
Abstract
To investigate the epidemiology of acute kidney injury and to clarify the risk factors associated with the prognosis of acute kidney injury in critically ill patients in the Gansu Province. This was a multicenter, retrospective study. The clinical data of all patients from January 1, 2017, to December 31, 2019, in the intensive care unit of the selected hospitals were screened. Descriptive statistical analysis was performed first, and then the patients were divided into a survival group and a nonsurvival group based on survival status at discharge. Univariate and multivariate logistic regression analyses were used to determine the risk factors for in-hospital mortality in patients with acute kidney injury. (1) Among the 8106 patients admitted, a total of 3019 patients were excluded according to the exclusion criteria. Among the included patients, 890 patients met the diagnostic criteria for AKI, with an incidence of 17.5% and mortality of 41.3%. (2) Logistic regression analysis showed that sex, age, AKI stage, infection, cardio-pulmonary resuscitation, cardiac output, mechanical ventilation, diuretics, white blood cells, platelets, blood urea nitrogen, prothrombin time, and activated partial thromboplastin time were significantly associated with the prognosis of acute kidney injury (p < 0.05). Large-scale epidemiological data from several representative general hospitals in the Gansu Province showed that the incidence and mortality of acute kidney injury in intensive care units were still very high.
What’s already known about this topic?
Acute kidney injury (AKI) is a common critical illness among in-hospital patients, especially critically ill patients. Due to the different criteria used, the incidence of AKI in critically ill patients has reported to be between 3.2% and 78%.However, there are few AKI epidemiological studies among critically ill patients in China, especially in western China, and the data are basically nonexistent.
What does this article add?
Our research “The epidemiology of acute kidney injury in critically ill patients in the Gansu Province (EACG)” series (Chinese clinical trial registration number: ChiCTR1800016945) will further expand upon the data collected from critically ill patients with AKI in the Gansu Province, establish a database and build a cross-field data sharing platform to help more clinical and scientific researchers interested in AKI quickly obtain clinical data and process these data.
Background
Acute kidney injury (AKI) is a common critical illness among in-hospital patients, especially critically ill patients.1–3 Broadly speaking, AKI is a sudden decrease in glomerular filtration rate (GFR) caused by a variety of etiologies and clinical symptoms. At present, there are many problems in the diagnostic criteria of acute kidney injury based on serum creatinine (SCr) and urine volume, and more than 30 definitions have been used to diagnose AKI. 4 Due to the different criteria used, the incidence of AKI in critically ill patients has reported to be between 3.2% and 78%. 5 Moreover, the diversity of AKI definition criteria led to an incomparability among the results of various studies and the inability to accurately evaluate the therapeutic effects of different treatment regimens and interventions for AKI. Although we have made great progress in basic research and the identification and treatment of AKI, the prognosis of AKI is still poor.6,7 The incidence and mortality of AKI show significant differences among countries due to the different backgrounds of AKI patients and the diversity of AKI definitions.8,9 The latest study reported that the incidence of AKI in patients admitted to the Mayo clinic was 6.7% and that in critically ill patients was 16.9% between 2006 and 2014. 10 Two other multinational prospective studies found that the incidence of AKI was 5.7% and 57.3%.11,12 However, there are few AKI epidemiological studies among critically ill patients in China, especially in western China, and the data are basically nonexistent. Therefore, this study intends to select three tertiary hospitals in the Gansu Province to obtain epidemiological data of AKI in critically ill patients to infer the epidemiology of AKI in critically ill patients in western China.
Data and methods
This is a multicenter retrospective observational study about the epidemiology of AKI in ICU patients in Gansu, China. The Ethics Committee of LanZhou University Second Hospital approved this study. The Chinese Clinical Trial Registry number is ChiCTR1800016945. All patients admitted to the ICU in three participating tertiary hospitals in the Gansu Province from January 1, 2017, to December 31, 2019, were retrospectively analyzed.
Inclusion criteria
During the study period (January 1, 2017 to December 31, 2019), all patients admitted to the ICU in three participating tertiary hospitals in the Gansu Province were enrolled.
Exclusion criteria
End stage renal disease (ESRD).
History of bilateral nephrectomy.
Kidney transplantation history within 3 months before ICU admission.
Readmission to the ICU during the same hospitalization period.
