
Abstract
Objectives:
Prenatal care starting in the first trimester is widely accepted as a best practice for improving maternal health. However, evidence is limited on the association between early prenatal care and maternal and infant health outcomes. This study evaluated maternal and infant health outcomes among nulliparous mothers to evaluate associations between late (≥4 months) prenatal care or no prenatal care compared with early (months 1-3) prenatal care.
Methods:
We used birth record data from the National Center for Health Statistics for this analysis. The study population consisted of singleton, nulliparous live births to mothers who gave birth in the United States from January 1, 2014, through December 31, 2022.
Results:
Compared with early prenatal care, late initiation of prenatal care was associated with an increased risk of preterm birth (risk ratio [RR] = 1.21; 99% CI, 1.15-1.28), insufficient gestational weight gain (RR = 1.23; 99% CI, 1.17-1.30), and no reported breastfeeding at discharge (RR = 1.09; 99% CI, 1.06-1.13). Compared with early prenatal care, no prenatal care was associated with substantially greater risk across nearly every measured outcome, including preterm birth (RR = 2.26; 99% CI, 1.82-2.80), low birth weight (RR = 2.03; 99% CI, 1.72-2.40), neonatal intensive care unit admission (RR = 1.88; 99% CI, 1.48-2.39), abnormal conditions of the newborn (RR = 1.87; 99% CI, 1.73-2.02), and no reported breastfeeding at discharge (RR = 1.90; 99% CI, 1.53-2.35). Prenatal care timing was not significantly associated with maternal morbidity.
Conclusion:
These findings highlight that although early prenatal care results in the best outcomes, late prenatal care still has important benefits relative to no prenatal care.
Early prenatal care starting in the first trimester of pregnancy (before the fourth month) is recommended by the American College of Obstetricians and Gynecologists and is widely accepted as a best practice for improving early detection and management of maternal and infant health concerns and decreasing poor maternal health outcomes. 1 Despite this widespread acceptance, to our knowledge, research on the importance of early initiation of prenatal care is largely lacking, and evidence on the association between early initiation of prenatal care and maternal and infant health outcomes is limited. The lack of research on associations between timing of prenatal care and maternal and infant health outcomes is constrained because no randomized controlled trial on early versus late initiation of prenatal care exists, and the ethics and logistics of such a trial make it unlikely that one will be conducted. Furthermore, confounding socioeconomic factors2-5 likely exist that are often difficult to control for in secondary data analysis. Prior research on early initiation of prenatal care is decades old or limited to small samples. A 2005 study demonstrated that missing visits early in pregnancy was associated with reduced birth weight. 6 Previous analyses of data from a single state or single health care facility found improvements in health outcomes associated with early prenatal care initiation. 7 A study using Fragile Families and Child Wellbeing data from 1998 through 2000 found associations between early prenatal care and maternal health behaviors relevant to child health (eg, smoking, breastfeeding, well-child visits). 8 A 2022 intervention study in Poland found that incentivizing early prenatal care improved infant health. 9 However, to our knowledge, no recent national analyses of the associations between early initiation of prenatal care and maternal and infant outcomes in the United States exist.
The objective of this study was to use national data to examine differences in pregnancy, birth, and delivery outcomes for nulliparous mothers and their infants based on whether women received early, late, or no prenatal care. 10
Methods
Data Source and Study Population
We used birth records data from the National Center for Health Statistics for this analysis. 11 The University of Arkansas for Medical Sciences Institutional Review Board determined this study was exempt from review because all records were deidentified. The study population consisted of singleton, nulliparous live births to mothers who gave birth in the United States from January 1, 2014, through December 31, 2022. We limited the study to nulliparous mothers to reduce the potential for confounding clinical or health-related factors prior to the current pregnancy. To examine the effects of prenatal care initiation on various birth outcomes, while reducing confounding cases, we included only singleton live births that were the first birth in the total birth order and excluded births with breech presentation.
