
Abstract
Objectives:
This study aimed to determine mastoid emissary canal’s (MEC) and mastoid foramen (MF) prevalence and morphometric characteristics on cone-beam computed tomography (CBCT) images to underline its clinical significance and discuss its surgical consequences.
Methods:
In the retrospective analysis, two oral and maxillofacial radiologists analyzed the CBCT images of 135 patients (270 sides). The biggest MF and MEC were measured in the images evaluated in MultiPlanar Reconstruction (MPR) views. The MF and MEC mean diameters were calculated. The mastoid foramina number was recorded. The prevalence of MF was studied according to gender and side of the patient.
Results:
The overall prevalence of MEC and MF was 119 (88.1%). The prevalence of MEC and MF is 55.5% in females and 44.5% in males. MEC and MF were identified as bilateral in 80 patients (67.20%) and unilateral in 39 patients (32.80%). The mean diameter of MF was 2.4 ± 0.9 mm. The mean height of MF was 2.3 ± 0.9. The mean diameter of the MEC was 2.1 ± 0.8, and the mean height of the MEC was 2.1 ± 0.8. There is a statistical difference between the genders (p = 0.043) in foramen diameter. Males had a significantly larger mean diameter of MF in comparison to females.
Conclusion:
MEC and MF must be evaluated thoroughly if the surgery is contemplated. Radiologists and surgeons should be aware of mastoid emissary canal morphology, variations, clinical relevance, and surgical consequences while operating in the suboccipital and mastoid areas to avoid unexpected and catastrophic complications. CBCT may be a reliable imaging diagnostic technique.
Keywords
Introduction
The cranial emissary veins (CEVs) are venous structures that link the intracranial and extracranial venous systems in the posterior cranial fossa.1,2 The emissary veins (EV) are located in the posterior cranial fossa, pass through the emissary ducts, and provide venous drainage through the dural venous sinuses. 3 Mastoid emissary canals are small, slender channels connecting the temporal bone's mastoid air cells to the external environment. They typically measure between 0.5 and 1 cm in length and are composed of a thin bony wall with a lumen that is lined with mucosal tissue. The canals run in a curved path, typically lateral and posterior, and terminate with a small opening on the posterior surface of the mastoid process.2,3 Some of these veins show many variations within the skull and have their foramen, while others connect the extracranial vessels and intracranial vessels through different canals. In the embryological period, these canals developed from the budding of the dural venous sinus. 4 The vena emissaries do not have a valve; the vessels’ blood flow is two-way. In this way, cold blood coming from the surface of the skull plays a balancing role in the temperature of intracranial venous blood. 5 They can also cause infection or transport tumor cells into the skull. These veins are also used for balancing intracranial pressure. When the internal jugular vein is blocked or restricted in patients with head or neck lesions, these vessels act as safety valves and play an essential role in venous drainage. 6 EVs and their canals have great surgical importance. In retro-sigmoid interventions performed in the posterior cranial fossa, emitting vessels may cause bleeding or embolism if the vessels or the associated sinuses are ruptured. Postoperatively, bleeding from the EV can cause epidural hematoma formation. Emissary vessels can also access intracranial dural venous sinuses with endovascular applications. 3
The mastoid emissary veins (MEV) join the suboccipital venous plexus, connecting the sigmoid sinus to the occipital or posterior auricular veins. 7 These veins emerge from the mastoid foramen around the occipitomastoid suture, passing through small canals at the posterior border of the temporal bone (mastoid section) called the mastoid emissary canal (MEC).7,8 Knowing the location and variations of the mastoid foramen, and reducing the risk of complications during surgical procedures in that area is critical.
Yurdabakan et al. conducted research to examine the morphometric analysis of mastoid foramen and mastoid emissary canal on cone-beam computed tomography (CBCT) in their study out of 472 patients. MF was present in 82% and absent bilaterally in 18% of the 472 patients. The prevalence of MF was 67.8% on the right side and 65.7% on the left. 9 This study suggests that CBCT provides three-dimensional images of the bony structures of the craniofacial region with a lower radiation dose, shorter time, and reduced costs compared to multi-detector computed tomography. 10
Aim
The present study aimed to evaluate the morphological and morphometric characteristics of mastoid emissary canals in patients using CBCT.
Materials and methods
Inonu University Non-Interventional Clinical Research Ethics Board (decision number: 2020/696) authorized the study protocol. Cone Beam Computed Tomography (CBCT) images from 135 patients were evaluated by two oral and maxillofacial radiologists (with 5 and 15 years of experience) with a common decision. The 3-dimensional volume-rendered (3DVR) images were used to define the mastoid foramen (MF). (Figures 1 and 2). The mean diameters of MF and MEC were measured. The total number of mastoid foramina was counted (Figure 3). We excluded patients with previous mastoid, skull base, posterior fossa surgery, dural sinus thrombosis, or vascular malformations. Patients with poor technique or motion artifacts, and whose anatomy could not be adequately assessed were excluded. We also excluded patients younger than five, since the JB may not be developed entirely. Consequently, thirty-one patients were excluded, and 119 patients were included in the study. All CBCT examinations were obtained using a NewTom 5G (QR Verona/Italy) dental volumetric system with a standard protocol without contrast administration. The scanning parameters included: rotation 360°, a field of view (FOV) 15X12 cm, 18-s scan time and 3.6-s exposure time, 110 V kVp tube voltage, 1-11 mA, and voxel size 0.3 µm. Patients were scanned in the caudal to cranial direction with a scan revolution time. Tube current was regulated by an automatic exposure control system. Images were reconstructed in axial, coronal, and sagittal planes with a slice thickness of 1 mm. The images were transmitted to the picture archiving and communication systems (PACS). Using 3-dimensional volume rendering images, mastoid foramen (MF) was detected. The assessment of the MF and MEC height was measured in the coronal plane. The biggest MF and mastoid emissary canal (MEC) were measured in axial, sagittal and coronal slices of the CBCT. The MF and MEC mean diameters were calculated. The mastoid foramen numbers were recorded. The prevalence of MF was studied according to gender and side of the patient.

