
Abstract
This study evaluated an antibiotic stewardship program (ASP) intervention aimed at reducing inpatient fluoroquinolone (FQ) use and examined its impact on ciprofloxacin susceptibilities of gram-negative bacteria in a large 611-bed community hospital. A two-step ASP intervention was implemented: an electronic medical record algorithm that prompted physicians to re-evaluate FQ use shortly after admission and changed institutional UTI/pneumonia guidelines that recommended options alternate to FQs for first-line empiric antibiotic therapy in 2010 and 2011 respectively. Between 2007 and 2017 FQ use and ciprofloxacin susceptibilities of all non-duplicate cultured isolates of Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, and Pseudomonas aeruginosa obtained ≥72 h after admission were reviewed. Ambulatory care isolates served as a comparison group. FQ utilization rates and relationships to ciprofloxacin susceptibility were evaluated using interrupted time series models. Over the 11-year period, FQ use decreased from 110.0 (2007) to 26.2 (2017) days of therapy/1000 days at risk (p < 0.001). Compared to pre-intervention, the estimated (post-intervention) reduction in FQ utilization was 28.4 (95% CI: 10.9–46) days of therapy/1000 days at risk. Reduced FQ utilization was correlated with increase susceptibilities to ciprofloxacin of hospital onset isolates of Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis (p < 0.02), and Pseudomonas aeruginosa (p = 0.07). No significant susceptibility change was observed in the ambulatory care isolates. Persuasive interventions by an ASP successfully modified physicians’ inpatient empiric antibiotic use, produced a sustained reduction in FQ utilization rates and increased ciprofloxacin susceptibility to four commonly encountered gram-negative bacteria in a community hospital.
Introduction
Antimicrobial resistance fueled by overuse and misuse of antibiotics has become a public health problem of global concern, resulting in limited treatment options. It is associated with increased morbidity, mortality, length of hospital stay, as well as overall cost. 1 Guidelines from several advisory bodies including the CDC strongly support and promote the role of antibiotic stewardship programs (ASP) that address these issues in various US healthcare settings. 2
Multiple studies have documented declining susceptibilities of gram-negative isolates to fluoroquinolones (FQ), in parallel with increased use of members of this class of antibiotic,3,4 and subsequent collateral issues such as colonization and infection with methicillin-resistant Staphylococcus aureus, carbapenem-resistant enterobacteriaceae, and Clostridioides difficile infections. 5
Studies exploring the relationship between FQ use and susceptibilities of gram-negative isolates to FQs through ASP initiatives in hospital settings have produced conflicting results.6–8 Most studies have used annual institutional antibiograms produced from data that pooled isolates from community and hospital onset (HO) infections. Few have examined the direct relationship between inpatient FQ use and susceptibility of isolates from the HO setting within a single large institution.
This report describes the effect of an ASP intervention designed specifically to decrease inpatient FQ use on utilization rates of this class of antibiotics, and susceptibility of the four most prevalent health-care associated gram-negative bacilli to ciprofloxacin in a US community hospital.
Methods
The BronxCare Health System (BCHS) consists of a large 611-bed community hospital in South-Central Bronx, New York that includes a 26-bed adult intensive care unit, an 11-bed coronary care unit and 42 associated outpatient clinics. Since 2007 BD HealthSight™ Clinical and Infection Advisor (MedMined™, Becton, Dickinson and Company, Franklin Lakes, NJ), has electronically monitored and reported all cultured isolates with their sensitivities to the Infection Control Department and the ASP team. The ASP team at BCHS has been in place since 2004 and is multidisciplinary, with representatives from pharmacy, infectious disease, nursing, infection control, laboratory, and information technology.
First ASP intervention
Commencing in 2010 a question “do you need to continue FQs?” and “if yes, can you use PO (oral route)?” was automatically triggered in the hospital’s electronic medical record (Allscripts) on the third day of all inpatients started on this class of antibiotic. This prompted house staff to consider transitioning from intravenous to oral, use an alternate antibiotic with either route that was guided by culture and sensitivity results, and/or to request an infectious disease consult.
