
Abstract
Overweight and obesity have become a significant health hazard among adolescents on account of quick growth in its occurrence rate and its common comorbidities like cardiometabolic disease (CMD). The aim of this study was to evaluate the prevalence of adiposity and assess the risk of CMD among university students in Eastern Province, Saudi Arabia. A cross-sectional study was conducted during the academic year 2017–2018, in a sample of 310 subjects (127 males; 183 females). The measurements were taken using standardized instruments including Body Mass Index (BMI), Fat Mass Index (FMI), Body Fat Percentage BFP), Mass of Body Fat (MBF), Visceral Fat Area (VFA), Waist Circumference (WC), and Waist to Hip Ratio (WHR). Moreover, CMD risk indicators were calculated by Conicity index (C index), WC, and WHR. The findings showed that the majority was overweight and obese (16.8% and 21.6%, respectively). While evaluating obesity indicators, males were found to have higher adiposity (obese students 34.6%) compared to female students (12.6%; p < 0.001). Additionally, FMI showed that the mean was significantly higher among males (8.65 ± 6.06) compared to females (7.26 ± 3.30; p < 0.019). Analysis of the predictors’ indices for cardiometabolic risk score highlighted a significantly higher percentage of WC, WHR, and C index among male students (50, 38.5, 59) compared to females (16.9, 14.2, 34; p < 0.001). Significant positive correlations were observed between C index quartiles and BMI with the other cardiometabolic indices (p < 0.001). This study highlighted a high prevalence of adiposity and CMD risk among university students. The prediction of CMD in early age is quite helpful in preventing adiposity related health issues. Decision makers need to spread awareness about healthy consumption as well as the relationship between physical inactivity and chronic diseases.
Introduction
Overweight and obesity are defined by the World Health Organization (WHO) as irregular or excessive fat build-up that could negatively affect health. 1
It was reported in several studies that accumulation of body fat increased morbidity and mortality related to cardiometabolic diseases (CMD),2,3 resulting in an increased risk of diabetes type 2, stroke, cardiovascular diseases,3,4 and hypertension. 5 Besides, increasing body fat percentage (BFP) became a critical health problem and a cause of concern globally. 6
Several socio-cultural changes have been documented among residents of the Gulf region. These changes were expected to affect the lifestyle of people and were linked to warning health outcomes because of the occurrence of both overweight and obesity in the region. 7
CMDs are a major public health concern due to their high prevalence locally as well as globally. There are several scoring systems available to predict the risk of developing CMD. The measurement of the anthropometric indices is the most useful and appropriate method to discriminate between low and high risk patients who require intensive control. 8
Anthropometric measurements are important tools to evaluate the tendency for the young to become overweight and/or obese as well as the tendency to develop poor lipo-metabolic profile. 9
The Conicity Index (C index) is another type of measurement of central obesity and is based on the hypothesis that the accumulated abdominal fat has a silhouette like a double cone “two cones sharing the same base, one positioned over the other” whereas participants with less visceral fat have the shape of a cylinder. Therefore, C index ranges from 1.73 (a perfect double cone) to 1.0 (a perfect cylinder). 10 As cited in the literature, C index is strongly associated with CMD as compared to other anthropometric indicators 11 and incorporates three measures namely height, weight and waist circumferences (WC). 12 Moreover, it was reported that C index and Waist to Hip Ratio (WHR) were good discriminators for CMD events as compared to the other obesity indices.13,14
The prevalence of CMD depends on many factors such as population characteristics (age, sex, and ethnicity), lifestyle and, geographic location. However, there is no data availability about the prevalence of CMD in Saudi academia. Recent studies on the clustering of the individual components within particular combined age, adiposity, anthropometric measurements, sex and CMD risk assessment in young Saudi population are limited. Therefore, this study aimed to determine the prevalence of adiposity as well as assess the risk of CMD on the basis of gender among university students in Eastern Province, Saudi Arabia.
Materials and methods
A cross-sectional study was conducted in the city of Dammam (Eastern Province, KSA), enrolling undergraduate students studying in preparatory year who were attending Imam Abdulrahman Bin Faisal University (IAU) during the academic year 2017/2018. Such students constituted the study population. All the students were asked to participate in the study. The participation was of voluntary nature. The students were notified by emails and WhatsApp messages. The students were informed about the study protocol and the methods of assessments before enrollment in the study. Data for each student were collected during official working hours by three trained researchers.