Design
The data were recorded in Microsoft Excel, and the research was divided into five steps:
First, all patients admitted to the hospital in 2017 and 2019 were recruited using the Hospital Information System (HIS).
In the second step, the medical records and laboratory examinations were checked one by one for all patients, and patients who met the exclusion criteria were excluded.
The third step was to check the medical records of all AKI patients and extract the data.
The fourth step was to sort out the collected data and import them into Excel.
The fifth step was to import the data into SPSS software for statistical analysis.
Definitions
AKI was defined by the KDIGO criteria. 13 To clarify the etiology of AKI, the AKI patients were divided into three categories according to etiology: prerenal, renal substantive, and postrenal. Baseline serum creatinine was defined as the lowest serum level during the preceding 3 months. 7
Statistics
SPSS software 21.0 (SPSS Inc. Chicago, IL, USA) was used for statistical analysis. Descriptive statistical analysis was conducted on the enumeration data, and statistical charts were drawn. Then, the characteristics of AKI patients were grouped according to their survival status at discharge. If the measurement data followed a normal distribution, the mean ± standard deviation (x ± s) was used. The t-test was used to compare the two groups, and the q-q normal probability graph was used for the normality test. If the measurement data did not follow a normal distribution, the median M and quartic interval (Qu, QL) were used. Comparisons between the two groups were conducted by the Mann–Whitney U test in the Spearman nonparametric test. Enumeration data were expressed as n (%), Pearson’s chi-square test was used to compare binary classification data between the two groups, and the Mann–Whitney U test was used for ordered multiclassification. Logistic regression analysis was used to evaluate the risk factors. First, univariate logistic regression analysis was performed on the demographic data, AKI stage, etiology classification, basic diseases, risk factors, vital signs, laboratory examination results, and whether RRT affected the prognosis of AKI patients, and a collinear judgment was made. Then, the variables with statistical significance in the univariate analysis were analyzed by multivariate logistic regression. If the variables were collinear and there were significant differences in the univariate logistic regression analysis, one of the variables was selected for multivariate logistic regression analysis. All tests were bilateral, with p < 0.05 defined as statistically significant.
