
Abstract
Augmented renal clearance (ARC) is a phenomenon that can lead to a therapeutic failure of those drugs of renal clearance. The purpose of the study was to ascertain the prevalence of ARC in the critically ill patient, to study the glomerular filtration rate (GFR) throughout the follow-up and analyze the concordance between the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) estimation formula and measured GFR. Observational, prospective, multicenter study. ARC was defined as a creatinine clearance greater than 130 ml/min/1.73 m2. Eighteen hospitals were recruited. GFR measurements carried out twice weekly during a 2-month follow-up period. A total of 561 patients were included. ARC was found to have a non-negligible prevalence of 30%. More even, up to 10.7% already had ARC at intensive care unit (ICU) admission. No specific pattern of GFR was found during the follow-up. Patients in the ARC group were younger 56.5 (53.5–58.5) versus 66 (63.5–68.5) years than in the non-ARC group, p < 0.001. ICU mortality was lower in the ARC group, 6.9% versus 14.5%, p = 0.003. There was no concordance between the estimation of GFR by the CKD-EPI formula and GFR calculated from the 4-h urine. ARC is found in up to 30% of ICU patients, so renal removal drugs could be under dosed by up to 30%. And ARC is already detected on admission in 10%. It is a dynamic phenomenon without an established pattern that usually occurs in younger patients that can last for several weeks. And the CKD-EPI formula does not work to estimate the real creatinine clearance of these patients.
Keywords
Background
Augmented renal clearance (ARC) is a phenomenon that may frequently occur in critically ill patients and may cause therapeutic failure of renal removal drugs. A clear association exists between ARC and infra therapeutic plasma levels of beta-lactams. 1 ARC is defined as a creatinine clearance greater than 130 ml/min/1.73 m2.1,2 ARC incidence can reach 100% in some subpopulation of critically ill patients.3–5 Those patients with sepsis, systemic inflammatory response syndrome (SIRS), serious neurological injuries and burns have been identified as groups at risk for ARC. 6 The exact pathophysiological mechanism of ARC in critical patients remains unknown, as well as the magnitude of their consequences. 7 In order to estimate glomerular filtration, a concentration of serum creatinine is employed, or estimations are made based on equations covering creatinine rate, race, sex, age, etc. However these estimations do not adequately adjust to the critically ill patient. Definitive diagnosis has to be made by glomerular filtration rate (GFR) for creatinine clearance, in 24-h urine collection or it can be made in only 2-h collection.8,9
The aim of this study was to determine the prevalence of ARC in critically ill patients, to study the GFR in the follow-up and to analyze the concordance of CKD-EPI formula and GFR measured in 4-h urine.
The main objectives were: (1) To determine the prevalence of patients with ARC in the intensive care setting; (2) To establish the incidence and natural history of ARC based on a prospective follow-up; (3) Compare the characteristics of the ARC and non-ARC groups; (4) Analyze the concordance between the calculated GFR and estimated GFR by means of the CKD-EPI formula.
Methods
This was a multicenter prospective observational study in the setting of critically ill patients. Ethical approval to report this case series was obtained from The Ethical Committee of Clinical Investigation (REF.CEI: PI-17-091) of the promoting center Germans Trias i Pujol Hospital approved the study. Likewise, as we recruited 18 hospitals, all corresponding Ethical Committees of Clinical Investigation of each participating center approved the project. The committee that approved the research confirmed that all research was performed in accordance with relevant guidelines/regulations. Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
We carried out three prevalence points in February, May, and November 2018. This three points prevalence were measured at these three particular points in time, to cover different seasons of the year, in order to avoid of seasonal biases.
Inclusion criteria
All patients aged 18 and older admitted in the intensive care unit (ICU) the day of the prevalence point at 8 AM
Exclusion criteria
Anuric patients or undergoing vesicle lavage or without urinary catheter or patients under renal replacement therapy (RRT), either continuous or intermittent.
Prospective follow-up criteria were: Patients admitted within 24 h of prevalence point, as well as those diagnosed of ARC. Afterwards, for those patients with prospective follow-up criteria, data collection continued, and they underwent measurements of GFR twice weekly over a period of 2 months.
ARC was established if GFR was over 130 mL/min/1.73 m2 and if the GFR was maintained between 90 and 130 mL/min/1.73 m2 then were non-ARC. Patients with GFR < 90 mL/min/1.73 m2 were not analyzed comparatively with the other two groups, ARC and non-ARC, because we wanted to compare patients with supposedly normal GFR.
