
Abstract
Objective:
This study aimed to examine the morphological characteristics of the nasopharynx in unilateral Cleft lip/palate (CL/P) children and non-cleft children using cone beam computed tomography (CBCT).
Methods:
A retrospective study consisted of 54 patients, of which 27 patients were unilateral CL/P, remaining 27 patients have no CL/P. Eustachian tubes orifice (ET), Rosenmuller fossa (RF) depth, presence of pharyngeal bursa (PB), the distance of posterior nasal spine (PNS)-pharynx posterior wall were quantitatively evaluated.
Results:
The main effect of the CL/P groups was found to be effective on RF depth-right (p < 0.001) and RF depth-left (p < 0.001). The interaction effect of gender and CL/P groups was not influential on measurements. The cleft-side main effect was found to be effective on RF depth-left (p < 0.001) and RF depth-right (p = 0.0002). There was no statistically significant relationship between CL/P groups and the presence of bursa pharyngea.
Conclusions:
Because RF is the most common site of nasopharyngeal carcinoma (NPC), the anatomy of the nasopharynx should be well known in the early diagnosis of NPC.
Keywords
Introduction
Pharyngeal recess (PR), also known as Rosenmuller fossa (RF), was first introduced by Johann Christian Rosenmuller in 1808. RF is a small bilateral diverticulum in the nasopharynx that is anatomically critical. RF is located posterior nasopharynx just below the skull base and posterior to the ostium of the Eustachian tube (ET). Its location becomes essential as it is separated from the internal carotid artery only by a thin tissue. 1 The posterior wall of the nasopharynx, which includes various anatomical landmarks such as RF, the opening of ET, and pharyngeal bursa (PB), is composed of loose connective tissue and may result in nasopharyngeal laceration if forceful insertion of the tube during the nasotracheal intubation. 2 Maxillofacial radiologists need to know more about this area because nasopharyngeal carcinoma (NPC), the most common malignant neoplasm of the nasopharynx, occurs in this region. 3 It has been reported that calcific formations such as rhinolith can be seen in this region. 4 The epithelial residue of embryological origin of the posterior wall of the nasopharynx may result in PB, 5 and Tornwaldt disease, which is cyst, abscess, or inflammation of the PB, may develop from PB. 6
Cleft lip and palate (CL/P) is a frequently occurring congenital disability affecting facial appearance, hearing, and speech. CL/P occurs due to the complete or incomplete union of the medial nasal prominence(s) on one or both sides in the embryological period. 7 Although children with isolated cleft lip often have normal or near-normal middle ear function, many children with CL/P experience chronic ET dysfunction, which may occur in the tympanic membrane (TM) retraction or recurrent acute otitis media. 8 Godinho et al. 9 showed in their studies that there might be changes in the normal anatomy of tensor veli palatine (TVP) muscle located laterally of RF. They contributed to opening ET orifice and levator veli palatine (LVP) muscle located anteriorly of RF. 9 Cone beam computed tomography (CBCT) is preferred not only by dentists but also by otolaryngologists thanks to the high image quality in the maxillofacial area, especially when it comes to hard tissue examinations such as bone. 10 We used CBCT to view and evaluate nasopharynx anatomy, including RF, ET, and PB.
This study aims to examine morphologic features of the nasopharyngeal region, which includes RF, ET, and PB in unilateral CL/P children and non-cleft.
Materials and methods
The study consisted of 54 patients, of which 27 patients were unilateral CL/P (18 male, 9 female, 15 cleft line left, 12 cleft line right, average age 11.3 ± 1.9). The remaining 27 patients have no CL/P (16 male, 11 female average age 11.3 ± 1.9). CBCT images of 54 patients aged 8–14 years were obtained from the radiology archive of inonu University Faculty of Dentistry between the years 2014 and 2020. The Clinical Research Ethics Committee of the University Faculty of Medicine approved the study (approval no. 2021/2772). Legal guardians of all participants gave written informed consent before the CBCT. Patients were excluded if the patient's record did not ensure enough quality, craniofacial syndrome, history of nasopharyngeal surgery and any pathological formations in the nasopharynx region. It was confirmed that the patient did not swallow during the CBCT taken. All measurements and image evaluations were performed by an oral and maxillofacial radiologist and head and neck anatomist with more than ten years of experience in the area of head and neck imaging. The level of intra- and inter-examiner agreement was evaluated.