Variables and Definitions
The primary independent variable of interest was the timing of prenatal care initiation, which was calculated by using the month of initiation of prenatal care and the total number of prenatal care visits. Early prenatal care was defined as initiating care within the first 3 months of pregnancy (months 1-3), late prenatal care as initiating care at month 4 or later, and never as having never received any prenatal care.
Delivery outcomes included cesarean delivery and maternal morbidity. Cesarean delivery was dichotomized as having a cesarean delivery or not. Maternal morbidity was a binary variable defined by using the Centers for Disease Control and Prevention User Guide for the Natality Public Use File 12 and captured whether the mother experienced a transfusion, a third- or fourth-degree perineal laceration, a uterine rupture, an unplanned hysterectomy, or intensive care unit (ICU) admission. Infant health outcomes included preterm birth, small for gestational age (SGA), low birth weight, admission to the neonatal ICU (NICU) for the newborn, abnormal conditions of the newborn (eg, assisted ventilation, surfactant, antibiotics for newborn, seizures), and no breastfeeding reported at discharge. Preterm birth was defined as birth occurring before 37 weeks of gestation. SGA was defined as birth weight lower than the 10th percentile for the given gestational age estimated by using the “growthstandards” R package.13,14 Low birth weight was defined as recorded weight of the newborn <2500 g. We examined 1 maternal health outcome, gestational weight gain, which we coded as insufficient, healthy, or excessive depending on whether the amount of weight gain was below, within, or greater than the current Institute of Medicine–recommended ranges based on prepregnancy body mass index (BMI) (underweight: 28-40 pounds; normal: 25-35 pounds; overweight: 15-25 pounds; obesity class I-III: 11-20 pounds).
We adjusted models for birth year (2014-2022), state of residence (including Washington, DC), maternal age (continuous, in years), maternal education level (elementary [did not graduate from high school]; secondary [graduated from high school]; postsecondary [some college or higher]), maternal nativity (native to the US or not), maternal race and ethnicity, maternal partner status (married, paternity acknowledged, or neither), prepregnancy BMI (kg/m2), prepregnancy diabetes, and prepregnancy hypertension.
Statistical Analysis
The final sample included approximately 10 million total births, although the sample size for specific health outcomes varied based on the missingness of those variables in the data (range, 9 940 128 to 10 495 726).
We fit logistic regression models by using the “fixest” R package to examine the adjusted association between prenatal care initiation (early, late, or never) and each health outcome. 15 For each outcome, we estimated both the difference in relative risk (risk ratio [RR]) and the difference in absolute risk (percentage-point difference) between the 3 levels of the prenatal care variable using the “marginaleffects” R package with cluster-robust SEs for state of residence. We computed pairwise contrasts as average marginal effects evaluated at the mean of the covariates. Because the RR and risk difference are nonlinear functions of the model parameters, we used the delta method to approximate their sampling distributions, propagating the cluster-robust SEs for state of residence from the underlying model. We used the resulting SEs to construct Wald-type 99% CIs and corresponding P values for each contrast. The reference group was early prenatal care, and we made all comparisons relative to this group unless otherwise specified. Because of the large sample size, we performed all analyses with significance set at P < .01 and calculated 99% CIs.
Results
Mothers who had early prenatal care initiation had higher educational attainment; were older; were more likely to be White, married, and a US native; and were more likely to have prepregnancy obesity than mothers without prepregnancy obesity (Table 1).