Results
Basic data and general information of the AKI patients
A total of 8,106 patients were admitted to the ICUs of the three hospitals. Of the 3019 patients excluded, the reasons were as follows: 517 patients were <18 years old, 1831 patients were admitted to the ICU for <24 h, 482 patients had chronic kidney disease, 16 patients had nephrectomy, five patients underwent kidney transplantation within 3 months before admission to the ICU, 52 patients were re-admitted to the ICU during the same hospital stay, and 116 patients had missing needed data for the study (Figure 1). The characteristics of the AKI patients are shown in Table 1.
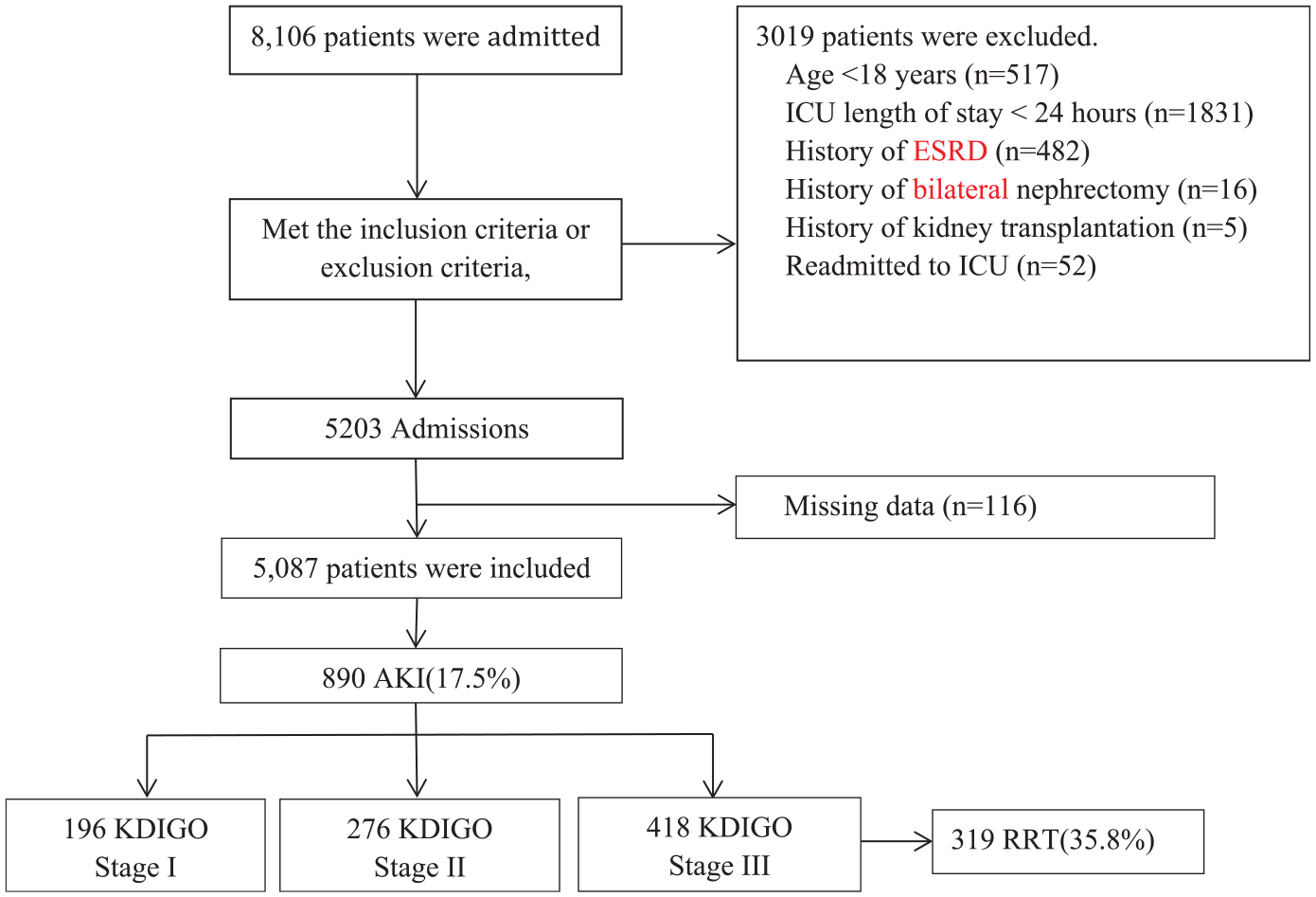
Flow chart.
Characteristics of the AKI patients.

COPD: chronic obstructive pulmonary disease; Scr: serum creatinine; Cardiac disease: cardiac dysfunction caused by a variety of reasons, cardiac ultrasound confirmed the presence of diastolic dysfunction or EF < 50%; Respiratory failure: severe disturbance of pulmonary ventilation due to a variety of causes, with arterial partial pressure of oxygen (PaO2) below 8 kPa (60 mmHg), or with a partial pressure of carbon dioxide (PaCO2) above 6.65 kPa (50 mmHg); APACHEII: acute physiology and chronic health evaluation II; ED: emergency department; MV: mechanical ventilation; SCr: serum creatinine; AKI: acute kidney injury.
Incidence of AKI
According to the KDIGO criteria, a total of 890 ICU patients developed AKI, with an incidence of 17.5% (890/5087).
AKI stage
According to the KDIGO criteria, AKI can be divided into KDIGO stages (I, II, III); this study included 22.02% (196/890) stage I cases, 31.01% (276/890) stage II cases, and 46.97% (418/890) stage III cases.
Etiology of AKI
Among which 64% (570/890) had pre-renal failure. The main causes included 255 cases of sepsis and septic shock, accounting for 44.7%; 130 cases of reduced cardiac output, accounting for 22.8%; 113 cases of fluid loss from various causes, accounting for 19.8%. A total of 33% (294/890) had renal substantial renal failure; 16.3% (48) had renal vascular and glomerular diseases, 75.9% (223) had renal tubular and interstitial diseases, 7.8% (23) had other unknown renal injury sites, and 2.7% (24) had postrenal failure. The main causes were 37.5% (9) cases of urinary tract stones, 25% (6) cases of urinary tract tumors, and 29.2% (9) cases of ureteral strictures, followed by prostate disease and neurogenic bladder.