The sample size was calculated using Raosoft software. The total number of preparatory year students is around 3900 students. The female students constitute two-thirds of students (n < 2600) whereas males constitute the remaining one third (n < 1300) of the preparatory year students. The sample size was calculated using a 5% margin of error and a confidence level of 95%. With an expected response rate of 50% based on a pilot study, the calculated sample size was 351. Therefore, 351 participants were enrolled to participate in the study.
Lactating and/or pregnant women and those individuals with chronic diseases or any other disabilities that might have affected their anthropometric measures were recognized during screening and exempted from the participation. The study was approved by the Ethics Committee of IAU, Institutional Review Board (IRB number: IRB-2018-19-112) and written consent was obtained from each participant.
Measurements were taken using standardized equipment. Participants were asked to wear light clothing and remove their shoes before taking their measurements. The height of students was documented to the nearby 0.1 cm, and weight was calculated to the nearby 0.1 kg (Seca 704; Seca, Hamburg, Germany). 7 The participants were instructed to fast for 4-h before body composition measurement.
The assessment of body composition was according to the manufacturer’s protocol of the Bioelectrical impedance analysis (BIA) (IOI 353, Jawon Medical, S. Korea). BIA device measured body segments through tetra-polar electrode method using 8 touch electrodes. The following parameters were determined: Body Mass Index (BMI), Body Fat Percentage (BFP), Mass of Body Fat (MBF) and Visceral Fat Area (VFA). Body composition was evaluated at normal body hydration in similar external temperature (22–24°C). 15 Subsequently, the subject’s hands and feet were cleaned using soap and water, then further dried, and cleaned with alcohol before electrodes were placed on the skin surface. The technique utilized bioelectrical impedance which presents a high correlation (R < 0.88) with dual X-ray absorptiometry. 16
According to both the National Institutes of Health (NIH) and WHO international classification, adults were classified based on their body mass index (BMI) to underweight (BMI < 18.5), normal (BMI = 18.5–24.9), overweight (BMI = 25–29.9), or obese (BMI ≥ 30).1,17–19 Furthermore, obesity is subdivided into three grades: Grade 1 (BMI = 30–34.9), Grade 2 (BMI = 35–39.9) and Grade 3 or extreme obesity (BMI ≥ 40). 19
Taking into consideration age and gender, the participants were classified as having low body fat percentage (BFP < 8), normal (BFP = 8–19.9), high (BFP = 20–24.9), or very high (BFP ≥ 25) body fat. 20
FMI was considered as fat mass (kg) ÷ height (m2). 21 Using FMI developed from the National Health and Nutrition Examination Survey, the participants were classified into categories of fat deficit, normal, excess fat, obese I and obese II–III using FMI cut offs of <3, 3–6, 6–9, 9–12 and <12 for males and <5, 5–9, 9–13, 13–17 and <17 for females. 22
Other anthropometric indices, such as WC as well as WHR, are two of the most commonly used non-invasive biomarkers in predicting cardiometabolic risk factors, “WC was measured with measuring tape (Gay Mill, WI) to the nearest centimeter (cm) midway between the inferior angle of the ribs and the suprailiac crest. Hip circumference was measured as the maximal circumference over the buttocks in cm. 23
According to the WHO, the recommended WC and WHR cut-off points for increased cardiometabolic risk in women is (<88 cm, ≥0.85) and (<94 cm, ≥0.90) in men. 24
For the calculation of the C index, “the measurements of weight, height, and WC were used” by means of the following mathematical equation 25 :

A score of ≥1.18 for women and ≥1.25 for men indicates a risk. 26 Furthermore, we categorized C index (CIC) into four quartiles [first Q <1.28, second Q 1.28–<1.34, third Q 1.34–<1.38, and fourth Q ⩾1.38 ] 27 for the comparison between the groups.
Statistical analysis
Data were analyzed using SPSS for Windows (version 25, SPSS, Inc., Chicago, IL, USA). The normality distribution was assessed using the Shapiro-Wilk test. The data were then categorized to compare gender differences in terms of the prevalence of obesity, overweight, excess fats and other categorical data using chi-square test. Student t-test was used to investigate gender differences in the continuous data for all variables and the mean ± SD were reported for each group associated with their p-value of the comparison results. In both cases, p-values below 0.05 were used as an indicator for statistical significance.
