
Abstract
This retrospective study was designed to describe the clinical characteristics and prognosis of human immunodeficiency virus (HIV)-infected diffuse large B-cell lymphoma (DLBCL) patients. We retrospectively enrolled 31 patients newly diagnosed with HIV-infected DLBCL from 2009 to 2019 in our institution. The median age of patients was 47 years, and most patients were male (n = 27, 87.1%). Baseline mean CD4+ count was 150.72 ± 146.57/μl. Eighteen (58.1%) patients had B symptoms. Categorized by international prognostic index (IPI) score, 7 cases (22.6%) were in low-risk group (IPI 0-1) and 24 cases (77.4%) were in medium-high risk group (IPI 2-5). Twenty-five (80.6%) patients received highly active antiretroviral therapy (HAART) and 16 (51.6%) underwent standard chemotherapy. The mortality rate was 58.1% (18/31). Univariate survival analysis revealed that HCV infection (p = 0.032), standard chemotherapy treatments (p = 0.038) were associated with overall survival (OS). Our results showed that HIV-infected DLBCL patients had high-risk stratification and high mortality. HCV-coinfection might be associated with poor OS. Early diagnosis and standardized treatments might be beneficial for promoting the survival of HIV-infected DLBCL patients.
Keywords
Introduction
Acquired immunodeficiency syndrome (AIDS) caused by the human immunodeficiency virus (HIV) infection is characterized by defects in T cells immune function. AIDS patients were prone to opportunistic infections and malignant tumors. Epidemiologic data suggested that AIDS-related lymphoma had become the most common neoplasm in patients with HIV in some current case series. 1 HIV-related lymphomas were predominantly B-cell lymphomas. Diffuse large B-cell lymphoma (DLBCL) was the most common subtype, which was highly heterogeneous in morphology, immunophenotype, genetics, clinical manifestations, and prognosis. Currently, there were no specific guidelines for the management of HIV-infected DLBCL patients. This retrospective study aimed to analyze the clinical features and discover new factors to improve our prognostic assessment.
Materials and methods
Patients and data collection
HIV-infected patients with newly diagnosed DLBCL from June 2009 to June 2019 were enrolled in our study according to the 2016 WHO criterion at the Second Hospital of Nanjing, Nanjing University of Chinese Medicine. We collected the following variables: age, gender, ECOG, Ann Arbor stage, IPI score, primary site, lactate dehydrogenase (LDH) level, lymphocyte-to-monocyte ratio, red blood cell distribution width (RDW), virus infection, CD4 count, B symptoms, OS, and treatments. Standard chemotherapy treatment meant receiving four or six cycles of chemotherapy. Overall survival (OS), as the most important endpoint, was defined as the time from diagnosis to the date of death or last follow-up. Because this was a retrospective study, we did not apply for relevant Ethics Committee or Institutional Review Board approval.
Statistical analysis
All statistical analyses were conducted by IBM SPSS (Statistical Package for Social Sciences) statistical software, version 22. Clinical characteristics were described through descriptive statistics. Quantitative data were performed by t-test or Mann-Whitney test according to normality. Comparison between groups was conducted by the Chi-square test. The Cox proportional hazard model was used to establish univariate and multivariate models for OS. We quoted 95% confidence intervals (95% CI) whenever applicable. p-Value < 0.05 was considered statistically significant.
Results
Patient characteristics
A total of 31 HIV-infected patients with DLBCL were included in our study. The clinical characteristics of all cases were summarized in Table 1. The median age of enrolled participants was 47 years (range, 24–69 years) with a gender ratio of 6.75:1. Among total patients, 22 (71%) had ECOG performance status of 0–2, 18 had an elevated LDH level (>300 IU/l) and 10 had CD4+ cells ≥150/mm3. Initial B symptoms were observed in 18 patients. The primary lymphoma site was nodal in 19 cases and extranodal in 12 cases. Patients were divided into two groups according to Ann Arbor stage (group1: I: n = 2 and II: n = 5, group 2 III: n = 4 and IV: n = 20) and grouped into two groups on the basis of IPI (group 1: low risk: n = 7, group 2: low-mediate risk: n = 10, mediate-high risk: n = 10, and high risk: n = 4). Seven patients were HBsAg-positive, in which two of them were HCV coinfection (a total of three cases were HCV-positive). Syphilis antibody positivity were observed in 10 patients. Fourteen patients were treated with CHOP and five patients were treated with R-CHOP (Rituximab 375 mg/m2, ±cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, Vincristine 1.4 mg/m2, Prednisone 60 mg/(m2 × d)). Three patients received EPOCH and three patients received R-EPOCH (Rituximab 375 mg/m2, ±etoposide 50 mg/(m2 × d), Vincristine 0.4 mg/m2, doxorubicin 10 mg/m2, cyclophosphamide 750 mg/m2, Prednisone 60mg/(m2 × d)). One of the patients who received R-CHOP was followed by radiation, as was the patient who received EPOCH. Six patients did not receive chemotherapy, two of whom only received radiotherapy, the remaining because of poor physical tolerance or financial incapacity. Nine patients discontinued treatment, of which two died after one course of treatment. Twenty-five patients received highly active antiretroviral therapy (HAART) including lamivudine, tenofovir, efavirenz, nevirapine, zidovudine, Stavudine. No patient was under fusion-inhibitors during treatment. The toxicities of treatment were mild and common, including infection, grade III or IV myelosuppression, digestive tract reaction, cardiac insufficiency, without significant liver and kidney damage. The median follow-up time was 10.3 months (0.3–97 months).