Representative CBCT images used for the measurement of mastoid foramen height (a) and diameter (b).

Representative CBCT images used for the measurement of mastoid emissary canal height (a) and diameter (b).

3D CBCT images with the mastoid foramen indicated by the arrowhead and the accessory mastoid canal indicated by the arrow.
Examiner calibration
Intraclass correlation coefficients were used to evaluate of examiner agreement. The results were 0.974 (0.935-0.990) for foramen diameter, 0.985 (0962-0.964) for foramen height, 0.988 (0.971-0.995) for canal diameter and 0.985 (0.962-0.994) for canal height.
Statistical analysis
Statistical analyses were performed using SPSS v.25.0 (SPSS Inc.). In statistical analysis, Kolmogorov-Smirnova test was used to evaluate the normality of the data distribution. Frequency analysis, Pearson chi-square, Mann-Whitney U test, and Spearman correlation test were used for the data evaluation.
Results
A total of 199 sides from 135 patients were evaluated in our study. MF and MEC were detected in 119 (88.1%) patients. Out of 119 patients, 66 were females, and 53 were males between 18 and 81 years old. The mean age was 36,5 ± 14,2 years in females and 37,7 ± 16,9 years in males. No significant difference in the presence of mastoid emissary canal was found between males and females (p = 0.233) (Table 1). Of the patients with MF and MEC, 80 (67.20%) were bilateral, and 39 (32.80%) were unilateral (Table 2). There was a statistically significant difference when comparing the unilateral-bilateral situation in the patient with the presence of MEC (p < 0.001). There was no significant difference between the numbers of patients with the presence of mastoid emissary canal males and females in both the unilateral patient group and the bilateral patient group (p > 0.05) (Table 3). The mean diameter of MF was 2.4 ± 0.9 mm. According to gender, there is a statistical difference between the two groups for the diameter of MF (p = 0.043). The features of the MF and MEC are summarized in Table 4. Age and MEC diameter did not show any significant correlation. There is a positive correlation between age and foramen diameter (Table 5). Accessory Mastoid Canal frequency was found as 97 (48.7%) single and 26 (13.1%) multiple in 199 temporal bones (Table 6).
Comparison of mastoid emissary canal presence between male and female patients, analyzed by Chi-square test (p = 0.233), indicating no significant difference in canal prevalence between the two genders.

The frequency and distribution of MEC in the unilateral group.