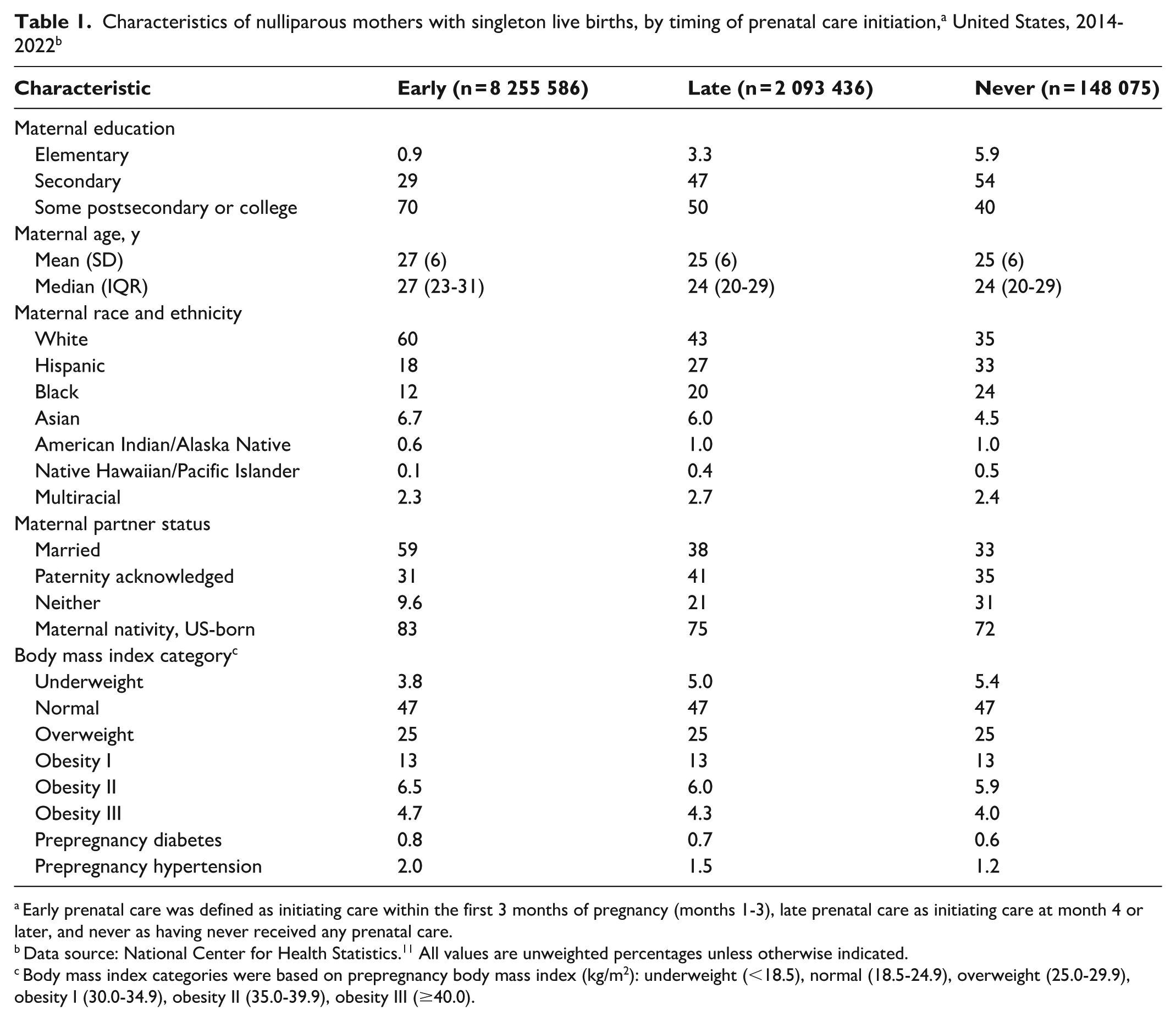
Early prenatal care was defined as initiating care within the first 3 months of pregnancy (months 1-3), late prenatal care as initiating care at month 4 or later, and never as having never received any prenatal care.
Data source: National Center for Health Statistics. 11 All values are unweighted percentages unless otherwise indicated.
Body mass index categories were based on prepregnancy body mass index (kg/m2): underweight (<18.5), normal (18.5-24.9), overweight (25.0-29.9), obesity I (30.0-34.9), obesity II (35.0-39.9), obesity III (≥40.0).
Weight Gain During Pregnancy
Late initiation of prenatal care was associated with a higher relative risk of insufficient gestational weight gain compared with early initiation of prenatal care (RR = 1.23; 99% CI, 1.17-1.30; P < .001; Table 2). Mothers who never received prenatal care had a higher relative risk of insufficient gestational weight gain than did mothers with late initiation of prenatal care (RR = 1.47; 99% CI, 1.25-1.74; P < .001).

