
Abstract
Urinary tract infections (UTIs) are one of the most important issues in modern medicine. In developing countries, the use of antibiotics is a common practice, and due to this, antibiotic resistance has increased. The objective of this research was to update and report on the microbiological profile of urinary tract infections based on the number of positive urine cultures (UCs), resistance, sensitivity, and the prevalence of bacterial strains. The results were obtained from the database of a tertiary medical facility in Western Mexico. The number of positive UCs was 1769 from inpatients and outpatients who were users of medical services in the hospital from January to December of 2017. The most commonly isolated microorganism was E. coli, with 1225 cases, of which 603 (49.2%) were ESBL (Extended-Spectrum Beta-Lactamase-producing bacteria) strains. The resistance rate of nitrofurantoin was 36.6%, and meropenem showed the most promising results with a resistance rate of only 7.1%. Resistances to quinolones and cephalosporins among the isolates investigated were 51%–67%. Based on our results, it is necessary to increase controls and to improve management protocols in order to achieve better medical practices by reducing antibiotic resistance.
Keywords
Introduction
Urinary tract infections (UTIs) are one of the most important public health problems in several countries. According with a 2007 report, there were 8642 ambulatory visits in thousands in the United States due to UTIs. 1 Based on the National Health System of Mexico, 1,077,230 new cases of UTIs were reported throughout the country in 2017. In Jalisco, a State located in the Western of Mexico, the number of cases was 62,750, corresponding to 5.8% of patients in Mexico. 2 Previous research from the Mexican Institute of Social Security in Jalisco reported 1512 cases of UTIs in 2015. 3
This trend in our institution has been accompanied by an increased resistance to antibiotics. The main concern in this regard is the need to use new broad-spectrum antibiotics—a practice which results in more economic costs for the National Health System.
These infections are caused by several pathogens including bacteria and fungi. More than 95% of cases are associated with one pathogen. The most frequent organism causing urinary tract infections is Escherichia coli, which has been isolated in 50%–90% of cases.4,5 Other common pathogens causing urinary tract infections are Proteus mirabilis and Klebsiella pneumoniae. 6
In general terms, UTIs are not a minor problem because they tend to increase in prevalence and feature antibiotic resistance. The aim of this research is to report epidemiological data regarding the antibiotic sensitivity and resistance of urinary tract infections in one of the largest tertiary medical centers in Mexico.
Materials and methods
The study was performed in The Western National Medical Center in Guadalajara, Jalisco Mexico, and included patients of both genders over 16 years of age who had been cared for at the hospital from January to December 2017. The sample included all urine cultures (inpatients and outpatients) that were requested for any reason in the medical facility. Outpatients samples were collected at their homes meanwhile inpatients samples were taken at the hospital.
For the statistical description, we used percentages, means, and frequencies. The analyzed data included urine culture results and demographic data from digital files.
Sample size was not calculated since all urine cultures were available for the study.
Urine cultures with more than 100,000 colony forming units/mL were considered as positive. Isolated bacteria, antibiotic resistance, and sensitivity were identified by an Automated Vitek® System (bioMérieux, Marcy I ‘Etoile, France).
Data were processed using Excel® (Microsoft, Redmond, WA, USA), and Open Epi (Open Source Epidemiologic Statistics for Public Health, Bill and Melinda Gates Foundation, Emory University, Atlanta, GA, USA).
This work was carried out with permission from the Research Ethics Committee, number 1001 (IMSS) with registration number 17 CI 11 020 146, and with authorization from the Federal Commission for Protection Against Sanitary Risk (COFEPRIS), registration number 11 CEI 003 2018080.
Results
A cross-sectional study was performed using data from digital files obtained from the Microbiology Laboratory of the Western National Medical Center. From January to December 2017, a total of 9928 samples were reported in the database. The number of samples included in the study was 6904, and the remaining samples were excluded (30.4%), due to contamination (more than three microorganisms and skin contamination) or inadequate sampling.
From the included samples, 25.6% were positive (n = 1769) and 74.4% were reported as being negative (n = 5135). From the positive culture, 1360 cases were outpatient samples and 409 were samples from inpatients. Table 1 shows the demographic data of the groups.
Demographic data of patients with positive cultures.