Second ASP intervention
In 2011 new institutional guidelines for antibiotic treatment of urinary tract infections (UTI) and pneumonia were developed promoting the use of alternate antibiotics as empiric initial therapy and recommending use of FQs as a second-line antibiotic. Both interventions were active interventions, consisting of changes in the electronic medical record, posting of institutional guidelines on the hospital’s intranet and supplemented by extensive education provided to all providers about antibiotic usage.
Study design
This was a retrospective study using the BD HealthSight™ Clinical Advisor database, between July 2007 and December 2017. FQ (primarily ciprofloxacin) sensitivity profiles of all non-duplicate (first isolate in 30 days) culture positive HO isolates (collected ≥72 h after admission) of Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis and Pseudomonas aeruginosa across all sources, excluding surveillance and environment, were evaluated. Susceptibilities for the same pathogens in ambulatory care settings (outpatient clinics part of BCHS) were also evaluated and served as a comparison group. All FQ susceptibilities were determined using prevailing Clinical and Laboratory Standards Institute guidelines and performed by Quest Diagnostics. We evaluated trends in inpatient FQ prescribing and those of three other broad-spectrum beta-lactam antibiotics (third and fourth generation cephalosporins [3rd/4th Ceph], piperacillin-tazobactam, and carbapenems). Antibiotic utilization rates were calculated as days of therapy per 1000 patient days at risk (DOT/1000 patient days at risk). Primary outcome measures were trends in FQ utilization rates and percent susceptibility to ciprofloxacin for HO isolates of each gram-negative bacilli by calendar year. Secondary outcome measures were susceptibility of HO isolates to 3rd/4th Ceph, piperacillin-tazobactam, and carbapenems. Antibiotic utilization data and susceptibility of Gram-negative bacilli were analyzed on a yearly basis.
Statistical analysis
As an exploratory phase of the analysis, we used Pearson Chi-square test and regular regression methods to explore the linear trend of data over time. It was found that our data series showed an autocorrelation (tested using Durbin-Watson tests). Therefore, we decided to use time series methods to analyze the data. Trend and intervention effects were evaluated using autoregressive integrated moving average (ARIMA) models including using the interrupted time series models to assess ASP intervention effects. All statistical assessment results reported in this study were based the analyses using ARIMA models. The statistical analyses were conducted using Statistical Analysis System (SAS) V9.4 (SAS Institute, Cary, NC) and SAS/ETS 13.1.
Results
Trend in antibiotic use and intervention effect
Over the 11-year period, FQ use significantly decreased from 110.0 (2007) to 26.2 (2017) DOT/1000 days at risk (p < 0.001), Figure 1. During that time there was an increase in use of 3rd/4th Ceph from 74.0 to 116.1 DOT/1000 days at risk (p < 0.001]), piperacillin-tazobactam from 74.6 to 105.8 (p = 0.21), and carbapenems from 18.0 to 31.3 (p = 0.001). Combined FQ, 3rd/4th Ceph, piperacillin-tazobactam, and carbapenems use was similar at the beginning and end of the study period, 276.6 and 279.4 DOT/1000 days at risk respectively (p = 0.415). There was a significant reduction in FQ use after implementation of the ASP intervention (p = 0.002) with an estimated amount of 28.4 (95% CI: 10.9–46.0) DOT/1000 days at risk, which indicated a strong effect of the intervention on FQ use. At the same time, we found that the intervention had a significant effect on piperacillin-tazobactam use (p = 0.001) with an estimated increase of 16.7 (95% CI: 6.5–27.0) DOT/1000 days at risk while the intervention effects on 3rd/4th Ceph and carbapenems uses were not significant (all p > 0.801).