GFR is calculated as follows:
Formula:

Where:
C x corresponds to creatinine clearance.
C o corresponds to the concentration of creatinine in urine.
C b corresponds to the concentration of the creatinine substance in blood.
V o corresponds to the volume of urine collected in 4 h expressed in mL/min
BSA corresponds to body surface area
The other variables registered were age, weight, height, sex, creatinine in blood and in urine, urine volume in 4 h, fluid balance, the sequential organ failure assessment score (SOFA), albumin, mechanical ventilation (MV), vasopressors, septic/infectious patient, neurological patient (NRL), ICU and hospital stay, and mortality in the ICU and hospital.
Statistical analysis
Values are described through their distribution of frequencies and their 95% CI. The normality of the quantitative variables was analyzed by the Shapiro-Wilk test. The quantitative variables are described by its median and 95% CI.
Univariate analysis
The qualitative variables were compared using the Chi-Square test.
The quantitative variables were compared by means of the t Student test or the U test of Mann-Whitney, according to whether they followed a normal distribution or not, respectively. A type 1 error less than 0.05 (p&It: 0.05) was considered statistically significant. For the concordance analysis, the Passing-Bablok regression and Bland-Alman plot were employed.
Results
A total of 561 patients were included in 18 sites. These had a median age of 65.5 (63.5–66.5) years and a majority of male gender (61.14%). ARC was found in the 31%. Only 22% had a GFR between 90 and 120 mL/min/1.73 m2 (non-ARC group). And the remaining 47% had a GFR < 90 mL/min/1.73 m2.
From those patients that had been admitted in the ICU the day of the prevalence point, up to 10.7% already presented ARC at admission. Upon admission in the ICU the SOFA was 6 (5–6), 63% required MV and 50.8% needed of vasopressors. Afterwards, the day of the prevalence point the SOFA was 3 (3–4), 46.5% required MV, and 24% needed vasopressors. The median ICU length of stay (LOS) was 15 (14–18) days and 29 (27–33) days in the hospital. In-hospital mortality was 17.83%, and the mortality in the ICU was 13.78%.
At prevalence point, GFR median was 176.4 mL/min/1.73 m2 (IQR 83.9) in the ARC group versus 105.9 mL/min/1.73 m2 (IQR 18.2) in the non-ARC group. In the group with GFR < 90 mL/min/1.73 m2 the median of GFR was 48.7 mL/min/1.73 m2 (IQR 39.1).
We found no specific pattern of GFR evolution in these patients (see Figures 1–3). The ARC patients maintained a GFR > 130 mL/min/1.73 m2 for 3 weeks, until the sixth follow-up. Another noteworthy fact is that the non-ARC’s became ARC’s, after the third follow-up, which means that a patient who initially do not have ARC could in fact develop it from the second week. The patients with GFR < 90 mL/min/1.73 m2 conversely, although improving their GFR after the first week, persisted with GFR between 80 and 90 mL/min/1.73 m2 and did not develop ARC (Figures 1–3).

GFR Follow-up in the ARC group.

GFR Follow-up in the non-ARC group.