Clinical characteristics of total patients.

LDH and HCV correlation with patient characteristics
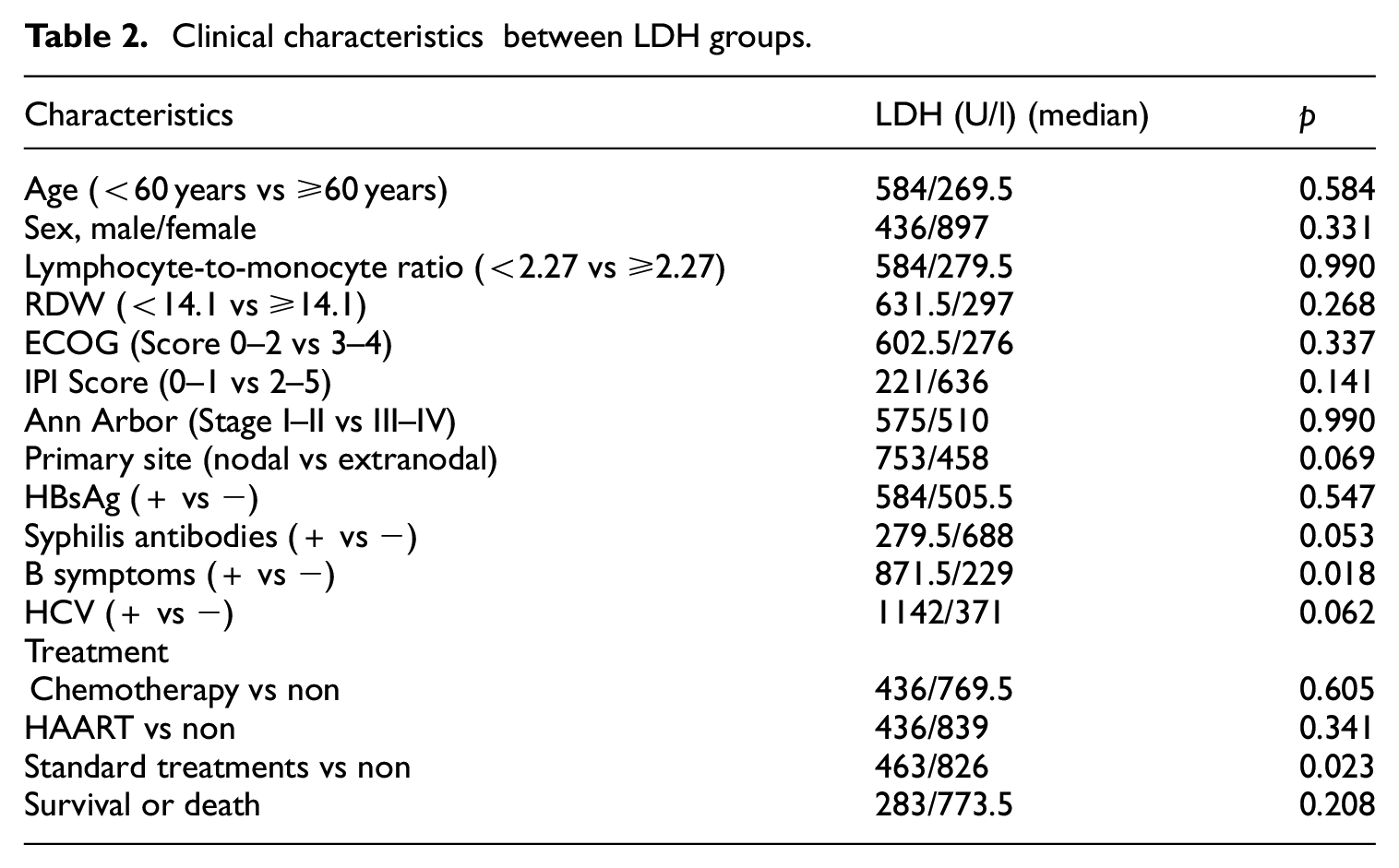
The comparison of clinical characteristics between LDH and HCV groups was shown in Tables 2 and 3. The LDH level of patients with initial B symptoms were significantly higher than those of patients with non-B symptoms (871.5 vs 229, p = 0.018). Patients with lower LDH levels were more acceptable to standard chemotherapy than those with higher levels (463/826, p = 0.023). A higher prevalence of HBV positivity was observed in the HCV positive group, although the association was only of borderline significance (2/3 66.7% vs 5/28 17.9%, p = 0.055). There was no difference in other characteristics between the HCV-positive and negative groups. More detailed information on three HCV patients was shown in Table 4. The three patients presented with HIV infection prior to the diagnosis of lymphoma. They were treated with HAART but did not receive chemotherapy and anti-HCV therapy.