Radiological evaluation and measurements
All patients’ records were obtained with New Tom 5G (QR Verona) dental volumetric systems, operating as follows, rotation 360°, a field of view (FOV) 15 cm × 12 cm, 18-s scan time and 3.6-s exposure time, 110 V kVp tube voltage, 1–11 mA and voxel size 0.2 µm. Quantitative radiology-NNT software program version 2.21 was used to evaluate the posterior wall of the nasopharynx of all images.
ET orifice, RF, posterior nasal spine (PNS), basion (Ba), and PB are shown in the CBCT axial section presented in Figure 1. For measurement, the axial image where Ba (midline point of the anterior margin of the foramen magnum) and PNS (most posterior point of the bony hard palate on the mid-sagittal plane) are seen in the same frame is selected.

(a) Stars: Rosenmuller Fossa, White Arrows: Eustachian Tube orifice, Black Arrow: basion, Arrow Head: Posterior Nasal Spine. (b) Star: Pharyngeal Bursa.
Statistical analysis
Normality was assessed for all continuous variables using the Shapiro–Wilk test, and non-normally distributed data were transformed using the natural log (Ln) value where relevant (Eustachian-right (LN), Eustachian-left (LN)). Multivariate analysis of variance (MANOVA) was used to evaluate the relationship between groups and measurements. Pearson Chi-squared test was used to assess the relationship between CL/P groups and the presence of bursa pharyngea.
Results
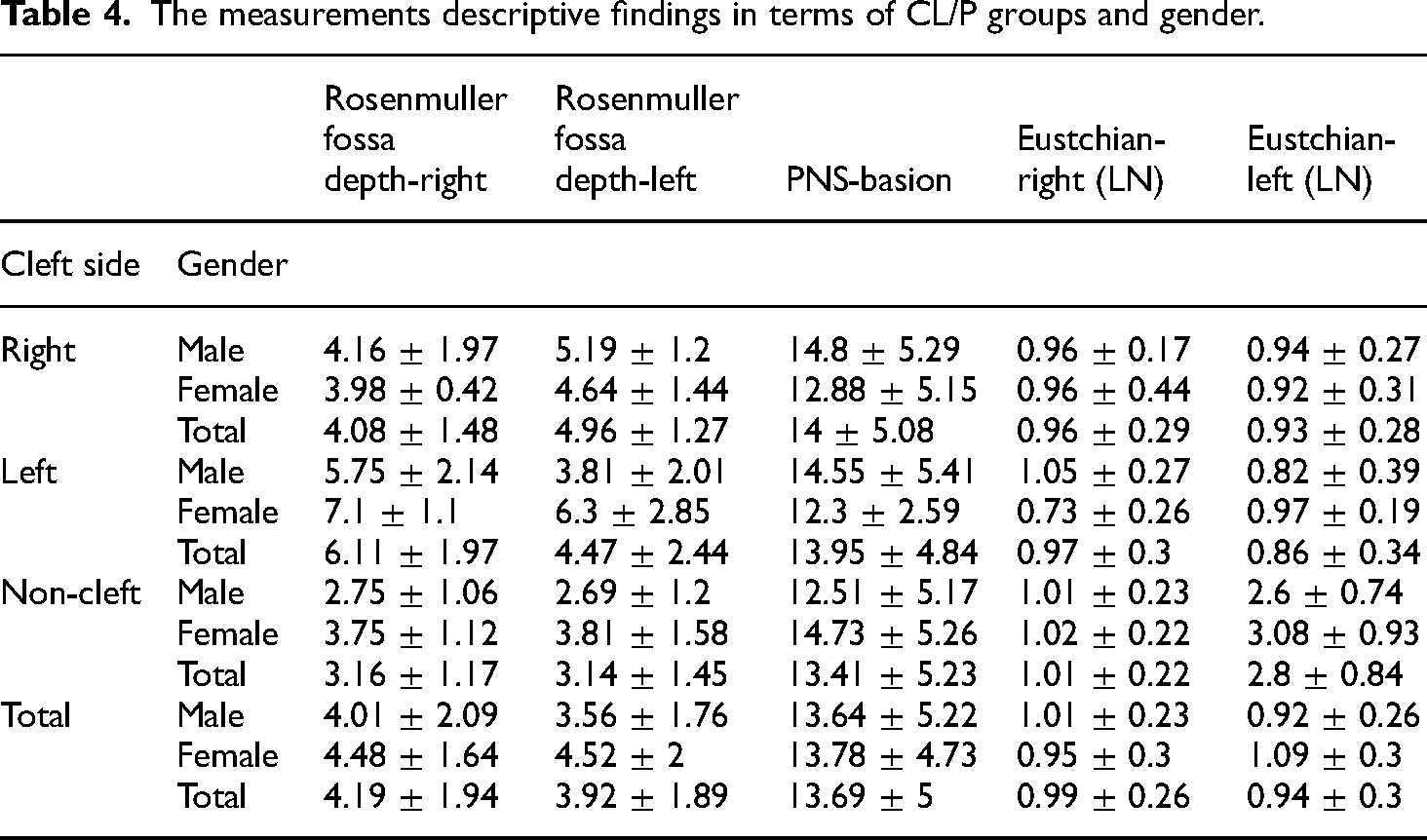
Sample size calculation was performed with G*Power 3.1.9.2 software with 0.424 effect size, at 5% significance level, power of 0.86. 11 This yielded total 54 individuals divided between the CL/P groups and control groups. The main effect of the CL/P groups was found to be effective on Rosenmuller fossa depth-right (p < 0.001) and Rosenmuller fossa depth-left (p < 0.001). The interaction effect of gender and CL/P groups was not effective on measurements (Table 