I: inpatient; O: outpatient; T: totals.
According to the database analysis, the most common pathogen was Escherichia coli, with 1225 cases. This corresponded to 69.2% of the total cases. The second most common microorganism was Klebsiella pneumoniae, with 223 cases (12.6%). Pseudomonas aeruginosa was the third most common, with 123 cases (7%). Related information is shown in Table 2.
Frequencies and percentages of isolated microorganisms from urine cultures.
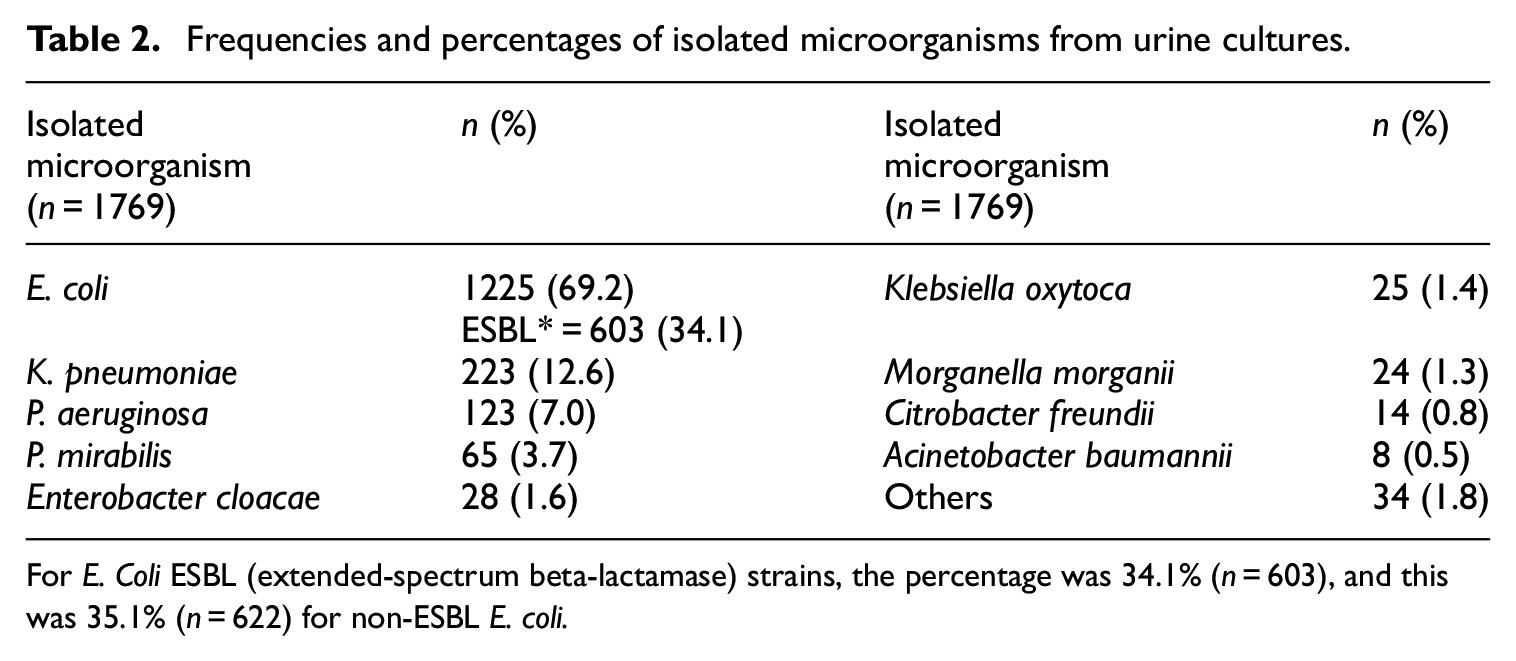
For E. Coli ESBL (extended-spectrum beta-lactamase) strains, the percentage was 34.1% (n = 603), and this was 35.1% (n = 622) for non-ESBL E. coli.
Regarding the microbiological profile (sensitivity and resistance), the research group reviewed the urine cultures in order to obtain independent results for outpatients and inpatients. As expected, P. aeruginosa and A. baumannii were the microorganisms with the highest resistance to antibiotics—at 70.4% and 74.2%, respectively. These microorganisms demonstrated a resistance higher than 50% for meropenem and ertapenem.
Table 3 shows the results regarding overall resistance to antibiotics in the entire group. Table 4 shows percentages, the average mean, and standard deviation (SD) with respect to resistance in both groups. Tables 5 and 6 denote the results for outpatients and inpatients, respectively.
Antibiotic resistance in both groups.

AMP: ampicillin; AMP/SUL: ampicillin/sulbactam; AZTREON: aztreonam; CEFAZOL: cefazoline; CEFTRIAX: ceftriaxone; CIPRO: ciprofloxacin; ERTAPEN: ertapenem; GENTAM: gentamicin; MEROPEN: meropenem; NITROF: nitrofurantoin; PIP/TAZ: piperacillin/tazobactam; SD: standard deviation; TIGECIC: tigecycline; TMP/SMX: trimethoprim-sulfametoxazole; TOBRA: tobramycin.
Specific percentages of resistance by microorganisms.