Clinical characteristics between LDH groups.
Clinical characteristics between HCV groups.

Detailed clinical information of 3 HCV patients.

Prognostic factors for OS in patients
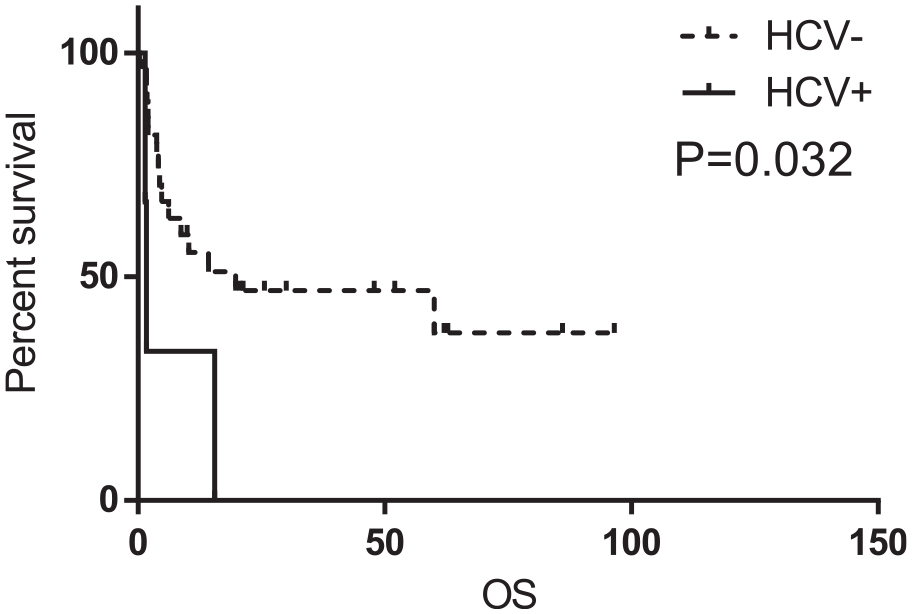
The results of univariate survival analysis were shown on Table 5. HCV-negative (10.4 vs 1.7 months, p = 0.032) (Figure 1) and standard chemotherapy treatment (20.3 vs 4.1 months, p = 0.038) (Figure 2) were significant predictors of better OS. No statistical significance was observed in other groups. We enrolled indicators that p-value <0.05 including HCV infection and standard chemotherapy treatments for multivariate Cox regression analysis. However, they did not affect the prognosis independently.
Univariate COX proportional hazards regression analysis with patients.

Note: Bold values represent HCV infection, without standard chemotherapy treatments were associated with poor overall survival (P<0.05).
Univariate COX proportional hazards regression analysis of OS according to HCV.

Univariate COX proportional hazards regression analysis of OS according to chemotherapy(standard treatment or non.
Discussion
We provided evidence that elevated LDH level was associated with initial B symptoms in HIV-infected DLBCL patients. Patients with lower LDH level were more acceptable to standard chemotherapy than those with higher level. Univariate analysis revealed that HCV infection (p = 0.032), standard chemotherapy treatments (p = 0.038) were associated with overall survival (p < 0.05).
The patients in this study were predominantly male. The male-to-female ratio was 6.75:1. The majority of transmission route was sexual contact for male patients, consistent with the transmission characteristics of the HIV epidemic from high-risk groups to the general population in China in recent years. Half of the patients were diagnosed with HIV and DLBCL at the same time.
Emerging researches about AIDS-related lymphoma (ARL) suggested that IPI score, molecular tumor markers (CD44, P53, IgM, EBV) and HIV scores that incorporate base-line CD4 count were better able to predict prognosis and mortality in ARL patients. 2 Barta et al. 3 established a new score (ARL-IPI) by assigning weights to each predictor (age, extranidal site, CD4 count, virus load, and prior history of AIDS) to assess risk of death in patients with ARL. A South African research study showed that an HIV-infected group with marked immunosuppression (CD4+ cells <150/mm3) acquired a significant inferior OS compared to the HIV-uninfected group.