1). Rosenmuller fossa depth-right was found as 3.16 ± 1.17 in non-cleft and 5.21 ± 2.02 in CL/P patients. Rosenmuller fossa depth-left was found as 3.14 ± 1.45 and 4.69 ± 1.99 in CL/P patients. The measurements descriptive findings in terms of CL/P groups and gender were summarized in Table 2. The cleft-side main effect was found to be effective on Rosenmuller fossa depth-left (p < 0.001) and Rosenmuller fossa depth-right (p = 0.0002). Gender main effect was found to be no effect on measurements. The interaction effect of gender and cleft side was not effective on measurements (Table 3). Rosenmuller fossa depth-right was found as 3.16 ± 1.17 in non-cleft, 4.08 ± 1.48 in cleft side-right patients and 6.11 ± 1.97 in cleft side-left patients. Rosenmuller fossa depth-left was found as 3.14 ± 1.45 in non-cleft, 4.96 ± 1.27 in cleft side-right patients and 4.47 ± 2.44 in cleft side-left patients. The measurements descriptive findings in terms of cleft side and gender were summarized in Table 4. There was no statistically significant relationship between CL/P groups and the presence of bursa pharyngea (p = 0.398). The findings of bursa pharyngea in terms of CL/P groups were summarized in Table 5.
The statistical findings of relationship between CL/P groups and measurements using multivariate analysis of variance (MANOVA).
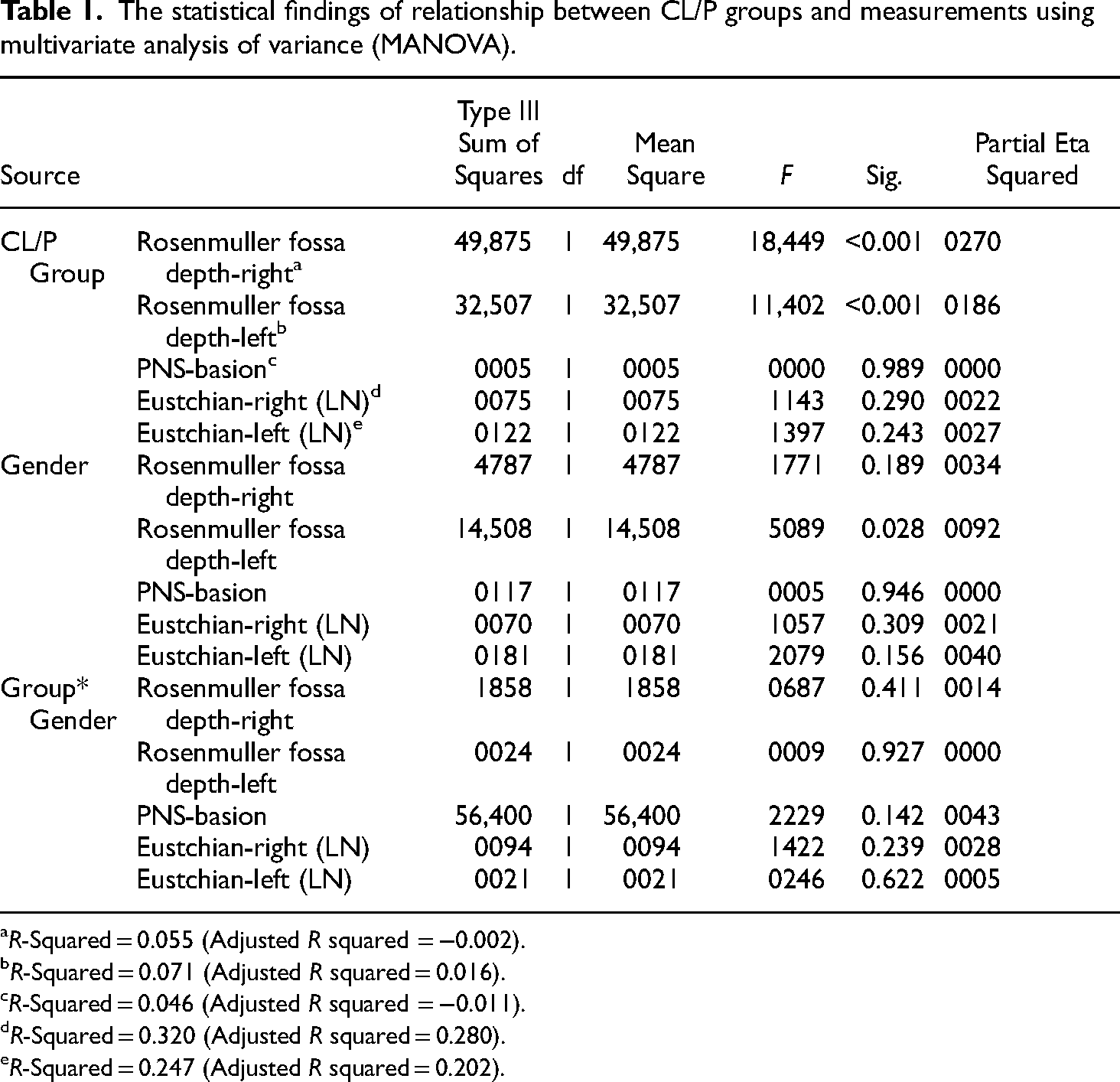
R-Squared = 0.055 (Adjusted R squared = −0.002).
R-Squared = 0.071 (Adjusted R squared = 0.016).
R-Squared = 0.046 (Adjusted R squared = −0.011).
R-Squared = 0.320 (Adjusted R squared = 0.280).
R-Squared = 0.247 (Adjusted R squared = 0.202).
The measurements descriptive findings in terms of CL/P groups and gender.

The statistical findings of relationship between cleft side and measurements using multivariate analysis of variance (MANOVA).

R-Squared = 0.098 (Adjusted R squared = 0.004).
R-Squared = 0.084 (Adjusted R squared =−0.011).