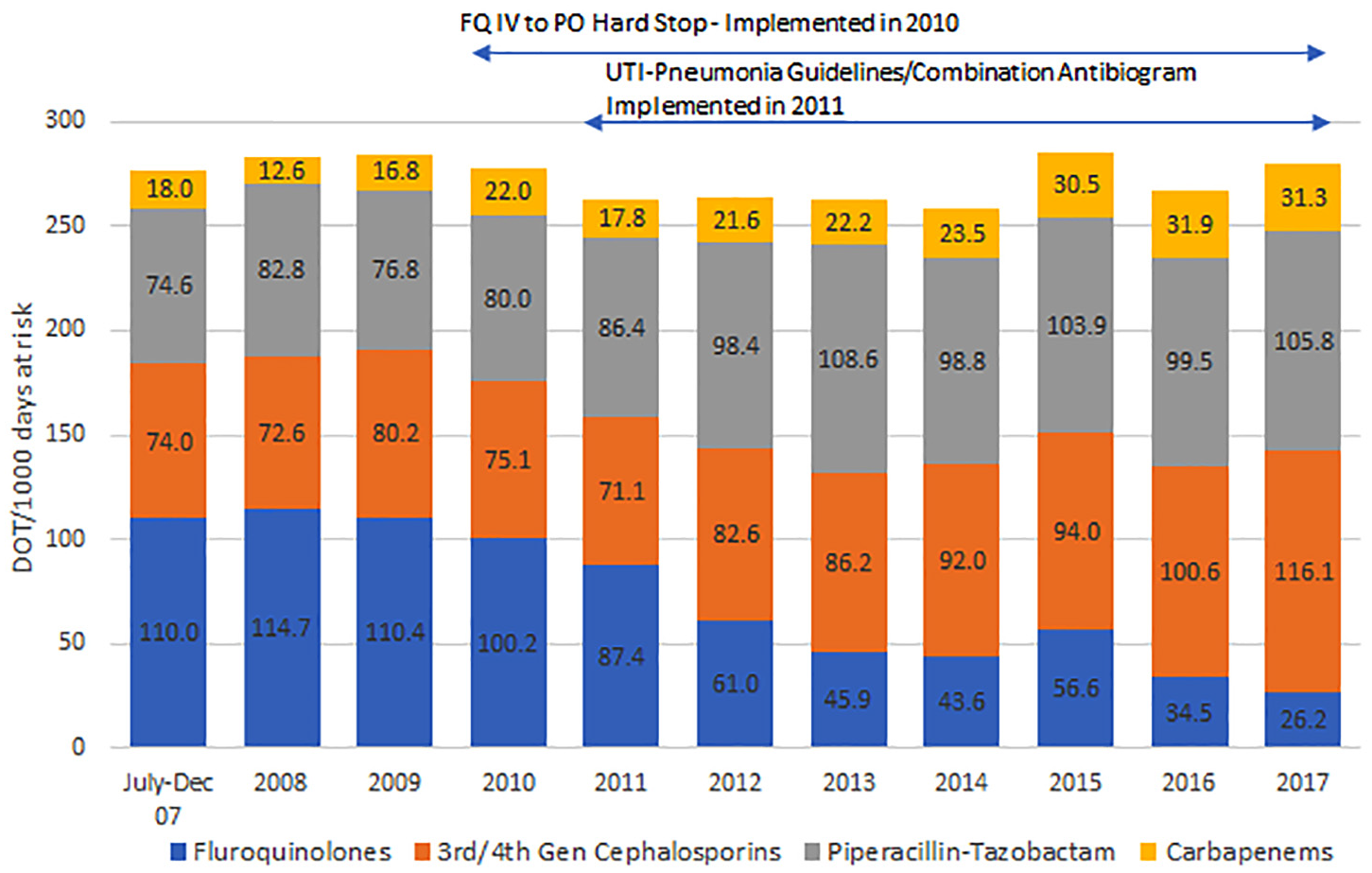
Fluoroquinolone utilization rates in an inpatient hospital setting compared to three other categories of broad-spectrum antibiotics by year, 2007–2017.
Trend in susceptibility
Overall 24,428 non-duplicate gram-negative isolates across all sources were analyzed, of which 7614 were HO and 16,814 were from the ambulatory care setting. For HO isolates (supplementary Table 1), Escherichia coli FQ susceptibility increased from 37.7% at baseline to 46.3% at the end of study period (p = 0.409); Klebsiella pneumoniae from 30.4% to 58.6% (p = 0.028); Proteus mirabilis from 37.0% to 72.9% (p = 0.024); and Pseudomonas aeruginosa from 52.6% to 66.7% (p = 0.721).
Correlation between antibiotic use and susceptibility
All correlations between reductions in FQ utilization rates and percent susceptibilities of HO isolates to ciprofloxacin were significant: p = 0.002 for Escherichia coli, p = 0.004 for Klebsiella pneumoniae, p = 0.02 for Proteus mirabilis, and p = 0.072) for Pseudomonas aeruginosa. The correlations between susceptibilities of HO isolates and other antibiotic use were not significant: all p > 0.138 for 3rd/4th Ceph, all p > 0.287 for piperacillin-tazobactam and all p > 0.082 except for Klebsiella pneumoniae (p = 0.035) for carbapenems.