Outcomes of AKI
The AKI patients were divided into two groups according to outcome: the survival group and the non-survival group. Of the patients with AKI hospitalized in the ICU, there are 368 deaths during hospitalization, and the mortality rate was 41.3% overall, 16% (59) for stage I AKI, 31.5% (116) for stage II AKI, and 52.4% (193) for stage III AKI; the higher the AKI stage was, the worse the prognosis. The mortality of patients without RRT was 37.1% (212), and 48.9% (156) of patients with RRT died (p = 0.001). Further analysis showed that patients treated with RRT had a higher AKI stage and more severe disease than those without RRT. And the ICU-LOS was 9 days (4–16).
Risk factors for death in AKI patients
Univariate analysis
Univariate logistic regression analysis showed that male sex, old age, high AKI stage, RRT, infection, cardio-pulmonary resuscitation, reduced cardiac output, mechanical ventilation, diuretics, and reduced white blood cells, platelets, blood urea nitrogen, serum albumin prothrombin time (PT), and activated partial thromboplastin time (APTT) were significantly correlated with death in AKI patients (all p-values were less than 0.05) (Table 2).
Univariate logistic regression analysis.

Multivariate analysis
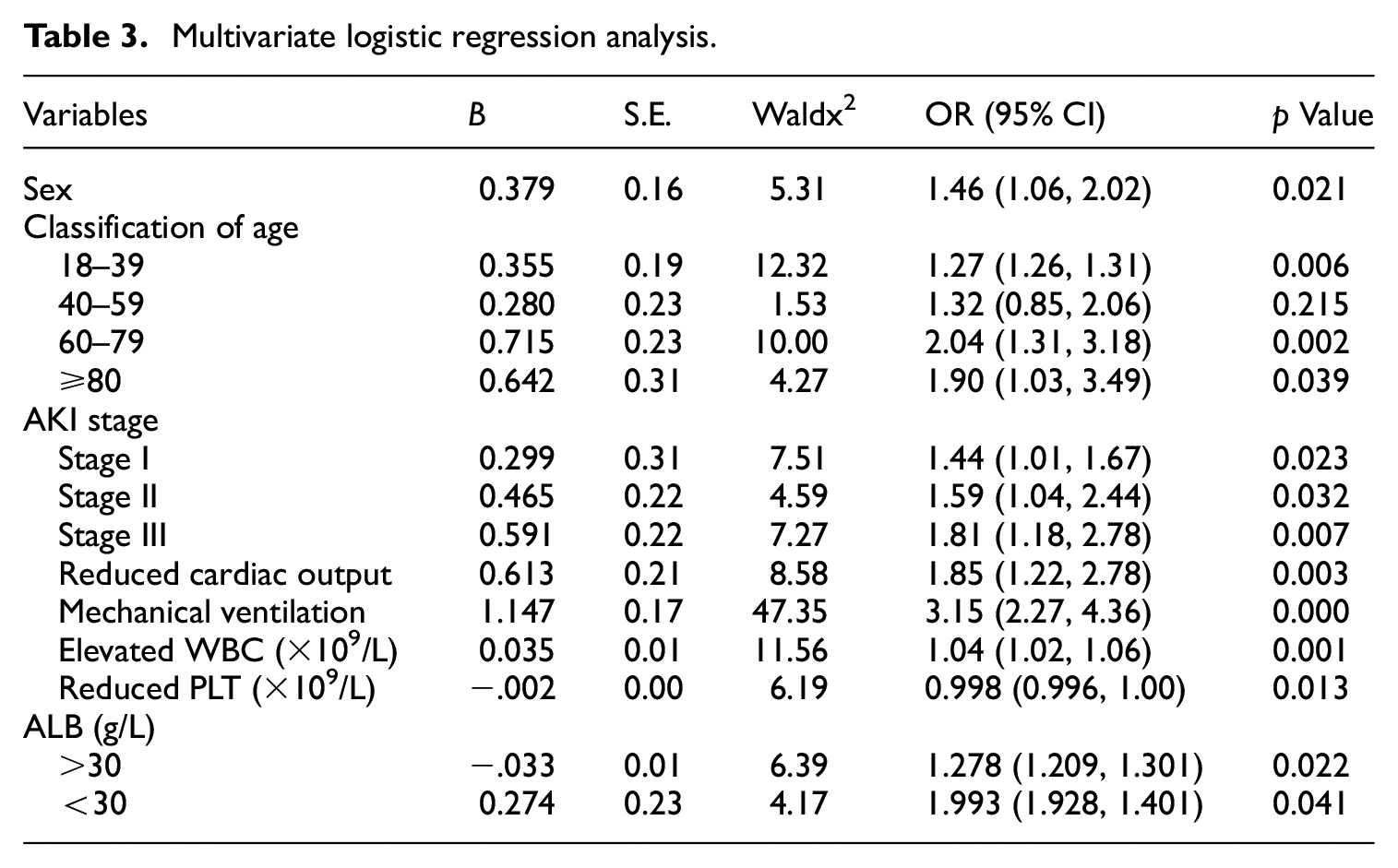
Multivariate logistic regression analysis showed that old age, male sex, high AKI stage, reduced cardiac output, mechanical ventilation, RRT, elevated leucocyte count, reduced platelet count, and reduced serum albumin were all independent risk factors for AKI death (Table 3).