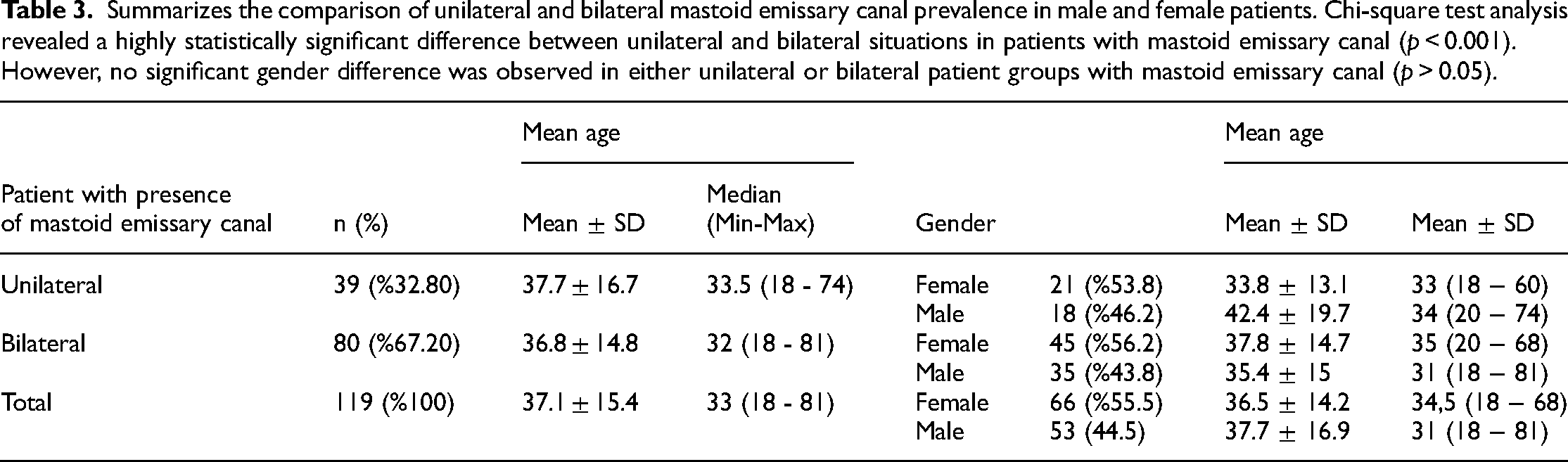
Summarizes the comparison of unilateral and bilateral mastoid emissary canal prevalence in male and female patients. Chi-square test analysis revealed a highly statistically significant difference between unilateral and bilateral situations in patients with mastoid emissary canal (p < 0.001). However, no significant gender difference was observed in either unilateral or bilateral patient groups with mastoid emissary canal (p > 0.05).
Presents information about the features of the mastoid emissary canal in the temporal bone and how they are utilized to determine the presence of the canal (n = 199 sides). The table summarizes the characteristics of the canal and provides details on how they were measured and analyzed in the study.

* There is a statistical difference between the two groups (p = 0.043), Mann-Whitney U test.
Displays the results of a Spearman correlation test measuring the relationship between age and foramen diameter. The test showed a positive correlation between these variables, indicating that as age increases, the foramen diameter tends to increase as well.

The frequency and distribution of accessory mastoid canal.