R-Squared = 0.047 (Adjusted R squared =−0.052).
R-Squared = 0.484 (Adjusted R squared = 0.430).
R-Squared = 0.322 (Adjusted R squared = 0.252).
The measurements descriptive findings in terms of CL/P groups and gender.
The relationship between CL/P groups and presence of bursa pharyngea.

Discussion
In recent years, our understanding of the genetic foundation of human disease and its impact on embryologic development has substantially advanced. A combination of poor migration and inadequate development of facial mesenchyma is thought to cause disorders of the first and second branchial arch. Because many head and neck structures migrate throughout fetal development, understanding embryologic development aids in determining the origin and nature of congenital abnormalities. A better knowledge of the pathophysiologic nature of craniofacial disorders is gained by familiarity with craniofacial embryology and its implications on the resulting anatomy. The first and second branchial arch syndromes are characterized by hypoplasia and aplasia of the components that make up these arches. Since the CL/P and the Eustachian tube are both derived from the same (first) sac (pouch), it could be to responsible for the alteration in morphology of the anatomy in the nasopharyngeal area. 12 Cleft lip-palate deformity is a problem that can cause insufficiency in the midface and velopharyngeal region in all three dimensions. Three-dimensional evaluation of these patients before surgical reconstruction is usually done with CBCT images. In one study, it was reported that the incidental findings discovered in CBCT scans of CL/P patients were three times more than the healthy group. 13 For this reason, when examining the radiological images of CL/P patients, not only the cleft line, but also every anatomical region within the imaging field should be interpreted carefully and comprehensively against the possibility of variability.