Multivariate logistic regression analysis.
Septic AKI
Sepsis and septic shock were the most common causes of AKI in critically ill patients. Among the AKI patients enrolled in this study, 28.7% (255/890) had AKI caused by sepsis and septic shock, which were the major causes of AKI. The main infection sites were the lung, abdomen, urinary system, skin, and soft tissue. Among the patients with AKI caused by sepsis and septic shock, 92 patients received RRT, accounting for 28.8% of the total patients treated with RRT. A total of 136 patients with sepsis and septic shock AKI died, leading to a mortality of 53.3%.
Discussion
Acute kidney injury is a major clinical problem in critically ill patients that leads to high medical costs and poor prognosis. AKI can arise from a variety of causes and is an important risk factor for chronic kidney disease (CKD). Recently, a southern medical university 14 conducted epidemiological studies on AKI in ICU inpatients in nine hospitals in different regions of China, but this study did not include the northwest region. Epidemiological investigations have shown that the occurrence and development of diseases will be affected by different regional environments, different study populations, different economic levels and different medical conditions.15–17 Here, we considered several representative hospitals in the Gansu Province in northwest China as investigation points to conduct a multicenter and retrospective study of 8106 patients admitted to a comprehensive ICU.
The results showed that the incidence of AKI was 17.5% overall, 22.02% for stage I, 31.01% for stage II, and 46.97% for stage III, and the mortality was 41.3%. A southern medical university study found that, on the basis of the KDIGO diagnostic criteria, the incidence of AKI among ICU inpatients was 30.04%, and AKI stages I, II, and III accounted for 52.1%, 19.7% and 28.2% of the patients, respectively. Another regional retrospective study that included five ICU centers in southwest China’s Sichuan province reported an incidence of AKI of 37.8% and hospital mortality as high as 51.8%. 18 In our study, in comparison, the incidence of AKI was lower, and stage III AKI had for the highest incidence of all stages. The reason may be that AKI lacks specific symptoms and is mainly diagnosed by monitoring the changes in serum creatinine in the short term. A low awareness of AKI would lead to repeated low serum creatinine readings, and the low recognition rate of AKI will cause treatment delays and speed up AKI progression. According to a multicenter survey, the repeated serum creatinine detection rate of hospitalized patients in mainland China was only 29.8%, which is lower than the number reported by developed countries (63.2%–67.6%). 19 Therefore, it is reasonable to believe that the incidence of AKI in the relatively underdeveloped northwest region may be underestimated.
Currently, the main treatment methods for AKI include identifying and removing causes and risk factors, treating the primary disease, improving renal insufficiency, providing kidney-preserving drugs, and administering continuous renal replacement therapy (CRRT). CRRT has been an important supportive therapy for patients with AKI, and there are multiple treatment models available based on different mechanisms. RRT procedures were continuous RRT (CRRT). Continuous veno-venous hemofiltration.
(CVVH) was the most common mode. Of the 890 AKI patients, 35.8% (319/890) received CRRT, including 6.3% (20/319) stage I patients, 21.6% (69/319 stage II patients), and 72.1% (230/319) stage III patients. CVVH was used in 298 patients and continuous veno-venous hemodiafiltration (CVVHDF) in 21 patients. And no patients received cytokine adsorber. The higher the AKI stage was, the more patients received CRRT. The timing of RRT initiation was 25 ± 2 h.
