hypertensive crisis, acute respiratory failure, elevated intracranial hypertension, active uncontrolled seizures, and unstable pelvic or spinal fracture, etc.) can act as definite contraindications to rehabilitation and may impede therapeutic efforts.20,27,28 Furthermore, certain comorbidities are likely to have deleterious effects on recovery or cause additional risk of death.20,29 On the other hand, treating comorbidities can bring benefits like decreasing metabolic costs, 20 or reducing the potentially modifiable risk factors to improving outcomes. 30 However, certain specific problems for patients with sABI can complicate the diagnosis of their comorbidities in clinical (e.g. patients in a state of seriously impaired consciousness or cognition are not able to report symptoms, the disappearance of cough reflex or ICU-AW may make the symptoms of pneumonia atypical). 20 Thus, it is essential for rehabilitation physicians to be aware of both common as well as relatively rare but potentially life-threatening comorbidities.
As our study is retrospective in nature, there are certain limitations which need to be acknowledged. The PCPC scale used in our study to indicate the primary effectiveness outcomes of our patients can be regarded only as a simple grading tool for basic assessment of patient condition. However, considering the heterogeneity of the patient population and the need for long-term follow up, it is infeasible to include detailed functional assessment scales in this study. Moreover, detailed data such as the regime of therapies and vital sign fluctuations during therapies was impossible to extract from medical records.
Conclusions
In summary, the centralized pediatric early rehabilitation unit is effective from the aspect of improving short-term and long-term functional recovery and reducing the risk of newly onset pneumonia or bronchitis without putting the additional risk of death or unexpected referral for children with sABI. Before widely promoting the centralized early rehabilitation unit, further multicenter prospective implementation studies on effectiveness, safety, and economic evaluation are needed.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504241236354 - Supplemental material for The effectiveness and safety of centralized early rehabilitation care for critically ill children with severe acquired brain injury: A retrospective cohort and implementation study
Supplemental material, sj-pdf-1-sci-10.1177_00368504241236354 for The effectiveness and safety of centralized early rehabilitation care for critically ill children with severe acquired brain injury: A retrospective cohort and implementation study by Ting Zhang, Xiao-ling Duan, Yu-xia Chen, Ying Feng, Qin-rong Huang, Xiang Tang, Li Lin and Nong Xiao in Science Progress
Supplemental Material
sj-docx-2-sci-10.1177_00368504241236354 - Supplemental material for The effectiveness and safety of centralized early rehabilitation care for critically ill children with severe acquired brain injury: A retrospective cohort and implementation study
Supplemental material, sj-docx-2-sci-10.1177_00368504241236354 for The effectiveness and safety of centralized early rehabilitation care for critically ill children with severe acquired brain injury: A retrospective cohort and implementation study by Ting Zhang, Xiao-ling Duan, Yu-xia Chen, Ying Feng, Qin-rong Huang, Xiang Tang, Li Lin and Nong Xiao in Science Progress
Supplemental Material
sj-pdf-3-sci-10.1177_00368504241236354 - Supplemental material for The effectiveness and safety of centralized early rehabilitation care for critically ill children with severe acquired brain injury: A retrospective cohort and implementation study
Supplemental material, sj-pdf-3-sci-10.1177_00368504241236354 for The effectiveness and safety of centralized early rehabilitation care for critically ill children with severe acquired brain injury: A retrospective cohort and implementation study by Ting Zhang, Xiao-ling Duan, Yu-xia Chen, Ying Feng, Qin-rong Huang, Xiang Tang, Li Lin and Nong Xiao in Science Progress
Footnotes
Acknowledgements
We would like to sincerely thank all the patients and their families involved in this study, as well as all the medical and allied health staff members who cared for these children and contributed to the initial exploration of appropriate rehabilitation strategies for critically ill children in China. We would also like to thank Rhea Seth for linguistic assistance during revision of the manuscript.
Authorship
TZ designed the study, collected and analyzed the data, and wrote the manuscript. XD participated in the study design and data collection. YC, YF, QH, XT, and LL made contributions to collect the data. NX organized the study group and directed this study. All authors have revised the manuscript and approved the final manuscript.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval to report this case was obtained from Ethics Committee of Children's Hospital of Chongqing Medical University (2021-34) on 12/01/2021.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Supplemental material
Supplemental material for this article is available online.
Author biographies
Ting Zhang is an attending physician of Pediatric Rehabilitation. Her area of research is the early and intensive rehabilitation management of neurocritically ill children.
Xiao-ling Duan holds a PhD in Pediatrics. Her area of research is the early and intensive rehabilitation management of neurocritically ill children.
Yu-xia Chen is an attending physician of Pediatric Rehabilitation. Her area of research is Pediatric Rehabilitation focusing on ultrasonic diagnosis and rehabilitation evaluation.
Ying Feng is an attending physician of Pediatric Rehabilitation. Her area of research is Pediatric Rehabilitation focusing on electrophysiological diagnosis.
Qin-rong Huang is an attending physician of Pediatric Rehabilitation. Her area of research is Pediatric Rehabilitation focusing on pediatric neuromuscular diseases.
Xiang Tang is an attending physician of Pediatric Rehabilitation. Her area of research is Pediatric Rehabilitation focusing on acquired brain injury.
Li Lin is an attending physician of Pediatric Rehabilitation. Her area of research is the early and intensive rehabilitation management of neurocritically ill children.
Nong Xiao is a professor in Pediatrics. His area of research is Pediatric Rehabilitation and Pediatric Neurology.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.