Results
Out of the total calculated sample size, 88% of the students only accepted to participate in the study. Therefore, the sample comprised of 310 subjects, selected by a convenience sampling method. Female (n = 183) students had greater representation as they comprised of 60% of the study population, whereas male (n = 127) students represented 40% of the sample. This was concordant with the gender proportions among the whole preparatory year students in the university. Male students had a slightly higher mean (18.57 ± 0.85) compared to female students (18.38 ± 0.76) in regard to age. The age of students ranged from 16 to 23 years (Table 1).
General characteristics of participants.
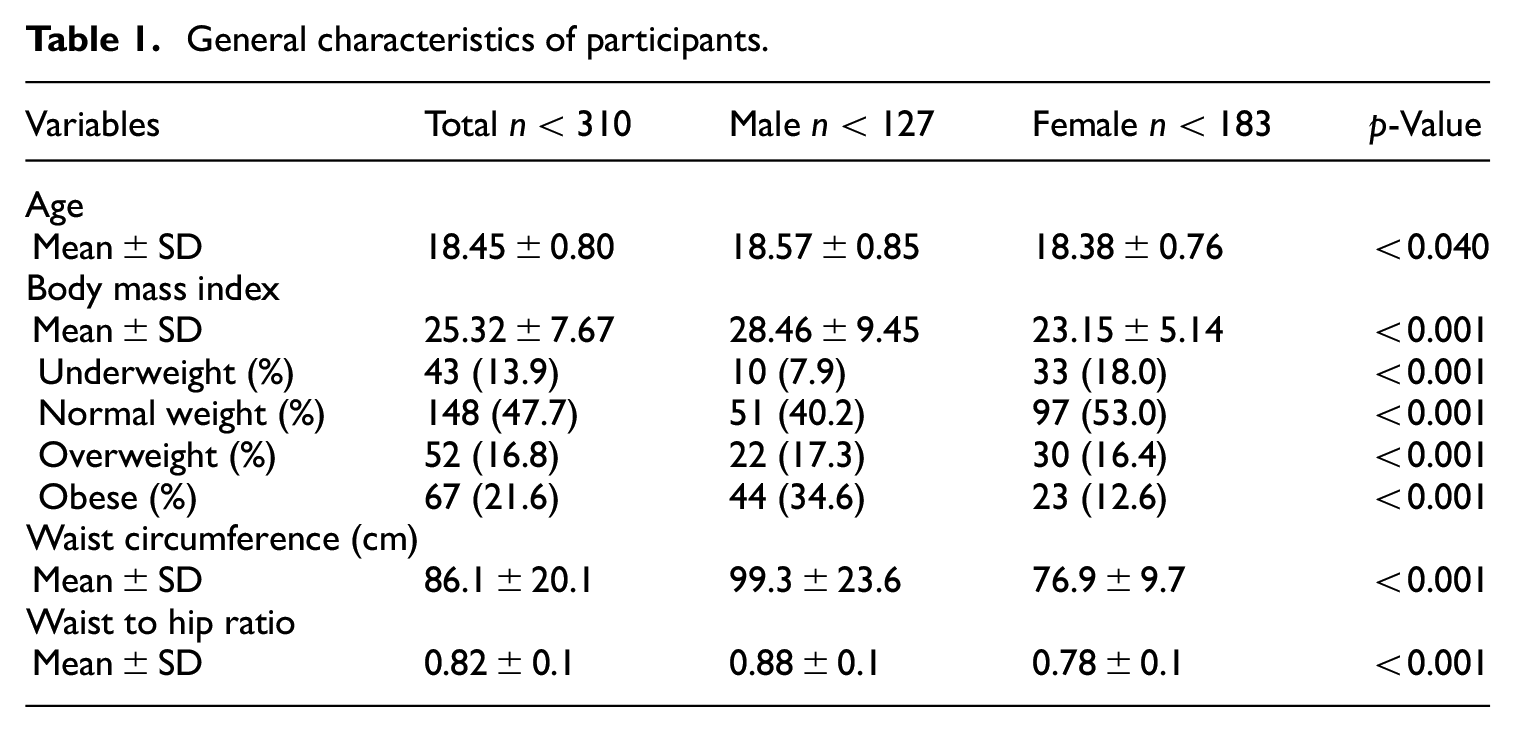
The study results revealed that mean BMI was above 25 among all study participants (25.32 ± 7.67). Among them, more than one-third of students were overweight and obese (16.8% and 21.6%, respectively). However, it was significantly higher among male students (28.46 ± 9.45) compared to females (23.15 ± 5.14; p < 0.001). Data showed male participants had a significantly higher proportion of obese students (34.6%) compared to female students (12.6%; p < 0.001). Similarly, the percentage of overweight males (17.3%) was slightly higher than that of female students (16.4%; p < 0.001). The study profile was also consistent with the results of the WC where males had also a higher mean (99.31 ± 23.61) compared to female students (76.91 ± 9.74; p < 0.000). This was also reflected in the higher mean WHR among male students (0.88 ± 0.12) compared to females (0.78 ± 0.08; p < 0.000) as shown in Table 1.