Early prenatal care was defined as initiating care within the first 3 months of pregnancy (months 1-3), late prenatal care as initiating care at month 4 or later, and never as having never received any prenatal care.
Data source: National Center for Health Statistics. 11
Reference group in model entered as early prenatal care.
Logistic regression models with cluster-robust SEs for state of residence. Significance set at P < .01.
We observed the opposite pattern for excessive gestational weight gain, with a relative reduction in risk for mothers with a late initiation of prenatal care compared with mothers with early initiation of prenatal care (RR = 0.93; 99% CI, 0.91-0.95; P < .001; Table 2). The relative risk of excessive gestational weight gain was lower for those who never received prenatal care than for those with early initiation of care (RR = 0.74; 99% CI, 0.68-0.81; P < .001). We also found a reduction in relative risk of excessive gestational weight gain for those who never received prenatal care compared with those with late initiation of prenatal care (RR = 0.80; 99% CI, 0.74-0.87; P < .001).
Preterm Birth
Late initiation of prenatal care was significantly associated with an increased relative risk of preterm birth compared with early initiation of prenatal care (RR = 1.21; 99% CI, 1.15-1.28; P < .001; Table 2). The effect was substantially larger for mothers who never received prenatal care (RR = 2.26; 99% CI, 1.82-2.80; P < .001) compared with mothers with early initiation of prenatal care. In addition, mothers who never received prenatal care had an increased relative risk compared with mothers with late initiation of prenatal care (RR = 1.86; 99% CI, 1.55-2.23; P < .001).
Cesarean Delivery and Maternal Morbidity
Late initiation of prenatal care was associated with a slightly lower relative risk of cesarean delivery compared with early initiation of prenatal care (RR = 0.98; 99% CI, 0.96-0.99; P < .001; Table 2). Mothers who never received prenatal care had an even lower relative risk of cesarean delivery than mothers with early initiation of prenatal care (RR = 0.87; 99% CI, 0.83-0.91; P < .001). Similarly, mothers with no prenatal care had a lower relative risk of cesarean delivery than mothers with late initiation of prenatal care (RR = 0.89; 99% CI, 0.84-0.93; P < .001). However, the timing of prenatal care use was not significantly associated with maternal morbidity being reported in the birth record (P = .93).
Low Birth Weight and SGA
Mothers with late initiation of prenatal care did not have a significant increase in low birth weight than mothers with early initiation of prenatal care (Table 2). However, no prenatal care was associated with more than twice the relative risk of low birth weight compared with early initiation of prenatal care (RR = 2.03; 99% CI, 1.72-2.40; P < .001). Similarly, the relative risk of low birth weight was higher among mothers with no prenatal care than among mothers with late initiation of prenatal care (RR = 2.08; 99% CI, 1.80-2.41; P < .001).
Mothers with late initiation of prenatal care had a slightly lower relative risk of SGA than mothers with no prenatal care (RR = 0.97; 99% CI, 0.96-0.99; P < .001; Table 2). No prenatal care was associated with a higher relative risk of SGA compared with early initiation of prenatal care (RR = 1.25; 99% CI, 1.18-1.32; P < .001). Similarly, no prenatal care was associated with a higher relative risk of SGA compared with late initiation of prenatal care (RR = 1.28; 99% CI, 1.20-1.36; P < .001).
NICU Admission and Abnormal Conditions of the Newborn
We found no difference in relative risk between late and early initiation of prenatal care related to NICU admission. No prenatal care was associated with nearly twice the relative risk of NICU admission compared with early initiation of prenatal care (RR = 1.88; 99% CI, 1.48-2.39; P < .001; Table 2). Similarly, no prenatal care was associated with a higher relative risk of NICU admission compared with late initiation of prenatal care (RR = 1.83; 99% CI, 1.69-1.99; P < .001).
Late initiation of prenatal care was not associated with an increase in the relative risk of abnormal conditions of the newborn. No prenatal care (vs early initiation of prenatal care) was associated with a large increase in the relative risk of abnormal conditions of the newborn (RR = 1.87; 99% CI, 1.73-2.02; P < .001; Table 2). Compared with late initiation of prenatal care, never receiving prenatal care was associated with a higher relative risk of abnormal conditions of the newborn (RR = 1.83; 99% CI, 1.69-1.99; P < .001).