Antibiotic resistance in outpatients (n = 1360) by microorganism.

Antibiotic resistance in inpatients (n = 409) by microorganism.

A total of 125 positive UCs were sensitive to the entire antibiotic group. Resistance to four or fewer antibiotics was present in 505 cases, and 1139 demonstrated resistance to five or more antibiotics. In 76 cases, UTIs-responsible microorganisms showed resistance to all tested antibiotics. Table 7 shows the data regarding the number of antibiotics that were not suitable for treatment.
Number and percentage of ineffective antibiotics against bacteria based on antibiograms.

Discussion
Antibiotic resistance is a common public health issue in many countries. Based on the reports by Masajtis-Zagajewska and Foxman,7,8 UTIs are the most common bacterial infections acquired in hospitals and communities irrespective of age. The results obtained in our research may present a similar situation to those in other tertiary public medical centers in Mexico. In general terms, the number of UTIs increased from 1512 in 2015 to 1769 in 2017. 3
The new report included nitrofurantoin and demonstrated interesting results. The drug showed a sensitivity of 63%, surpassing broad-spectrum antibiotics such as ceftriaxone (45.8%), cefepime (48.6%) and ciprofloxacin (32.2%). The overall sensitivity for nitrofurantoin did not differ between outpatients and inpatients (62.8% and 64.7%). The antibiotic with the highest sensitivity was meropenem (92.8%), followed by ertapenem and amikacin, with sensitivities of 92.7% and 91.2%, respectively.
The resistances for ampicillin, ciprofloxacin, and trimethoprim-sulfamethoxazole were the highest in terms of percentages. In 2015, the reported resistance was 72.8% for ciprofloxacin, and its resistance decreased by 5%. In contrast, the resistance to ampicillin increased by 5.3%. Other broad-spectrum antibiotics such as meropenem (7.4% vs 7.1%) did not demonstrate any outstanding changes in resistance.
The microbiological profile showed no changes with respect to the most common microorganism, which was E. coli. The percentage of Echerichia coli producing β lactamases with an extended spectrum in 2015 was 48.5%, and in 2017, the number of cases was 49.2%. However, there was a difference in the second most common microorganism, which in 2015, was P. aeruginosa and in 2017, was K. pneumoniae.
Other authors have reported resistance to ciprofloxacin and ampicillin in different areas of Mexico. The percentages show a positive trend regarding ciprofloxacin; however, the trend was negative for ampicillin. Figure 1 shows the data from the preceding 7-year period regarding resistances for some antibiotics in Mexico.3,9–12