Comparison of FMI highlighted that, the mean was statistically higher among males (8.65 ± 6.06) compared to females (7.26 ± 3.30; p < 0.019). In contrast, BFP data presented a different tendency, where female students had significantly higher mean of BFP (29.91 ± 6.88) in comparison with males (27.15 ± 10.58; p < 0.010). The MBF results were consistent with most parameters, where males scored significantly higher means (25.27 ± 17.99) compared to females (17.94 ± 8.21; p < 0.001). Similarly, VFA results indicated that males had significantly higher mean fat in the viscera (118.83 ± 81.83) when compared to their female counterparts (58.55 ± 36.25; p < 0.001) as presented in Table 2.
Differences in adiposity indicators.

The FMI data showed a similar prevalence for excess fat (14.8%) and obesity (20.7%) among the preparatory year students in general. However, statistically significant differences (p < 0.000) were also observed between male (39.2%) and female (7.8%) students in terms of obesity. Comparison of BFP data revealed a very high fat percentage (65.8%) and high fat percentage (19.4%) among all students. However, in this case female students had a significantly higher percentage of BFP (74.3%) compared to males (53.5%; p < 0.001) (Table 2).
The MBF results displayed a consistent trend with most parameters, where males scored significantly higher means (25.2 ± 17.9) compared to females (17.9 ± 8.2; p < 0.001). Similarly, VFA results indicated that males had significantly higher mean fat in the viscera (118.83 ± 81.8) when compared to their female counterparts (58.5 ± 36.2; p < 0.001). This occurrence was also consistent with the results of the WC and WHR as reported before (Table 2).
Results show that male students were positively correlated with the increased quartiles of C index at the significance level (p < 0.001) than females, which indicated the double cone shape and higher cardiometabolic risk score (Figure 1)

Pearson correlation coefficient of gender differences, according to quartiles of C Index.
As the BMI and CIC increased, the proportion of cardiometabolic risk increased significantly for both male and female students. Results show that BMI was significant and positively associated with WHR (r = 0.91; p < 0.001), WC (r = 0.71; p < 0.001), and C index (r = 0.26; p < 0.001). CIC was positively and significantly correlated with BMI (r = 0.71; p < 0.001), WHR (r = 0.75; p < 0.001), and WC (r = 0.85; p < 0.001) as presented in Table 3.
Pearson correlation coefficient of BMI and quartiles of C Index with cardiometabolic indices.

BMI: body mass index; C Index: conicity index; CIC: conicity index categories; WC: waist circumference (cm); WHR waist to hip ratio.
p < 0.001.
Analysis of the predictors’ indices for cardiometabolic risk score by gender showed a significantly higher percentage of WC (Figure 2(a)), WHR (Figure 2(b)), and C index (Figure 2(c)), among male students (50, 38.5, 59) compared to females (16.9, 14.2, 34; p < 0.001) respectively.

Cardiometabolic risk score assessments among participants. Classification according to the recommended cutoff points for increased cardiometabolic risk (female/male) WC score: (<88 cm/<94 cm); WHR score: (≥0.85/≥0.90); C index risk score: (≥1.18/≥1.25): (a) waist circumference (%), (b) waist to hip ratio (%), and (c) conicity index (%).