No Breastfeeding at Discharge
Late initiation of prenatal care (vs early initiation of prenatal care) was associated with a higher relative risk of no breastfeeding reported at discharge (RR = 1.09; 99% CI, 1.06-1.13; P < .001; Table 2). No prenatal care (vs early initiation of prenatal care) was associated with a significant increase in relative risk of no breastfeeding reported at discharge (RR = 1.90; 99% CI, 1.53-2.35; P < .001). Compared with mothers with late initiation of prenatal care, mothers with no prenatal care had an increased relative risk of no breastfeeding reported at discharge (RR = 1.74; 99% CI, 1.40-2.15; P < .001).
Discussion
This national study evaluated the rates of adverse maternal and infant health outcomes associated with late (≥4 months gestation) initiation of prenatal care or no prenatal care compared with early initiation of prenatal care among nulliparous mothers. Consistent with current guidance, the results demonstrate that better perinatal health outcomes are associated with early prenatal care initiation across most study outcomes. Early initiation of prenatal care was associated with reduced rates of insufficient weight gain, preterm birth, low birth weight, NICU admission, and abnormal newborn conditions, as well as higher rates of breastfeeding at discharge, although rates of cesarean delivery and excessive weight gain were modestly lower among mothers initiating care late or not at all. No prenatal care was associated with increased risk of adverse health outcomes relative to late initiation of prenatal care across nearly every measured health outcome, including preterm birth, low birth weight, NICU admission, abnormal conditions of the newborn, and lower rate of reported breastfeeding at discharge. These findings highlight that although early initiation of prenatal care may result in the best health outcomes, late initiation of prenatal care still has important benefits relative to no prenatal care.
Limitations
This study had several limitations. First, the study used observational data and, therefore, did not establish causation. Second, birth record data were used for prenatal care initiation and other variables, and some have questioned the reliability of birth record data, which vary substantially depending on the variables of interest.16,17 Although the accuracy of demographic and birth weight data from birth records is generally high, data on the early initiation of prenatal care is generally considered moderate. 18 Agreement between birth records and medical records for the derived item of first-trimester prenatal care initiation has been documented at 83%. 19 Misclassification of a categorical independent variable may bias estimates depending on the direction and pattern of error. Third, there are likely confounding variables for women who receive no prenatal care, such as sociodemographic, behavioral, and health-seeking characteristics. There are also possible constraints and confounding reasons why pregnant women receive no prenatal care. These constraints include language barriers, delayed Medicaid approval, lack of transportation, lack of paid leave, or living in maternity care deserts.2-5 These confounding variables are not captured on the birth record and, therefore, could not be controlled for. Finally, previous studies have found that prenatal care adequacy is an important predictor of birth outcomes. Although such information was available in the current study data, this study focused on the timing of prenatal care initiation, a key component of prenatal care adequacy 20 and an easily communicated recommendation.
Conclusions
Although previous studies have found improvements in maternal and infant health outcomes associated with prenatal care initiation, evaluations of early initiation of prenatal care relative to late initiation of prenatal care have been limited, leaving researchers, policymakers, and health care providers without evidence to support recommendations. This article adds to the literature by documenting important associations between early initiation of prenatal care and a reduction in many adverse maternal and infant health outcomes. Given the health and cost implications of adverse perinatal health outcomes for maternal and infant health throughout the life course, reducing adverse infant and delivery outcomes is a national priority. 21 Policies and practices to help ensure women receive early prenatal care could improve maternal and infant health outcomes and reduce health care costs. Effective policies could include prepregnancy and presumptive Medicaid and programs, which have helped women with socioeconomic constraints overcome social barriers.4,22,23
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by University of Arkansas for Medical Sciences Translational Research Institute funding awarded through the National Center for Advancing Translational Sciences of the National Institutes of Health (UL1 TR003107).
Disclaimer
All statements in this article, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the funder.