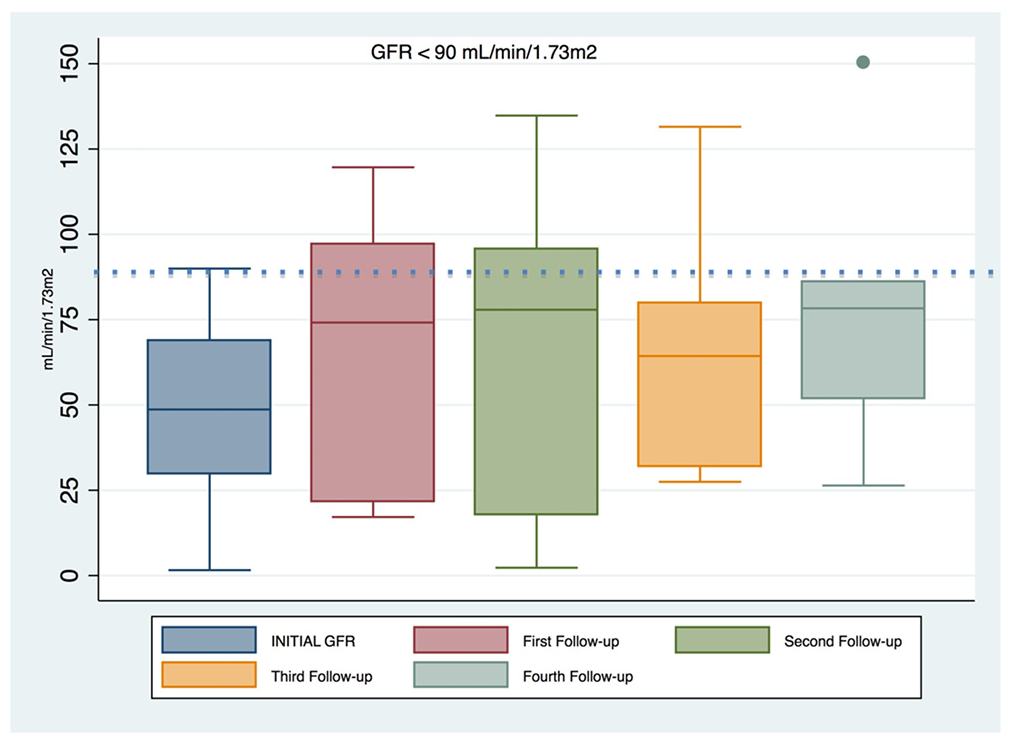
GFR Follow-up of the in the group of patients with GFR < 90 mL/min/1.73 m2.
UNIVARIATE ANALYSIS between the ARC and non-ARC groups (see Table 1):
Univariate analysis of the ARC and non-ARC groups.
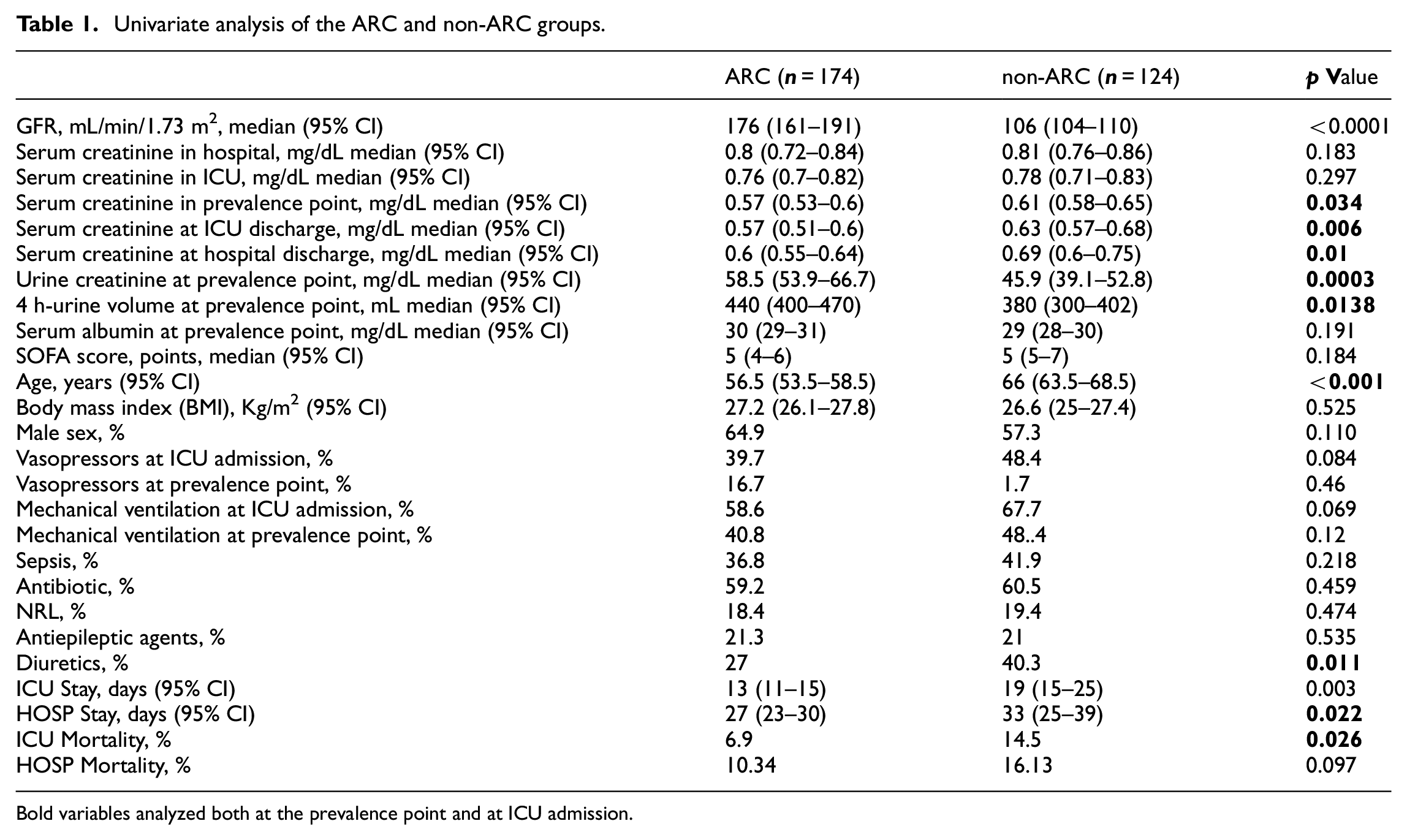
Bold variables analyzed both at the prevalence point and at ICU admission.