Discussion
This study revealed several interesting observations. The occurrence of adiposity and CMD risk indicators in males was significantly greater than females.
Higher family income could predispose a male individual to overweight and obesity. 28 Furthermore, as indicated by another study that environmental and social factors in the college of medicine appears to be a strong influential factor that force male students try to gain weight intentionally despite their medical knowledge. On the other hand, female students appear motivated to control their diet to maintain the preferred body size while utilizing their medical background. 28
However, female subjects had a significantly higher BFP than male students, that can be explained due to the physiological difference between both genders as females naturally store fat subcutaneously, and males store fat viscerally.29,30
The majority of males in this study were overweight and obese. This occurrence is also seen in other parts of the world. 31 The rates of overweight and obesity observed were alarming since they were similar to one of the highest rates in the world.32,33
A potential indicator of body adiposity that may prove to be highly useful in this research field is the FMI. 34 The baseline means FMI for our sample was (♂8.65 and ♀7.26) which are higher than the figures reported in previous studies.35,36
The results of the present study showed that 85.2% of the whole sample either had a high fat or a very high fat percentage, according to their BFP. The findings also revealed that the total body fat exceeded the proper values in male subjects (VFA ≥ 100 cm2). It has been noted that visceral fats could lead to CMD. 37 Consequently, it was stated that nutritional management would go with consistent medical follow-up to cope or reduce the risk of the aforementioned illnesses in Saudi college students with high VFL. 38
Obesity has been recognized in terms of adiposity. 39 Measuring adiposity parameters beside to BMI could help to identify people with a higher risk of CMD. 40
Central obesity indicator is a major CMD risk predictor because it is associated with diabetes type 2, metabolic syndrome and dyslipidemia which increases atherogenic risk. 41 Central obesity as indicated by C index and WC is more appropriate in predicting CMD and its components as compared to the peripheral obesity, as indicated by the BMI. However, a recent study found that both central and peripheral obesity indicators showed similar associations with CMD risk 30 and both were found significantly higher among male students. Furthermore, WC correlated strongly with C index more than WHR, suggesting that WC could be preferred over WHR for predicting central obesity and CMD risk. The use of ratios such as WHR to assess central obesity may not be appropriate because they are highly age dependent 42 and may obscure stronger relations that may be present with separate circumference measurements. 43 Additionally, differences in skeletal structure may confound the results. 44
In the present data there were apparent gender-based differences in the prevalence of CMD risk in male students. Such a difference was documented in a similar screening program done in Saudi Arabia. 45
Preparatory students start university as adolescents, while they orient themselves in new lifestyle and environmental changes, it may predispose them to obesity and CMD risk factors. This together with the impact of urbanization may add to increasing the prevalence of CMD in Saudi Arabia. 46
Many factors have been recognized in the literatures that have led to growing obesity in the Gulf region. For instance, fast food chains, ease of transportation, and increased popularity of processed food are few to name.47,48 Additional significant factors have also been noted are the extreme consumption of fatty and salty food 49 and living a sedentary lifestyle. 47 Another important factor that has been observed is the increased use of mobile technologies, TVs, and internet that are most common leisure activities among populations. 50
Many healthy individuals with abnormal adiposity profile may have variable degrees of CMD risk and according to the previous report, an early screen for young individuals could be a good predictor for various CMD. 8
The study was cross-sectional in design and thus it may not representative, and the results of present study do not correlate the data related to cardiometabolic profile and other health and lifestyle information of participants. These aspects are important and recommended to be included in future data collection.
Conclusion
This study highlights a high prevalence of adiposity and CMD risk among male Saudi adolescent students. The prediction of CMD risk among students in early age may prove helpful in preventing any untoward complication in future. Adiposity may result in high social cost and damage to public health; therefore, this finding is alarming and necessitates the provision of public awareness about healthy food intake and impact of physical inactivity on chronic diseases.
Footnotes
Acknowledgements
The authors wish to acknowledge the preparatory year students, teachers, and administrations in IAU for collaboration in the study. We also thank the anonymous reviewers for their constructive comments that helped strengthen the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from *Ethical Committee of Imam Abdulrahman Bin Faisal University (IAU) (IRB-2018-19-112)*.
Informed consent
Written informed consent was obtained from all subjects before the study.