Antibiotic resistance trend in Mexico.
In 2011, Molina-Lopez et al. 9 outlined E. coli resistance in Mexico City. Amikacin demonstrated the lowest resistance during the previous years, compared to 2.5% in 2015 3 and our latest results of 9%. The same authors indicated similarities between ciprofloxacin and trimethoprim–sulfamethoxazole (56%), and some variations were revealed in 2017, based on the reports by Miranda-Estrada and Paniagua-Contreras, which demonstrated resistances of 45.8% and 66%, respectively.10,11 One of the most significant changes in the graph is the upward trend of ceftriaxone, which showed a resistance of 0% in 2014. 12 In addition, several changes were observed in 2015 and 2017.
There are no official data regarding an increase in ceftriaxone resistance. This fact notwithstanding, a possible reason for this increase is that, in the preceding 10-year period in Mexico, antibiotics such as levofloxacin and ceftriaxone have been over-prescribed by many health professionals without a credible rationale for doing so.
The management of urinary tract infections has been regulated based on antibiogram results. This clinical behavior was implemented in order to fulfill the economic objectives of different health systems around the world. Miller and Tang 13 reported on the risks and complications derived from the treatment of uncomplicated urinary tract infections with trimethoprim–sulfamethoxazole and showed suboptimal clinical outcomes. The same study described how antibiogram overestimates the number of cases which are resistant to trimethoprim-sulfamethoxazole. Fourteen years ago, the aforementioned authors described the current situation: the percentage of antibiotic resistance is increasing due to inadequate clinical practice in hospitals, especially in developing countries where the control of antibiotics is sub-optimal. According to the manuscript and clinical guidelines, antibiotics such as trimethoprim–sulfamethoxazole should not be used if resistance towards them is greater than 10%.
If our clinical practice is based on the prior statement, we have few options to manage UTIs. Thus, antibiotics such as ciprofloxacin, ampicillin, piperacillin/tazobactam, cefazoline, ceftriaxone, gentamicin, tobramycin and trimethoprim–sulfamethoxazole are not suitable for managing patients with UTIs since their resistances are greater than 20%.
UTIs are a public health concern in our institution, especially in patients who are being prepared for surgical procedures. This is not only a problem for the Urology department, but also for many surgical departments, such as in the cardiovascular and orthopedics departments, which have to postpone surgical procedures and manage complicated UTIs using a multidisciplinary approach. These problems result in delays in treatment for many patients, which puts their health at risk, and results in unnecessary expenses.
Based on the data from Table 7, we are investigating microorganisms that are resistant to all antibiotics that are exhibited in the antibiograms. The determination of the number of positive UCs for P. aeruginosa is a challenging problem that causes morbidity, mortality, and higher costs for patients that need to be free from infection in order to undergo surgery on the urinary tract. For patients who are asymptomatic, and where there is no adherence to surgery protocols, the use of antibiotics might be unnecessary. 14 Regarding positive UCs for Acinetobacter baumannii, cases are treated in a multidisciplinary way through the prescription of antibiotics such as daptomycin or linezolid which, in our medical facility, have zero resistance. Such cases are always managed by the Department of Infectious Diseases and supervised by the Department of Epidemiology. Fortunately, only eight cases derived from urine samples were reported in 2017.
Waller et al. 15 reported that it is important to know the local microbiological profile in order better clinical practice prescribing antibiotics and decreasing resistances in urinary tract infections worldwide. Recent research supports our statement regarding to avoiding the use of antibiotic management in asymptomatic UTIs in selected patients. Such measures have a great potential to decrease antibiotic resistance at some level. 16
Multidrug-resistant bacteria as a serious concern should be studied always is detected. An option is the use of combination therapy based on minimum inhibitory concentrations (MICs). Some antibiotics such as fosfomycin, tigecycline and minocycline have been used in combination with carbapenems managing imipenem-resistant Acinetobacter baumannii infections. The reported effects are a clear example that MICs should be taken in account when dealing with multidrug-resistant bacteria. 17 A better and innovative option for MDR microorganism management is Next-Generation Sequencing (NGS). This method is suitable to identify bacteria in UCs from patients with chronic or persistence UTIs. Gasiorek et al. 18 reported that the use of NGS could have a positive impact in outcomes, however, because the high cost its use is limited.
It is within our power to suggest the cautious use of antibiotics in our medical center by prescribing antibiotics based on an antibiogram and by resolving the source of infection in a multidisciplinary manner. However, as a tertiary medical center, many patients have been treated previously in other secondary and primary health institutions, where there are no data on antibiotic resistance, and as such, certain events and clinical decisions may be beyond our control. The problem is not only regional. A lack of information regarding the microbiological profile of UTIs is limited to some tertiary centers in Mexico. The findings reported in this work serve as an initiative. We will employ a hands-on approach when dealing with other institutions in order to share data and to obtain a larger database for establishing norms and guidelines that in turn, will be utilized to improve medical practices.
One of the strengths of this work is that it is the only study at the regional level supported by a previous publication, 3 showing that antibiotic resistance is a serious issue for public health in the west of Mexico. However, more research and epidemiologic data are necessary to make statements about this national and international health issue.
Conclusions
Urinary tract infections are an important public health issue, and, at present, they have worsened due to an increasing prevalence of antibiotic resistance, especially in hospitalized patients. Treatment should be based on the microbiological profile of the region or of a medical facility using broad-spectrum antibiotics to manage multidrug-resistant bacteria, while reducing the constraints associated with conventional antibiotic treatments. The results acquired should be useful in understanding how antibiotic resistance is developing and lead to better clinical practices. The information collected suggests that there must be better control of the selection and dosage of antibiotics and patient compliance with respect to their use. As a final point, antibiotic sensitivity and resistance could have far-reaching differences between regions and health facilities. In view of the above, it is recommended that the microbiological profile be measured in health facilities in order to obtain regional results and better clinical results for UTIs management and for other infections.
Footnotes
Acknowledgements
We sincerely thank the University of Guadalajara and the Mexican Institute of Social Security (IMSS). Without their assistance, this work would not have been possible.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This work was carried out with permission from the Research Ethics Committee, number 1001 (IMSS) with registration number 17 CI 11 020 146, and with authorization from the Federal Commission for Protection Against Sanitary Risk (COFEPRIS), registration number 11 CEI 003 2018080.
Informed consent
Not applicable. All data were reviewed from electronic files under permission of the Research Ethics Committee, number 1001 (IMSS).
Availability of data and materials
The data that supports the findings of this study is available from the corresponding author (Dr. Erick Sierra Diaz) but restrictions apply to the availability of this data, which was used under license for the current study, and as such, is not publicly available. Data is however available from the authors upon reasonable request and with permission from the Urology Department of the Western National Medical Center (IMSS).