The patients in the ARC group were younger than those in the non-ARC one: 56.5 (53.5–58.5) versus 66 (63.5–68.5) years, p < 0.001. In the ARC group we find a tendency of more males (65% vs 57%, p = 0.11), and a reduced need for both mechanical ventilation (59% vs 68%, p = 0.07) and vasopressors (40% vs 48%, p = 0.08), respectively.
As expected, patients in the ARC group had a lower rate of serum creatinine than those in the non-ARC one, as well as a higher rate of creatinine in urine and also a higher volume of urine on the day of the prevalence point, variables that define the augmented renal clearance. These differences in the value of serum creatinine were maintained until hospital discharge. However, upon admission the rates of serum creatinine were not different in both the ARC and non-ARC groups. The patients in the ARC group received fewer diuretics (27% vs 40%, p = 0.011) than those in the non-ARC one.
We found no significant differences regarding weight, height, SOFA score, or albumin between both groups. There were neither differences with respect to the number of septic patients (37% vs 42%, p = 0.22) nor neurocritical patients (32% vs 33%, p = 0.44) between both the ARC and non-ARC groups.
ICU mortality was lower in the ARC group, 6.9% versus 14.5%, p = 0.003. Accordingly, a tendency was found of lower hospital mortality in the ARC group, 10.34% versus 16.13%, p = 0.1. The median ICU stay was lower in the ARC group: 13 (11–15) days versus 19 (15–25), p = 0.03. Likewise, hospital stay was lower in the ARC group: 27 (23–30) versus 33 (25–39) days, p = 0.02.
Concordance analysis
The concordance analysis realized between the estimated GFR by the CKD-EPI formula the measured GFR through the 4-h urine highlighted that there is no concordance between the estimation CKD-EPI formula and the GFR calculated from 4-h urine (see Figures 4 and 5).

Concordance analysis: Bland-Altman Agreement.

Concordance analysis: Passing Bablock Regression line.
Discussion
This study highlights that ARC is a frequent phenomenon, with a prevalence of around 30%. And also that ARC is found in a 10% at ICU admission. Moreover, ARC may last more than 3 weeks and non-ARC patients can develop ARC over time. However, in this observational study we have been unable to determine a concrete pattern of the progression of GFR in these patients.
This study also demonstrates the lack of concordance between the estimation CKD-EPI formula and the measured GFR calculated through the 4-h urine sample.
Regarding the characteristics of ARC patients when compared non-ARC ones, we have observed no notable differences except in age, with ARC’s being younger.
The ARC phenomenon is worrying because it may be relevant in patients treated with renal removal drugs, so that the efficacy of the medication administered can be compromised. 10 The possible clinical implications derived from the under exposure to renal elimination drugs may be relevant; in some cases may be catastrophic. If not reaching pharmokinetic/pharmodinamic (PK/PD) objectives, the probability of treatment failure increases. The physiological fluctuations seen in critically ill patients involve an altered pharmokinetic and a higher risk of suboptimal exposure of antibiotics, especially if a standard dose is administered following current guidelines.11–18 In addition to antibiotics, there are other kinds of drugs with risk of under exposure such as some antiepileptic drugs and low molecular weight heparins that are also removed by the kidney. These drugs dosage in ARC should be revised, dosing interval may need to be shorter with higher doses.