Discussion
The venous drainage of the brain is divided into three central systems: superficial, middle, and deep. 5 In this system, the anastomoses between the superficial and middle layers commonly represent the emissary veins. 11 Emissary veins have a limited role when the venous drainage of the brain is normal. These veins may be the primary outlet in high-flow vascular malformation, intracranial hypertension, hypoplasia, or aplasia of the internal jugular veins. 12 The mastoid emissary vein passes through the mastoid foramen. It connects the intracranial sinuses to the extracranial venous system, creating a risk of infectious spread from the extracranial to the intracranial areas. 3
Variations of the foramen in the cranium are crucial in maxillofacial surgery, neurosurgery, otolaryngology, and neurology. 13 Knowing the variations of the foramen will eliminate iatrogenic errors by the operators. Bleeding due to emissary vein injury may occur during operations in the posterior cranial fossa, resulting in epidural and subdural hematoma. 14 Surgical interventions in this area may lead to venous infarction or sigmoid sinus thrombosis. Hemostatic agents such as bone wax are reported to be applied to control bleeding in this area.15,16 The connection of the mastoid emissary vein with the sigmoid sinus and its bilateral flow may cause embolism or thrombus. 13 There are also reports of thromboembolism moving retrograde into the sigmoid sinus due to middle ear surgery or infective mastoiditis surgery. 17 In addition, there are studies in which embolization and dilatation in the mastoid emissary vein were associated with tinnitus.18,19
The number of mastoid foramina through which the mastoid emissary vein passes varies between 0 and 4, and their diameters vary in line with the size of the vessels passing through.13,20 In their research on CT angiograms, Pekcevik et al. found the prevalence of the mastoid emissary vein to be 49.4% bilaterally and 28.3% unilaterally, but they did not discuss the canals in hard tissues such as bones. 3 In their examination of 106 skulls, Kim et al. found the mean diameter of the mastoid foramen to be 1.64 mm. 20 In the same study, the average diameters of the right and left mastoid foramen were different, with the largest mastoid foramen diameter being 7 mm. Louis et al. analyzed the mastoid emissary foramen on 200 samples. They found the prevalence of the foramen to be 98% on the right side and 72% on the left side, and the mean mastoid emissary vein diameter to be 3.5 mm (1.1–5.6 mm). 5 In our study, the incidence of unilateral mastoid foramen on the right side (74.4%) was higher than on the left side (25.6%).
Murlimanju et al. 13 examined 96 temporal bones of 48 cadaver skulls to analyze the mastoid foramen's prevalence, morphology, and number. Mastoid foramen was seen in 91.7% of the 96 temporal bones examined; one mastoid foramen was observed in 62.5%, two mastoid foramina in 22.9%, and three mastoid foramina were observed in 6.2%. In addition, they found that their findings were similar to the results of previous studies and concluded that the incidence of mastoid emissary veins did not show a significant difference among different races. Comparing the prevalence of the mastoid foramen in men and women, Peira et al. 21 observed the mastoid foramen on the right side in 72.7% of female skulls, on the left side in 81.8%, on the right side in 90% of male skulls, and on the left side in 85%. Demirpolat et al. 12 analyzed the prevalence and diameters of the mastoid foramen and mastoid emissary canal with three-dimensional images obtained by multi-detector computed tomography from 248 patients. The study found the prevalence of mastoid emissary canal to be 91.5% in women, 93.3% in men, 84.7% on the right side, and 82.3% on the left side in unilateral cases. Similarly, in this study, the prevalence of the mastoid emissary canal was examined based on gender and the side. The diameters of the mastoid foramen and mastoid emissary canal were measured. However, three-dimensional images were obtained in a shorter time and with a lower radiation dose using cone-beam computed tomography instead of multi-detector computed tomography.
Conclusion
MEC and MF are anatomical structures that surgeons should not ignore. It is essential to analyze these anatomical structures systematically before the surgical intervention as they cannot be defined anatomically and may cause surgical complications. In CBCT scans, not knowing the MF and MEC variations may wrongly suggest a pathological condition, leading to misdiagnosis and unnecessary procedures. Detection of the MEC on CBCT images can show the topography of the emissary veins and help radiologists and surgeons understand the course of the emissary vein.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was obtained from ERC (ethical review committee) (Approval/2020/696).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Mustafa Temiz holds a PhD in oral and maxillofacial surgery. His interests are orthognathic surgery and cleft lip and palate patients.
Duygu Celik Ozen is research assistant in the field of oral and maxillofacial radiology. Her interests are CBCT and artificial intelligence.
Suayip Burak Duman holds the title of associate professor in oral and maxillofacial radiology. His interests are CBCT and artificial intelligence.
Ibrahim Sevki Bayrakdar holds the title of associate professor in oral and maxillofacial radiology. His interests are CBCT and artificial intelligence.
Orhan Kazan has a specialist title in oral and maxillofacial surgery. His interests are orthognathic surgery and artificial intelligence
Rohan Jagtap holds a PhD in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.
Oguzhan Altun holds the title of associate professor in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.
Ahmed Z. Abdelkarim holds a PhD in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.
Ali Z. Syed holds a M.S in oral and maxillofacial radiology. His interests are CBCT and craniofacial disorders.
Kaan Orhan holds the title of Full Professor in oral and maxillofacial radiology. His interests are CBCT, digital dentistry, craniofacial disorders and artificial intelligence.