In our study, we also found that HIV-infected DLBCL patients with HCV-positive were associated with a higher risk of death compared with HCV-negative (1.7 vs 10.4 months, p = 0.032), consistent with the study conducted by Besson. They proposed that chronic HCV infection tended to pejoratively impact the 2-year overall survival rate in HIV-patients with NHL. 4 Some studies adopted HCV load ≥1 × 106 IU/ml as a cutoff value for survival analysis. Patients with HCV load <1×106 IU/ml displayed a significantly longer OS compared with HCV load ≥1 × 106 IU/ml.5,6 The limitation of our research was unable to carry out quantitative analysis of HCV viral load. HCV infection might be one of the reasons for the unexplained increase of NHL incidence. HCV infection might explain the increase of NHL incidence. A recent large European study of people living with HIV demonstrated an increased risk of NHL among patients with HCV co-infection receiving HAART. 7 However, the mechanism of HCV involved in lymphoma remains unclear. It might be that direct genetic involvement, or viral infection mediated chronic inflammatory responses, or viral infection destroyed immune surveillance. HCV envelope protein E2 bound to B-cell receptor CD81, which could reduce B-cell activation threshold. B cells responded to lower concentrations of antigenic stimulation and promote itself proliferation. 8 Persistent HCV infection was associated with abnormal immune receptor rearrangement, especially leading to t (14;18) translocation. Following t (14;18), BCL-2 was activated, which occurs during early B-cell development.9,10 HCV-associated lymphatic proliferation was also related to interference in the interferon signaling pathways. Interruption of IFN-γ decreased the sensitivity to Fas-mediated apoptosis and caspases-3/7/9 messenger RNA enzymatic activity, which in turn increased BCL-2 expression. 11 A Spanish study showed that HCV infection frequently occurred in marginal B-cell lymphomas, diffuse large B-cell lymphoma, and B-cell lymphomas not otherwise specified. After interferon treatment, a decrease in t (14;18) translocated lymphocytes and regression of lymphoma in the spleen marginal zone could be observed. 12 Thus, anti-HCV therapy after chemotherapy remission could improve overall survival and progression-free survival. 13
The degree of immunosuppression was the risk factor for lymphoma onset. The introduction of highly active antiretroviral therapy (HAART) combined with chemotherapy had led to an increase in survival time. 14 In the recent combined antiretroviral therapy (cART) era, HIV-positive DLBCL patient outcomes after R-CHOP therapy were similar to HIV-negative patients. 15 However, we did not observe a significant difference in survival between HAART and non-HAART groups (p = 0.214) in HIV-DLBCL patients. Standard chemotherapy treatments (p = 0.038) were associated with improved overall survival (20.3 vs 4.1 months, p = 0.038). Lim et al. 16 showed that the survival of patients with HIV-related Burkitt’s lymphoma was significantly inferior to that of patients with HIV-DLBCL in the era of HAART. Spina et al. 17 also proposed that HIV-related factors were becoming less important, given the availability of HAART. Thus, standard chemotherapy may expose patients to improve their survival by rescuing CD4+ cell counts in the era of HAART. An advantage may also be in the quality of appropriate chemotherapeutic regimens, which was associated with better OS. A research suggested that compared with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP), initial therapy with more dose-intense regimens (ACVBP (doxorubicin, cyclophosphamide, vindesine, bleomycin, and prednisolone)) resulted in better CR rates, PFS, and OS. Rituximab usage was only significantly related with improved outcomes for patients with CD4 counts ≥50 cells/μl. In this study, the use of rituximab did not affect the prognosis (p = 0.334). When adjusted for the baseline of aaIPI and CD4 count, R-EPOCH was favored significantly over R-CHOP for CR, OS and EFS. 18 Dunleavy et al. 19 demonstrated a CR rate of 92% and 4-year PFS and OS rates of 86% and 70% in patients who received EPOCH-RR (rituximab on days 1 and 5 of each cycle). A random trial in HIV-negative patients showed that dose-adjusted R-EPOCH did not improve progression-free survival or overall survival when compared with R-CHOP. 20 The 2-year event-free survival rates were similar in the patients with complete response who received four or fewer cycles of EPOCH compared with those who received five or six cycles of EPOCH because a complete response was first documented after cycle 4. 21 In this research, there was no significant difference in prognosis between the R ± CHOP and R ± EPOCH regimens (p = 0.353) in HIV-DLBCL, so both regimens were considered valid choices for HIV-DLBCL patients. 22 Of the four patients with radiotherapy, two received radiotherapy after chemotherapy and two received radiotherapy only. Our results showed that radiotherapy had also no effect on survival (p = 0.360).
In conclusion, we conducted HCV infection and standard chemotherapy treatment as prognostic factors in HIV-positive patients with DLBCL. However, this study was only a retrospective analysis of a small sample and short follow-up at a single center. The reliability of the sample verification results required to be further expanded.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.