We have not encountered a study comparing the RF of children with CL/P and non-cleft children to our best knowledge. Looking at the results of this present study, RF depth was significantly deep in children with CL/P. Given the finding, it can be said that NPC diagnosis in RF location may be overlooked in CL/P patients. Increased RF depth may cause the NPC to hide in this fossa, and the NPC may not be detectable until it reaches considerable size. 14 Because of the irregular shape of the NPC, it is recommended to be examined from different sections in radiological examinations. 15 Hoe et al., 16 in a study of CT images of patients with biopsy-proven NPC, observed that asymmetry of the mucosal airway contour with RF blunting associated with infiltration of the musculus levator palatini. The similarity of NPC and temporomandibular dysfunction (TMD) symptoms such as trismus, headache, facial and ear pain is an essential issue that oral radiologists should consider. While 36% of NPC patients have trismus as the first symptom, 17 in another study, trismus was observed in 9% of NPC patients. 18 Other pathologies may develop in RF other than NPC. A case report of RF rinolith presented by Shilston et al. 19 with CT, RF based a lipoma case introduced by Kalan et al. 20 Also, a case report in the literature figures out the removal of bullets from RF. 21
Even though nasotracheal intubation is necessary procedure, especially if working in the dental area, it could be a traumatic procedure such as epistaxis. Due to the left face slope of the tube facing away from the turbinates, thus crossing the vocal cords more efficiently, the general view is that nasotracheal intubation through the right nostril is safer than the one through the left nostril. 22 Takasugi et al. 23 have studied that whether PR variations are effective in nasotracheal intubation in patients using multiplanar CT. Researchers have argued that during the nasotracheal intubation procedure, the tip of the nasotracheal tube may become trapped in the RF and cause unsuccessful nasotracheal intubation. They also stated that the tube tip might cause nasopharyngeal laceration and nasopharyngeal dissection during this procedure due to hitting the recess strongly. 23 Increasing RF depth may increase the difficulty of nasotracheal intubation, as demonstrated in CL/P patients in this study. ET morphology is one of the critical anatomical structures that can change in CL/P patients. 11 Because E/T dysfunction is connected to many problems such as chronic otitis media, 24 health E/T is considerably necessary for seamless hearing. Patients with CL/P often have ET problems because the levator veli palatini and tensor veli palatini muscles may not function normally. In addition to these, ETs of CL/P patients invite middle ear diseases, depicted as horizontal, short, and floppy. 25 In this study, only the opening of ET to the posterior nasopharyngeal region was measured, and no statistical difference was found. PB, which may host a Tornwaldt cyst, may develop in the posterior wall of the nasopharynx, which consists of loose connective tissue. Gallagher et al. 26 reported that their blind nasotracheal intubation attempt failed due to the presence of PB.
This study contains some limitations. First, although we obtained all patients in the same CBCT taken procedures because the recess walls can adhere to each other in the supine position, it has been suggested that PR can be hidden. 27 They claim that gravity can change oropharyngeal structures, especially in postural changes such as upright and supine positions. However, this study aimed to compare the morphological features of the nasopharyngeal regions in patients with CL/P and non-cleft, and since the images of the two groups included were obtained under the same procedures, it is thought that this situation did not adversely affect the results of the study. Secondly, we conducted the study with a limited population due to the insufficient number of unilateral CL/P patients.
Conclusion
Because RF is the most frequent site for NPC, it is crucial to have a thorough understanding of nasopharyngeal anatomy. In CL/P patients, RF depth may increase, and this should be considered while evaluating disorders in this region.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was obtained from ERC (Ethical Review Committee) (Approval/2021/2772).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Mustafa Temiz holds a PhD in oral and maxillofacial surgery. His interests are orthognathic surgery and cleft lip and palate patients.
Suayip Burak Duman holds the title of associate professor in oral and maxillofacial. His interests are CBCT and artificial intelligence.
Ahmed Z. Abdelkarim holds a PhD in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.
Ibrahim Sevki Bayrakdar holds the title of associate professor in oral and maxillofacial. His interests are CBCT and artificial intelligence.
Ali Z. Syed holds a M.S in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.
Gozde Eser is research assistant in the field of oral and maxillofacial radiology. Her interests are CBCT and artificial intelligence.
Duygu Celik Ozen is research assistant in the field of oral and maxillofacial radiology. Her interests are CBCT and artificial intelligence.
Hatice Tugce Gedik holds a PhD in Anatomy. Her interests are dental anatomy and variations.
Mehmet Ugurlu has a specialist title in orthodontics. His interests are orthognathic disorders and craniofacial development.
Rohan Jagtap holds a PhD in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.