In addition, the analysis of laboratory indicators showed that elevated white blood cells, thrombocytopenia and decreased serum albumin were risk factors for death in patients with AKI. Domestic studies have also shown that elevated white blood cells are an independent predictor of AKI death, which may be associated with increased inflammatory response and increased inflammatory mediators. The pathophysiological mechanisms of AKI are multifactorial, including direct inflammatory injury and systemic inflammatory response caused by ischemia/reperfusion injury. A recent study reported a significant association between decreased platelet count after coronary artery bypass grafting and short-term mortality from AKI. 20 Platelet is an important mediator of ischemia and inflammation of vital organs, and thrombocytopenia is an indicator of the severity of severe diseases. This can be explained by the role of platelets in microthrombosis, which may cause microvascular occlusion with clinical manifestations of AKI, stroke, or myocardial ischemia. 21 In other words, a low platelet count could indicate active microthrombosis causing microvessel blockage. The decrease of albumin can lead to the decrease of colloid osmotic pressure in blood vessels, and the decrease of effective circulating blood volume, which will lead to the decrease of renal blood flow and renal injury. In addition, albumin contributes to the body’s anti-oxidation and damage repair, and hypoproteinemia can reduce the resistance of patients, leading to poor prognosis.22,23
We also found that APTT and PT were significant in univariate analysis, but no statistical difference was found in multivariate analysis. It is well known that patients with AKI may experience disorders of coagulation, from hypercoagulability in the early stage to hypocoagulability in the late stage. Therefore, although there was no statistical difference, clinical attention should still be paid to the monitoring of coagulation function in such patients.
It is noteworthy that this study found an increased risk of death in male AKI patients compared to in female AKI patients, which was inconsistent with previous studies that showed no significant impact from sex on the prognosis of AKI patients, but a recent study also showed that the male sex was a risk factor for poor prognosis in AKI patients. 24 Further studies are needed to confirm the effect of sex on the prognosis of AKI patients.
Limitations and strengths
This study selected three hospitals that can represent the medical situation of the Gansu Province. From the perspective of epidemiological sampling, there is sampling bias, which may affect the epidemiological results for AKI. In the future, more data from hospitals of different regions and levels can be collected for further research.
Our study is a retrospective study and thus cannot accurately monitor the urine volume of patients, which may underestimate the incidence of acute kidney injury.
Although this study has some shortcomings, it is also innovative and practical, which is of great benefit for guiding clinical treatment. First, epidemiological studies on acute kidney injury in critically ill patients are mostly single-center, small-sample studies with poor representativeness. Our study is a multicenter study with a large sample size, which is closer to the overall sample size. The results of our study are more conducive to guiding clinical treatment and scientific research. Second, laboratory indicators were added to the analysis of prognostic risk factors in our study, and these indicators were simple and economical to obtain and had good clinical application prospects. At present, most scholars are committed to studying the pathogenesis of AKI and the risk factors affecting the occurrence of AKI, while research on the factors affecting the prognosis of acute kidney injury has relatively lagged behind. In the future, predicting the prognosis of AKI will arouse the interest of many researchers. Most importantly, with the rapid development of big data in medicine, an increasing number of people will realize the importance of data science. The development of medical science and technology is also inseparable from big data. Specialized development, collation, and analysis of big data may bring unexpected benefits to our scientific research. Therefore, our research “The epidemiology of acute kidney injury in critically ill patients in the Gansu Province (EACG)” series (Chinese clinical trial registration number: ChiCTR1800016945) will further expand upon the data collected from critically ill patients with AKI in the Gansu Province, establish a database and build a cross-field data sharing platform to help more clinical and scientific researchers interested in AKI quickly obtain clinical data and process these data. Furthermore, data from China, the world’s largest developing country, will provide valuable information for improving the current situation and economic burden of acute renal impairment worldwide.
Conclusion
Large-scale epidemiological data from several representative general hospitals in the Gansu Province showed that the incidence and mortality of acute kidney injury in intensive care units were still very high. Sepsis and septic shock are the main causes of AKI.
Footnotes
Author contributions
Conducted the study: YC, FF.
Collected all data: DL, YY, ML, J-jY, C-hM, C-mD.
Did the statistical analysis: YC, X-nC.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The Ethics Committee of LanZhou University Second Hospital approved this study, and the number was 2018-043. Written informed consent was obtained from individual or guardian participants.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.