Recovery and maintenance of susceptibility to FQ in HO isolates following ASP interventions in comparison to the high and relatively constant susceptibility of ambulatory isolates is shown in Figure 2.

Change in percent of ambulatory and inpatient hospital isolates susceptible to ciprofloxacin for four commonly encountered gram-negative bacteria by year, 2007–2017.
Discussion
Using a multifaceted intervention FQ use was reduced by 77% over an 11-year period, from 2007 to 2017, at a community-based teaching hospital. Previous studies have noted an increase in use of other broad-spectrum antibiotics when restrictions were applied to one group of antibiotics, a phenomenon described as “squeezing the balloon.” 9 In our study there was a corresponding increase in use of 3rd/4th Ceph, piperacillin-tazobactam, and carbapenems so that overall usage of broad-spectrum antibiotics did not change significantly over the study period
Most effective ASPs center around restrictive interventions and policies such as prior approval to curb unnecessary use of antibiotics. Two recent studies on interventions to improve antibiotic prescribing practices for hospitalized patients both concluded that enablement and restrictive interventions were independently effective. 10 Davey et al. defined enablement as “reducing barriers and/or increasing means to increase capability or opportunity” for change. In this study a series of persuasive interventions, including the development of disease specific guidelines using local susceptibility data and analytics, computer algorithms and education introduced over time were very effective in curbing FQ use. These interventions can appropriately be termed enablement, as each provided opportunity and capability to achieve the desired outcome.
The increase in FQ usage from July to September of 2015 that contributed to an overall increase that year was due to an outbreak of Legionella in the Bronx region of New York during those months. There was concern that the newly established hospital culture of avoiding FQs may have been broken. However, with re-emphasis of ASP interventions, usage was brought back under control shortly after the outbreak was declared officially over.
In light of the sustained decrease in FQ use, we looked at microbial sensitivities of gram-negative bacteria to ciprofloxacin as this was the most commonly used FQ in the institution. Prior studies have used annual institutional antibiograms which combined community-onset with HO isolates. We observed a relationship between hospital FQ use and FQ susceptibility of only HO gram-negative bacteria with significant improvement in susceptibilities. Susceptibilities to ciprofloxacin in HO organisms were used instead of overall antibiogram data as these isolates would be most affected by change in antibiotic usage within the hospital. We acknowledge that our intervention was not design to prove causality; nevertheless the association is a significant one and has clinical implications. The finding is further supported by the fact that susceptibility of ambulatory gram-negative isolates, measured over the same time period showed a trend toward increasing resistance to ciprofloxacin.
In conclusion, a simple persuasive ASP intervention was shown to have a durable effect on the reduction of FQ utilization rates. Even though performed at a single center, this institution is an inner-city hospital that shares common features with other hospitals in major urban centers in the US, many of which now utilize the services of an ASP, and electronic medical records. Thus, these findings can be generalized to other hospitals within the US.
Supplemental Material
sj-docx-1-sci-10.1177_00368504211011876 – Supplemental material for Association between fluoroquinolone utilization rates and susceptibilities of gram-negative bacilli: Results from an 8-year intervention by an antibiotic stewardship program in an inner-city United States hospital
Supplemental material, sj-docx-1-sci-10.1177_00368504211011876 for Association between fluoroquinolone utilization rates and susceptibilities of gram-negative bacilli: Results from an 8-year intervention by an antibiotic stewardship program in an inner-city United States hospital by Cosmina Zeana, Frank E. Palmieri, Vikas Gupta, Gang Ye, Peter Lao, Kalvin Yu, Kyoung-Sil Kang, Larry Schiller and Murli Purswani in Science Progress
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Vikas Gupta, Gang Ye, and Kalvin Yu are employees of Becton, Dickinson and Company, and may own stock and/or hold stock options in BD. The other authors have none to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
An expedited IRB approval was obtained, IRB # 05141507, and requirement for informed consent was waived for this study as the study was an anonymous retrospective analysis of existing data.
Informed consent
Requirement for informed consent was waived by the IRB.
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.