The main problem stems from the diagnosis of these patients, given that the concentration of serum creatinine remains well below the normal range and generally goes unnoticed. Additionally, the formulas that estimate the glomerular filtration (CKD-EPI, modification of diet in renal disease study equation; MDRD, and Cockcroft Gault formula; CG) do not have good concordance with the measured GFR,19–24 and in ARC estimation formulas are not validated. 22 Our study demonstrates the lack of concordance between the estimation by the CKD-EPI formula and the measured GFR calculated through the 4-h urine sample. Furthermore, since it is a dynamic phenomenon, follow-up during ICU admission is recommendable in order to avoid overdose or therapeutic failures.
Limitations
We must point out that this is an observational study and therefore this in itself is a limiting factor to deduce prognostic relations. The outcome obtained results should be viewed with caution, given that this type of observational study is unable to control potentially confounding variables. Associations found between two variables could in fact be due to another, and the clinical result could depend on this third variable. As we did not find any differences in both patients-group characteristics we couldn’t conduct a multivariate regression and any differences between the two groups could be attributed to confounding.
Nevertheless, we must bring to light that this multicenter epidemiological study covers a representative sample population of Catalonia, a Spanish region, with the inclusion of the majority of third level reference hospitals as well as local ones, with which the results can be extrapolated to the general population of this geographic area of the country. The study’s most noteworthy results have underscored that ARC is frequent and affects younger subjects, and also shows that GFR estimation formulas are not useful in diagnosing ARC, and that GFR should be measured to determine creatinine clearance in critically ill patients.
In sum, the critically ill patient can commonly suffer from ARC and its diagnosis depends on the degree of clinical suspicion. Since the serum creatinine level does not stand out, nor estimation formulas, a normal renal function is presumed, and the doses of renal-clearance drugs are titrated consequently. The possible implications are therapeutic failure, as beta-lactam antibiotics and other medications with renal clearance. Regarding the COVID pandemic and the need of anticoagulants for thromboembolic events prevention, physicians have to be aware of this ARC phenomenon.25–28 A 30% of these critically ill patients could be at risk of under exposure to low molecular weight heparins.
Conclusions
This multicenter epidemiological study underlines the fact that the Augmented Renal Clearance is quite common in critical patients, found in up to 30% of ICU patients at some point in their evolution. This is a dynamic entity without an established pattern that can persist for some weeks and usually affects younger patients. ARC is a relevant phenomenon because it may cause therapeutic failure of renal removal drugs. Finally, we have observed that ARC goes unnoticed on the clinician’s part because neither the creatinine value nor the estimation formulas detect it, making it essential to calculate GFR to determine accurate creatinine clearance in these patients.
Footnotes
Acknowledgements
Blood Purification Therapies Collaboration Group. Catalan Society of Intensive Care Medicine.
As all hospitals/institutions covered the costs of urinalysis, we want to acknowledge them.
Author contributions
The author(s) read and approved the final manuscript.
TMTI is the person that planned the study, contributed to its design, advanced it by contacting other centers for recruitment, was in charge of resolving doubts from other investigators related to data collection, performed part of data collection in her center and wrote the manuscript; JSR contributed in data collection in his center, was in charge of resolving doubts concerning urine collection for the protocol and data collection, and corrected the manuscript; MPC was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in his center; POB was in charge of resolving doubts from other collaborators related to urine collection for the protocol and data collection and performed the data collection in her center; YDB was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in her center. ANP was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in her center; ABR was in charge of resolving doubts from other collaborators related to urine collection for the protocol and data collection and performed the data collection in his center; MRL was in charge of resolving doubts from other collaborators related to urine collection for the protocol and data collection and performed the data collection in his center; MIV was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in her center; AOI was in charge of resolving doubts from other collaborators related to urine collection for the protocol and data collection and carried out the data collection in his center; IOZ was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in her center; CRA was in charge of resolving doubts from other collaborators related to urine collection for the protocol and data collection and performed the data collection in his center; SCH was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and performed data collection in her center; EVT was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in his center; RMCI was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and performed the data collection in her center; MMT was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in her center; JGM was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and performed the data collection in her center; JXC was in charge of resolving doubts of other collaborators concerning urine collection for the protocol and data collection and carried out the data collection in her center, and PMN revised the global data base and did the statistical analysis.
Ethics approval
Ethical approval to report this case series was obtained from The Ethical Committee of Clinical Investigation (REF.CEI: PI-17-091).
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Availability of data and materials
All papers included in the full-text.